Embed Size (px)
Citation preview

Thorax 1982;37:822-827
Interpretation of pleural biopsy specimens andaspirates with the immunoperoxidase techniqueAMANDA HERBERT, PATRICK J GALLAGHER
From the Department ofPathology, Southampton General Hospital, Southampton
SUMMARY In pleural biopsy specimens and histological sections from the fibrin clots of pleuralfluid aspirates it may be difficult to distinguish reactive mesothelial cells from malignantmesothelial cells and metastatic carcinoma. Reactive pleurisy with effusion is usually associatedwith loss of cohesion and exfoliation of mesothelial cells, which is consistent with the hypothesisthat they act as facultative histiocytes. A series of biopsy specimens and sections of clots frombenign and malignant pleural effusions have been stained by the immunoperoxidase technique forthe histiocytic markers a,-antitrypsin, a -antichymotrypsin, and lysozyme (muramidase). Eightcases of mesothelioma were included. Mesothelial cells when seen as a monolayer lining the pleuralsurface were negative. Reactive mesothelial cells, usually seen as exfoliated cells, were consistentlystrongly positive for a -antichymotrypsin and more variably for al-antitrypsin and lysozyme.Malignant cells, whether from carcinoma or from mesothelioma, were usually but not alwaysnegative. Consequently immunohistochemical staining for ac-antichymotrypsin is often helpful indistinguishing reactive mesothelial cells from malignant cells.
In a recent study of the morphological interpretationof pleural biopsy specimens and sections of the fibrinclots from aspirates we observed that reactive pleu-risy was usually associated with loss of cohesion andexfoliation of mesothelial cells.I This helped todistinguish reactive from neoplastic mesothelium,which was suggested by cohesive papillary prolifera-tion. Despite this it may be difficult on purelymorphological criteria to differentiate reactive fromneoplastic mesothelial cells on the one hand and frommetastatic carcinoma on the other. The same prob-lem exists in the interpretation of cytologicalpreparations of pleural fluid, where reactivemesothelial cells may be difficult to distinguish frommalignant cells, particularly in certain conditionssuch as pulmonary infarction and hepatic cirrhosis.9Furthermore, the cytological diagnosis of meso-thelioma tends to be less reliable than that ofcarcinoma,21 although cytological examinationusually yields more positive diagnoses of malignancythan does closed biopsy. ' I
Two approaches have been made in thehistochemical interpretation of pleural fluids. One isto stain positively for the malignant cells. Epithelial
Address for reprint requests: Dr A Herbert, Department ofPathology, Level E, South Pathology and Laboratory Block,Southampton General Hospital, Southampton S09 4XY.
membrane antigen has proved helpful in this respectas it shows a constant though quantitative differencein staining between most malignant cells and reactivemesothelial cells.6 The other approach is to stainpositively for the reactive cells. Mesothelial cells, likemacrophages and histiocytes, have been shown tocontain enzymes such as non-specific esterase andnaphthol A-SD chlordcetate,7 but the staining pat-terns have not been found to be useful fordistinguishing benign and malignant cells.8 Further-more, these enzymes cannot be readily demonstratedin formalin-fixed paraffin-embedded tissue.One constant observation has been that reactive
mesothelial cells contain brightly staining periodic-acid-Schiff '(PAS)-positive, diastase-resistant gran-ules in their cytoplasm."' This renders the PAStechnique of little value in the distinction of reactivecells from adenocarcinoma, which often containsintracytoplasmic PAS-positive, diastase-resistantepithelial mucin. Similar granules are also present inhistiocytes such as pulmonary macrophages and theycorrelate with positive staining for the glycoproteinprotease inhibitor a,-antitrypsin. This is now knownto be synthesised by histiocytes"2 and rat pulmonarymacrophages,"3 although not being entirely specificfor this series of cells. Alpha-1-antichymotrypsin hasalso been shown to be positive in malignanthistiocytosis'4 and malignant fibrous histiocytoma."
822
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from

Interpretation ofpleural biopsy specimens and aspirates with the immunoperoxidase technique
Alpha-1-antitrypsin as well as a,-antichymotrypsinand lysozyme are useful markers for histiocytes,which can be readily identified in formalin-fixedparaffin-embedded histological sections. The objectof this study was to examine their range of staining innormal, reactive, and neoplastic mesothelium and inmetastatic carcinoma. This technique has advantagesfor the interpretation of pleural biopsy specimens.
Methods
PATIENTS STUDIEDThe material was taken from a series of 95 closedbiopsies, 23 open biopsies and pleurectomies, and158 sections of pleural clots, which represented allthe surgical specimens of pleura received from theSouthampton General and Western Hospitals duringone year (1976). Sections from all 22 closed biopsyspecimens that included recognisable reactive orneoplastic mesothelium were cut and stained. Speci-mens from a selection of open biopsies, includingcases of mesothelioma, fibrous pleurisy, empyema,and eosinophilic pleuritis associated with pleurec-tomies for pneumothorax, were also stained, as wereeight fibrin clots from cases of proved reactivepleurisy and 16 fibrin clots from cases of provedmalignant effusion. In some of the small biopsyspecimens there was no mesothelial tissue left in theblock when they were recut. Patients' notes hadbeen available for follow-up and confirmation ofdiagnoses.
IMMUNOPEROXIDASE STAININGSections were stained for a -antitrypsin, a1-antichymotrypsin, and lysozyme by the unlabelledantibody peroxidase-antiperoxidase (PAP) tech-nique16 with -prior trypsinisation,' rabbit antihumanserum obtained from Dako-immunoglobulins beingused. For a -antitrypsin and lysozyme control sec-tions were biocked with purified antigens, but thesewere not available for al-antichymotrypsin. As anegative control whole rabbit serum was substitutedfor the rabbit antihuman primary antiserum in eachof the staining procedures.
Results
NORMAL AND REACTIVE MESOTHELIUMIn six cases in which there was a single layer ofcuboidal mesothelial cells lining the pleural surfaceor inflammatory bands and adhesions these cellswere found to be negative for al-antitrypsin, al-antichymotrypsin, and lysozyme. Diffuse palecytoplasmic staining was occasionally noted, but thisis regarded as a non-specific finding. Positivity istaken as granular intracytoplasmic staining.
In eight cases clumps of reactive mesothelial cellswere included which were either closely applied tothe surface of a reactive pleurisy or exfoliated. Thesecells stained strongly for a1-antichymotrypsin andrather more variably for a1-antitrypsin and lysozyme.The same staining pattern was seen in the exfoli-
ated cells in eight fibrin clots from pleural effusionsproved to be reactive (fig 1-3). Granulation tissuelining and chronic fibrous pleurisy organisingempyema (four cases stained) showed strong stainingof tissue histiocytes for a1-antitrypsin, a1-antichymotrypsin, and lysozyme. Surface meso-thelial cells were not seen in these cases.
Giant cell histiocytes, as seen in tuberculousempyema and the pleuritis associated with pneu-mothorax, showed strong positive staining forlysozyme but were negative for a1-antitrypsin and a1-antichymotrypsin. These findings are summarised intable 1.
MESOTHELIOMASections of the final, definitive thoracotomy orpostmortem specimens were stained from eight pa-tients in this series who proved to have malignantmesothelioma. The staining reactions aresummarised in table 2.
All sections were negative for lysozyme. Two outof eight showed focal fine granular staining for a,-antitrypsin in epithelial-type cells. Four out of eightshowed similar focal staining for a1-antichymotrypsin(figs 4 and 5). In one case there was also some focalintracytoplasmic staining in fibroblastic areas. In allthese cases the majority of the tumour cells werenegative and the positive staining was less intensethan seen in reactive exfoliated mesothelial cells.
Sheets of abnormal mesothelial cells and papillaryproliferations stained in three small biopsy specimensfrom patients later shown to have mesothelioma werenegative for both protease inhibitors and lysozyme.Exfoliated papillary structures in pleural clots fromtwo patients later shown to have mesothelioma werealso negative.
METASTATIC CARCINOMAFourteen sections from fibrin clots of proved carcino-matous malignant effusions and four biopsyspecimens in which there was a mixture of malignantcells and reactive mesothelial cells were stained. Thestaining reactions for a1-antichymotrypsin, which wasmost sensitive for demonstrating reactive mesothelialcells, are summarised in table 3. There were noinstances of a1-antitrypsin staining in the absence ofal-antichymotrypsin in benign or malignant cells. Thebackground of reactive cells in these biopsy speci-mens and clots stained strongly for a1-antichymotrypsin, whereas in most cases the
823
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from

Herbert, Gallagher
a
4~~~~~~~~~h4
~ . 3 ;
* 5 12 t4 * ~4*
f
4
~~ ~ ~ ~ ~ 1.
1 2 3
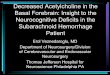
Figs 1-3 Pleuralfluid clotfrom a patient with reactive pleurisy. 1 Mixed lymphocytes and reactive mesothelial cells.
(Haematoxylin and eosin, x400.) 2 Reactive cells staining intensively for ca,-antichymotrypsin. (Peroxidase-
antiperoxidase, x540). 3 Only occasional cells (arrow) staining for lysozyme. (Peroxidase-antiperoxidase, x400.)
Table 1 Results ofimmunoperoxidase staining ofreactive mesothelial cells and histiocytes
No ofcases a,-Antitrypsin a,-Antichymotrypsin Lysozyme
Surface lining mesothelial cells 6 - - -Reactive and exfoliated
mesothelial cells 16 + + +Tissue histiocytes in
pleural granulation tissue 4 + + +Giant cells 4 - - +
+Strong granular cytoplasmic staining; ±weak or variable staining; -no staining reaction.
Table 2 Results ofimmunoperoxidase staining ofmalignant mesotheliomas
a,-Antitrypsin a,-Anichymotrypsin Lysozyme
EpithelialMixed,, + + _
- +_,, +,,
+Fn
+Focal intracytoplasmic staining; -no staining reaction.
Table 3 Alpha-1-antichymotrypsin staining ofmalignantcells (background of reactive cells strongly positivein all cases)
Strongly positive Weakly positive Negative
CarcinomaClosed biopsy
specimen 1 3Fibrin clot 1 1 12
MesotheliomaClosed biopsy
specimen 2Fibrin clot 2
824
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from

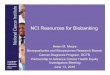
Fig 4 Biphasic malignant mesothelioma with both glandular epithelial and mesenchymal components. (Haematoxylin andeosin, x160.)Fig 5 Biphasic malignant mesothelioma (same case as infig 4): stainingfor a,-antichymotrypsin on right but not on leftside. (peroxidase-antiperoxidase, x660); detailed view ofdark positive cytoplasmic staining in inset (c x2000.)
S.L, on.&
I . .Z, SIt
4*. ,e.s. o, 4 *
*~~~~* C
S
r
a
0
*a
a
0 4p~~~~~.1p 4 a
9;.a
t PO a40
6
a t*..i, or:..t.
*k f
*0'A
I. 9 ' S.
4,.~~~~~~~~41 0 9OS1
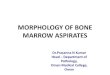
Fig 6 Pleuralfluid clotfrom metastatic mammary carcinoma: two malignant acini stand out against associated reactive
mesothelial cells. (Haematoxylin and eosin, x660.)
Fig 7 Pleuralfluid clotfrom metastatic mammary carcinoma (same case as infig 6): reactive pleural cells stainingpositively for a,-antichymotrypsin (black) but malignant acini negative. (Peroxidase-antiperoxidase technique, x 660.)
4*
S *.,r
-: 4,
E ;. i S;F;< .. :2tl;-
:- ....
^ ' :#
*' :h:0 i:
X
_ ;
s: S
bawOr.-..z..g..s..i.. ..
a:'s
It
r*
..*::'Ps,
C.
A:o.
4
a
S'.9.
**S4k.)w
07
F..
*16
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from

Herbert, Gallagher
*8 , #
S '4 ~~~~
,,*Wt'¼; g+ *r t'* X
* * 4'4 4 4 ;# s..
(Heaoyi a&ndL eosin, w20.. Ap fi ( w g
8
Fig 8 Numerous acinarformations in pleuralfluid clotfrom(Haematoxylin and eosin, x280.)
i4~
Ms a..
..; A..0*.
;-)
9a patient with metastatic mammary carcinoma.
Fig 9 Pleuralfluid clotfrom metastatic mammary carcinoma (same case as infig 8): in contrast to the general rulemalignant cells staining positively (black) for a,-antichymotrypsin. (Peroxidase-antiperoxidase technique, x280.)
malignant cells were negative. In two cases car-cinoma cells also were strongly positive and in onecase they were weakly positive. The results ofstaining cells from malignant effusions and biopsyspecimens for a antichymotrypsin are summarised intable 3.Where the malignant cells were negative or weakly
positive they stood out clearly against a backgroundof strongly positive reactive cells (figs 6 and 7). In theunusual cases in which tumour cells were stronglypositive, reactive and malignant cells could not bedistinguished by this method (figs 8 and 9).
Discussion
The staining of exfoliated mesothelial cells for a1-antitrypsin and lysozyme is consistent with thehypothesis that in pleural effusions and reactivepleurisy mesothelial cells can act as facultativehistiocytes. Immunohistochemical studies on pleuralcells suggest that forms transitional betweenmesothelial cells and macrophages exist in pleural
fluid,9 and ultrastructural studies on pleural fluid cellsshow evidence of exfoliation of mesothelial cellsassociated with gradual alterations in membranestructure and forms transitional between mesothelialcells and macrophages. 18 Staining for epithelial mem-brane antigen also shows differences betweenexfoliated mesothelial cells, which retain surfaceantigen, and macrophages.1 The ability ofmesothelial cells to synthesise a1-antitrypsin is re-flected in the proportion of mesotheliomas whichshow focal positive staining. This pattern of stainingis very similar to that seen in malignant fibroushistiocytomas.'5 The strong staining of reactiveexfoliated pleural cells for a1-antichymotrypsin cor-related with previous observations of PAS-positivegranules in reactive mesothelial cells and pleuralmacrophages, and we have found that this is areliable way of demonstrating reactive cells in pleuralbiopsy specimens and fibrin clots because it is moresensitive than a,-antitrypsin and lysozyme. We areaware that for this study we did not have purifiedblocking antigen for controlling the specificity of the
826
't' ....l. gol
*9-1
A ..k .:
4W,VCe.1""W
AIII
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from

Interpretation ofpleural biopsy specimens and aspirates with the immunoperoxidase technique
ai-antichymotrypsin antiserum. In this instance it isto some extent compensated for by the fact that weare emphasising the significance of negative-stainingmalignant cells with a background of positive-stain-ing reactive cells rather than vice versa.
It must be emphasised that carcinomas of varioustypes can synthesise antiproteases. In this series theseenzymes were seen in isolated cases of breast,gastrointestinal, and pulmonary metastases. Thepractical use of the technique lies in the fact that ithelps to identify malignant cells in small biopsyspecimens and fibrin clots, which may be difficult todistinguish from reactive mesothelial cells bymorphology alone. The fact that neoplasticmesothelial cells are usually negative is sometimesalso helpful in assessing small biopsy specimens in thediagnosis of malignant mesothelioma.
We thank the Southampton pathologists and pulmo-nary physicians for access to their histologicalmaterial and clinical records, Karen Britten andMary Judd for the immunohistochemical prepara-tions and illustrations, and Penny Robertson fortyping the manuscript.
References1 Herbert A, Gallagher PJ. Pleural biopsy in the diagnosis
of malignant mesothelioma. Thorax 1982;37:816-21.2 Naylor B. The exfoliative cytology of diffuse malignant
mesotheliomaJ Pathol Bacteriol 1963;86:293-8.Roberts GH, Campbell GM. Exfoliative cytology of
diffuse mesothelioma. J Clin Pathol 1972;25:577-82.Tao LC. The cytopathology of mesothelioma. Acta Cytol
1979;23:209-13.Frist B, Kahan AV, Koss LG. Comparison of the
diagnostic values of biopsies of the pleura and cytologicevaluations of pleural fluids. Am J Clin Pathol1979;72:48-51.
6 To A, Coleman DV, Deamaley DP, Ormerod MG,
Steele K, Neville AM. Use of antisera to epithelialmembrane antigen for the cytodiagnosis of malignancyin serous effusions. J Clin Pathol 1981;34:1326-32.
Efrati P, Nir E. Morphological and cytochemical inves-tigation of human mesothelial cells from pleural andperitoneal effusions. IsraelJ Med Sci 1976;12:662-73.
8 Clausen PP, H0jgaard K, Thommesen N. The diagnosticvalue of cytochemical staining for non-specific esterasein the search for cancer cells in effusions. Acta PathMicrobiol Scand Sect. A. 1979;87:347-52.
9 Koss LG. Effusions in the absence of cancer. Diagnosticcytology and its histopathological basis. 3rd ed. Phila-delphia: JP Lippincott, 1979:878-910.
10 Pfitzer P, Huth F. Alcian-PAS positive granules inmesothelioma and mesothelial cells. Acta Cytol1966;10:205-13.
" Foot NC. The identification of mesothelial cells in sedi-ments of pleural effusions. Cancer 1959;12:429-37.
12 Isaacson P, Jones DB, Millward-Sadler GH, Judd MA,Payne S. Alpha-1-antitrypsin in human macrophages. JClin Pathol 1981 ;34:982-90.
13 White RR, Lee DK, Habicht GS, Janoff A. Secretion ofa protease inhibitor by cultured rat alveolar macro-phages. Am Rev Respir Dis 1981;123, No 4 part 2(suppl): 222.
14 Meister P, Huhn D, Nathrath W. Malignant histiocytosis.Immunohistochemical characterization on paraffinembedded tissue. Virchows Arch A Path Anat Histol1980;385:233-46.
15 du Boulay CEH. Demonstration of a, antitrypsin and a,antichymotrypsin in fibrous histiocytomas using theimmunoperoxidase technique. Am J Surg Pathol1982;6:559-64.
16 Sternberger LA. Immunocytochemistry 2nd ed. NewYork: John Wiley and Sons, 1979:104-69.
17 Mepham BL, Frater W, Mitchell BS. The use ofproteolytic enzymes to improve immunoglobulin stain-ing by the PAP technique. Histochem J 1979;11:345-57.
18 Domagala W, Koss LG. Configurations of surfaces ofcells in effusions by scanning electron microscopy. In:Koss LG, Coleman DV, eds. Advances in clinicalcytology. London: Butterworths, 1981:270-313.
827
on 2 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.37.11.822 on 1 Novem
ber 1982. Dow
nloaded from