Embed Size (px)
Citation preview
IMPACT Act: Standardized Patient Assessment Data Activities
March 29, 2017
Disclaimer
This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently so links to the source documents have been provided within the document for your reference.
This presentation was prepared as a service to the public and is not intended to grant rights or impose obligations. This presentation may contain references or links to statutes, regulations, or other policy materials. The information provided is only intended to be a general summary. It is not intended to take the place of either the written law or regulations. We encourage readers to review the specific statutes, regulations, and other interpretive materials for a full and accurate statement of their contents.
2
Acronyms in this Presentation • DE – Data element
HHAs – Home health agencies• IMPACT Act – Improving Medicare Post-Acute Care
Transformation Act of 2014• IRFs – Inpatient rehabilitation facilities• IRF-PAI – IRF-Patient Assessment Instrument• LCDS – LTCH CARE Data Set• LTCHs – Long-term care hospitals• MDS – Minimum Data Set• OASIS – Outcome and Assessment Information Set• PAC – Post-acute care• PAC-PRD – Post-Acute Care Payment Reform
Demonstration• QRP – Quality reporting program• SNFs – Skilled nursing facilities• TEP – Technical Expert Panel
3
BS – Home and Community Based Services •
• FASI – Functional Assessment Standardized Items• HC
Agenda
4
• The Goal of the IMPACT Act • Timeline of Activities • Alpha 1 Results • Alpha 2 Progress • Plans for Beta Test • How to Get Involved
Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014
• Bipartisan bill passed on September 18, 2014 and signed into law by on October 6, 2014
• Requires standardized patient assessment data across Post-Acute Care (PAC) settings to enable: ‒ Improvements in quality of care and outcomes ‒ Comparisons of quality across PAC settings ‒ Information exchange across PAC settings ‒ Enhanced care transitions and coordinated care ‒ Person-centered and goals-driven care planning and
discharge planning
5
Purposes of the IMPACT Act
• Improve Medicare beneficiary outcomes• Facilitate comparable data and quality across PAC
settings• Support provider access to longitudinal information
to facilitate coordinated care• Develop payment models based on patient
characteristics
6
Providers Covered by the IMPACT Act
• Skilled Nursing Facilities (SNFs) • Home Health Agencies (HHAs) • Inpatient Rehabilitation Facilities (IRFs) • Long-Term Care Hospitals (LTCHs)
7
IMPACT Act Identifies Categories that Require the Use of Standardized Data
• Function (e.g., self care and mobility) • Cognitive function (e.g., express & understand
ideas; mental status, such as depression and dementia)
• Special services, treatments & interventions (e.g., need for ventilator, dialysis, chemotherapy, and total parenteral nutrition)
• Medical conditions and co-morbidities (e.g., diabetes, heart failure, and pressure ulcers)
• Impairments (e.g., incontinence; impaired ability to hear, see, or swallow)
8
IMPACT Act Identifies Domains for Quality Measures that Use Standardized Assessment Data
• Functional status, cognitive function, and changes in function and cognitive function
• Skin integrity and changes in skin integrity • Medication reconciliation • Incidence of major falls • Communicating and providing for the transfer of
health information and care preferences of an individual when the individual transitions
9
Current Assessments
• 4 Different Settings, 4 Different Assessment Tools • Skilled Nursing Facilities (SNF) Minimum Data Set
(MDS) • Home Health Agencies (HHA) Outcome and
Assessment Information Set (OASIS) • Inpatient Rehabilitation Facilities (IRF) IRF-Patient
Assessment Instrument (IRF-PAI) • Long Term Care Hospitals (LTCH) LTCH CARE
Data Set (LCDS) • Overlapping domains and purposes but specific
items measuring common domains differ across settings
10
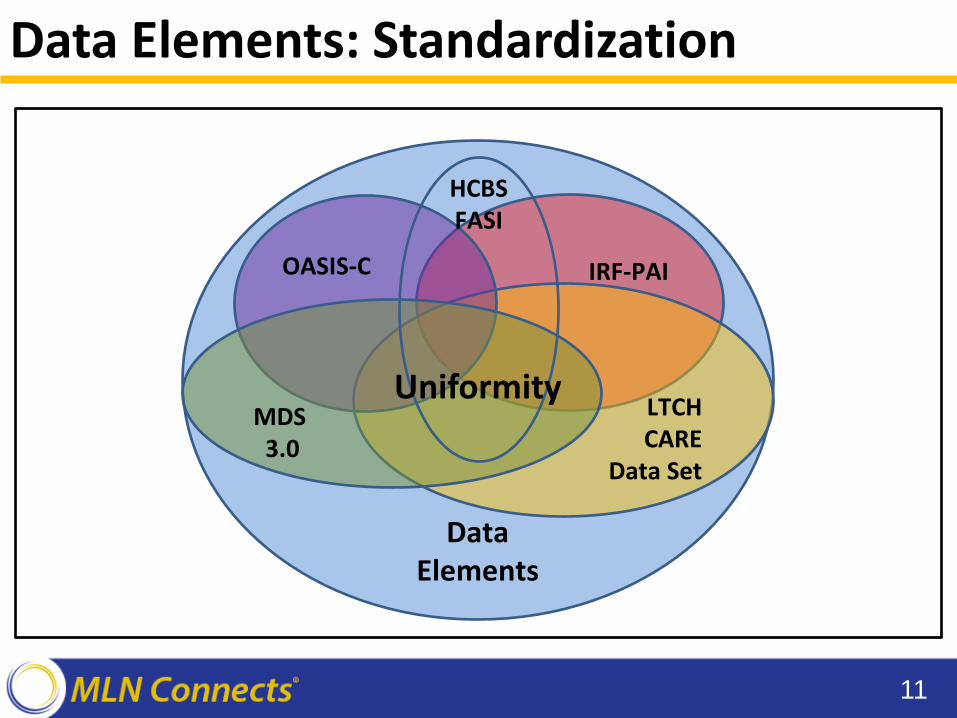
IRF-PAI
LTCH CARE
Data Set
OASIS-C
MDS 3.0
Data Elements
HCBS FASI
Uniformity
Data Elements: Standardization
11
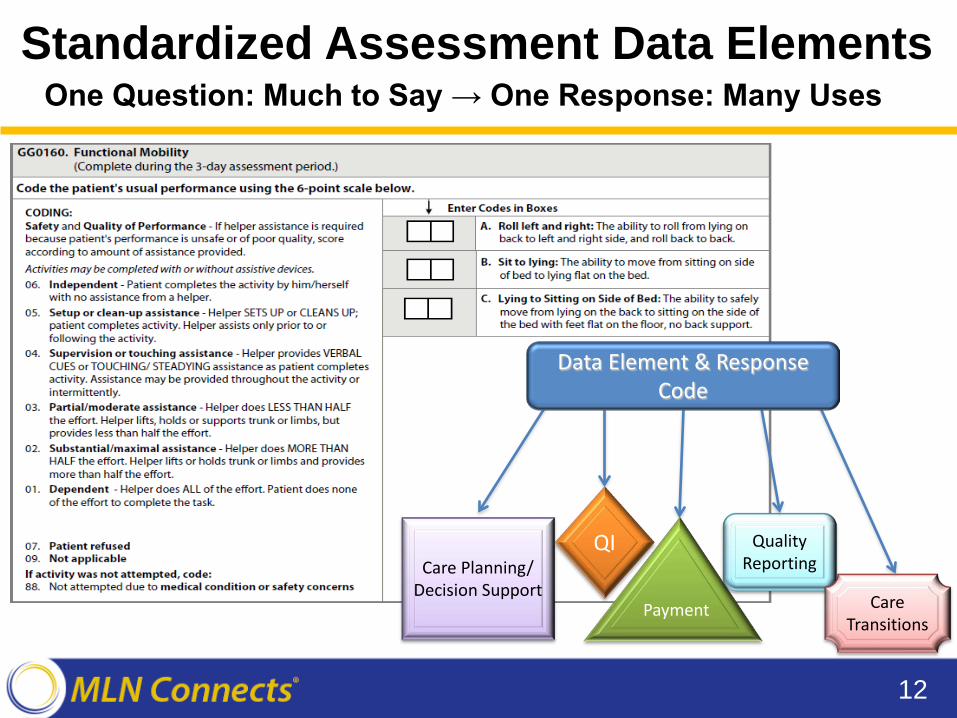
Standardized Assessment Data Elements One Question: Much to Say → One Response: Many Uses
12
Care Planning/ Decision Support
Payment
Quality Reporting
QI
Care Transitions
Data Element & Response Code
Scope of Work and Timelines
Overview of the RAND Contract
• Project goal is to develop, implement, and maintain standardized PAC patient assessment data
• Project phases: 1. Information Gathering: Sep 2015 – Apr 2016 2. Pilot Testing (Alpha 1 and Alpha 2): Aug 2016 –
July 2017 3. National Beta Testing: Begins Fall 2017
• Focus on 6 domains: cognitive status, mental status, medical conditions, impairments, care preferences, medication reconciliation
14
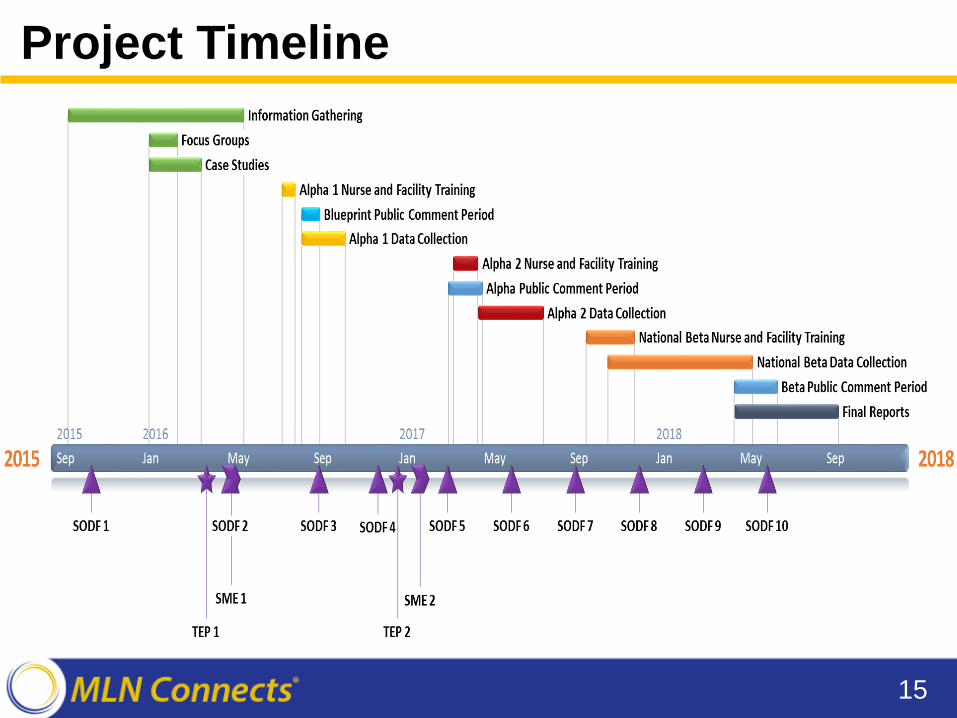
Project Timeline
15
Information Gathering
• Identify candidate data elements for testing• Based on:
‒ Literature review ‒ Focus groups (winter 2016) ‒ Technical Expert Panels (TEPs) (April 2016, Jan. 2017) ‒ Ongoing stakeholder engagement
• Candidate data elements evaluated on:‒ Potential for improving quality ‒ Validity and reliability ‒ Feasibility for use in PAC ‒ Utility for describing case mix
16
Development and Implementation of Data Elements
• Track 1: Blueprint Public Comment Data Elements ‒ Strong evidence for feasibility and reliability in PAC settings ‒ Tested and performed well in PAC PRD ‒ Posted for public comment in August 2016
• Track 2: Alpha 1 Data Elements ‒ Rated highly by the TEP (in April 2016) and stakeholders, but
require feasibility testing in PAC settings ‒ Tested in cross-setting PAC facility field test
• Track 3: Alpha 2 Data Elements ‒ Identified and developed during Summer - Fall 2016 ‒ Rated highly by the TEP (in Jan. 2017) and stakeholders ‒ Will be tested in upcoming cross-setting PAC facility field test
17
Alpha 1 Field Test
Alpha 1 Field Test
• August – October 2016 • 8 facilities in Greater Hartford, Connecticut area
‒ 2 LTCH, 2 IRF, 2 SNF, and 2 HHA providers • 120 admission assessment forms collected
• (~15 per setting) • Debrief interviews with facility staff and research
nurses
19
Alpha 1 Data Elements
• Alpha 1 Data Elements being tested include‒ Medical Conditions – Pain ‒ Impairments – Hearing and Vision ‒ Impairments – Bladder and Bowel Continence ‒ Cognitive Function ‒ Mental Status - Mood ‒ Medication Reconciliation ‒ Care Preferences
20
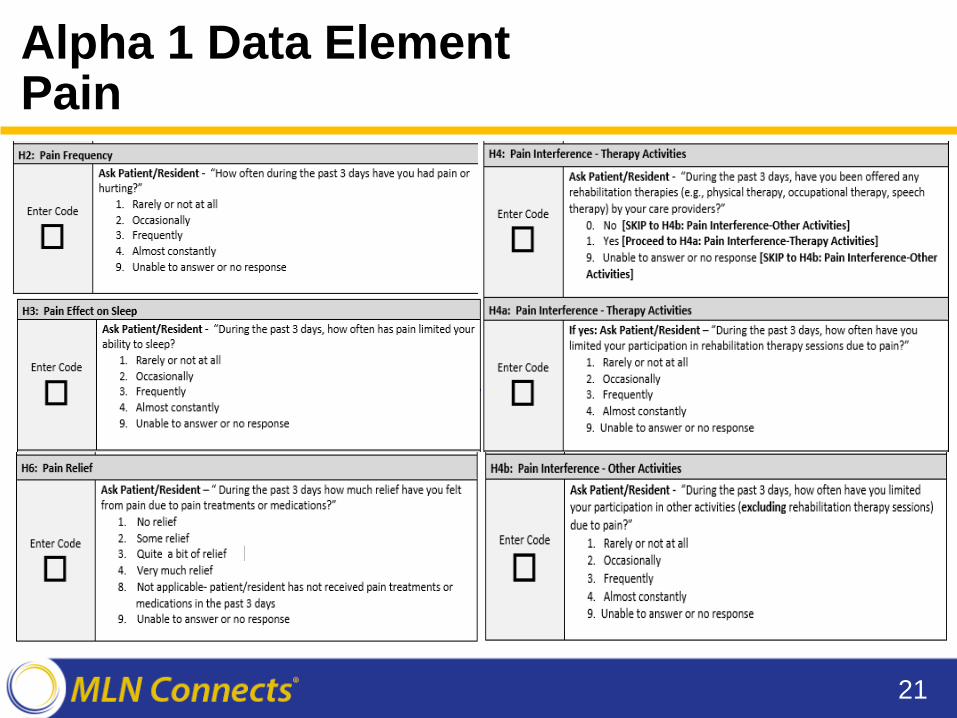
Alpha 1 Data Element Pain
21
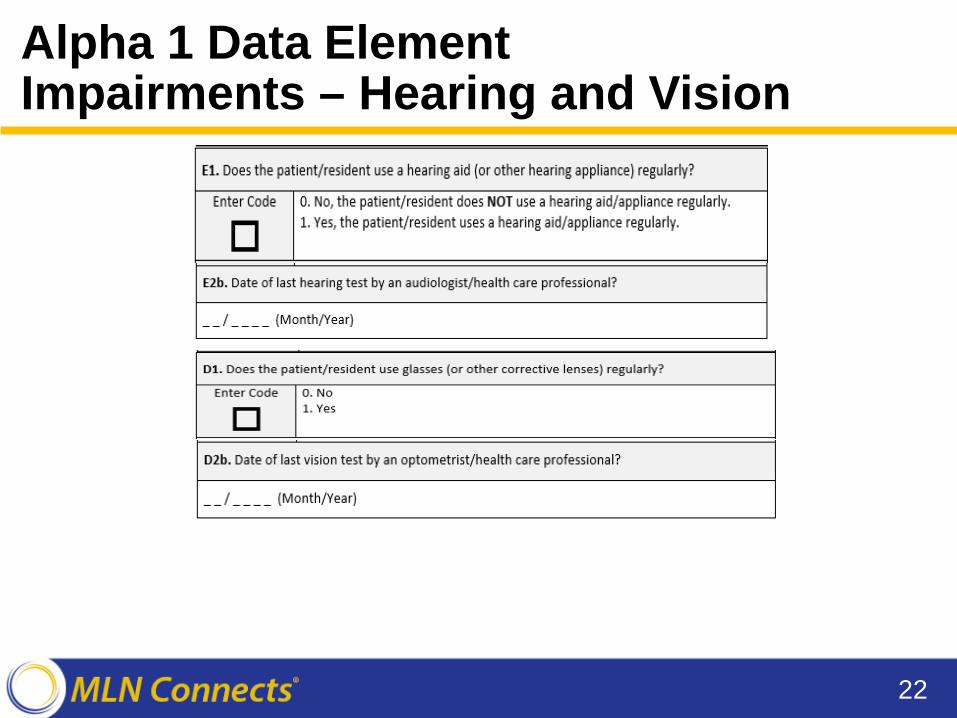
Alpha 1 Data Element Impairments – Hearing and Vision
22
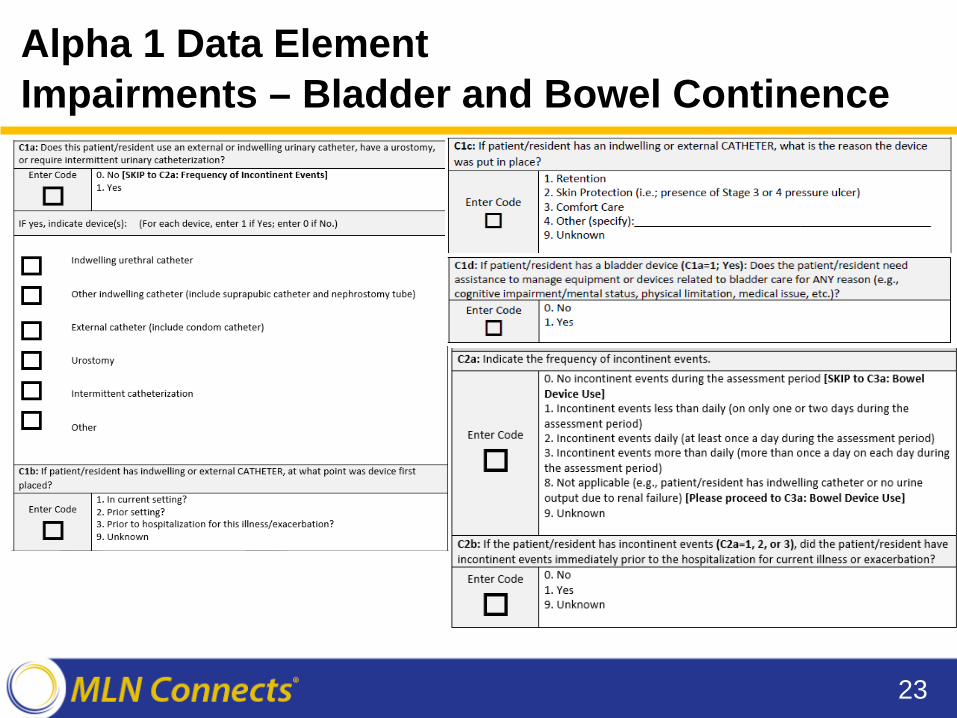
Alpha 1 Data Element Impairments – Bladder and Bowel Continence
23
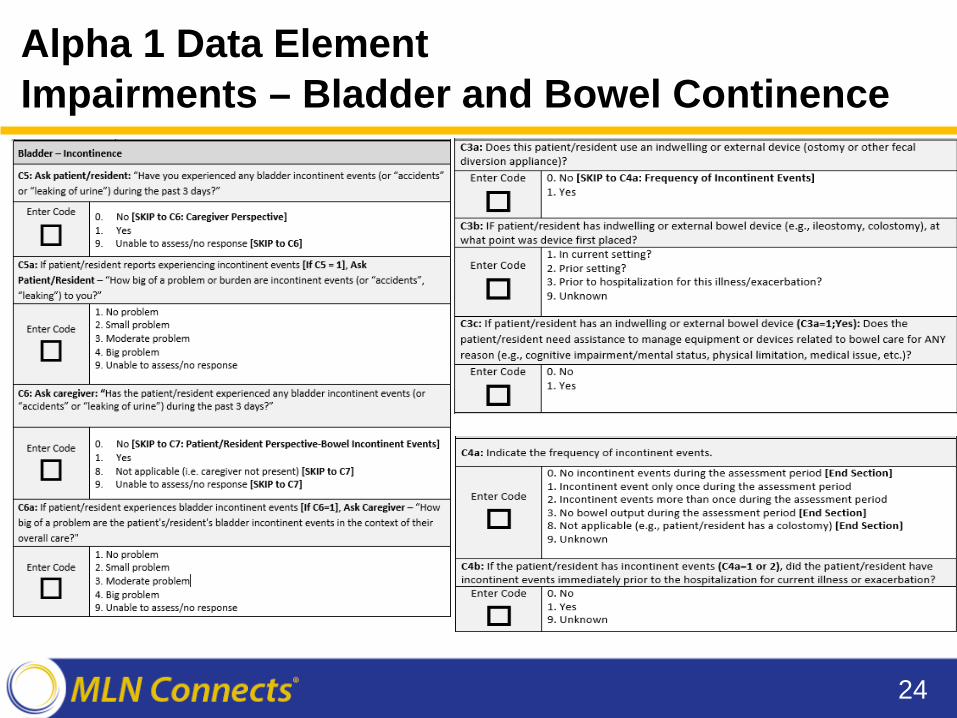
Alpha 1 Data Element Impairments – Bladder and Bowel Continence
24

Alpha 1 Data Element Impairments – Bladder and Bowel Continence
25
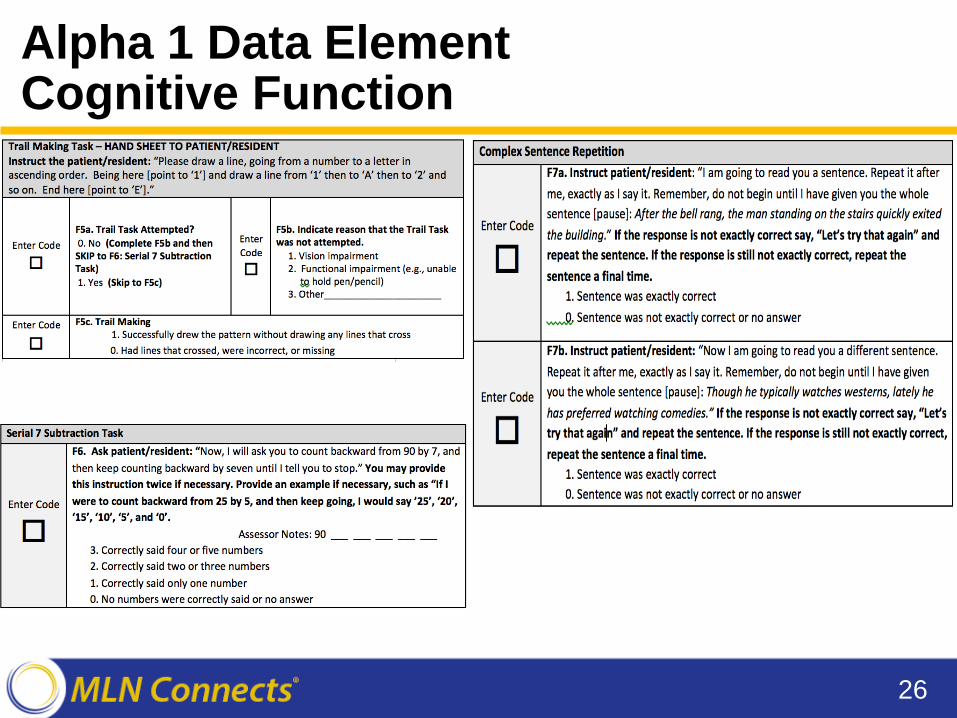
Alpha 1 Data Element Cognitive Function
26
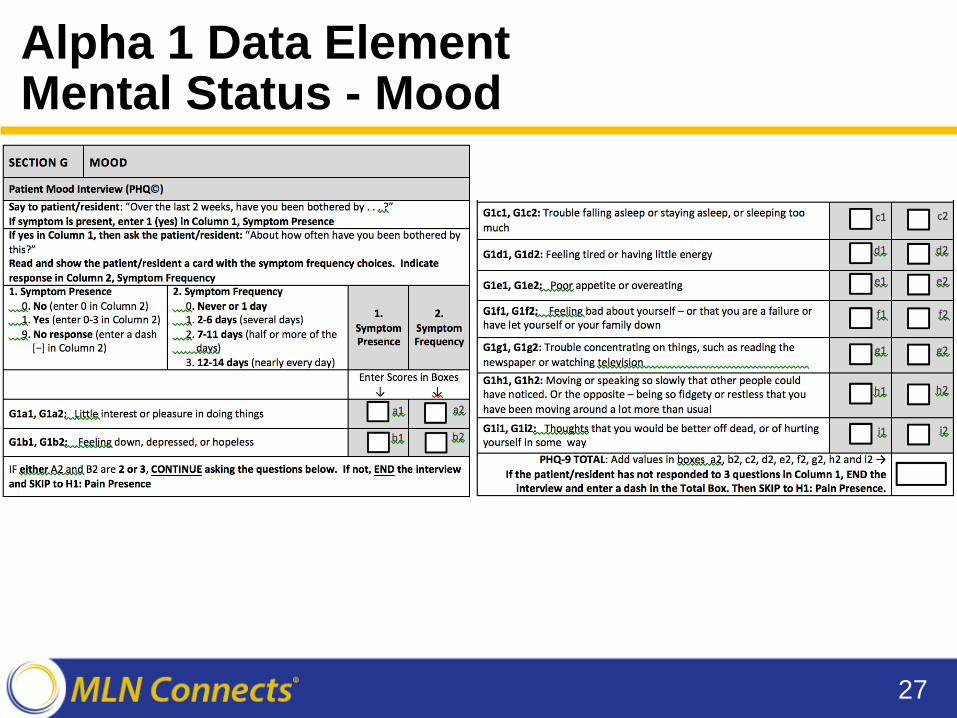
Alpha 1 Data Element Mental Status - Mood
27
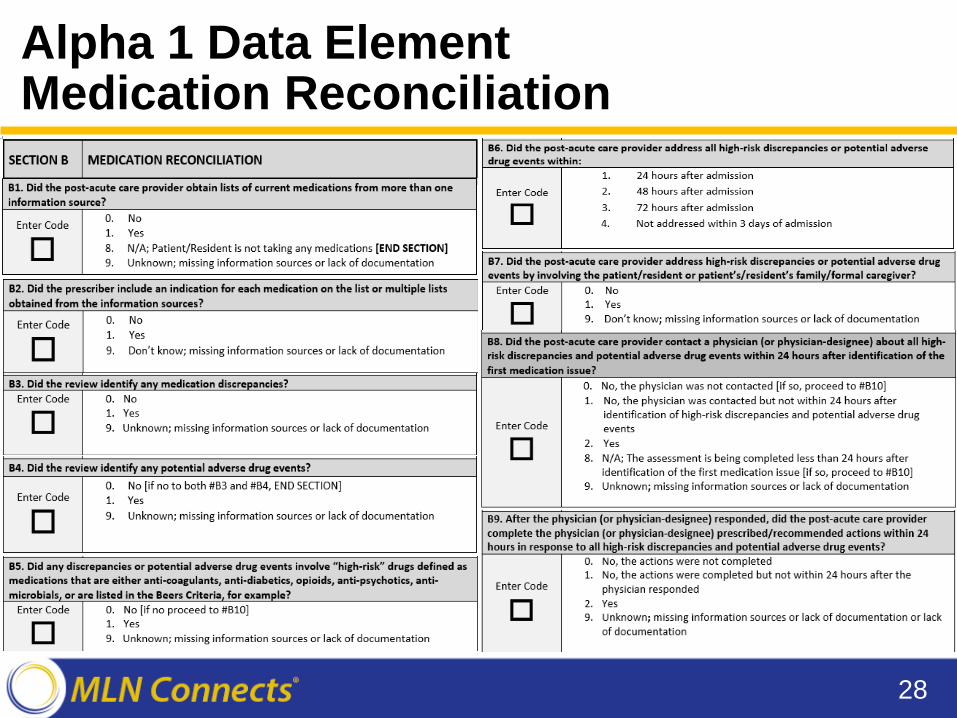
Alpha 1 Data Element Medication Reconciliation
28
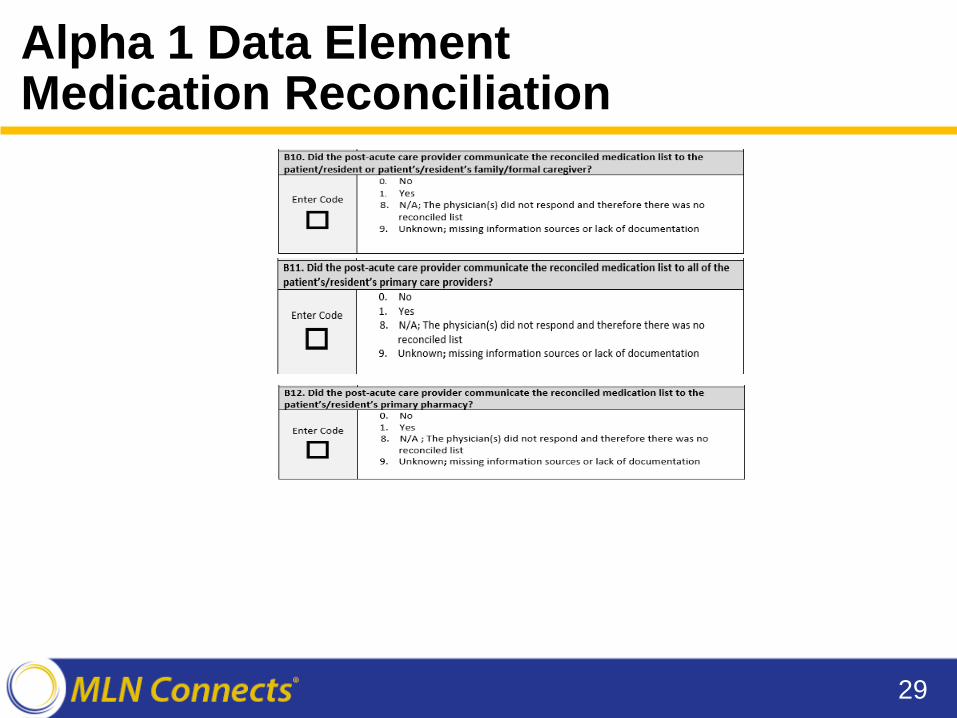
Alpha 1 Data Element Medication Reconciliation
29
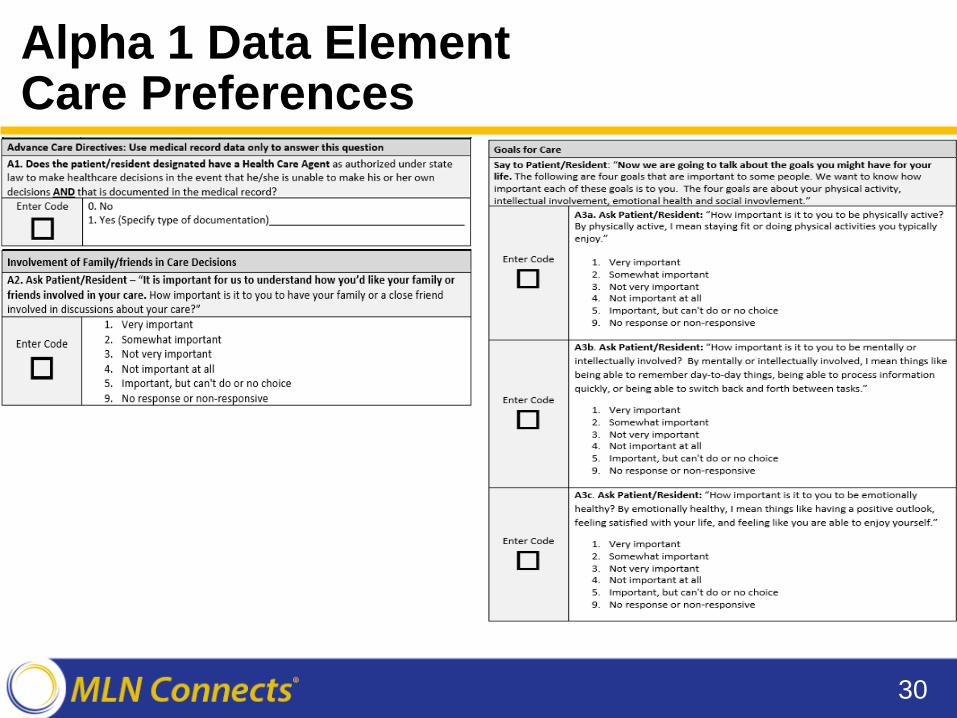
Alpha 1 Data Element Care Preferences
30
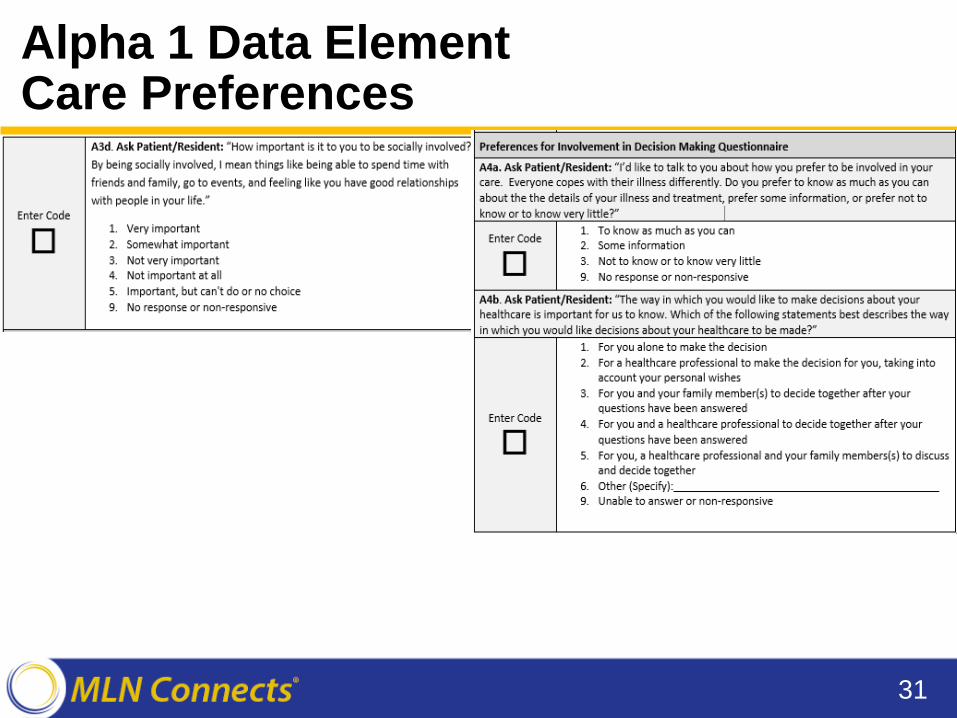
Alpha 1 Data Element Care Preferences
31
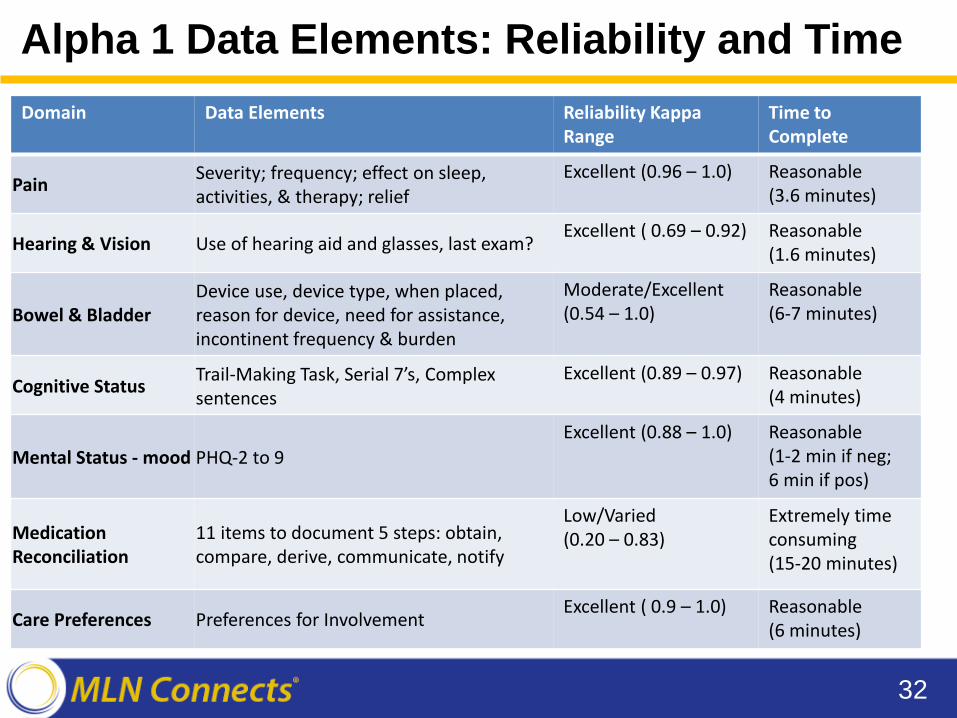
Alpha 1 Data Elements: Reliability and Time
32
Domain Data Elements Reliability Kappa Time to Range Complete
Pain Severity; frequency; effect on sleep, activities, & therapy; relief
Excellent (0.96 – 1.0) Reasonable (3.6 minutes)
Hearing & Vision Use of hearing aid and glasses, last exam? Excellent ( 0.69 – 0.92) Reasonable
(1.6 minutes)
Device use, device type, when placed, Moderate/Excellent Reasonable Bowel & Bladder reason for device, need for assistance, (0.54 – 1.0) (6-7 minutes)
incontinent frequency & burden
Cognitive Status Trail-Making Task, Serial 7’s, Complex sentences
Excellent (0.89 – 0.97) Reasonable (4 minutes)
Excellent (0.88 – 1.0) Reasonable Mental Status - mood PHQ-2 to 9 (1-2 min if neg;
6 min if pos)
Medication Reconciliation
Low/Varied 11 items to document 5 steps: obtain, (0.20 – 0.83) compare, derive, communicate, notify
Extremely time consuming (15-20 minutes)
Care Preferences Preferences for Involvement Excellent ( 0.9 – 1.0) Reasonable
(6 minutes)
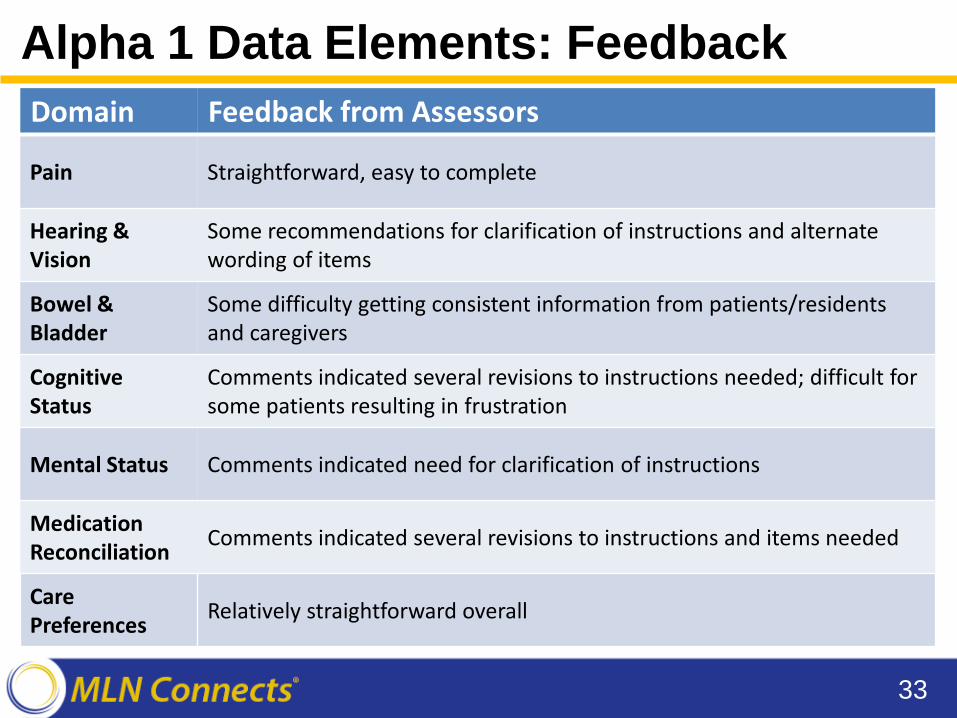
Alpha 1 Data Elements: Feedback
33
Domain Feedback from Assessors
Pain Straightforward, easy to complete
Hearing & Vision
Some recommendations for clarification of instructions and alternate wording of items
Bowel & Bladder
Some difficulty getting consistent information from patients/residents and caregivers
Cognitive Status
Comments indicated several revisions to instructions needed; difficult for some patients resulting in frustration
Mental Status Comments indicated need for clarification of instructions
Medication Reconciliation Comments indicated several revisions to instructions and items needed
Care Preferences Relatively straightforward overall
Alpha 1 Data Elements: Next Steps
• Data elements and instructions are beingrevised per alpha 1 results‒Some data elements may be removed from further
consideration • Revised data elements will be
‒ Posted for public comment on the MMS Public Comment Webpage ‒ Considered for inclusion in beta testing
34

Upcoming Field Tests
Alpha 2 Field Test
• Field test: April – July 2017 • Three US markets:
‒ Houston, Texas ‒ Chicago, Illinois ‒ Denver, Colorado
• 16 facilities: ‒ 4 LTCH, 4 IRF, 4 SNF, and 4 HHA providers ‒ 120 observational assessments ‒ 120 interview admission assessments ‒ 60 interview discharge assessments
36
Alpha 2 Data Elements
• Revised items from Alpha 1 ‒ Medication Reconciliation ‒ Care Preferences
• New items to assess Cognitive Function • Observation items for patients/residents who are
unable to communicate to assess: • Pain • Cognitive Function • Depressed Mood
37
Alpha 2 Analyses
• Feasibility of items will be evaluated based on same criteria used for alpha 1 ‒ Correspondence between research and facility nurse
assessors ‒ Time to complete ‒ Qualitative feedback from assessors
• Report of results will be generated in early fall 2017
• Will hold webinar for provider participants to review results and lessons learned from field test
38
National Beta Test: Oct 2017-May 2018
• Goal is to obtain a national sample that reflects US provider and patient/resident variability
• Data from national test will provide setting-specific reliability and validity data on included items
• Items will be based on alpha 1 and alpha 2 test results and feedback from public comment
39
Beta Design
• National sample will include: ‒ 210 PAC facilities from 14 geographic/metropolitan areas ‒ 28 IRFs, 28 LTCHs, 84 SNFs, and 70 HHAs ‒ An average of 2 IRFs, 2 LTCHs, 6 SNFs, and 5 HHAs per
PAC market • Providers will be randomly selected to participate • Patients/residents will be enrolled upon admission • Design will include admission and discharge
assessments • Subset of patients/residents will be double-assessed
by research and facility staff (as in Alpha test) to evaluate reliability
40
Beta Test Market Areas
• Boston, MA • Chicago, IL • Dallas, TX • Durham, NC • Fort Lauderdale, FL • Harrisburg, PA • Houston, TX
41
14 geographic/metropolitan areas for Beta include:
• Kansas City, MO • Los Angeles, CA • Nashville, TN • Philadelphia, PA • Phoenix, AZ • St. Louis, MO • San Diego, CA
Benefits of Participating
42
• Understand/influence cross-setting PAC assessment items with implications for quality reporting and value-based payment
• Increase staff skills in quality improvement, use of data to improve care, and support professional development/retention for high value employees
• Internal and external publicity to emphasize your commitment to quality and participation in national standard setting/showcase innovation in post-acute care
• National visibility/networking with peer organizations and national stakeholders participating in the testing and rollout
• Research experience to support future grant applications, potential for additional collaboration with national stakeholders and policy-makers, and recruitment of candidates for key staff positions
How to Get Involved
Ongoing Outreach Activities
• Stakeholder meetings • Professional conference participation • Public comment on proposed items
‒ Blueprint ‒ Item list distributions (via email) ‒ Formal public comment
44
Beta Recruitment Activities/ Opportunities
• Mailings to be sent out in late April early May 2017 to invite providers to participate in beta
• Recruitment outreach calls from Abt Associates team members will closely follow mailings
• Providers will need to identify clinical teams to participate as assessors
• Field period runs from October 2017 – May 2018 • Debrief activities will occur in early summer 2018
45
Points of Contact
• CMS IMPACT Mailbox for comments/ideas: ‒ [email protected]
• IMPACT item development general information: ‒ [email protected]
• Field testing and recruitment information: ‒ [email protected]
46
For More Information
• IMPACT Act website • PAC QRP listserv- https://public-
dc2.govdelivery.com/accounts/USCMS/subscriber/new?topic_id=USCMS_12265
47
Evaluate Your Experience
• Please help us continue to improve the MLN Connects® National Provider Call Program by providing your feedback about today’s call.
• To complete the evaluation, visit http://npc.blhtech.com and select the title for today’s call.
48
Thank You
• For more information about the MLN Connects® National Provider Call Program, visit https://www.cms.gov/Outreach-and-Education/Outreach/NPC/National-Provider-Calls-and-Events.html
• For more information about the Medicare Learning Network®, visit https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNGenInfo/Index.html
The Medicare Learning Network® and MLN Connects® are registered trademarks of the U.S. Department of Health and
Human Services (HHS).
49





























