Embed Size (px)
Citation preview
Parasitology International 55 (2006) 233–236www.elsevier.com/locate/parint
Short communication
Impact of single dose of diethylcarbamazine and other antifilarialdrug combinations on bancroftian filarial infection variables:
Assessment after 2 years
I.P. Sunish a,⁎, R. Rajendran a, T.R. Mani a, A. Munirathinam a, R. Reuben b, A.P. Dash c
a Centre for Research in Medical Entomology (Indian Council of Medical Research), 4 Sarojini Street, Chinna Chokkikulam, Madurai-625 002, Tamil Nadu, Indiab 52 Rashmi Apartments, D′Monte Park Road, Bandra, Mumbai-400 050, India
c National Institute of Malaria Research, #22 Sham Nath Marg, Delhi-110 054, India
Received 12 January 2006; received in revised form 12 May 2006; accepted 17 May 2006Available online 27 June 2006
Abstract
The impact of single dose mass drug administration of diethylcarbamazine (DEC), DEC with albendazole (ALB), and ivermectin (IVR) withalbendazole, was examined on the human bancroftian filarial infections in village scale trials in south India, from a follow-up study after 2 years.The treatment arms administered with DEC alone and DEC+ALB demonstrated long-term benefits in reducing microfilaraemia significantly(P<0.05), while antigenaemia reduction was negligible. The arm with ALB+IVR did not show such reductions. Among the antigenaemic andmicrofilaraemic individuals, 87% became amicrofilaraemic in DEC+ALB arm, which were higher than that observed in the other 2 treatmentarms. Among amicrofilaraemics (but Ag+), nearly 35% cleared of infection in DEC+ALB, while 26% and 6% in DEC alone and IVR+ALBarms, respectively. The drug combination DEC+ALB was observed to demonstrate a significant impact in reducing filarial infection even after2 years post treatment.© 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Bancroftian filariasis; Diethylcarbamazine; Ivermectin; Albendazole; Microfilaraemia; Antigenaemia; Mass drug administration; South India
1. Introduction
The revised elimination strategy for lymphatic filariasis (LF)has been launched in many countries, and is designed to blockthe transmission in populations exposed to infection by a singledose of two drugs annually for 5–6 years [1]. Globally, over120 million people have been affected by it; over 40 million ofthem are seriously incapacitated and disfigured by the disease.One third of the people infected with the disease live in India[2]. The global programme for elimination of lymphaticfilariasis (GPELF) has identified the Indian subcontinent asthe region in which the greatest number of people is at riskfrom lymphatic filaraisis: 514 million, 454 million of whom are
⁎ Corresponding author. Tel.: +91 452 2525131x2530746; fax: +91 452530660.
E-mail addresses: [email protected] (I.P. Sunish), [email protected](R. Reuben), [email protected] (A.P. Dash).
1383-5769/$ - see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.parint.2006.05.003
in India alone [3]. In the global effort to eliminate lymphaticfilariasis the major strategy used to interrupt transmission isreducing the reservoir of infection in humans by annual single-dose mass treatment with antifilarial drugs [4]. Several new andeffective combinations and strategies are being proposed forelimination of lymphatic filariasis. Although investigationshave been carried out to bring out the impact of combinationeffect of DEC (diethylcarbamazine), IVR (ivermectin) andALB (albendazole), most of them are hospital-based studies[5,6] and few community trials have been carried with drugcombinations DEC+ALB and IVR+ALB [7,8]. But there areno community trials comparing the effect of DEC alone withDEC+ALB and IVR+ALB, two years after the single dose ofdrug was given. Therefore, the effectiveness of single dose of1) DEC alone 2) a combination of DEC and ALB and 3) acombination of ivermectin and ALB, in reducing filarialinfection after 2 years of treatment, in followed-up humansubjects was carried out in a field setting in south India.

234 I.P. Sunish et al. / Parasitology International 55 (2006) 233–236
2. Materials and methods
Three filariasis endemic villages in Tirukoilur area (latitude:11°57′00″; longitude: 79°12′00″) of Villupuram district,southern India, with a human population of 1026, 2429 and3258, respectively, were chosen for mass drug administration(MDA) in the year 1999. The average age group of the studypopulation was 19.32, 21.03 and 18.62 years in the 3 villages,respectively. Baseline status of microfilaraemia and antigenae-mia were determined prior to this MDA from all the eligiblesubjects [9]. Blood survey was carried out during 21.00–24.00 h by finger prick method. For microfilaraemia 20 μlblood was collected, while 100 μl for determining theantigenaemia status using ICT card test kit (Binax, USA).Treatment strategy administered in each village was (i) DEC(6 mg/kg bodywt), (ii) DEC with ALB (400 mg/person) and(iii) IVR (200 μg/kg bodyweight) with ALB. The MDA wascarried out by door-to-door visit, and more than 95% of theeligible residents were treated (children <2 years, pregnant andlactating women were excluded from MDA). Prior oralconsent was obtained from villagers at the time of drugadministration. Post treatment survey for microfilaraemia (Mf)and antigenaemia was carried out in 10% of the populationcovering equal proportion in all the age groups, after a gap of2 years (i.e., in the year 2001). The procedure of sampling wassimilar in all the 3 drug regimens. In this communication, theanalysis was restricted to those subjects who were screenedduring both the time points (i.e. in 1999 and in 2001). Thus atotal of 121, 193 and 223 subjects were screened in IVR+ALB, DEC+ALB and DEC alone arms, respectively, duringboth the years. This project has been cleared by theinstitutional ethical committee.
Data were analyzed using SPSS software package version11.0. The chi-square test was used to assess the significance ofthe difference in prevalence of microfilaraemia betweentreatment arms, before and after treatment. Geometric meanintensities (GMIs) of microfilaraemia were calculated as antilog[Σ log(x+1)/n]−1, with ‘x’ being the number of Mf/20 μl ofblood and ‘n’ the number of individuals examined, including theMf negative persons.
Table 1Changes in filarial infection status among human subjects after 2 years of single do
Pre treatment infectionstatus during 1999
Treatmentarm
Number ofpersonsfollowed
Infec
Micro(Ag+
Num
Microfilaraemic (Ag+/Mf+) IVR+ALB 26 19DEC+ALB 16 2DEC alone 28 11
Amicrofilaraemic (Ag+/Mf−) IVR+ALB 18 4DEC+ALB 26 1DEC alone 23 2
Negative (Ag−/Mf−) IVR+ALB 77 1DEC+ALB 151 0DEC alone 172 0
a, b—significant difference with respect to other 2 treatment arms separately.
3. Results and discussion
The antigenaemia prevalence (AGP) in the followed-uppopulation was 36.4%, 21.8% and 22.9% during the baselinesurvey in the year 1999, in IVR+ALB, DEC+ALB and DECalone arms, respectively. After 2 years (i.e., during posttreatment period), there was no change in AGP values in anyof the treatment arms. Even though albendazole was suggestedto have an antifilarial effect on the adult filarial worm [10,11],the impact (assessed by the AGP levels) could not bedemonstrated after a gap of 2 years. However, the change ininfection levels in the longitudinally followed-up subjects after2 years of MDAwas analysed to determine the loss and gain ofinfection in the 3 communities with different treatmentstrategies (Table 1). In this community trial, those personswho were negative for Mf were also administered treatment bywhich the loss and gain of infection in the study subjects can beexamined. This was an advantage in a community trial, which isdifficult to infer in a hospital-based approach. The disadvantageis that, the side effects occurring after drug administrationcannot be systematically assessed and quantified as in a hospitalstudy.
The individuals followed up were grouped into 3 categoriesfor the purpose of analysis with respect to the loss and gain ofinfection over a period of 2 years. The 3 categories include (i)Ag+/Mf+, (ii) Ag+/Mf−, (iii) Ag−/Mf−. In IVR+ALB, theinfection status in >70% of individuals did not change in the 3categories, while in the other two arms, there was greater clea-rance of infection. Under normal circumstances, the prevalencereduction is likely to be greater in areas with high prevalence andintensity. It is difficult to reduce infection levels in areas, whichare already at a low level. Therefore, in the present study, theinfection in IVR+ALB is the highest and the reduction wasexpected to be more in this village than in the other 2 villageswhere the pre-treatment prevalences are lower. Of the indivi-duals who were found microfilaraemic in 1999 (Ag+/Mf+),87.6% and 60.7% became amicrofilaraemic in DEC+ALB andDEC alone arms, respectively during 2001 survey. In the armadministered with IVR+ALB, only 26.9% became amicrofilar-aemic (including those cleared of antigenaemia). The percentage
se MDA
tion status after 2 years in 2001
filaraemic/Mf+)
Amicrofilaraemic(Ag+/Mf−)
Negative (Ag−/Mf−)
ber % Number % Number %
73.1 6 23.1 1 3.812.5 13 81.3a 1 6.339.3 16 57.1 1 3.622.2 13 72.2 1 5.63.8 16 61.5 9 34.6b
8.7 15 65.2 6 26.11.3 8 10.4 68 88.30.0 10 6.6 141 93.40.0 12 7.0 160 93.0
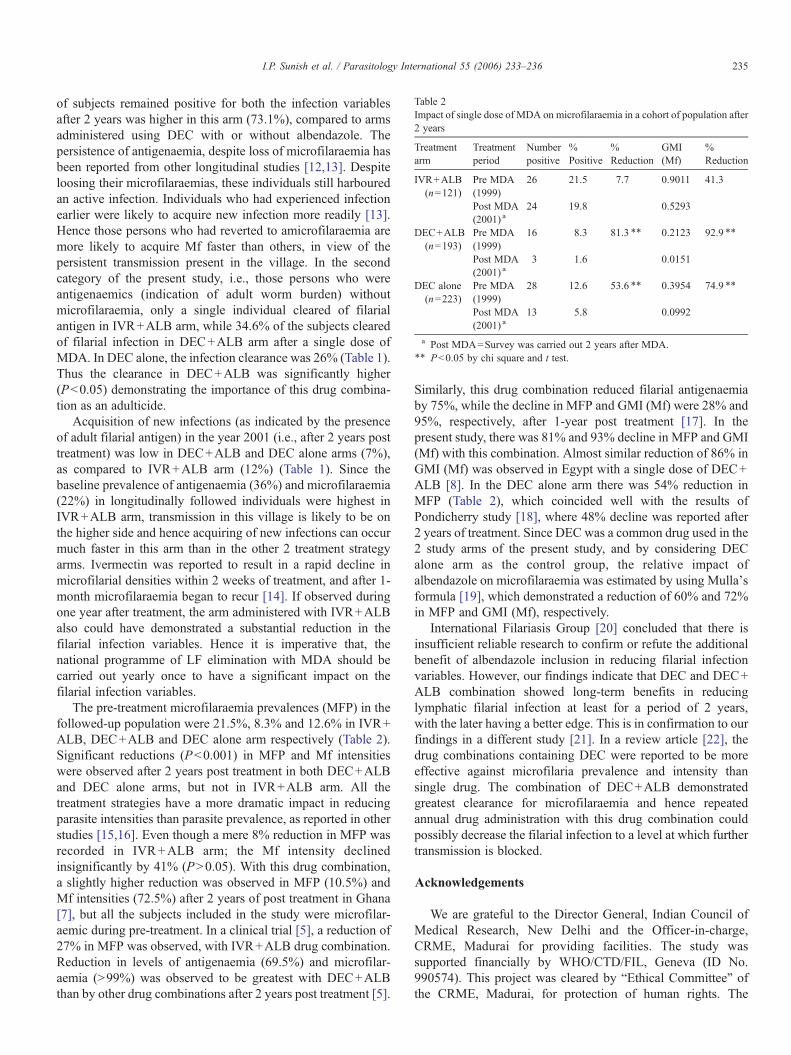
Table 2Impact of single dose of MDA on microfilaraemia in a cohort of population after2 years
Treatmentarm
Treatmentperiod
Numberpositive
%Positive
%Reduction
GMI(Mf)
%Reduction
IVR+ALB(n=121)
Pre MDA(1999)
26 21.5 7.7 0.9011 41.3
Post MDA(2001) a
24 19.8 0.5293
DEC+ALB(n=193)
Pre MDA(1999)
16 8.3 81.3 ⁎⁎ 0.2123 92.9 ⁎⁎
Post MDA(2001) a
3 1.6 0.0151
DEC alone(n=223)
Pre MDA(1999)
28 12.6 53.6 ⁎⁎ 0.3954 74.9 ⁎⁎
Post MDA(2001) a
13 5.8 0.0992
a Post MDA=Survey was carried out 2 years after MDA.⁎⁎ P<0.05 by chi square and t test.
235I.P. Sunish et al. / Parasitology International 55 (2006) 233–236
of subjects remained positive for both the infection variablesafter 2 years was higher in this arm (73.1%), compared to armsadministered using DEC with or without albendazole. Thepersistence of antigenaemia, despite loss of microfilaraemia hasbeen reported from other longitudinal studies [12,13]. Despiteloosing their microfilaraemias, these individuals still harbouredan active infection. Individuals who had experienced infectionearlier were likely to acquire new infection more readily [13].Hence those persons who had reverted to amicrofilaraemia aremore likely to acquire Mf faster than others, in view of thepersistent transmission present in the village. In the secondcategory of the present study, i.e., those persons who wereantigenaemics (indication of adult worm burden) withoutmicrofilaraemia, only a single individual cleared of filarialantigen in IVR+ALB arm, while 34.6% of the subjects clearedof filarial infection in DEC+ALB arm after a single dose ofMDA. In DEC alone, the infection clearance was 26% (Table 1).Thus the clearance in DEC+ALB was significantly higher(P<0.05) demonstrating the importance of this drug combina-tion as an adulticide.
Acquisition of new infections (as indicated by the presenceof adult filarial antigen) in the year 2001 (i.e., after 2 years posttreatment) was low in DEC+ALB and DEC alone arms (7%),as compared to IVR+ALB arm (12%) (Table 1). Since thebaseline prevalence of antigenaemia (36%) and microfilaraemia(22%) in longitudinally followed individuals were highest inIVR+ALB arm, transmission in this village is likely to be onthe higher side and hence acquiring of new infections can occurmuch faster in this arm than in the other 2 treatment strategyarms. Ivermectin was reported to result in a rapid decline inmicrofilarial densities within 2 weeks of treatment, and after 1-month microfilaraemia began to recur [14]. If observed duringone year after treatment, the arm administered with IVR+ALBalso could have demonstrated a substantial reduction in thefilarial infection variables. Hence it is imperative that, thenational programme of LF elimination with MDA should becarried out yearly once to have a significant impact on thefilarial infection variables.
The pre-treatment microfilaraemia prevalences (MFP) in thefollowed-up population were 21.5%, 8.3% and 12.6% in IVR+ALB, DEC+ALB and DEC alone arm respectively (Table 2).Significant reductions (P<0.001) in MFP and Mf intensitieswere observed after 2 years post treatment in both DEC+ALBand DEC alone arms, but not in IVR+ALB arm. All thetreatment strategies have a more dramatic impact in reducingparasite intensities than parasite prevalence, as reported in otherstudies [15,16]. Even though a mere 8% reduction in MFP wasrecorded in IVR+ALB arm; the Mf intensity declinedinsignificantly by 41% (P>0.05). With this drug combination,a slightly higher reduction was observed in MFP (10.5%) andMf intensities (72.5%) after 2 years of post treatment in Ghana[7], but all the subjects included in the study were microfilar-aemic during pre-treatment. In a clinical trial [5], a reduction of27% in MFP was observed, with IVR+ALB drug combination.Reduction in levels of antigenaemia (69.5%) and microfilar-aemia (>99%) was observed to be greatest with DEC+ALBthan by other drug combinations after 2 years post treatment [5].
Similarly, this drug combination reduced filarial antigenaemiaby 75%, while the decline in MFP and GMI (Mf) were 28% and95%, respectively, after 1-year post treatment [17]. In thepresent study, there was 81% and 93% decline in MFP and GMI(Mf) with this combination. Almost similar reduction of 86% inGMI (Mf) was observed in Egypt with a single dose of DEC+ALB [8]. In the DEC alone arm there was 54% reduction inMFP (Table 2), which coincided well with the results ofPondicherry study [18], where 48% decline was reported after2 years of treatment. Since DEC was a common drug used in the2 study arms of the present study, and by considering DECalone arm as the control group, the relative impact ofalbendazole on microfilaraemia was estimated by using Mulla'sformula [19], which demonstrated a reduction of 60% and 72%in MFP and GMI (Mf), respectively.
International Filariasis Group [20] concluded that there isinsufficient reliable research to confirm or refute the additionalbenefit of albendazole inclusion in reducing filarial infectionvariables. However, our findings indicate that DEC and DEC+ALB combination showed long-term benefits in reducinglymphatic filarial infection at least for a period of 2 years,with the later having a better edge. This is in confirmation to ourfindings in a different study [21]. In a review article [22], thedrug combinations containing DEC were reported to be moreeffective against microfilaria prevalence and intensity thansingle drug. The combination of DEC+ALB demonstratedgreatest clearance for microfilaraemia and hence repeatedannual drug administration with this drug combination couldpossibly decrease the filarial infection to a level at which furthertransmission is blocked.
Acknowledgements
We are grateful to the Director General, Indian Council ofMedical Research, New Delhi and the Officer-in-charge,CRME, Madurai for providing facilities. The study wassupported financially by WHO/CTD/FIL, Geneva (ID No.990574). This project was cleared by “Ethical Committee” ofthe CRME, Madurai, for protection of human rights. The

236 I.P. Sunish et al. / Parasitology International 55 (2006) 233–236
authors wish to express their thanks to the staff of Department ofPublic Health and Preventive Medicine, Tamil Nadu for theirkind cooperation by providing assistance during the field work.We thank all the field staff of Tirukoilur for their excellenttechnical assistance, and also Dr. M.S. Elango for his clinicalexpertise during the MDA programme. Shri A. Venkatesh,CRME, Madurai is acknowledged in the preparation of thismanuscript, particularly in DTP work.
Conflicts of interest statementThe authors have no conflicts of interest concerning the work
reported in this paper.
References
[1] Ottesen EA, Weil GJ. Towards a strategic plan for research to support theglobal programme to eliminate lymphatic filariasis. Am J Trop Med Hyg2004;71:1–2.
[2] WHO. Fact sheet on lymphatic filariasis. Geneva: World HealthOrganization; 2000. No. 102.
[3] World Health Organization. Global programme to eliminate lymphaticfilariasis. Wkly Epidemiol Rec 2005;80:202–12.
[4] Ottesen EA, Duke BOL, Karam M, Behbehani K. Strategies and tools forthe control/elimination of lymphatic filariasis. Bull World Health Org1997;75:491–503.
[5] Ismail MM, Jayakody RL, Weil GJ, Nirmalan N, Jayasinghe KS,Abeyewickrema W, et al. Efficacy of single dose combinations ofalbendazole, ivermectin and diethylcarbamazine for the treatment ofbancroftian filariasis. Trans R Soc Trop Med Hyg 1998;92:94–7.
[6] Ismail MM, Jayakody RL, Weil GJ, Deepika Fernando, De Silva MSG, DeSilva Gac. Long-term efficacy of single-dose combinations of albendazole,ivermectin and diethylcarbamazine for the treatment of bancroftianfilariasis. Trans R Soc Trop Med Hyg 2001;95:332–5.
[7] Dunyo SK, Simonsen PE. Ivermectin and albendazole alone and incombination for the treatment of lymphatic filariasis in Ghana: follow-upafter re-treatment with the combination. Trans R Soc Trop Med Hyg2002;96:189–92.
[8] El SetouthyM, Ramzy RM, Ahmed ES, Kandil AM, Hussain O, Farid HA,et al. A randomized clinical trial comparing single and multi-dosecombination therapy with diethylcarbamazine and albendazole fortreatment of bancroftian filariasis. Am J Trop Med Hyg 2004;70:191–6.
[9] Sunish IP, Rajendran R, Satyanarayana K, Munirathinam A, Gajanana A.Immunochromatographic test (ICT) for estimation of true prevalence ofbancroftian filariasis in an endemic area in southern India. Trans R SocTrop Med Hyg 2001;95:605–7.
[10] Ottesen EA, Ismail MM, Horton J. The role of albendazole in programmesto eliminate lymphatic filariasis. Parasitol Today 1999;15:382–6.
[11] Gyapong JO, Kumaraswami V, Biswas G, Ottesen EA. Treatmentstrategies underpinning the global programme to eliminate lymphaticfilariasis. Expert Opin Pharmacother 2005;6:179–200.
[12] Beuria MK, Bal MS, Mandal NN, Das MK. Antigenaemia at 10 years afterdiethylcarbamazine treatment of asymptomatic microfilaraemic indivi-duals: marginal conversion to infection-free state. Parasite Immunol2002;24:109–11.
[13] Meyrowitsch DW, Simonsen PE, Magesa SM. Long-term effect of threedifferent strategies for mass diethylcarbamazine administration inbancroftian filariasis: follow-up at 10 years after treatment. Trans R SocTrop Med Hyg 2004;98:627–34.
[14] Brown KR, Ricci FM, Ottesen EA. Ivermectin: effectiveness in lymphaticfilariasis. Parasitology 2000:S133–46.
[15] Bockarie MJ, Alexander ND, Hyun P, Dimber Z, Bockarie F, Ibam E, et al.Randomized community-based trial of annual single-dose diethylcarbam-azine with or without ivermectin againstWuchereria bancrofti infection inhuman beings and mosquitoes. Lancet 1998;351:162–8.
[16] Das PK, Ramaiah KD, Vanamail P, Pani SP, Yuvaraj J, Balarajan K, et al.Placebo-controlled community trial of four cycles of single-dosediethylcarbamazine or ivermectin against Wuchereria bancrofti infectionand transmission in India. Trans R Soc Trop Med Hyg 2001;95:336–41.
[17] Pani S, Subramanyam Reddy G, Das L, Vanamail P, Hoti S, Ramesh J, etal. Tolerability and efficacy of single dose albendazole, diethylcarbama-zine citrate (DEC) or co-administration of albendazole with DEC in theclearance of Wuchereria bancrofti in asymptomatic microfilaraemicvolunteers in Pondicherry, South India: a hospital based study. Fil J2002;1:1.
[18] Subramanyam Reddy G, Vengatesvarolu N, Das PK, Vanamail P, VijayanAP, Kala S, et al. Tolerability and efficacy of single dose diethylcarbam-azine (DEC) or ivermectin in the clearance of Wuchereria bancroftimicrofilaraemia in Pondicherry, south India. Trop Med Int Health 2000;5:779–85.
[19] Mulla MS, Norland RL, Fanara DM, Darwazeh HA, Mokean DW. Controlof chironomid midges in recreational lakes. J Econ Entomol 1971;264:300–7.
[20] International Filariasis Review Group. Albendazole for lymphaticFilariasis. (Cochrane Review). Cochrane Library, vol. 1. Chichester, UK:John Wiley & Sons, Ltd.; 2004.
[21] Rajendran R, Sunish IP, Mani TR, Munirathinam A, Abdullah SMd,Arunachalam N, et al. Impact of two annual single-dose mass drugadministrations with diethylcarbamazine alone or in combination withalbendazole onWuchereria bancrofti microfilaraemia and antigenaemia inSouth India. Trans R Soc Trop Med Hyg 2004;98:174–81.
[22] Tisch DJ, Michael E, Kazura JW. Mass chemotherapy options to controllymphatic filariasis: a systematic review. Lancet Inf Dis 2005;5:514–23.





























