Embed Size (px)
Citation preview

Implementation and Interpretation of Respiratory Sinus ArrhythmiaMeasures in Psychosomatic Medicine: Practice Against Better Evidence?THOMAS RITZ, PHD, AND BERNHARD DAHME, PHD
Respiratory sinus arrhythmia (RSA) or high-frequency heart rate variability has been widely used as a noninvasive measure of cardiacvagal tone. However, their dependency on both respiration rate and tidal volume is largely ignored. Only a minority of studies publishedin Psychosomatic Medicine in recent years has implemented precautions for controlling respiration rate in RSA measures, and tidalvolume effects were only rarely addressed. We discuss methodologic issues related to respiratory control methods and present data thatdemonstrate that both respiration rate and tidal volume contribute substantially to the within-individual RSA variance under conditionsof variable breathing, with tidal volume contributing up to one third beyond respiration rate. Finally, we outline a respiratory controlmethod for the time-domain index of RSA and review research pertaining to its reliability, validity, and experimental application. Keywords: respiratory sinus arrhythmia, heart rate variability, respiration, vagal tone.
HRV � heart rate variability; pCO2 � partial pressure of carbondioxide; RSA � respiratory sinus arrhythmia; RR � respiration rate;TTOT � total respiratory cycle time; VT � tidal volume.
INTRODUCTION
The phenomenon of respiratory sinus arrhythmia (RSA) isknown as fluctuations of heart rate associated with breath-
ing, with heart rate acceleration during inspiration and heartrate deceleration during expiration (1,2). RSA can be quanti-fied in the time-domain, where the amplitude of heart ratefluctuations related to each breathing cycle is extracted (e.g.,the difference between the fastest heart rate during inspirationand the slowest heart rate during expiration, known as thepeak-valley method) (3). Alternatively, variability of heart ratecan be broken down into its frequency components by meth-ods such as spectral analysis, where the spectral power at thefrequency of breathing can be extracted as a measure of RSA.Influences on vagal efferent nerve traffic from both the centralrespiratory rhythm generator and peripheral afferents from thelungs are thought to be the main contributors to this phenom-enon (for reviews see, 1,2,4). RSA, or heart rate variability(HRV) at the frequency of breathing, has been linked tocardiac vagal tone in studies using autonomic blockade (5–7).1
Thus, these indices may offer a convenient noninvasive win-dow into the vagal control of cardiac activity. In particular,indices of HRV power spectra have become widely used inbasic studies of autonomic regulatory processes and in clinicalresearch on cardiovascular disease and autonomic neuropathy(2,8,9).
However, there is also ample evidence that respiration rate(RR) and tidal volume (VT) have a profound influence onRSA, and this influence is independent from actual changes incardiac vagal outflow (10–15). Within the range of normalbreathing (approximately 6–30 breaths/min) faster RR and
lower VT lead to reductions in RSA in an approximately linearfashion. Up to the early 1990s, studies in cardiovascularphysiology and psychophysiology have discussed such influ-ences and their implications for interpretation of RSA atlength (11,13,16,17). This evidence has also been acknowl-edged in guidelines on the analysis and interpretation of RSAin 1997 (1). More recently, arguments for a control of respi-ratory parameters in RSA studies have been reiterated in detailby Grossman and Taylor (18). However, research in psycho-somatic medicine has largely lagged behind these develop-ments. An earlier editorial on RSA has focused on othermethodologic issues such as stationarity of heart rate andpsychometric properties of HRV (19). The present article willmainly deal with issues of respiratory control. In the follow-ing, we will briefly review attempts to control for respiratoryinfluences on RSA in studies published in PsychosomaticMedicine since 1994, which followed the peak of the meth-odologic discussion in the early 1990s.
Respiratory Control in RSA Studies in PsychosomaticMedicine, 1994 to 2004
A total of 39 studies (75–113) that included measures ofRSA have been published in Psychosomatic Medicine from1994 to 2004 (approximately 3.5 per year). In the same timeperiod, 171 studies were published that included heart rate(approximately 15.5 per year), and 54 studies that includedmeasures of the respiratory system (approximately 5 per year).Main topics of the RSA studies were cardiovascular psycho-physiology/disease (10 studies), psychopathology (eight stud-ies), general autonomic/immune/endocrine psychophysiology(five studies), gastrointestinal disease (four studies), relax-ation/breathing/biofeedback intervention (four studies), respi-ratory disease (two studies), menstruation (two studies), sleep(two studies), fitness (one study), and multiple chemical sen-sitivity (one study). RSA was more frequently quantified byhigh-frequency HRV (30 studies) than with time-domain mea-sures such as SD, mean square of successive differences, orthe peak-valley index (14 studies; some studies included bothmeasures). Frequency ranges for the high frequency HRVanalysis varied across studies, with 0.12 to 0.18 Hz for thelower limit and 0.35 to 0.50 Hz as the upper limit.
Almost half of the studies ignored respiratory influences onRSA completely (Table 1). Authors typically did not reflect ona lack of respiratory control as a potential limitation in dis-cussion of their data. If control for respiration was attempted,
1In the following, we use the term RSA as an overall term including thetime-domain measures of RSA, as well as the frequency domain measure ofhigh-frequency HRV.
From the Department of Psychology, Southern Methodist University, Dal-las, Texas (T.R.); Department of Psychology, University of Hamburg, Ham-burg, Germany (B.D.).
Address correspondence and reprint requests to Thomas Ritz, PhD, De-partment of Psychology, Southern Methodist University, 6424 Hilltop Lane,Dallas, TX 75205. E-mail: [email protected]
Received for publication June 27, 2005; revision received March 30, 2006.Work on this manuscript was partly supported by the Deutsche Forschungs-
gemeinschaft (DFG Ri 957/3-1).DOI: 10.1097/01.psy.0000228010.96408.ed
617Psychosomatic Medicine 68:617–627 (2006)0033-3174/06/6804-0617Copyright © 2006 by the American Psychosomatic Society

it was mostly restricted to RR. Often, measures were takenfrom one strain gauge (positioned over the thorax, abdomen,or between both), in some cases also extracted from theimpedance cardiography signal or estimated from the heartperiod time series. Four more studies used uncalibrated tho-racic and abdominal bands or attempted to estimate volumefrom the amplitude of a single respiratory band, both of whichdo not allow a valid determination of VT. A number of studiesalso paced respiration throughout some or all measurementintervals, using pacing frequencies similar to normal breathing(12–15 breaths/min) or a wider frequency range (6–30breaths/min), if pacing was central to the aims of the experi-mental intervention (breathing relaxation, hyperventilationtesting). Other strategies were reporting of RR group meansand interpreting changes concomitant with RSA changes, orpartialling out variance of RR from RSA measures by use ofanalysis of covariance. Both RR and VT were measured in avalid way in four studies, and only one used this informationfor a within-individual correction of RSA.
Control of Respiratory Influences on RSA
Lack of control of respiratory influences on RSA canrender results of a study ambiguous and uninformative withrespect to a potential vagal origin of the observed effects. Forexample, one study sought to explore vagal tone in patientswith panic disorder, social phobia, and controls during hypo-,normo-, and hyperventilation using paced breathing trials at 6,12, and 20 breaths/min (75). The findings were similar in allthree groups and perfectly reflected the known influences ofRR on RSA: the participants, who breathed at a baseline rateof approximately 14 to 16 breaths/min, increased their uncor-rected RSA when slowing down to 12 breaths/min and evenfurther (to almost double the size) at 6 breaths/min; when
breathing faster at 20 breaths/min, their uncorrected RSAmarkedly dropped. Before and after these paced breathingtrials, RSA remained on a relatively constant level. The ob-served increases and decreases in RSA were interpreted by theauthors as augmentations or attenuations of vagal tone, re-spectively. However, given a substantial literature demonstrat-ing effects of RR and VT, an interpretation of these findings interms of changes in vagal tone is clearly not warranted.
A variety of strategies has been devised to account forportions of RSA variance due to changes in respiration. Theiraim is to arrive at a “purer” measure of vagal tone changes,which implies that respiratory changes are not linked to vagaltone changes. However, correction for respiration could, undercertain conditions, also remove variance due to “true” changesin vagal output. Under these conditions, respiratory correctionprocedures yield conservative estimates of vagal changes.
In the following, we will discuss issues central to therespiratory correction of RSA that have surfaced in our reviewof publications in Psychosomatic Medicine. Specifically, wewill discuss the following questions: a) Should control forrespiratory parameters be implemented between or withinindividuals? b) Should control procedures address RR, VT, orboth? c) Is paced breathing is a valid strategy for respiratorycontrol? d) Which instrumentation is required for a validcontrol of respiratory parameters? And e) does the comparisonof RSA with or without respiratory control produce valuableinformation regarding individual differences in vagal tone?We will also present data to estimate the relative importanceof RR and VT influences on RSA under controlled conditions.Finally, we will present the rationale and method of a controlprocedure for respiratory influences on RSA. A more detaileddiscussion of other respiratory control procedures is presentedby Grossman and Taylor (18).
Between—Versus Within—Individual Control
It is sometimes assumed that a lack of changes in RR andVT on the group level implies that measurements of RSA arenot influenced by respiration. This argument may hold underconditions in which very little interindividual variation can beexpected in respiratory variables. However, if individuals varyin their respiratory adjustments across situations and thesevariations are cancelled out in the mean of respiratory vari-ables, it cannot be excluded that any observed RSA changesare actually due to these inconspicuous respiratory variations.This is due to a considerable interindividual variation in theextent to which RR modulates RSA (e.g., 14,20). While someindividuals show massive increase in RSA when e.g., chang-ing their total respiratory cycle duration (TTOT) from 4 s to 6 s(RR of 15 to 10 breaths/min), others may only show smallthough reliable increases. If a within-regression analysis ofRSA on TTOT would be calculated across a representativerange of RRs for both individuals, the former individual wouldshow a very steep and the latter a much shallower positiveslope.
We can illustrate the possible consequences on a measureof vagal tone in an extreme example based on typical empir-
TABLE 1. Measurement and Control of Respiration in RSA StudiesPublished in Psychosomatic Medicine, 1994 to 2004
Total number of RSA studies 39No control of respiration, no discussion of limitations 19No control of respiration, discussion of limitations 2Paced breathing during measurements 7Measurement of respiration rate only 20Attempt to control for respiration rate 14
Control of respiration rate by paced breathing 5Analysis of concomitant respiration rate 7Adjustment for respiration rate by covariance
analysis3
Adjustments for respiration rate within individuals 1Measurement of respiration rate and tidal volume 4Attempt to control for both respiration rate and tidal
volume2
Control of respiration rate and tidal volume bypaced breathing
0
Analysis of concomitant respiration rate and tidalvolume
2
Adjustments for respiration rate and tidal volumeby covariance analysis
0
Adjustments for respiration rate and tidal volumewithin individuals
1
T. RITZ AND B. DAHME
618 Psychosomatic Medicine 68:617–627 (2006)

ically determined within-individual regression equations oftwo individuals (see also 20). Assume that individual A has arather steep slope of RSA/VT on TTOT, with y � �70 � x �60, and individual B has a shallower slope, with y � �50 �x � 20; in this example we use RSA normalized for VT (seebelow under A Method to Control . . .), which shows a varia-tion in slopes across individuals similar to RSA. With bothindividuals breathing at a TTOT of 6 s (10 breaths/min) underbaseline condition, their respective RSA/VT values would be290 and 70 ms/l (M � 180 ms/l). If under hypothetical taskconditions, individual A would switch to breathing faster at aTTOT of 4 s, his or her RSA/VT would be reduced markedly to170 ms/l due to the steep slope. If individual B under the sameexperimental condition would switch to breathing slower at aTTOT of 8 s, his or her respective RSA/VT would be increasedonly slightly to 110 ms/l, due to the shallower slope. While themean TTOT of both individuals again would be 6 s, their groupmean RSA/VT would be M � 140 ms/l. Thus, despite nochange in mean TTOT, values of RSA/VT would suggest adecrease in vagal tone on the group level. This effect couldmaterialize independently from any actual change in vagaltone.
Limitations of the between-individual approach also applyto attempts to control for respiratory influences using analysisof covariance: RSA values are adjusted without regard tovariation in individual sensitivities of RSA modulation byrespiration (for an illustration, see 18). Thus, strategies infer-ring respiratory influences on RSA from a between-individualanalysis of respiratory parameters are not suitable to capturethe full extent of possible influences. Interpretation based onmean respiratory changes is less likely to fail if there is reasonto expect little interindividual variation in respiratory responses.This is more likely the case in situations of basic biologicaladaptation such as in physical activity increase but less likelyin response to situations of psychological challenge. However,even with a reduced interindividual variability in RRs and VT,in smaller samples the estimate of cardiac vagal tone can bebiased considerably, if a few individuals with strong sensitiv-ities of respiratory RSA modulation diverge in their responsefrom the mean group response.
Control for RR, VT, or Both?
Continuing uncertainty seems to exist regarding the impor-tance of controlling for RR or both RR and VT. While researchhas demonstrated that both affect RSA profoundly, the relativeimportance of both has been debated. Because normally RRand VT are tightly coupled to match metabolic demand, within-
individual variations in RR or VT alone may indeed accountfor most of the variation in RSA under regular conditions.However, voluntary influences on breathing pattern, phasicadaptation to environmental challenges, and central nervoussystem processes related to stress and anxiety (21–23) oftenlead to a disruption of brain stem respiratory control and thusthe coupling of RR and VT. As a consequence, substantialindependent contributions of RR and VT to RSA can beexpected.
Using data from a previous study (20), we compared theinfluence of both parameters on RSA under conditions ofbaseline measurements (coupling of RR and VT) versus ex-perimental instructions to change the breathing pattern sys-tematically (partial uncoupling of RR and VT). Participantswere 25 healthy students (10 women). They breathed at fourdifferent RR, with 8, 10.5, 13, and 18 breaths/min (TTOT 7.5,5.7, 4.6, and 3.3 s), following a pretaped auditory signal withrising pitch of the tone for inspiration and falling tone forexpiration. These paced breathing sequences were performedin supine posture with the instruction to a) only follow thetones with the breathing excursions and b) vary VT voluntarilywhile adhering to the speed of the signal. From continuousmeasurements of respiration (pneumotachograph with FleischNo. 2 transducer) and the electrocardiogram, we extractedTTOT and VT, as well as RSA using the peak-valley method(3,24).
As expected, results showed marked differences in theaverage within-individual correlation between TTOT and VT
for the condition with spontaneous breathing versus voluntaryvariation of VT, with r � 0.80 (range: 0.57 to 0.92) versus r �0.37 (range: �0.002 to 0.68), respectively (for direct compar-ison of both conditions, we analyzed only breaths within theVT range observed under spontaneous VT conditions). Al-though TTOT and VT were both highly correlated with RSA,the median of the within-individual partial correlations be-tween VT and RSA controlled for TTOT was rather low onaverage during the spontaneous VT condition (Table 2), due tothe high correlation between TTOT and VT. For the conditionwith varying VT, the partial correlation was higher, indicatingan increasing importance of VT for RSA modulation with thesmaller correlation between TTOT and VT.
For both conditions, spontaneous and voluntary varyingVT, we also calculated within-individual hierarchical linearregressions to estimate the variance of RSA explained byTTOT when entering it as the first predictor and the additionalvariance explained when entering VT as the second predictor.While under spontaneous VT, most of the variance was indeed
TABLE 2. Within-Individual Correlations of RSA With TTOT and VT, and Partial Correlations Between RSA and VT Controlling for TTOT forConditions With Spontaneous VT (n � 119–139 Respiratory Cycles) vs. Varying VT (n � 60–135 Respiratory Cycles)
rRSA � TTOT rRSA � VT rRSA � VT with TTOT
Median Range Median Range Median Range
Spontaneous VT .72 .38–.87 .67 .31–.85 .24 �.08–.51Varying VT .54 .16–.80 .60 .10–.79 .56 .18–.74
RESPIRATORY SINUS ARRHYTHMIA AND RESPIRATION
619Psychosomatic Medicine 68:617–627 (2006)

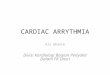
explained by TTOT, under conditions of voluntary variation ofVT, the contribution of VT rose more than threefold (Figure 1).The increase in explained variance was even greater when therange of VT was not restricted to the range observed underspontaneous VT conditions. (Note that in a number of casesthe intercorrelation between TTOT and VT would be viewed astoo high for multiple regression (multicollinearity), e.g., r �0.80 in 11 cases for the spontaneous VT condition). When theorder of predictors was reversed, VT initially accounted foronly slightly less RSA variance under spontaneous breathing,but for similar or slightly greater portions of the varianceunder voluntary variation of VT. Depending on the condition,approximately 45% to 55% of the total RSA variance wasexplained by respiratory parameters, and VT contributed up toone third to this prediction after TTOT had been accounted for.
Thus, changes in VT substantially contribute to the varia-tion in RSA. When analyzing data from conditions where RRand VT are tightly coupled, this contribution may not beimportant and remain mostly unrecognized. However, uncou-pling of RR and VT may occur in situations where the indi-vidual is behaviorally challenged. Ignoring VT under theseconditions may lead to erroneous inferences regarding cardiacvagal tone.
Paced Breathing as a Control Strategy
One approach to control the influence of respiration onRSA is to pace the participants’ respiration at a standard speedthroughout the experiment. The goal is to eliminate fluctua-tions of RR across experimental conditions and thus prohibita contamination of RSA changes with potential task-inducedchanges in respiration. Auditory pacing using a metronome ora computer-generated tone pattern has been used for thispurpose, as well as visual pacing in which individuals matchtheir breathing excursions to a predetermined template usingbiofeedback.
However, a number of issues limit the usefulness of pacedbreathing during experiments. First, auditory pacing can onlyaccount for RR. Automatic adjustment of VT to a particular RRcan be expected in periods of steady state, but this is not guar-anteed under conditions of behavioral demand (see above). Al-though visual matching of the VT curve using biofeedback wouldallow an additional tight control for volume aspects, it is imprac-tical in combination with many behavioral tasks, in particularwith those requiring visual processing. As a minimum require-ment for pacing procedures, a manipulation check with measuresof rate and volume would be required throughout the task periodsof interest. Second, pacing requires dividing information process-ing capacities, which can distract from tasks and thus makeperformance suboptimal. Although the paced breathing pattern issometimes trained before the experiment, it can be doubted thatin complex behavioral tasks (in particular in tasks that changemetabolic demand) such learned breathing patterns prevail overthe automatic regulation through the respiratory center. Third,psychological and physiologic responding under study can bemodified by voluntary alterations in breathing pattern. Pacedbreathing at a slower speed has been used to modify anxiety andautonomic response to stress (e.g., 25,26). Irregularity in breath-ing has been observed in clinical populations (27,28), and theimposition of regularity may alter typical response characteristicsin these individuals. In addition, voluntary imposition of breath-ing patterns against metabolic demand has been shown to affectgas exchange unfavorably (29), which in turn could affect auto-nomic activity. Fourth, given the interindividual variation in basalRR, a particular standard pacing speed may not be acceptable forall subjects under particular task conditions. Theoretically, themost comfortable speed would have to be determined for eachindividual across the range of conditions to be studied, but thiswould be impractical for most experimental protocols.
The role of paced breathing as a respiratory control in RSAstudies is probably restricted to protocols in which compari-sons between repeated baseline measurements are being made.We found that under baseline conditions, pacing at differentspeeds (eight to 18 breaths per minute) for 2 to 3 minutes istypically tolerated well in healthy participants and asthmapatients, with little impact on symptom and mood ratings (30).
Additional Control for Carbon Dioxide PartialPressure (pCO2)?
There is evidence from experimental studies that alteredpCO2 levels can influence RSA (31–33). There is a wide
0
10
20
30
40
50
60
ops
enatn
TV suo iyrav
TV gn TV gniyrav
)lluf(
SR ni ecnairav denialpxe
%A
% variance VT% variance TTOT
0
10
20
30
40
50
60
V suoenatnops
T TV gniyrav
)lluf( TV gniyrav
SR ni ecnairav denialpxe
%A
% variance TTOT% variance VT
Figure 1. Percent RSA variance accounted for in within-individual hierar-chical linear regressions with (A) TTOT or (B) VT entering as the firstpredictor for conditions of spontaneous VT and voluntary variation of VT (VT
range restricted to match spontaneous VT conditions, and full VT range).
T. RITZ AND B. DAHME
620 Psychosomatic Medicine 68:617–627 (2006)

variation of basal pCO2 levels in the population (34) makingthis potentially an additional complication in interpreting RSAdifferences between individuals. Also, substantial changes inpCO2 during stress and anxiety states can be observed withinindividuals (e.g., 23,35). Because changes in pCO2 normallydepend closely on changes in ventilation, potential effects ofchanges in pCO2 on RSA will often be masked by effects ofRR and VT. Thus, for a given metabolic state, pCO2 isinversely proportional to alveolar ventilation, which is theproduct of RR and (VT minus Vds), where Vds is the volumeof anatomical (or physiological, if one wishes to calculate it)dead space. Increases in alveolar ventilation and decreases inpCO2 may occur, with constant VT and dead space, by anincrease in RR alone, which decreases RSA. Or, increases inalveolar ventilation and decreases in pCO2 may occur atconstant RR and constant dead space by an increase in VT
alone, which would lead to an increase in RSA. Alterna-tively, an increase in alveolar ventilation and decrease inpCO2 may be linked to increases in both RR and VT, whichmight cancel out respiratory influences on RSA or lead todecreases or increases in RSA, depending on whether RR orVT contribute to a greater degree. Thus, changes in pCO2
could be associated with any outcome in (respiration-un-corrected) RSA.
Ventilation (and thus RR and VT) is normally adjustedautomatically to maintain or reinstate CO2 homeostasis acrossa variety of internal and environmental challenges. However,under experimental conditions of tightly controlled RR and VT
by paced breathing, Sasano et al. (33) observed increase inRSA when the fraction of CO2 in the inspired air was in-creased. The extent to which similar dramatic decouplingmight occur under psychophysiologic laboratory conditionsremains speculative, and the extent of any influence of pCO2
on RSA, in addition to effects of RR and VT, remains to beexplored. Manipulations of anatomical dead space at constantRR and VT may be an avenue to explore such influences. Forexample, under the influence of a potent anticholinergic agentsuch as inhaled tiotropium bromide, normal individuals man-ifest a significant increase in dead space (36). Combined withan experimentally fixed RR and VT by paced breathing, thiswould lead to decreased alveolar ventilation due to increasedanatomical dead space and, accordingly, an increase in pCO2.In asthma, provocation with methacholine or cold dry air leadsto constriction of the large airways, thereby decreasing ana-tomical dead space. Alternatively asthmatic patients with air-way constriction can be given bronchodilating agents, therebyincreasing anatomical dead space. In these cases, maintenanceof constant RR and VT will result in decreased pCO2 (withprovocation) or increased pCO2 (with dilation). If pCO2
changes should prove to contribute substantial independenteffects on RSA under such conditions, then future correctionmethods may have to incorporate additional adjustments forthis factor. It should be noted that some of these conditions aremore likely to occur between individuals than within the sameindividual over time. Also, because considerable voluntaryeffort must be directed at maintaining a constant breathing
pattern in the face of changes in pCO2, it remains to be shownthat such experimental manipulations are representative ofreal-life situations.2
Instrumentation Issues
Often, the only respiratory measure included in studies isRR derived from measurements with one strain gauge orfrom secondary processing of the interbeat-interval timeseries or the impedance cardiography signal. This approachdoes not allow for an estimation of VT and thus generatesrather limited information about the respiratory system. Inparticular, when studying the respiratory autonomic rela-tionship, measurements of VT are needed, which allow thederivation of multiple indices of interest (23). VT can beestimated indirectly using thoracic and abdominal sensorssuch as inductance plethysmography bands, pneumaticbelts, or piezoelectric strain gauges, or directly using spi-rometry or pneumotachography (22,37). Interpretation ofindirect measurements requires a precalibration using in-strumentation for direct volume measurement or isovolumemaneuvers (38). It should be noted that costs for suchequipment and computational requirements in data process-ing are rather modest compared with more demandingtechniques commonly used in psychophysiology (39).
A Note on the Comparison of Absolute RSA Levels
It has become common to compare absolute levels of RSAor HRV between groups. Comparisons of absolute levels ofRSA between groups was reported in 24 of the 39 studiespublished in Psychosomatic Medicine in the 11-year period. Incardiology, a host of studies has demonstrated improved clin-ical outcome in patients with myocardial infarct who have ahigher cardiac interbeat-interval variability (for reviews, see2,8). Although impressive on a practical level, the interpreta-tion of these findings in terms of cardiac vagal outflow istentative at best. The assumption that the absolute level ofcardiac vagal outflow can be estimated by RSA and can becompared between individuals rests on animal experiments,which have shown that the vagus is silent or almost silentduring inspiration, whereas its excitation is maximal duringexpiration (for a review, see 17). However, in humans aresidual vagal tone is observed in inspiration to maximalinspiratory level, and this residual vagal activity is not relatedto RSA (40). With this added uncertainty, an interpretation ofRSA as a between-individual measure of cardiac vagal tone isnot well justified. Even controlling for respiratory parameterscannot alleviate the problem. Findings with complete vagalblockade suggest that the prediction can be improved by alinear combination of heart rate and RSA, but this awaitsevaluation in larger samples (17,40). Additional problemsarise from a strong dependency of RSA on physical activitylevels (41). Because the immediate autonomic adjustment tophysical activation is a vagal withdrawal, varying levels of
2We thank Michael D. Goldman (personal communication, February 2006)for comments and suggestions on this paragraph.
RESPIRATORY SINUS ARRHYTHMIA AND RESPIRATION
621Psychosomatic Medicine 68:617–627 (2006)

activation or deactivation, body movements, or static tensionbetween individuals during baseline measurements can intro-duce substantial error when individuals are being comparedregarding their “basal” vagal tone. Given these doubts, differ-ences in RSA values between individuals would be morecautiously interpreted as evidence for respiratory modulationof heart rate.
A Method to Control for RR and Volume Effects onthe Time-Domain Index of RSA
Procedures have been proposed to control for RR and VT inthe frequency domain measure of high frequency HRV (42)and in the time-domain peak-valley index (20). Without re-spiratory correction, high-frequency HRV and the peak-valleyindex yield almost identical results (3), but data comparing therespiration-corrected indices of both methods are still missing.Frequency- and time-domain measures both require unique pre-cautions in quantification, have unique advantages and disad-vantages for addressing different research questions, and varytheir suitability for different experimental designs and settings(for a detailed comparison, see 43). Here, we will focus on abrief introduction of a correction procedure for the time-domain method. This method has the advantage of yielding abreath-by-breath index of corrected RSA, which also allowsan estimation of short-term, phasic changes in cardiac vagaltone. Frequency domain indices typically require uninter-rupted measurement epochs of at least 1 minute to yield validestimates (2). In the following, we briefly present the rationaleand method of this correction procedure, followed by exam-ples of its application.
Basic Rationale and Method
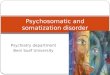
The time-domain correction method is based on observa-tions that the quotient of RSA per liter VT shows a systematicdecline across a range of increasing RR (13,14). The declineof RSA/VT is fairly linear from approximately 6 to 30 breaths/min, which covers a great part of the spectrum of naturallyoccurring RRs in healthy human individuals (note: For moreclarity we will only refer to TTOT in the following, which is theinverse of RR). A change in vagal tone within an individualaffects the intercept of the regression equation (elevation ofthe regression line) of RSA/VT on TTOT but not the slope(15,17,44,45) (Figure 2A). Grossman and colleagues (13)introduced this idea to psychophysiology and showed thatRSA/VT corrected for TTOT is closely correlated within indi-viduals with changes in �-blocked heart rate across a range ofexperimental tasks. We utilized this concept for a within-individual correction procedure of the peak-valley RSA mea-sure for TTOT and VT (20,46). The procedure requires abaseline calibration procedure to determine each individual’sunique modulation of RSA/VT by TTOT using three to fourepochs of paced breathing across a representative range ofTTOT (e.g., 7.5, 5, and 3.3 s, equals 8, 12, and 18 breaths/min).RSA/VT during the main experiment is then expressed as adeviation from RSA/VT observed under baseline conditions ata particular TTOT. For each respiratory cycle during the main
experiment, the index is calculated as the deviation from thevalue predicted on the basis of the preexperimental pacedbreathing trials (see Figure 2B; Appendix 1 for computationalprocedures).3 A similar method has been employed for esti-mation of additional heart rate, with preexperimental calibra-tion trials for metabolically justified heart rate using stepwiseincreases in exercise workload (47).
3A Matlab routine to extract a respiration-corrected index of RSA fromheart period and VT curve data can be obtained upon request (Schulz SM,Gerlach AL, Ritz T. A Matlab routine for analyzing respiration-controlledrespiratory sinus arrhythmia in the time domain. Unpublished program doc-umentation, 2006). In addition to the experimental data, the program requiresdata from an adequate paced-breathing baseline calibration period. To per-form the regression analysis (Appendix 1, step 5) without a third-partyproduct, the Matlab Statistics Toolbox is required. Alternatively, a datainterface for supplementing this step per using your preferred statistics pro-gram (e.g. SPSS with the syntax provided in this paper) is implemented.
Figure 2. A, The slope of the regression (sensitivity parameter) is thoughtto be a stable characteristic of the individual, whereas the intercept varies withchanges in cardiac vagal tone (reproduced with permission from Grossmanand Kollai, 1993); x-axis: respiration rate (in Hz), y-axis: RSA/VT. The twolines represent the same individual at different levels of cardiac vagal tone. B,Example for two individuals with different sensitivities of the respiratorymodulation of RSA/VT. In this illustrative case, both show decreases ofcardiac vagal tone from baseline to the experimental phase; solid lines:RSA/VT regression line during baseline paced breathing calibration with threerespiration rates (TTOT � 6.5, 5, and 3.5 s, equaling 9.2, 12, and 17.1breaths/min); dashed lines: hypothetical level of RSA/VT for the three respi-ration rates during a subsequent experiment that led to a decrease in vagaltone. RSA/VT for the experiment is calculated for each breath as observedRSA/VT minus RSA/VT baseline at the observed TTOT of the respectivebreath.
T. RITZ AND B. DAHME
622 Psychosomatic Medicine 68:617–627 (2006)

Empirical Validation
An important aspect of the correction procedure is that it isperformed on a within-individual level because of the varia-tion in slopes of the regression of RSA/VT on TTOT betweenindividuals. Slopes and intercepts of the model are calculatedfor each participant separately (Figure 2B). The validity of thecorrection procedure rests on the assumption that the slope ofthe model is a stable characteristic of the individual, while theintercept changes with manipulations of vagal tone.
In support of the basic assumption of the model, we foundthat the slope parameter was sufficiently stable across months(46,48) and across voluntary variations in VT (20). As pre-dicted, for variations in posture (standing versus supine),which typically have a pronounced effect on vagal tone, wefound strong effects only on the intercept and considerablestability of the slope parameter on the group level (20). How-ever, stability of the individual differences in slopes was lowbetween postures; thus, determination of the slope parameterfor within-individual correction should take into account theposture at which measurements in the main experiment areundertaken.
Accurate estimation of the slope parameter is dependent ona stable level of vagal tone throughout the paced breathingtrials. Changes in the level of vagal tone during paced breath-ing would lead to steeper or flatter slopes or a reduced preci-sion in determining the slope parameter of the individual,depending on which breathing frequencies were affected.There has been some disagreement on the stability of cardiacvagal tone during paced breathing (49,50). In our study (20),mean heart rate (used as an estimator of vagal tone under theseconditions) was relatively stable across the four paced breath-ing trials from 8 to 18 breaths/min during the supine condition(maximum difference between conditions 0.6 beats/min), butshowed significant increases (though minimal, with 0.9–2.8beats/min) from slower to faster breathing frequencies forconditions standing and supine with variable VT. Substantialdecreases in heart rate were observed during supine conditionsfor two participants and during standing conditions for sixindividual participants. Excluding these individuals did notgreatly affect the findings regarding the stability of the slopeparameter.
In further analyses, we addressed the argument that theslope parameter may only reflect aspects of the individual’shabitual breathing pattern. It could be speculated that the maindeterminant of the slope of RSA/VT against TTOT is theindividual’s inherent tendency to vary VT in a characteristicfashion across breathing cycles of different duration. Thus,individuals with very high volumes at longer cycles and verysmall volumes at shorter cycles would have a reduced steep-ness of their RSA/VT slope (e.g., individual ID 2 in Figure 2B)compared with individuals with only moderately high vol-umes at longer cycles and moderately small volumes at shortercycles, who would have a steeper RSA/VT slope (e.g., indi-vidual ID 1 in Figure 2B) (in this example identical RSAvalues are assumed for both individuals). We tested this as-
sumption by correlating the slopes of VT on TTOT with theslope of RSA/VT on TTOT in three samples (total N � 129(51)) and observed only low to moderate correlations betweenthese slope parameters. Thus, individual tendencies to modu-late VT across the TTOT range are only a small source ofvariance in the RSA/VT change. These findings also demon-strate that adjustment of RSA for both VT and TTOT is nec-essary.
Experience comparing corrected and uncorrected indicesshows that controlling for respiratory effects can uncovereffects on vagal tone that are predicted but are masked byconcomitant changes in respiration. For example, vagal with-drawal can be expected as a consequence of static skeletalmuscle activation (52). At the same time, increases in VT dueto muscle activation will increase RSA and thus mask theactual effects on cardiac vagal tone in this parameter (whichwould be expected to materialize in a decrease of RSA) to acertain extent. In a study with brief contractions of facial andforearm muscles, we found little effect of the experimentalprotocol on uncorrected RSA but clear reductions in therespiration-corrected measure of RSA (53). A comparison ofindices showed that using RSA/VT uncorrected for RR yieldedthe most favorable results, whereas additional correction forthe reduction of RSA/VT across RR yielded slightly lesspowerful results (46). This can be expected as skeletal muscletension is also expected to increase RR, thus reducing RSAand playing in favor of the expected direction of changes inRSA by vagal withdrawal.
On the other hand, in situations where vagal activation isexpected, correction for concomitant changes has slightlyattenuated the effects on RSA but not abolished them alto-gether. For example during facial cold stimulation, which isknown to produce vagal slowing of heart rate (54,55), weobserved increases in both RSA and RSA/VT corrected forTTOT; however, only the former were statistically significant,while the latter were reduced to a trend (46). In another studythat included viewing of specifically selected categories ofaffective pictures (56,57), robust increases in RSA were seenduring erotic pictures that were also accompanied by increasesin TTOT. Using RSA/VT corrected for TTOT did not change thefindings of an increase in vagal tone, thus confirming assump-tions that in early stages of erotic tension, parasympatheticexcitation is prominent (58).
In other studies using experimental emotion induction, theuncorrected peak-valley RSA index suggested increases incardiac vagal tone, but these findings were not retained aftercorrection for respiratory parameters. In one study, partici-pants viewed a mixed selection of positive, negative, andneutral pictures (59), whereas in the other study they werepresented with homogeneous blocks of happy and depressingpictures and self-referring statements (60). In interpretingthese findings, we preferred to retain the more conservativenull hypothesis of no changes in cardiac vagal tone, given thelimited empirical evidence on emotion-induced vagal excita-tion, which includes a lack of corroborating evidence fromanimal and pharmacologic blockade studies. Also, in these
RESPIRATORY SINUS ARRHYTHMIA AND RESPIRATION
623Psychosomatic Medicine 68:617–627 (2006)

and other studies using the correction procedure, the results inthe corrected RSA measure were often not predicted frompatterns of group mean changes in RR and/or VT, which canbe due to the within-individual nature of the correction pro-cedure. Findings of emotion induction studies vary with re-gard to observed changes in respiratory parameters (e.g., 61–63), which could indicate a considerable individual responsespecificity or situation by individual response specificity inthe activation of this system. Especially the former in combi-nation with interindividual differences in the sensitivity ofRSA to respiratory changes would be likely to produce spu-rious findings in the estimation of vagal activation.
Finally, we used corrected and uncorrected RSA indices inanalyses addressing a clinical hypothesis on depression andasthma. It has been assumed for some time that depressivestates are particularly potent in eliciting asthmatic airwayobstruction due to vagal excitation (64,65). Vagal activity isknown to be a potent constrictor of the airways (66). In twostudies with asthma patients (56,67), we found positive cor-relations between changes in RSA/VT corrected for TTOT andthe degree of airway obstruction during or after emotioninduction with depressing pictures or self-referring statements.Although a tight relationship between cardiac and airwayvagal tone is not necessarily guaranteed (68) and the correla-tions were calculated between individuals, the findings areconsistent with the hypothesis concerning depression andasthma, and with the long-held assumption that the vagus isthe pathway for psychologically induced airway obstruction(69,70). Most important in the present context, this relation-ship was not seen with uncorrected RSA.
In summary, in a number of studies corrected RSA wassuperior over uncorrected RSA by supporting plausible phys-iological (53) and clinical (56,67) hypotheses. It is likely thatin at least some of these instances respiratory parameters haveworked against the directions of changes in RSA, such asincreases in RSA during muscle tension due to increases inVT. Without correction for respiratory parameters, the estima-tion of vagal changes would have been too conservative inthese cases. In other studies, respiratory correction did notlead to greatly diverging results (46,56). These could beinstances of strong vagal excitation and/or little accompanyingchanges of respiratory parameters working in the directions ofRSA changes. Finally, in studies in which respiratory correc-tion abolished changes seen in uncorrected RSA (59,60),respiratory parameters either may have worked progressivelytoward producing RSA changes, or interindividual variationsin respiratory changes in combination with interindividualvariation in the sensitivity of RSA to respiratory changes mayhave existed. These were also mostly instances in which noclear a priori hypothesis on vagal changes existed.
CONCLUSIONThe study of respiration-related HRV will continue to offer
unique insights into the autonomic regulation of the heart.However, a greater degree of complexity regarding thesemeasures has to be conceded if psychosomatic research aims
to make progress in this area. Controlling for respiratoryfactors, which constitute the most significant contributors toRSA, is among the greatest concerns. The number of situa-tions in which correction of respiratory influences on RSA isof secondary importance, such as strong vagal changes withvery little respiratory changes (on the group level and in termsof interindividual variation in the direction of changes), isprobably very limited. The small increment in procedural andcomputational efforts involved in respiratory control is faroutweighed by the advantage of a more stringent estimation ofcardiac vagal tone. To allow for comparison among the sub-stantial body of literature that, thus far, has primarily reporteduncontrolled indices, future studies should report both find-ings with controlled and uncontrolled indices.
It should be noted that the concerns raised about respiratorycontrol are relevant for the interpretation of RSA changeswithin individuals (and for between-individual comparison ofreactivity scores, e.g., difference scores of task minus base-line). Respiratory control is important when respiration-re-lated HRV should be interpreted with respect to underlyingautonomic mechanisms, such as vagal activity. This is oftenthe case in experiments that test hypotheses about disease-relevant psychobiological models. In the between-individualcomparison of absolute RSA values, substantial uncertaintyremains about the interpretation in terms of autonomic activ-ity. This is particularly due to the residual vagal activityduring inspiration in humans, which has been shown to atten-uate substantially the between-individual relationship of vagaltone and absolute RSA values. Nevertheless, research onthe predictive power of absolute HRV values for cardio-vascular health is valuable on a practical level and can beimportant in shaping behavioral prevention and interven-tion techniques.
Available procedures for respiratory control show progressover uncontrolled practice, but these controlled measures ofRSA are by no means perfect. As with any other research area,research on respiration-related perturbations of autonomicoutflow is constantly evolving in its exploration of the originsof RSA, its physiological mechanisms, and factors influencingit. It is now known that potential autonomic determinants ofRSA are not restricted to the vagal system and contributions ofadrenergic and peptidergic systems require further explorationand possibly future precautions in study design and interpre-tation (18). These and other research directions, such thepotential function of RSA for optimizing gas exchange(71,72), links of RSA with central nervous system pathways(73), and the genetic determination (74) of RSA, will bothprofit from respiratory control procedures and enable us torefine these techniques in the future.
APPENDIXComputational steps and procedures involved in determin-
ing respiration-corrected RSA as an indicator of cardiac vagaloutput.
First step: Measuring the shortest and the longest heartperiod (HPmin and HPmax) within each breathing cycle.
T. RITZ AND B. DAHME
624 Psychosomatic Medicine 68:617–627 (2006)

Second step: Calculation of (uncorrected) peak-valley RSAfor each breathing cycle: HPmax � HPmin (under the condi-tion that HPmin precede HPmax in time).
Third step: Normalization of RSA: RSA divided by VT foreach breath: RSA/VT.
Fourth step: Repeating steps 1 through 3 for each pacedbreathing epoch from the baseline calibration procedure andthe experimental data.
Fifth step: Calculation of the within-individual regressionof RSA/VT on TTOT (measured in seconds: s; TTOT � 1/RR �60) across the whole paced breathing task (all paced breathingepochs from the baseline calibration procedure concatenated):y� � a � bx, with a � My � b � Mx, b � cov (x,y)/s2, andx � (TTOT)calibration. Mx, My are the means, sx
2 the variance ofthe x values, cov (x,y) � 1/N �i (x � Mx) (y � My). Moreprecisely, x, y, y� and yresidual must be stated: xi, yi, y�i yresidualiwith i � 1 . . . .N.
Using the SPSS routine REGRESSION you will get themeans (Mx,My), variance of the x values (s2x), the covariancecov (x,y), the intercept a and the slope b, the predicted y�, andthe residuals, which are our wanted (RSA/VT)corrected values.To get these parameters, you have to apply the followingSPSS syntax:
REGRESSION/MISSING LISTWISE/STATISTICS COEFF OUTS BCOV/CRITERIA � PIN(0.05) POUT(0.10)/NOORIGIN/DEPENDENT RSADIVVT/METHOD � ENTER TTOT
Sixth step: Calculating the corrected RSA index for eachrespiratory cycle during the main experiment [yresidual �(RSA/VT)corrected] as the deviation from the value predicted onthe basis of the preexperimental paced breathing trials:yresidual � y � y�, with y � (RSA/VT)experiment, and y� �(RSA/VT)predicted by taking the regression coefficients a and bfrom the concatenated paced breathing trials.
In SPSS, this is realized by the following COMPUTEcommand:
COMPUTE YRESEXP � Y � (A � B � TTOTEXP).
We wish to thank Michael D. Goldman, Paul Grossman, Andreas vonLeupoldt, Stefan M. Schulz, and three anonymous reviewers forvaluable comments.
REFERENCES1. Berntson GG, Bigger JT Jr, Eckberg DL, Grossman P, Kaufmann PG,
Malik M, Nagaraja HN, Porges SW, Saul JP, Stone PH, van der MolenMW. Heart rate variability: origins, methods, and interpretive caveats.Psychophysiology 1997;34:623–48.
2. Task Force of the European Society of Cardiology and the NorthAmerican Society of Pacing and Electrophysiology. Heart ratevariability: standards of measurement, physiological interpretation, andclinical use. Eur Heart J 1996;17:354–81.
3. Grossman P, van Beek J, Wientjes C. A comparison of three quantifi-cation methods for estimation of respiratory sinus arrhythmia. Psycho-physiology 1990;27:702–14.
4. Berntson GG, Cacioppo JT, Quigley KS. Respiratory sinus arrhythmia:autonomic origins, physiological mechanisms, and psychophysiologicalimplications. Psychophysiology 1993;30:183–96.
5. Akselrod S, Gordon D, Madwed JB, Snidman NC, Shannon DC, CohenRJ. Hemodynamic regulation: investigation by spectral analysis. Am JPhysiol 1985;249:H867–75.
6. Katona PG, Jih F. Respiratory sinus arrhythmia: noninvasive measure ofparasympathetic cardiac control. J Appl Physiol 1975;39:801–5.
7. Yongue BG, McCabe PM, Porges SW, Rivera M, Kelley SL, AcklesPK. The effects of pharmacological manipulations that influence vagalcontrol of the heart on heart period, heart-period variability and respi-ration in rats. Psychophysiology 1982;19:426–32.
8. Kleiger RE, Stein PK, Bigger JT Jr. Heart rate variability: measurementand clinical utility. Ann Noninvasive Electrocardiol 2005;10:88–101.
9. Buchman TG, Stein PK, Goldstein B. Heart rate variability in criticalillness and critical care. Curr Opin Crit Care 2002;8:311–5.
10. Angelone A, Coulter NA Jr. Respiratory sinus arrhythmia: a frequencydependent phenomenon. J Appl Physiol 1964;19:479–82.
11. Brown TE, Beightol LA, Koh J, Eckberg DL. Important influence ofrespiration on human R-R interval power spectra is largely ignored.J Appl Physiol 1993;75:2310–7.
12. Davies CT, Neilson JM. Sinus arrhythmia in man at rest. J Appl Physiol1967;22:947–55.
13. Grossman P, Karemaker J, Wieling W. Prediction of tonic parasympa-thetic cardiac control using respiratory sinus arrhythmia: the need forrespiratory control. Psychophysiology 1991;28:201–16.
14. Hirsch JA, Bishop B. Respiratory sinus arrhythmia in humans: howbreathing pattern modulates heart rate. Am J Physiol 1981;241:H620–9.
15. Saul JP, Berger RD, Chen MH, Cohen RJ. Transfer function analysis ofautonomic regulation, II: respiratory sinus arrhythmia. Am J Physiol1989;256:H153–61.
16. Grossman P, Stemmler G, Meinhardt E. Paced respiratory sinus arrhyth-mia as an index of cardiac parasympathetic tone during varying behav-ioral tasks. Psychophysiology 1990;27:404–16.
17. Grossman P, Kollai M. Respiratory sinus arrhythmia, cardiac vagal tone,and respiration: within- and between-individual relations. Psychophys-iology 1993;30:486–95.
18. Grossman R, Taylor EW. Respiratory sinus arrhythmia, cardiac vagaltone, and a critique of the polyvagal theory: toward a theory of biobe-havioral allostasis of energy exchange. Biol Psychol. In press.
19. Jennings JR, McKnight JD. Inferring vagal tone from heart rate vari-ability. Psychosom Med 1994;56:194–6.
20. Ritz T, Thons M, Dahme B. Modulation of respiratory sinus arrhythmiaby respiration rate and volume: stability across postures and volumevariations. Psychophysiology 2001;38:858–62.
21. Keating WR, Nadel JA. Immediate respiratory response to suddencooling of the skin. J Appl Physiol 1965;20:65–9.
22. Harver AR, Lorig T. Respiration. In: Cacioppo JT, Tassinary LG,Berntson GG, eds. Handbook of Psychophysiology. Cambridge: Cam-bridge University Press; 2000:265–93.
23. Wientjes CJ. Respiration in psychophysiology: methods and applica-tions. Biol Psychol 1992;34:179–203.
24. Eckberg DL. Human sinus arrhythmia as an index of vagal cardiacoutflow. J Appl Physiol 1983;54:961–6.
25. Clark ME, Hirschman R. Effects of paced respiration on anxiety reduc-tion in a clinical population. Biofeedback Self Regul 1990;15:273–84.
26. Harris VA, Katkin ES, Lick JR, Habberfield T. Paced respiration as atechnique for the modification of autonomic response to stress. Psycho-physiology 1976;13:386–91.
27. Abelson JL, Weg JG, Nesse RM, Curtis GC. Persistent respiratoryirregularity in patients with panic disorder. Biol Psychiatry 2001;49:588–95.
28. Stein MB, Millar TW, Larsen DK, Kryger MH. Irregular breathingduring sleep in patients with panic disorder. Am J Psychiatry 1995;152:1168–73.
29. Ceugniet F, Cauchefer F, Gallego J. Voluntary decreases in breathingfrequency in exercising asthmatic subjects. Eur Respir J 1996;9:2273–9.
30. Dahme B, Thons M, Ritz T. Ventilation-correction of respiratory sinusarrhythmia: experienced symptoms during paced breathing in healthyparticipants and asthma patients [abstract]. Psychophysiology 2003;40:S35.
31. Al-Ani M, Forkins AS, Townend JN, Coote JH. Respiratory sinusarrhythmia and central respiratory drive in humans. Clin Sci (Lond)1996;90:235–41.
32. Poyhonen M, Syvaoja S, Hartikainen J, Ruokonen E, Takala J. Theeffect of carbon dioxide, respiratory rate and tidal volume on humanheart rate variability. Acta Anaesthesiol Scand 2004;48:93–101.
RESPIRATORY SINUS ARRHYTHMIA AND RESPIRATION
625Psychosomatic Medicine 68:617–627 (2006)

33. Sasano N, Vesely AE, Hayano J, Sasano H, Somogyi R, Preiss D,Miyasaka K, Katsuya H, Iscoe S, Fisher JA. Direct effect of Pa(CO2) onrespiratory sinus arrhythmia in conscious humans. Am J Physiol HeartCirc Physiol 2002;282:H973–6.
34. Jack S, Rossiter HB, Pearson MG, Ward SA, Warburton CJ, Whipp BJ.Ventilatory responses to inhaled carbon dioxide, hypoxia, and exercisein idiopathic hyperventilation. Am J Respir Crit Care Med 2004;170:118–25.
35. Ritz T, Wilhelm FH, Gerlach AL, Kullowatz A, Roth WT. End-tidalpCO2 in blood phobics during viewing of emotion- and disease-relatedfilms. Psychosom Med 2005;67:661–8.
36. Goldman M, Saadeh C, Ross D. Clinical applications of forced oscil-lation to assess peripheral airway function. Respir Physiol Neurobiol2005;148:179–94.
37. Ritz T, Dahme B, DuBois AB, Folgering H, Fritz GK, Harver AR,Kotses H, Lehrer PM, Ring C, Steptoe A, Van de Woestijne KP.Guidelines for mechanical lung function measurements in psychophys-iology. Psychophysiology 2002;39:546–67.
38. Sackner MA, Watson H, Belsito AS, Feinerman D, Suarez M, GonzalezG, Bizousky F, Krieger B. Calibration of respiratory inductive plethys-mograph during natural breathing. J Appl Physiol 1989;66:410–20.
39. Cacioppo JT, Tassinary LG, Berntson GG, eds. Handbook of Psycho-physiology. Cambridge: Cambridge University Press; 2000.
40. Kollai M, Mizsei G. Respiratory sinus arrhythmia is a limited measureof cardiac parasympathetic control in man. J Physiol 1990;424:329–42.
41. Grossman P, Wilhelm FH, Spoerle M. Respiratory sinus arrhythmia,cardiac vagal control, and daily activity. Am J Physiol Heart CircPhysiol 2004;287:H728–34.
42. Wilhelm FH, Grossman P, Coyle MA. Improving estimation of cardiacvagal tone during spontaneous breathing using a paced breathing cali-bration. Biomed Sci Instrum 2004;40:317–24.
43. Grossman P. Respiratory and cardiac rhythms as windows to central andautonomic biobehavioral regulation: selection of window frames, keep-ing the panes clean and viewing the neural topography. Biol Psychol1992;34:131–61.
44. Berger RD, Saul JP, Cohen RJ. Transfer function analysis of autonomicregulation, I: canine atrial rate response. Am J Physiol 1989;256:H142–52.
45. Saul JP, Berger RD, Albrecht P, Stein SP, Chen MH, Cohen RJ.Transfer function analysis of the circulation: unique insights into car-diovascular regulation. Am J Physiol 1991;261:H1231–45.
46. Ritz T, Wagner C, Dahme B. A paced breathing procedure for the inter-and intraindividual estimation of cardiac vagal tone [abstract]. Psycho-physiology 1996;33:S70.
47. Turner RJ, Carroll D. Heart rate and oxygen consumption during mentalarithmetic, a video game, and graded exercise: further evidence ofmetabolically-exaggerated cardiac adjustments? Psychophysiology1985;22:261–7.
48. Ritz T, Thons M, Dahme B. Ventilation-correction of respiratory sinusarrhythmia: the sensitivity of the respiratory modulation of vagal out-flow is stable across time [abstract]. Psychophysiology 2003;40:S71.
49. Patwardhan AR, Evans JM, Bruce EN, Eckberg DL, Knapp CF. Vol-untary control of breathing does not alter vagal modulation of heart rate.J Appl Physiol 1995;78:2087–94.
50. Sargunaraj D, Lehrer PM, Hochron SM, Rausch L, Edelberg R, PorgesSW. Cardiac rhythm effects of. 125-Hz paced breathing through aresistive load: implications for paced breathing therapy and the polyva-gal theory. Biofeedback Self Regul 1996;21:131–47.
51. Ritz T, Dahme B. Estimating the sensitivity of respiratory RSAmodulation: the role of volume compensation with changing respirationrate [abstract]. Psychophysiology 2004;41:S85.
52. Pollak MH, Obrist PA. Effects of autonomic blockade on heart rateresponses to reaction time and sustained handgrip tasks. Psychophysi-ology 1988;25:689–95.
53. Ritz T, Dahme B, Wagner C. Effects of static forehead and forearmmuscle tension on total respiratory resistance in healthy and asthmaticparticipants. Psychophysiology 1998;35:549–62.
54. Khurana RK, Watabiki S, Hebel JR, Toro R, Nelson E. Cold face test inthe assessment of trigeminal-brainstem-vagal function in humans. AnnNeurol 1980;7:144–9.
55. Ritz T, Thons M, Dahme B. Increases in total respiratory resistanceduring forehead temperature stimulation. Biol Psychol 2000;55:119–35.
56. Ritz T, Thons M, Fahrenkrug S, Dahme B. Airways, respiration, and
respiratory sinus arrhythmia during picture viewing. Psychophysiology2005;42:568–78.
57. Ritz T, Thons M, Dahme B. Effects of erotic picture viewing andexpression of anger on cardiac vagal tone: comparison of three indicesof respiratory sinus arrhythmia [abstract]. Psychophysiology 2004;41:S85.
58. Wenger MA, Jones FN, Jones MH. Physiological Psychology. NewYork: Henry Holt; 1956.
59. Ritz T, Alatupa S, Thons M, Dahme B. Effects of affective pictureviewing and imagery on respiratory resistance in nonasthmatic individ-uals. Psychophysiology 2002;39:86–94.
60. Ritz T, George C, Dahme B. Respiratory resistance during emotionalstimulation: evidence for a nonspecific effect of emotional arousal? BiolPsychol 2000;52:143–60.
61. Boiten FA. The effects of emotional behaviour on components of therespiratory cycle. Biol Psychol 1998;49:29–51.
62. Gomez P, Zimmermann P, Guttormsen-Schar S, Danuser B. Respiratoryresponses associated with affective processing of film stimuli. BiolPsychol 2005;68:223–35.
63. Ritz T, Steptoe A, DeWilde S, Costa M. Emotions and stress increaserespiratory resistance in asthma. Psychosom Med 2000;62:401–12.
64. Knapp PH, Carr HE Jr, Mushatt C, Nemetz SJ. Asthma, melancholia,and death, II: psychosomatic considerations. Psychosom Med 1966;28:134–54.
65. Miller BD. Depression and asthma: a potentially lethal mixture. JAllergy Clin Immunol 1987;80:481–6.
66. Barnes PJ. Neural control of human airways in health and disease. AmRev Respir Dis 1986;134:1289–314.
67. Ritz T, Claussen C, Dahme B. Experimentally induced emotions, facialmuscle activation, and respiratory resistance in asthmatic and nonasth-matic subjects. Br J Med Psychol 2001;74:167–82.
68. McAllen RM, Spyer KM. Two types of vagal preganglionic motoneu-rones projecting to the heart and lungs. J Physiol 1978;282:353–64.
69. McFadden ER, Luparello T, Lyons HA, Bleeker E. The mechanism ofaction of suggestion in the induction of acute asthma attacks. Psycho-som Med 1969;31:134–43.
70. Isenberg SA, Lehrer PM, Hochron S. The effects of suggestion andemotional arousal on pulmonary function in asthma: a review and ahypothesis regarding vagal mediation. Psychosom Med 1992;54:192–216.
71. Giardino ND, Glenny RW, Borson S, Chan L. Respiratory sinus ar-rhythmia is associated with efficiency of pulmonary gas exchange inhealthy humans. Am J Physiol Heart Circ Physiol 2003;284:H1585–91.
72. Hayano J, Yasuma F, Okada A, Mukai S, Fujinami T. Respiratory sinusarrhythmia: a phenomenon improving pulmonary gas exchange andcirculatory efficiency. Circulation 1996;94:842–7.
73. Gianaros PJ, Van Der Veen FM, Jennings JR. Regional cerebral bloodflow correlates with heart period and high-frequency heart period vari-ability during working-memory tasks: implications for the cortical andsubcortical regulation of cardiac autonomic activity. Psychophysiology2004;41:521–30.
74. Kupper N, Willemsen G, Posthuma D, de Boer D, Boomsma DI, deGeus EJ. A genetic analysis of ambulatory cardiorespiratory coupling.Psychophysiology 2005;42:202–12.
75. Asmundson GJ, Stein MB. Vagal attenuation in panic disorder: anassessment of parasympathetic nervous system function and subjectivereactivity to respiratory manipulations. Psychosom Med 1994;56:187–93.
76. Bonnet MH, Arand DL. Heart rate variability in insomniacs andmatched normal sleepers. Psychosom Med 1998;60:610–5.
77. Bosch JA, de Geus EJ, Ligtenberg TJ, Nazmi K, Veerman EC, Hoog-straten J, Amerongen AV. Salivary MUC5B-mediated adherence (exvivo) of Helicobacter pylori during acute stress. Psychosom Med 2000;62:40–9.
78. Bosch JA, de Geus EJ, Veerman EC, Hoogstraten J, Nieuw AmerongenAV. Innate secretory immunity in response to laboratory stressors thatevoke distinct patterns of cardiac autonomic activity. Psychosom Med2003;65:245–58.
79. Burleson MH, Malarkey WB, Cacioppo JT, Poehlmann KM, Kiecolt-Glaser JK, Berntson GG, Glaser R. Postmenopausal hormonereplacement: effects on autonomic, neuroendocrine, and immune reac-tivity to brief psychological stressors. Psychosom Med 1998;60:17–25.
80. Cacioppo JT, Hawkley LC, Crawford LE, Ernst JM, Burleson MH,Kowalewski RB, Malarkey WB, Van Cauter E, Berntson GG. Loneli-
T. RITZ AND B. DAHME
626 Psychosomatic Medicine 68:617–627 (2006)

ness and health: potential mechanisms. Psychosom Med 2002;64:407–17.
81. Cacioppo JT, Malarkey WB, Kiecolt-Glaser JK, Uchino BN, Sgoutas-Emch SA, Sheridan JF, Berntson GG, Glaser R. Heterogeneity inneuroendocrine and immune responses to brief psychological stressorsas a function of autonomic cardiac activation. Psychosom Med 1995;57:154–64.
82. Carney RM, Freedland KE, Stein PK, Watkins LL, Catellier D, JaffeAS, Yeragani VK. Effects of depression on QT interval variability aftermyocardial infarction. Psychosom Med 2003;65:177–80.
83. Carney RM, Freedland KE, Stein PK, Skala JA, Hoffman P, Jaffe AS.Change in heart rate and heart rate variability during treatment fordepression in patients with coronary heart disease. Psychosom Med2000;62:639–47.
84. Elsenbruch S, Lovallo WR, Orr WC. Psychological and physiologicalresponses to postprandial mental stress in women with the irritablebowel syndrome. Psychosom Med 2001;63:805–13.
85. Feldman JM, Lehrer PM, Hochron SM, Schwartz GE. Defensivenessand individual response stereotypy in asthma. Psychosom Med 2002;64:294–301.
86. Fiedler N, Giardino N, Natelson B, Ottenweller JE, Weisel C, Lioy P,Lehrer P, Ohman-Strickland P, Kelly-McNeil K, Kipen H. Responses tocontrolled diesel vapor exposure among chemically sensitive Gulf Warveterans. Psychosom Med 2004;66:588–98.
87. Grossman P, Wilhelm FH, Kawachi I, Sparrow D. Gender differences inpsychophysiological responses to speech stress among older socialphobics: congruence and incongruence between self-evaluative andcardiovascular reactions. Psychosom Med 2001;63:765–77.
88. Hall M, Vasko R, Buysse D, Ombao H, Chen Q, Cashmere JD, KupferD, Thayer JF. Acute stress affects heart rate variability during sleep.Psychosom Med 2004;66:56–62.
89. Haug TT, Svebak S, Hausken T, Wilhelmsen I, Berstad A, Ursin H. Lowvagal activity as mediating mechanism for the relationship betweenpersonality factors and gastric symptoms in functional dyspepsia. Psy-chosom Med 1994;56:181–6.
90. Horsten M, Ericson M, Perski A, Wamala SP, Schenck-Gustafsson K,Orth-Gomer K. Psychosocial factors and heart rate variability in healthywomen. Psychosom Med 1999;61:49–57.
91. Hughes JW, Stoney CM. Depressed mood is related to high-frequencyheart rate variability during stressors. Psychosom Med 2000;62:796–803.
92. Krittayaphong R, Cascio WE, Light KC, Sheffield D, Golden RN,Finkel JB, Glekas G, Koch GG, Sheps DS. Heart rate variability inpatients with coronary artery disease: differences in patients with higherand lower depression scores. Psychosom Med 1997;59:231–23.
93. Laederach-Hofmann K, Mussgay L, Buchel B, Widler P, Ruddel H.Patients with erythrophobia (fear of blushing) show abnormal auto-nomic regulation in mental stress conditions. Psychosom Med 2002;64:358–65.
94. Lehrer PM, Hochron S, Carr R, Edelberg R, Hamer R, Jackson A,Porges S. Behavioral task-induced bronchodilation in asthma duringactive and passive tasks: a possible cholinergic link to psychologicallyinduced airway changes. Psychosom Med 1996;58:413–42.
95. Lehrer P, Sasaki Y, Saito Y. Zazen and cardiac variability. PsychosomMed 1999;61:812–21.
96. Lehrer PM, Vaschillo E, Vaschillo B, Lu SE, Eckberg DL, Edelberg R,Shih WJ, Lin Y, Kuusela TA, Tahvanainen KU, Hamer RM. Heart ratevariability biofeedback increases baroreflex gain and peak expiratoryflow. Psychosom Med 2003;65:796–805.
97. Lucini D, Covacci G, Milani R, Mela GS, Malliani A, Pagani M. Acontrolled study of the effects of mental relaxation on autonomic exci-tatory responses in healthy subjects. Psychosom Med 1997;59:541–52.
98. Matthews KA, Salomon K, Brady SS, Allen MT. Cardiovascular reac-tivity to stress predicts future blood pressure in adolescence. PsychosomMed 2003;65:410–5.
99. Mezzacappa ES, Kelsey RM, Katkin ES, Sloan RP. Vagal rebound andrecovery from psychological stress. Psychosom Med 2001;63:650–7.
100. Muth ER, Koch KL, Stern RM, Thayer JF. Effect of autonomic nervoussystem manipulations on gastric myoelectrical activity and emotionalresponses in healthy human subjects. Psychosom Med 1999;61:297–303.
101. Nakao M, Nomura S, Shimosawa T, Yoshiuchi K, Kumano H, KubokiT, Suematsu H, Fujita T. Clinical effects of blood pressure biofeedbacktreatment on hypertension by auto-shaping. Psychosom Med 1997;59:331–8.
102. Rossy LA, Thayer JF. Fitness and gender-related differences in heartperiod variability. Psychosom Med 1998;60:773–81.
103. Sakakibara M, Hayano J. Effect of slowed respiration on cardiac para-sympathetic response to threat. Psychosom Med 1996;58:32–7.
104. Sato N, Miyake S, Akatsu J, Kumashiro M. Power spectral analysis ofheart rate variability in healthy young women during the normal men-strual cycle. Psychosom Med 1995;57:331–5.
105. Schachinger H, Weinbacher M, Kiss A, Ritz R, Langewitz W. Cardio-vascular indices of peripheral and central sympathetic activation. Psy-chosom Med 2001;63:788–76.
106. Schwarz AM, Schachinger H, Adler RH, Goetz SM. Hopelessness isassociated with decreased heart rate variability during championshipchess games. Psychosom Med 2003;65:658–61.
107. Sloan RP, Bagiella E, Shapiro PA, Kuhl JP, Chernikhova D, Berg J,Myers MM. Hostility, gender, and cardiac autonomic control. Psycho-som Med 2001;63:434–40.
108. Sloan RP, Shapiro PA, Bagiella E, Bigger JT Jr, Lo ES, Gorman JM.Relationships between circulating catecholamines and low frequencyheart period variability as indices of cardiac sympathetic activity duringmental stress. Psychosom Med 1996;58:25–31.
109. Sloan RP, Shapiro PA, Bagiella E, Myers MM, Gorman JM. Cardiacautonomic control buffers blood pressure variability responses tochallenge: a psychophysiologic model of coronary artery disease. Psy-chosom Med 1999;61:58–68.
110. Virtanen R, Jula A, Salminen JK, Voipio-Pulkki LM, Helenius H,Kuusela T, Airaksinen J. Anxiety and hostility are associated withreduced baroreflex sensitivity and increased beat-to-beat blood pressurevariability. Psychosom Med 2003;65:751–6.
111. Watkins LL, Grossman P, Krishnan R, Sherwood A. Anxiety and vagalcontrol of heart rate. Psychosom Med 1998;60:498–502.
112. Watkins LL, Grossman P, Krishnan R, Blumenthal JA. Anxiety reducesbaroreflex cardiac control in older adults with major depression. Psy-chosom Med 1999;61:334–40.
113. Wilhelm FH, Gerlach AL, Roth WT. Slow recovery from voluntaryhyperventilation in panic disorder. Psychosom Med 2001;63:638–49.
RESPIRATORY SINUS ARRHYTHMIA AND RESPIRATION
627Psychosomatic Medicine 68:617–627 (2006)