Embed Size (px)
Citation preview
Articles
866 www.thelancet.com/neurology Vol 9 September 2010
Implementation and outcome of thrombolysis with alteplase 3–4·5 h after an acute stroke: an updated analysis from SITS-ISTRNiaz Ahmed, Nils Wahlgren, Martin Grond, Michael Hennerici, Kennedy R Lees, Robert Mikulik, Mark Parsons, Risto O Roine, Danilo Toni, Peter Ringleb, for the SITS investigators*
Summary Background In September, 2008, the European Acute Stroke Study III (ECASS III) randomised trial and the Safe Implementation of Treatment in Stroke-International Stroke Thrombolysis Registry (SITS-ISTR) observational study reported the effi cacy and safety of the extension of the time window for intravenous alteplase treatment from within 3 h to within 4∙5 h after stroke onset. We aimed to assess the implementation of the wider time window, its eff ect on the admission-to-treatment time, and safety and functional outcome in patients recorded in SITS-ISTR.
Methods Patients treated according to the criteria of the European Summary of Product Characteristics, except for the time window, were included. Patients were grouped according to whether they were registered into SITS-ISTR before or after October, 2008. We measured admission-to-treatment time and rates of symptomatic intracerebral haemorrhage, mortality, and functional independence at 3 months.
Findings 23 942 patients were included in SITS-ISTR between December, 2002, and February, 2010, of whom 2376 were treated 3–4·5 h after symptom onset. The proportion of patients treated within 3–4∙5 h by the end of 2009 was three times higher than in the fi rst three quarters of 2008 (282 of 1293 [22%] vs 67 of 1023 [7%]). The median admission-to-treatment time was 65 min both for patients registered before and after October, 2008 (p=0∙94). 352 (2%) of 21 204 patients treated within 3 h and 52 (2%) of 2317 treated within 3–4∙5 h of stroke had symptomatic intracerebral haemorrhage at 3 months (adjusted odds ratio [OR] 1∙44, 95% CI 1∙05–1∙97; p=0∙02). 2287 (12%) of 18 583 patients who were treated within 3 h and 218 (12%) of 1817 who were treated within 3–4∙5 h had died by the 3-month follow-up (adjusted OR 1∙26, 95% CI 1∙07–1∙49; p=0∙005); 10 531 (57%) of 18 317 patients treated within 3 h of stroke and 1075 (60%) of 1784 who were treated within 3–4·5 h were functionally independent at 3 months (adjusted OR 0∙84, 95% CI 0∙75–0∙95; p=0∙005).
Interpretation Since October, 2008, thrombolysis within 3–4∙5 h after stroke has been implemented rapidly, with a simultaneous increase in the number of patients treated within 3 h; admission-to-treatment time has not increased. Safety and functional outcomes are less favourable after 3 h, but the wider time window now off ers an opportunity for treatment of those patients who cannot be treated earlier. Thrombolysis should be initiated within 4·5 h after onset of ischaemic stroke, although every eff ort should be made to treat patients as early as possible after symptom onset.
Funding Boehringer Ingelheim, Ferrer, the European Union Public Health Executive Authority, and Medical Training and Research (ALF) from Stockholm County Council and Karolinska Institutet.
IntroductionIntravenous thrombolysis with alteplase has been evaluated in randomised controlled trials,1–7 pooled analyses8–10 and safety-monitoring studies.11–14 The early studies1–5 resulted in regulatory approval of intravenous alteplase within 3 h after onset of an ischaemic stroke. In September, 2008, the outcome of the European Acute Stroke Study III (ECASS III) randomised controlled trial6 and the Safe Implementation of Treatment in Stroke-International Stroke Thrombolysis Registry (SITS-ISTR)14 observational study provided evidence supporting an expansion of the alteplase treatment time window up to 4∙5 h after stroke onset. On the basis of these studies, the European Stroke Organisation changed the guidelines for management of acute ischaemic stroke and transient ischaemic attack.15,16 The American Heart Association and
the American Stroke Association subsequently published a Science Advisory on the same topic,17 and now both these European and US organisations recommend use of intravenous alteplase within 4∙5 h after stroke onset.16,17
Although more patients should receive alteplase treatment because of the increased time window for thrombolysis, the investigators in the ECASS III6 and the SITS-ISTR14 studies were concerned that the increased time window would result in an increased delay from admission of patients with stroke at the emergency department to the start of alteplase treatment. This would be a negative eff ect of the prolonged time window because treatment benefi t declines with time.8 SITS-ISTR14 reported a possible increase in symptomatic intracerebral haemorrhage (according to the SITS-Monitoring Study [SITS-MOST] defi nition12) (p=0∙052) and mortality rates
Lancet Neurol 2010; 9: 866–74
Published OnlineJuly 27, 2010
DOI:10.1016/S1474-4422(10)70165-4
Refl ection and Reactionpage 843
*Scientifi c committee listed at end of paper
Department of Neurology, Karolinska University Hospital,
and Department of Clinical Neurosciences, Karolinska
Institutet, Stockholm, Sweden (N Ahmed MD,
Prof N Wahlgren MD); Department of Neurology, Kreiskrankenhaus Siegen,
Siegen, Germany (Prof M Grond MD); Department
of Neurology, University of Heidelberg, Mannheim,
Germany (Prof M Hennerici MD); Department of Neurology,
University of Heidelberg, Heidelberg, Germany
(P Ringleb MD); Department of Medicine and Therapeutics,
Gardiner Institutet, University of Glasgow, Glasgow, UK
(Prof K R Lees FRCP); Neurology Department, International
Clinical Research Center, St Anne’s Hospital, Brno, Czech
Republic (R Mikulik MD); John Hunter Hospital, New South
Wales, Australia (M Parsons FRACP); Department of Neurology, Turku University
Hospital, Turku, Finland (Prof R O Roine MD); and
Department of Neurology, Department of Neurological
Sciences, La Sapienza University Hospital, Rome,
Italy (Prof D Toni MD)
Correspondence to:Prof Nils Wahlgren, SITS
International Coordination Offi ce, Karolinska Stroke
Research, Department of Neurology, Karolinska
University Hospital, Solna, SE-171 76 Stockholm, [email protected]

Articles
www.thelancet.com/neurology Vol 9 September 2010 867
(p=0∙053) with late (3–4∙5 h) compared with early (<3 h) treatment with alteplase. In addition, a possible increase in mortality rates was reported in a pooled analysis.9
We therefore aimed to assess the implementation of the prolonged time window for thrombolysis with alteplase after September, 2008, to investigate whether the increased time window has resulted in prolongation of admission-to-treatment time, and to evaluate treatment safety and functional outcome in a large patient cohort of the SITS registry.
MethodsStudy population650 centres in Europe, Asia, and Australia participated in the study from December, 2002 to February, 2010. Patients were included if they presented with ischaemic stroke and were treated with intravenous alteplase (Actilyse, Boehringer-Ingelheim, Ingelheim, Germany) within 4∙5 h after symptom onset. Patients were compliant with the European Summary of Product Characteristics criteria (see webappendix p 1), except for the time since stroke onset (per-protocol group). A full dose of alteplase was defi ned as 0∙9 mg/kg (with an upper limit of 90 mg) given as a continuous infusion over 60 min, with 10% of the total dose given as a bolus.
The need for ethical approval or patient consent for participation in the SITS-ISTR varied among participating countries, but ethics approval and patient consent were obtained in countries that required this; other countries approved the register for conduct as an anonymised audit. SITS-MOST was approved by the Ethics Committee of the Karolinska Institutet in Stockholm, Sweden, as well as by the Swedish Medical Products Agency.
ProceduresDetails of the methods, including data collection and management for SITS-ISTR and SITS-MOST have been described previously.12 In brief, SITS-ISTR is a prospective, multinational, internet-based register of patients treated with alteplase after acute ischaemic stroke. SITS-ISTR is an ongoing review and contains data about alteplase treatment independent of the time since stroke onset.
We documented demographics and baseline characteristics, stroke severity (measured by National Institutes of Health stroke scale [NIHSS] score14), onset-to-treatment time, risk factors, drug treatment history, admission time, and data from baseline and follow-up imaging scans. The NIHSS records the amount of neurological defi cit on an ordinal scale (range 0–42, with 0 representing normal neurological function). Although SITS-ISTR encourages the NIHSS to be done by certifi ed users, it is not possible to ensure that assessments were done by certifi ed examiners.
To assess the impact of the ECASS III and the SITS-ISTR study results on implementation of alteplase within 3–4·5 h, all patients compliant with the European Summary of Product Characteristics were included.
Patients were separated according to the month of their treatment and were grouped by quartile. We then calculated the absolute numbers of patients treated within 3–4∙5 h and those treated within 3 h before and after Oct 1, 2008.
We compared admission-to-treatment time between patients registered from Oct 1, 2008, to Feb 28, 2010, and those registered from Jan 1, 2007, to May 30, 2008. The period between June and September, 2008, was excluded because some individuals knew the outcome of ECASS III, which could have infl uenced the outcome of a comparison. We also calculated admission-to-treatment time for each 30-min interval of the time between symptom onset and hospital admission. We categorised the time between stroke symptom onset and hospital admission by 30-min intervals (from 30 min to 180 min) and examined the median hospital admission-to-treatment time for each 30-min category before and after October, 2008.
To investigate the eff ect of the extended time window on symptomatic intracerebral haemorrhage, mortality, and functional outcome at 3 months, we included all per-protocol patients registered in SITS-ISTR between December, 2002, and February, 2010. We calculated the proportion of patients who had symptomatic intracerebral haemorrhage, who died, and who were functionally independent, and calculated corresponding unadjusted and adjusted odds ratios for patients treated within 3–4∙5 h and those treated within 3 h. We used the same primary defi nition of symptomatic intracerebral haemorrhage as in SITS-MOST:12 a local or remote type 2 parenchymal haemorrhage on imaging 22–36 h after treatment, combined with a neurological deterioration of 4 or more points on the NIHSS from baseline or from the lowest NIHSS score between baseline and 24 h, or leading to death. A grading of type 2 parenchymal haemorrhage for intracranial haemorrhage indicates a blood clot exceeding 30% of the infarct area, with substantial space occupation—ie, a clot large enough to result in increased pressure on the adjacent intact brain region.
In addition to the SITS-MOST defi nition, we used two more defi nitions of symptomatic intracerebral haemorrhage to enable comparisons with other published data: the National Institute of Neurological Disorders and Stroke (NINDS) defi nition—any intracranial haemorrhage on post-thrombolysis imaging that was not seen on a previous imaging scan and any decline in neurological status; and the ECASS II defi nition—any form of intracerebral haemorrhage and increase of four or more points on the NIHSS. All assessments of imaging studies and neurological status were done according to clinical routine at the local centres. All deaths within 3 months were included and the cause of death was reported. For functional outcomes, a modifi ed Rankin scale (mRS) score of 2 or less at 3 months indicated functional independence and a mRS score of 1 or less at 3 months indicated minimal or no disability.
See Online for webappendix
For more information on the SITS-ISTR see https://sitsinternational.org/
Articles
868 www.thelancet.com/neurology Vol 9 September 2010
Statistical analysisWe used descriptive statistics for baseline and demographic data for patients treated with intravenous alteplase between 3 and 4∙5 h compared with those treated within 3 h. For categorical variables, we calculated percentage proportions by dividing the number of events by the total number of patients, excluding missing or unknown cases. For calculation of a signifi cant diff erence between proportions, we used the χ² method and for medians the Mann-Whitney U test.
We also did a multivariate analysis to identify any diff erence in outcome parameters between patients treated within 3 h versus 3–4∙5 h, after adjusting for the variables that were signifi cant at the 25% level. The following variables were included in the multivariate model: age, sex, hyperlipidaemia, atrial fi brillation, minimal or no disability before present stroke (measured by mRS 0–1), smoking, baseline NIHSS score, baseline blood glucose, baseline diastolic blood pressure, and signs of infarction on baseline imaging. Multivariate analyses were done using generalised linear or non-linear models, and estimated odds ratios were calculated by logistic regression. We did all analyses using STATISTICA software version 9.1.
The SITS International Coordination Offi ce did regular online monitoring of the SITS-ISTR data and checked individual patient data monthly to identify errors or inconsistencies. For a sample of patients included in SITS-MOST (n=6483), source data were verifi ed onsite by monitors under the supervision of the relevant national coordinator.
Role of the funding sourceThe study sponsors had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. NW and NA had full access to all the data in this study and had the fi nal responsibility for the decision to submit for publication. NW and NA vouch for the accuracy and completeness of this report.
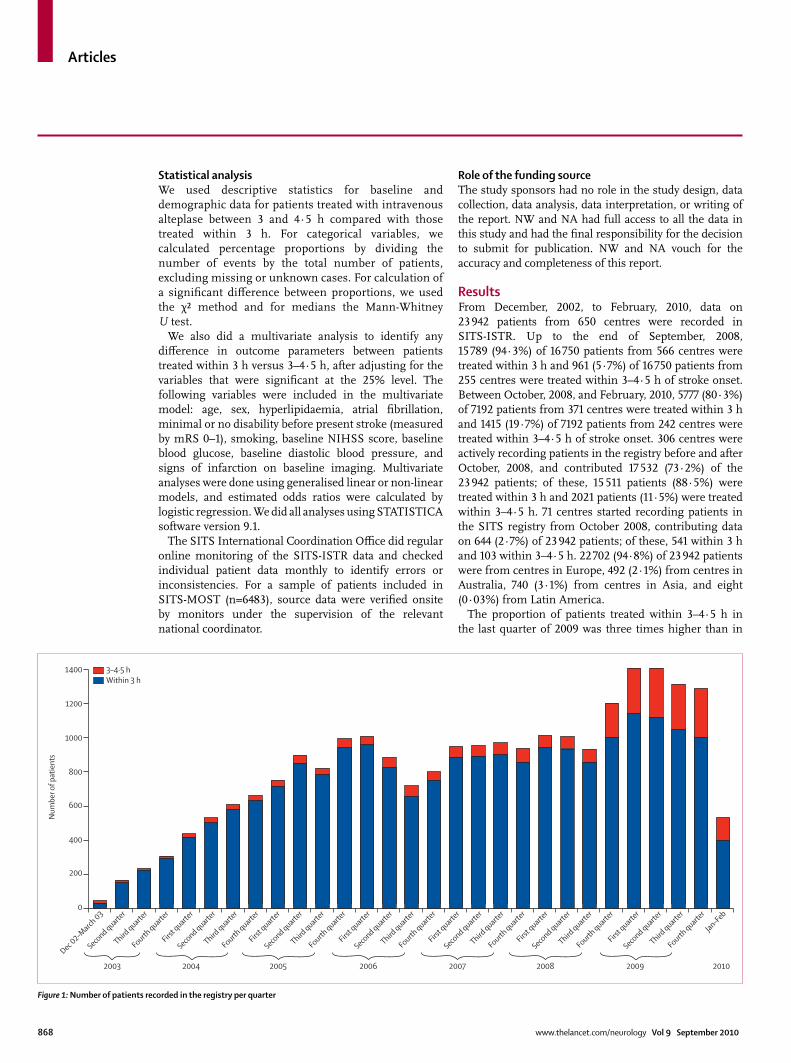
ResultsFrom December, 2002, to February, 2010, data on 23 942 patients from 650 centres were recorded in SITS-ISTR. Up to the end of September, 2008, 15 789 (94∙3%) of 16 750 patients from 566 centres were treated within 3 h and 961 (5∙7%) of 16 750 patients from 255 centres were treated within 3–4∙5 h of stroke onset. Between October, 2008, and February, 2010, 5777 (80∙3%) of 7192 patients from 371 centres were treated within 3 h and 1415 (19∙7%) of 7192 patients from 242 centres were treated within 3–4∙5 h of stroke onset. 306 centres were actively recording patients in the registry before and after October, 2008, and contributed 17 532 (73·2%) of the 23 942 patients; of these, 15 511 patients (88·5%) were treated within 3 h and 2021 patients (11·5%) were treated within 3–4∙5 h. 71 centres started recording patients in the SITS registry from October 2008, contributing data on 644 (2·7%) of 23 942 patients; of these, 541 within 3 h and 103 within 3–4∙5 h. 22 702 (94·8%) of 23 942 patients were from centres in Europe, 492 (2·1%) from centres in Australia, 740 (3·1%) from centres in Asia, and eight (0·03%) from Latin America.
The proportion of patients treated within 3–4∙5 h in the last quarter of 2009 was three times higher than in
Figure 1: Number of patients recorded in the registry per quarter
Dec 02–M
arch 03
Second quarte
r
Third quarte
r
Fourth quarte
r
2003
First q
uarter
Second quarte
r
Third quarte
r
Fourth quarte
r
2004
First q
uarter
Second quarte
r
Third quarte
r
Fourth quarte
r
2005
First q
uarter
Second quarte
r
Third quarte
r
Fourth quarte
r
2006
First q
uarter
Second quarte
r
Third quarte
r
Fourth quarte
r
2007
First q
uarter
Second quarte
r
Third quarte
r
Fourth quarte
r
2008
First q
uarter
Jan–Feb
Second quarte
r
Third quarte
r
Fourth quarte
r
2009 2010
0
200
400
600
800
Num
ber o
f pat
ient
s
1000
1200
1400 3–4·5 hWithin 3 h
Articles
www.thelancet.com/neurology Vol 9 September 2010 869
the fi rst quarter of 2008 (282 of 1293 [22%] vs 67 of 1023 [7%]; fi gure 1).
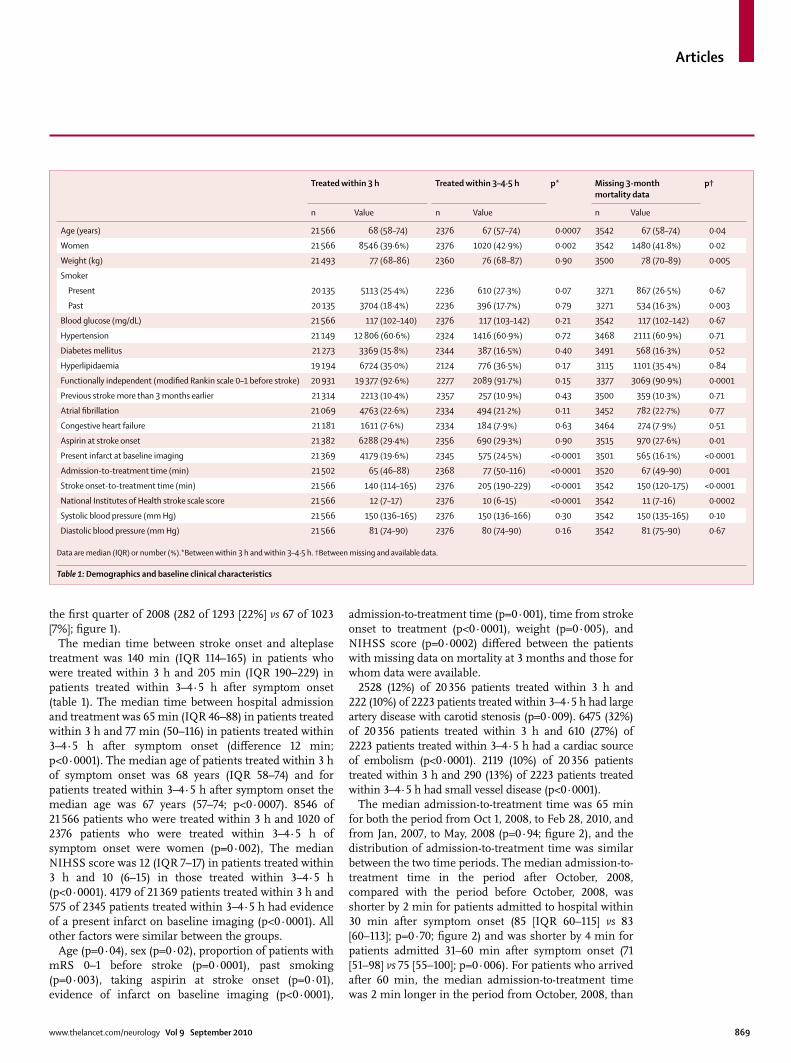
The median time between stroke onset and alteplase treatment was 140 min (IQR 114–165) in patients who were treated within 3 h and 205 min (IQR 190–229) in patients treated within 3–4∙5 h after symptom onset (table 1). The median time between hospital admission and treatment was 65 min (IQR 46–88) in patients treated within 3 h and 77 min (50–116) in patients treated within 3–4·5 h after symptom onset (diff erence 12 min; p<0·0001). The median age of patients treated within 3 h of symptom onset was 68 years (IQR 58–74) and for patients treated within 3–4·5 h after symptom onset the median age was 67 years (57–74; p<0·0007). 8546 of 21 566 patients who were treated within 3 h and 1020 of 2376 patients who were treated within 3–4·5 h of symptom onset were women (p=0·002), The median NIHSS score was 12 (IQR 7–17) in patients treated within 3 h and 10 (6–15) in those treated within 3–4·5 h (p<0·0001). 4179 of 21 369 patients treated within 3 h and 575 of 2345 patients treated within 3–4·5 h had evidence of a present infarct on baseline imaging (p<0∙0001). All other factors were similar between the groups.
Age (p=0·04), sex (p=0·02), proportion of patients with mRS 0–1 before stroke (p=0·0001), past smoking (p=0·003), taking aspirin at stroke onset (p=0·01), evidence of infarct on baseline imaging (p<0·0001),
admission-to-treatment time (p=0·001), time from stroke onset to treatment (p<0·0001), weight (p=0·005), and NIHSS score (p=0·0002) diff ered between the patients with missing data on mortality at 3 months and those for whom data were available.
2528 (12%) of 20 356 patients treated within 3 h and 222 (10%) of 2223 patients treated within 3–4·5 h had large artery disease with carotid stenosis (p=0∙009). 6475 (32%) of 20 356 patients treated within 3 h and 610 (27%) of 2223 patients treated within 3–4·5 h had a cardiac source of embolism (p<0∙0001). 2119 (10%) of 20 356 patients treated within 3 h and 290 (13%) of 2223 patients treated within 3–4∙5 h had small vessel disease (p<0∙0001).
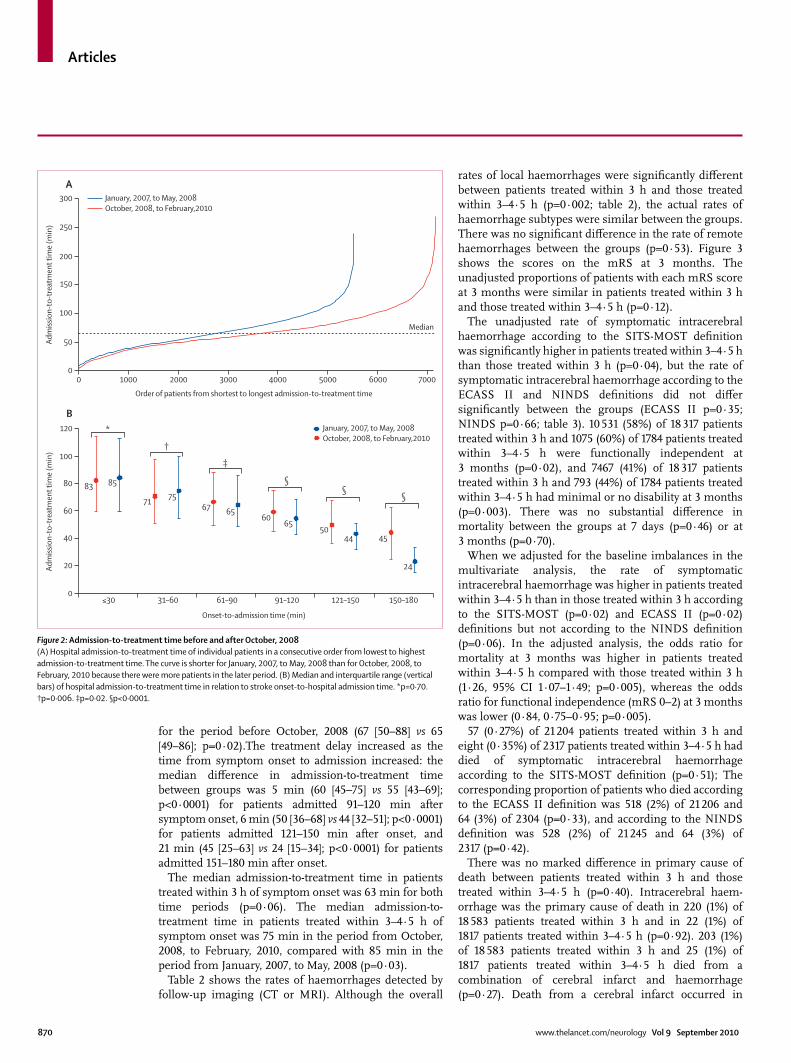
The median admission-to-treatment time was 65 min for both the period from Oct 1, 2008, to Feb 28, 2010, and from Jan, 2007, to May, 2008 (p=0∙94; fi gure 2), and the distribution of admission-to-treatment time was similar between the two time periods. The median admission-to-treatment time in the period after October, 2008, compared with the period before October, 2008, was shorter by 2 min for patients admitted to hospital within 30 min after symptom onset (85 [IQR 60–115] vs 83 [60–113]; p=0·70; fi gure 2) and was shorter by 4 min for patients admitted 31–60 min after symptom onset (71 [51–98] vs 75 [55–100]; p=0·006). For patients who arrived after 60 min, the median admission-to-treatment time was 2 min longer in the period from October, 2008, than
Treated within 3 h Treated within 3–4·5 h p* Missing 3-month mortality data
p†
n Value n Value n Value
Age (years) 21 566 68 (58–74) 2376 67 (57–74) 0·0007 3542 67 (58–74) 0·04
Women 21 566 8546 (39·6%) 2376 1020 (42·9%) 0·002 3542 1480 (41·8%) 0·02
Weight (kg) 21 493 77 (68–86) 2360 76 (68–87) 0·90 3500 78 (70–89) 0·005
Smoker
Present 20 135 5113 (25·4%) 2236 610 (27·3%) 0·07 3271 867 (26·5%) 0·67
Past 20 135 3704 (18·4%) 2236 396 (17·7%) 0·79 3271 534 (16·3%) 0·003
Blood glucose (mg/dL) 21 566 117 (102–140) 2376 117 (103–142) 0·21 3542 117 (102–142) 0·67
Hypertension 21 149 12 806 (60·6%) 2324 1416 (60·9%) 0·72 3468 2111 (60·9%) 0·71
Diabetes mellitus 21 273 3369 (15·8%) 2344 387 (16·5%) 0·40 3491 568 (16·3%) 0·52
Hyperlipidaemia 19 194 6724 (35·0%) 2124 776 (36·5%) 0·17 3115 1101 (35·4%) 0·84
Functionally independent (modifi ed Rankin scale 0–1 before stroke) 20 931 19 377 (92·6%) 2277 2089 (91·7%) 0·15 3377 3069 (90·9%) 0·0001
Previous stroke more than 3 months earlier 21 314 2213 (10·4%) 2357 257 (10·9%) 0·43 3500 359 (10·3%) 0·71
Atrial fi brillation 21 069 4763 (22·6%) 2334 494 (21·2%) 0·11 3452 782 (22·7%) 0·77
Congestive heart failure 21 181 1611 (7·6%) 2334 184 (7·9%) 0·63 3464 274 (7·9%) 0·51
Aspirin at stroke onset 21 382 6288 (29·4%) 2356 690 (29·3%) 0·90 3515 970 (27·6%) 0·01
Present infarct at baseline imaging 21 369 4179 (19·6%) 2345 575 (24·5%) <0·0001 3501 565 (16·1%) <0·0001
Admission-to-treatment time (min) 21 502 65 (46–88) 2368 77 (50–116) <0·0001 3520 67 (49–90) 0·001
Stroke onset-to-treatment time (min) 21 566 140 (114–165) 2376 205 (190–229) <0·0001 3542 150 (120–175) <0·0001
National Institutes of Health stroke scale score 21 566 12 (7–17) 2376 10 (6–15) <0·0001 3542 11 (7–16) 0·0002
Systolic blood pressure (mm Hg) 21 566 150 (136–165) 2376 150 (136–166) 0·30 3542 150 (135–165) 0·10
Diastolic blood pressure (mm Hg) 21 566 81 (74–90) 2376 80 (74–90) 0·16 3542 81 (75–90) 0·67
Data are median (IQR) or number (%).*Between within 3 h and within 3–4·5 h. †Between missing and available data.
Table 1: Demographics and baseline clinical characteristics
Articles
870 www.thelancet.com/neurology Vol 9 September 2010
for the period before October, 2008 (67 [50–88] vs 65 [49–86]; p=0·02).The treatment delay increased as the time from symptom onset to admission increased: the median diff erence in admission-to-treatment time between groups was 5 min (60 [45–75] vs 55 [43–69]; p<0·0001) for patients admitted 91–120 min after symptom onset, 6 min (50 [36–68] vs 44 [32–51]; p<0·0001) for patients admitted 121–150 min after onset, and 21 min (45 [25–63] vs 24 [15–34]; p<0·0001) for patients admitted 151–180 min after onset.
The median admission-to-treatment time in patients treated within 3 h of symptom onset was 63 min for both time periods (p=0·06). The median admission-to-treatment time in patients treated within 3–4·5 h of symptom onset was 75 min in the period from October, 2008, to February, 2010, compared with 85 min in the period from January, 2007, to May, 2008 (p=0·03).
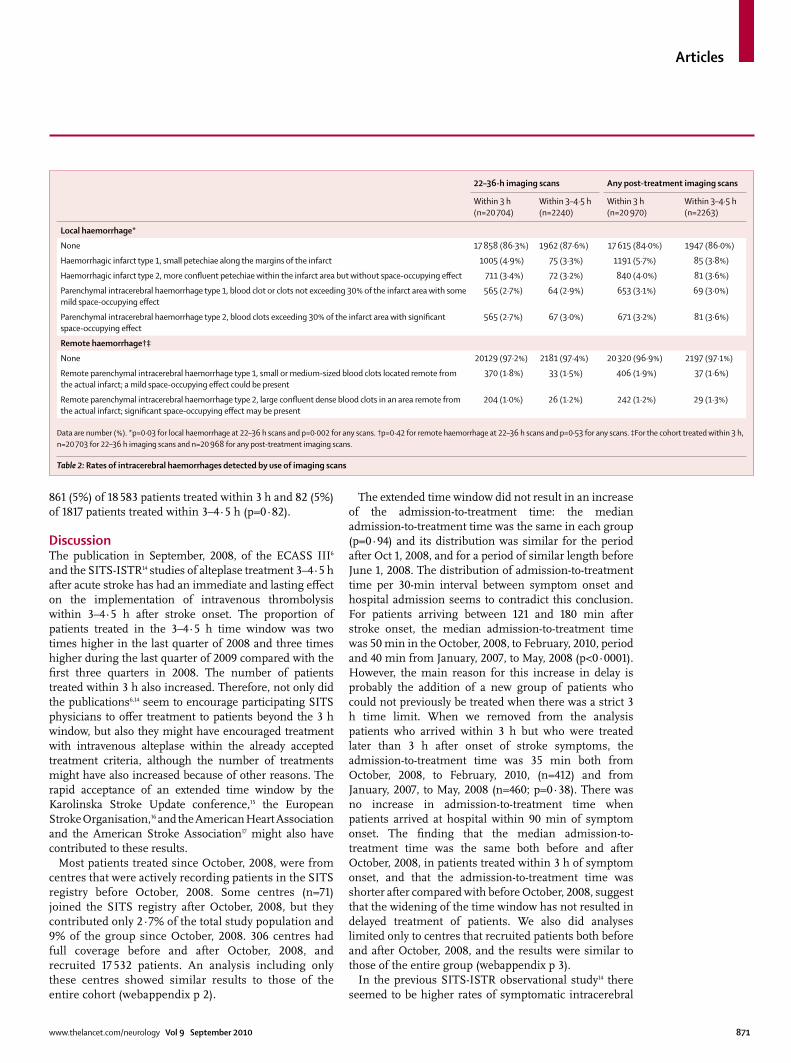
Table 2 shows the rates of haemorrhages detected by follow-up imaging (CT or MRI). Although the overall
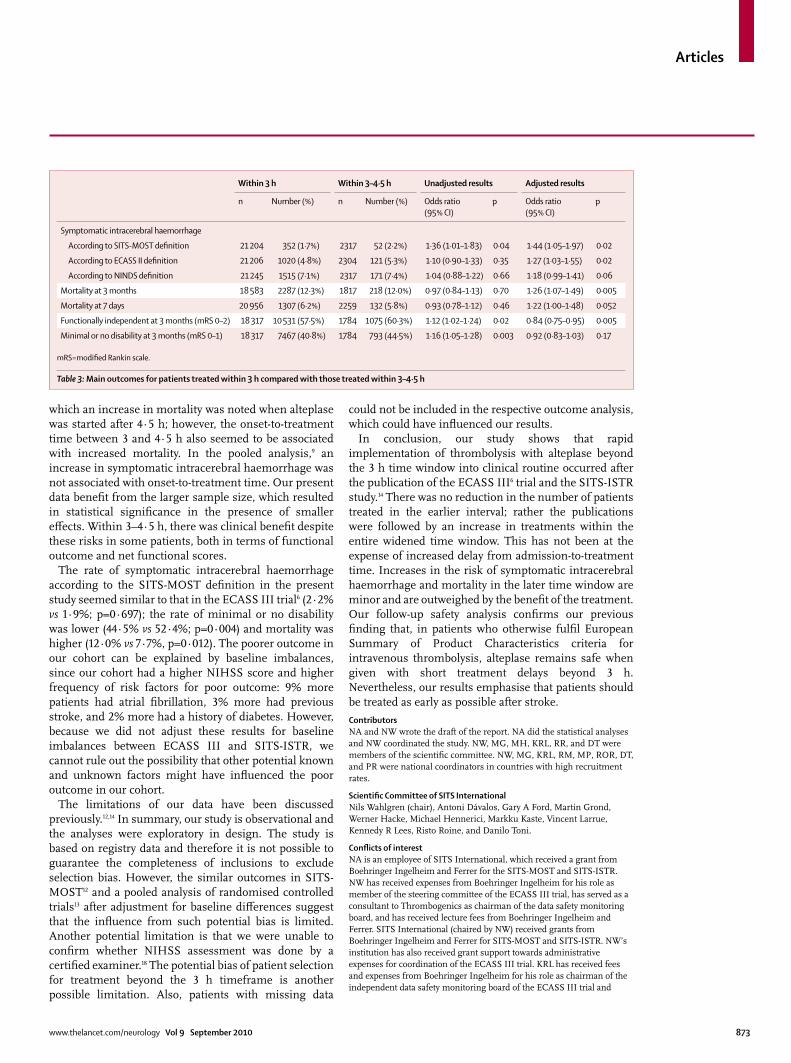
rates of local haemorrhages were signifi cantly diff erent between patients treated within 3 h and those treated within 3–4∙5 h (p=0·002; table 2), the actual rates of haemorrhage subtypes were similar between the groups. There was no signifi cant diff erence in the rate of remote haemorrhages between the groups (p=0·53). Figure 3 shows the scores on the mRS at 3 months. The unadjusted proportions of patients with each mRS score at 3 months were similar in patients treated within 3 h and those treated within 3–4·5 h (p=0·12).
The unadjusted rate of symptomatic intracerebral haemorrhage according to the SITS-MOST defi nition was signifi cantly higher in patients treated within 3–4·5 h than those treated within 3 h (p=0·04), but the rate of symptomatic intracerebral haemorrhage according to the ECASS II and NINDS defi nitions did not diff er signifi cantly between the groups (ECASS II p=0·35; NINDS p=0·66; table 3). 10 531 (58%) of 18 317 patients treated within 3 h and 1075 (60%) of 1784 patients treated within 3–4·5 h were functionally independent at 3 months (p=0·02), and 7467 (41%) of 18 317 patients treated within 3 h and 793 (44%) of 1784 patients treated within 3–4·5 h had minimal or no disability at 3 months (p=0·003). There was no substantial diff erence in mortality between the groups at 7 days (p=0·46) or at 3 months (p=0∙70).
When we adjusted for the baseline imbalances in the multivariate analysis, the rate of symptomatic intracerebral haemorrhage was higher in patients treated within 3–4·5 h than in those treated within 3 h according to the SITS-MOST (p=0·02) and ECASS II (p=0·02) defi nitions but not according to the NINDS defi nition (p=0·06). In the adjusted analysis, the odds ratio for mortality at 3 months was higher in patients treated within 3–4·5 h compared with those treated within 3 h (1·26, 95% CI 1·07–1·49; p=0·005), whereas the odds ratio for functional independence (mRS 0–2) at 3 months was lower (0·84, 0·75–0·95; p=0·005).
57 (0∙27%) of 21 204 patients treated within 3 h and eight (0∙35%) of 2317 patients treated within 3–4∙5 h had died of symptomatic intracerebral haemorrhage according to the SITS-MOST defi nition (p=0∙51); The corresponding proportion of patients who died according to the ECASS II defi nition was 518 (2%) of 21 206 and 64 (3%) of 2304 (p=0∙33), and according to the NINDS defi nition was 528 (2%) of 21 245 and 64 (3%) of 2317 (p=0∙42).
There was no marked diff erence in primary cause of death between patients treated within 3 h and those treated within 3–4∙5 h (p=0∙40). Intracerebral haem-orrhage was the primary cause of death in 220 (1%) of 18 583 patients treated within 3 h and in 22 (1%) of 1817 patients treated within 3–4∙5 h (p=0∙92). 203 (1%) of 18 583 patients treated within 3 h and 25 (1%) of 1817 patients treated within 3–4∙5 h died from a combination of cerebral infarct and haemorrhage (p=0∙27). Death from a cerebral infarct occurred in
Figure 2: Admission-to-treatment time before and after October, 2008(A) Hospital admission-to-treatment time of individual patients in a consecutive order from lowest to highest admission-to-treatment time. The curve is shorter for January, 2007, to May, 2008 than for October, 2008, to February, 2010 because there were more patients in the later period. (B) Median and interquartile range (vertical bars) of hospital admission-to-treatment time in relation to stroke onset-to-hospital admission time. *p=0·70. †p=0·006. ‡p=0·02. §p<0·0001.
0
0
20
40
60
80
100
120
50
Median
0 1000
≤30
83
†‡
§§ §
*
85
71 7567 65
6050
44 45
24
65
31–60 61–90 91–120 121–150 150–180
2000 3000 4000
Order of patients from shortest to longest admission-to-treatment time
Onset-to-admission time (min)
5000 6000 7000
Adm
issio
n-to
-tre
atm
ent t
ime
(min
)Ad
miss
ion-
to-t
reat
men
t tim
e (m
in)
100
150
200
250
300
A
B
January, 2007, to May, 2008October, 2008, to February,2010
January, 2007, to May, 2008October, 2008, to February,2010
Articles
www.thelancet.com/neurology Vol 9 September 2010 871
861 (5%) of 18 583 patients treated within 3 h and 82 (5%) of 1817 patients treated within 3–4∙5 h (p=0∙82).
DiscussionThe publication in September, 2008, of the ECASS III6 and the SITS-ISTR14 studies of alteplase treatment 3–4∙5 h after acute stroke has had an immediate and lasting eff ect on the implementation of intravenous thrombolysis within 3–4∙5 h after stroke onset. The proportion of patients treated in the 3–4·5 h time window was two times higher in the last quarter of 2008 and three times higher during the last quarter of 2009 compared with the fi rst three quarters in 2008. The number of patients treated within 3 h also increased. Therefore, not only did the publications6,14 seem to encourage participating SITS physicians to off er treatment to patients beyond the 3 h window, but also they might have encouraged treatment with intravenous alteplase within the already accepted treatment criteria, although the number of treatments might have also increased because of other reasons. The rapid acceptance of an extended time window by the Karolinska Stroke Update conference,15 the European Stroke Organisation,16 and the American Heart Association and the American Stroke Association17 might also have contributed to these results.
Most patients treated since October, 2008, were from centres that were actively recording patients in the SITS registry before October, 2008. Some centres (n=71) joined the SITS registry after October, 2008, but they contributed only 2·7% of the total study population and 9% of the group since October, 2008. 306 centres had full coverage before and after October, 2008, and recruited 17 532 patients. An analysis including only these centres showed similar results to those of the entire cohort (webappendix p 2).
The extended time window did not result in an increase of the admission-to-treatment time: the median admission-to-treatment time was the same in each group (p=0·94) and its distribution was similar for the period after Oct 1, 2008, and for a period of similar length before June 1, 2008. The distribution of admission-to-treatment time per 30-min interval between symptom onset and hospital admission seems to contradict this conclusion. For patients arriving between 121 and 180 min after stroke onset, the median admission-to-treatment time was 50 min in the October, 2008, to February, 2010, period and 40 min from January, 2007, to May, 2008 (p<0∙0001). However, the main reason for this increase in delay is probably the addition of a new group of patients who could not previously be treated when there was a strict 3 h time limit. When we removed from the analysis patients who arrived within 3 h but who were treated later than 3 h after onset of stroke symptoms, the admission-to-treatment time was 35 min both from October, 2008, to February, 2010, (n=412) and from January, 2007, to May, 2008 (n=460; p=0∙38). There was no increase in admission-to-treatment time when patients arrived at hospital within 90 min of symptom onset. The fi nding that the median admission-to-treatment time was the same both before and after October, 2008, in patients treated within 3 h of symptom onset, and that the admission-to-treatment time was shorter after compared with before October, 2008, suggest that the widening of the time window has not resulted in delayed treatment of patients. We also did analyses limited only to centres that recruited patients both before and after October, 2008, and the results were similar to those of the entire group (webappendix p 3).
In the previous SITS-ISTR observational study14 there seemed to be higher rates of symptomatic intracerebral
22–36-h imaging scans Any post-treatment imaging scans
Within 3 h (n=20 704)
Within 3–4·5 h (n=2240)
Within 3 h (n=20 970)
Within 3–4·5 h (n=2263)
Local haemorrhage*
None 17 858 (86·3%) 1962 (87·6%) 17 615 (84·0%) 1947 (86·0%)
Haemorrhagic infarct type 1, small petechiae along the margins of the infarct 1005 (4·9%) 75 (3·3%) 1191 (5·7%) 85 (3·8%)
Haemorrhagic infarct type 2, more confl uent petechiae within the infarct area but without space-occupying eff ect 711 (3·4%) 72 (3·2%) 840 (4·0%) 81 (3·6%)
Parenchymal intracerebral haemorrhage type 1, blood clot or clots not exceeding 30% of the infarct area with some mild space-occupying eff ect
565 (2·7%) 64 (2·9%) 653 (3·1%) 69 (3·0%)
Parenchymal intracerebral haemorrhage type 2, blood clots exceeding 30% of the infarct area with signifi cant space-occupying eff ect
565 (2·7%) 67 (3·0%) 671 (3·2%) 81 (3·6%)
Remote haemorrhage†‡
None 20129 (97·2%) 2181 (97·4%) 20 320 (96·9%) 2197 (97·1%)
Remote parenchymal intracerebral haemorrhage type 1, small or medium-sized blood clots located remote from the actual infarct; a mild space-occupying eff ect could be present
370 (1·8%) 33 (1·5%) 406 (1·9%) 37 (1·6%)
Remote parenchymal intracerebral haemorrhage type 2, large confl uent dense blood clots in an area remote from the actual infarct; signifi cant space-occupying eff ect may be present
204 (1·0%) 26 (1·2%) 242 (1·2%) 29 (1·3%)
Data are number (%). *p=0·03 for local haemorrhage at 22–36 h scans and p=0·002 for any scans. †p=0·42 for remote haemorrhage at 22–36 h scans and p=0·53 for any scans. ‡For the cohort treated within 3 h, n=20 703 for 22–36 h imaging scans and n=20 968 for any post-treatment imaging scans.
Table 2: Rates of intracerebral haemorrhages detected by use of imaging scans

Articles
872 www.thelancet.com/neurology Vol 9 September 2010
haemorrhage according to the SITS-MOST defi nition (p=0∙052) and mortality within 3 months (p=0∙053) in patients treated within 3–4∙5 h compared with those treated within 3 h. In the present study—in which more patients were treated within 3–4∙5 h (n=2376) than in our previous study (n=664)—after adjusting for confounding variables, the rates of symptomatic intracerebral haemorrhage according to the SITS-MOST defi nition and mortality at 3 months were higher in patients treated within 3–4∙5 h than in patients treated within 3 h. In unadjusted analyses, more patients treated within 3–4∙5 h had functional independence and minimal or no disability than patients treated within 3 h, but when we adjusted for baseline imbalances, the outcome seemed to favour treatment within 3 h rather than treatment within 3–4∙5 h. This shift can be explained by the lower median NIHSS score and the younger population of patients treated within 3–4∙5-h than those treated within 3 h. By contrast, more patients treated within 3–4∙5 h than those treated within 3 h had signs of present infarction, which is a known predictor of symptomatic intracerebral haemorrhage and poor outcome. Although after
adjustment, patients treated within 3–4∙5 h had higher symptomatic intracerebral haemorrhage and mortality rates and worse functional outcome than patients treated within 3 h, the overall proportion of these outcomes was still low in the cohort treated within 3–4∙5 h and the statistical signifi cance can probably be explained by the large sample size. The unadjusted outcomes in patients treated within 3–4∙5 h compared with those treated within 3 h in randomised controlled trials1–3,5,8,12 are similar or even better: symptomatic intracerebral haemorrhage according to the NINDS defi nition was 7∙4% versus 8∙6% (p=0∙36); mortality within 3 months was 12∙0% versus 17∙3% (p=0∙002); and functional independence at 3 months was 60∙3% versus 50∙1% (p=0∙0001). Nonetheless, stroke onset-to-treatment time should be regarded as one of the most important contributing factors for favourable outcome, and the statistical signifi cance is a warning for clinicians that treatment should not be delayed even though we now have an extended time window.
The present fi ndings are confi rmed by the updated pooled analysis of randomised controlled trial data,9 in
Figure 3: Modifi ed Rankin scale scores at 3 monthsComparison of unadjusted mRS score at 3 months between patients treated within 3–4·5 h and within 3 h stratifi ed by baseline NIHSS score. Percentages do not add up to 100% in some cases because of rounding. mRS=modifi ed Rankin scale. NIHSS=National Institutes of Health Stroke scale.
0 1 2 3 4 5 6
All patients treatedwithin 3–4·5 h (n=1784)
All patients treatedwithin 3 h (n=18 317)
NIHSS score ≤5,within 3–4·5 h (n=372)
NIHSS score ≤5,within 3 h (n=2284)
NIHSS score 6–10,within 3–4·5 h (n=593)
NIHSS score 11–15,within 3–4·5 h (n=394)
NIHSS score 16–20,within 3–4·5 h (n=312)
NIHSS score 21–25,within 3–4·5 h (n=113)
NIHSS score 16–20,within 3 h (n=4197)
NIHSS score 21–25,within 3 h (n=1839)
NIHSS score 6–10,within 3 h (n=5558)
NIHSS score 11–15,within 3 h (n=4439)
mRS score
0 20 40 60
Patients (%)
22 22 16 12 11 5 12
20 20 17 13 12 5 12
41 31 15 4 45
40 31 17 6 3 3
30 27 18 11 6 1 6
30 28 20 11 6 2 5
10 21 19 17 13 7 13
17 19 19 16 13 5 12
9 10 12 16 23 9 22
8 12 13 17 21 218
2 4 9 10 22 13 40
4 7 11 16 19 12 31
80 100
Articles
www.thelancet.com/neurology Vol 9 September 2010 873
which an increase in mortality was noted when alteplase was started after 4∙5 h; however, the onset-to-treatment time between 3 and 4∙5 h also seemed to be associated with increased mortality. In the pooled analysis,9 an increase in symptomatic intracerebral haemorrhage was not associated with onset-to-treatment time. Our present data benefi t from the larger sample size, which resulted in statistical signifi cance in the presence of smaller eff ects. Within 3–4∙5 h, there was clinical benefi t despite these risks in some patients, both in terms of functional outcome and net functional scores.
The rate of symptomatic intracerebral haemorrhage according to the SITS-MOST defi nition in the present study seemed similar to that in the ECASS III trial6 (2·2% vs 1·9%; p=0∙697); the rate of minimal or no disability was lower (44∙5% vs 52∙4%; p=0∙004) and mortality was higher (12∙0% vs 7∙7%, p=0∙012). The poorer outcome in our cohort can be explained by baseline imbalances, since our cohort had a higher NIHSS score and higher frequency of risk factors for poor outcome: 9% more patients had atrial fi brillation, 3% more had previous stroke, and 2% more had a history of diabetes. However, because we did not adjust these results for baseline imbalances between ECASS III and SITS-ISTR, we cannot rule out the possibility that other potential known and unknown factors might have infl uenced the poor outcome in our cohort.
The limitations of our data have been discussed previously.12,14 In summary, our study is observational and the analyses were exploratory in design. The study is based on registry data and therefore it is not possible to guarantee the completeness of inclusions to exclude selection bias. However, the similar outcomes in SITS-MOST12 and a pooled analysis of randomised controlled trials13 after adjustment for baseline diff erences suggest that the infl uence from such potential bias is limited. Another potential limitation is that we were unable to confi rm whether NIHSS assessment was done by a certifi ed examiner.18 The potential bias of patient selection for treatment beyond the 3 h timeframe is another possible limitation. Also, patients with missing data
could not be included in the respective outcome analysis, which could have infl uenced our results.
In conclusion, our study shows that rapid implementation of thrombolysis with alteplase beyond the 3 h time window into clinical routine occurred after the publication of the ECASS III6 trial and the SITS-ISTR study.14 There was no reduction in the number of patients treated in the earlier interval; rather the publications were followed by an increase in treatments within the entire widened time window. This has not been at the expense of increased delay from admission-to-treatment time. Increases in the risk of symptomatic intracerebral haemorrhage and mortality in the later time window are minor and are outweighed by the benefi t of the treatment. Our follow-up safety analysis confi rms our previous fi nding that, in patients who otherwise fulfi l European Summary of Product Characteristics criteria for intravenous thrombolysis, alteplase remains safe when given with short treatment delays beyond 3 h. Nevertheless, our results emphasise that patients should be treated as early as possible after stroke.
ContributorsNA and NW wrote the draft of the report. NA did the statistical analyses
and NW coordinated the study. NW, MG, MH, KRL, RR, and DT were
members of the scientifi c committee. NW, MG, KRL, RM, MP, ROR, DT,
and PR were national coordinators in countries with high recruitment
rates.
Scientifi c Committee of SITS InternationalNils Wahlgren (chair), Antoni Dávalos, Gary A Ford, Martin Grond,
Werner Hacke, Michael Hennerici, Markku Kaste, Vincent Larrue,
Kennedy R Lees, Risto Roine, and Danilo Toni.
Confl icts of interestNA is an employee of SITS International, which received a grant from
Boehringer Ingelheim and Ferrer for the SITS-MOST and SITS-ISTR.
NW has received expenses from Boehringer Ingelheim for his role as
member of the steering committee of the ECASS III trial, has served as a
consultant to Thrombogenics as chairman of the data safety monitoring
board, and has received lecture fees from Boehringer Ingelheim and
Ferrer. SITS International (chaired by NW) received grants from
Boehringer Ingelheim and Ferrer for SITS-MOST and SITS-ISTR. NW’s
institution has also received grant support towards administrative
expenses for coordination of the ECASS III trial. KRL has received fees
and expenses from Boehringer Ingelheim for his role as chairman of the
independent data safety monitoring board of the ECASS III trial and
Within 3 h Within 3–4·5 h Unadjusted results Adjusted results
n Number (%) n Number (%) Odds ratio (95% CI)
p Odds ratio (95% CI)
p
Symptomatic intracerebral haemorrhage
According to SITS-MOST defi nition 21 204 352 (1·7%) 2317 52 (2·2%) 1·36 (1·01–1·83) 0·04 1·44 (1·05–1·97) 0·02
According to ECASS II defi nition 21 206 1020 (4·8%) 2304 121 (5·3%) 1·10 (0·90–1·33) 0·35 1·27 (1·03–1·55) 0·02
According to NINDS defi nition 21 245 1515 (7·1%) 2317 171 (7·4%) 1·04 (0·88–1·22) 0·66 1·18 (0·99–1·41) 0·06
Mortality at 3 months 18 583 2287 (12·3%) 1817 218 (12·0%) 0·97 (0·84–1·13) 0·70 1·26 (1·07–1·49) 0·005
Mortality at 7 days 20 956 1307 (6·2%) 2259 132 (5·8%) 0·93 (0·78–1·12) 0·46 1·22 (1·00–1·48) 0·052
Functionally independent at 3 months (mRS 0–2) 18 317 10 531 (57·5%) 1784 1075 (60·3%) 1·12 (1·02–1·24) 0·02 0·84 (0·75–0·95) 0·005
Minimal or no disability at 3 months (mRS 0–1) 18 317 7467 (40·8%) 1784 793 (44·5%) 1·16 (1·05–1·28) 0·003 0·92 (0·83–1·03) 0·17
mRS=modifi ed Rankin scale.
Table 3: Main outcomes for patients treated within 3 h compared with those treated within 3–4·5 h

Articles
874 www.thelancet.com/neurology Vol 9 September 2010
related lectures, and has received fees from Paion, Forest, and Lundbeck
for the trials of desmoteplase in acute ischaemic stroke. KRL’s institute
has received grant assistance towards administrative expenses for
coordination of SITS in the UK. DT has served as a consultant for
Boehringer Ingelheim and has received lecture fees for attending and
speaking at workshops held by Boehringer Ingelheim, Sanofi -Aventis, and
Novo Nordisk. PR has received honoraria and payment for manuscript
preparation from Boehringer Ingelheim and PAION; and travel or
accommodation expenses from Boehringer Ingelhei, Sanofi , PAION,
Ferrer, and Lilly. All other authors have no confl icts of interest.
AcknowledgmentsSITS-ISTR is funded by an unrestricted grant from Boehringer
Ingelheim, Ferrer, and by a grant from the European Union Public
Health Executive Authority. Financial support was also provided through
the regional agreement on medical training and research (ALF) between
Stockholm County Council and Karolinska Institutet. J Tyler received
funding from Boehringer Ingelheim to provide editorial assistance in the
coordination of the submission. The views expressed are those of the
authors. Uppsala Clinical Research (UCR) centre, Sweden, develops,
maintains, and upgrades the software for the SITS register in close
collaboration with SITS. UCR team members are Sören Gustavsson,
Botond Pakucs, Olof Felton, and Niclas Eriksson. Alteplase (recombinant
tissue plasminogen activator) is not approved in the USA or Europe for
routine use in acute ischaemic stroke when initiated beyond 3 h from
symptom onset. We thank all the SITS-ISTR investigators and their
centres for their participation. We also thank all patients who participated
in SITS-ISTR.
References1 The National Institute of Neurological Disorders and Stroke rt-PA
Stroke Study Group: tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333: 1581–87.
2 Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: The European Cooperative Acute Stroke Study (ECASS). JAMA 1995; 274: 1017–25.
3 Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998; 352: 1245–51.
4 Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (alteplase) for ischemic stroke 3 to 5 hours after symptom onset: the ATLANTIS study: a randomized controlled trial: Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA 1999; 282: 2019–26.
5 Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study. Thrombolytic therapy in acute ischemic stroke study investigators. Stroke 2000; 31: 811–16.
6 Hacke W, Kaste M, Bluhmki E, et al, for the ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008; 359: 1317–29.
7 Davis SM, Donnan GA, Parsons MW, et al, for the EPITHET investigators. Eff ects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET). Lancet Neurol 2008; 7: 299–309.
8 Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004; 363: 768–74.
9 Lees KR, Bluhmki E, von Kummer R, et al, for the ECASS, ATLANTIS, NINDS, and EPITHET rt-PA Study Group Investigators. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010; 375: 1695–703.
10 Wardlaw JM, Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2003; 3: CD000213.
11 Hill MD, Buchan AM, Canadian Alteplase for Stroke Eff ectiveness Study (CASES) Investigators. Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Eff ectiveness Study. CMAJ 2005; 172: 1307–12.
12 Wahlgren N, Ahmed N, Davalos A, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet 2007; 369: 275–82.
13 Wahlgren N, Ahmed A, Eriksson N, et al, for the SITS-MOST investigators. Multivariable analysis of outcome predictors and adjustment of main outcome results to baseline data profi le in randomized controlled trials; Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS-MOST). Stroke 2008; 39: 3316–22.
14 Wahlgren N, Ahmed N, Dávalos A, et al. Thrombolysis with alteplase 3–4.5 h after acute ischaemic stroke (SITS-ISTR): an observational study. Lancet 2008; 372: 1303–09.
15 Karolinska Stroke Update Consensus Statement. Should the time window for intravenous thrombolysis be extended? http://www.strokeupdate.org/Cons_thrombolysis_2008.aspx (accessed April 5, 2010).
16 European Stroke Organisation. Update Guidelines January 2009. http://www.eso-stroke.org/pdf/ESO_Extended_Thrombolysis_KSU.pdf (accessed April 5, 2010).
17 Del Zoppo GJ, Saver J, Jauch EC, Adams HP, on behalf of the American Heart Association Stroke Council. Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke 2009; 40: 2945–48.
18 Lyden P, Raman R, Liu L, et al. National Institutes of Health Stroke Scale certifi cation is reliable across multiple venues. Stroke 2009; 40: 2507–11.