Embed Size (px)
Citation preview

RESEARCH Open Access
Implementation of clinical practice changesin the PICU: a qualitative study using andrefining the iPARIHS frameworkKatherine M. Steffen1* , Laura M. Holdsworth2, Mackenzie A. Ford3, Grace M. Lee4, Steven M. Asch5 andEnola K. Proctor6
Abstract
Background: Like in many settings, implementation of evidence-based practices often fall short in pediatricintensive care units (PICU). Very few prior studies have applied implementation science frameworks to understandhow best to improve practices in this unique environment. We used the relatively new integrated PromotingAction on Research Implementation in Health Services (iPARIHS) framework to assess practice improvement in thePICU and to explore the utility of the framework itself for that purpose.
Methods: We used the iPARIHS framework to guide development of a semi-structured interview tool to examinebarriers, facilitators, and the process of change in the PICU. A framework approach to qualitative analysis, developedaround iPARIHS constructs and subconstructs, helped identify patterns and themes in provider interviews. Weassessed the utility of iPARIHS to inform PICU practice change.
Results: Fifty multi-professional providers working in 8 U.S. PICUs completed interviews. iPARIHS constructs shapedthe development of a process model for change that consisted of phases that include planning, a decision toadopt change, implementation and facilitation, and sustainability; the PICU environment shaped each phase. Large,complex multi-professional teams, and high-stakes work at near-capacity impaired receptivity to change. While theunit leaders made decisions to pursue change, providers’ willingness to accept change was based on the evidencefor the change, and provider’s experiences, beliefs, and capacity to integrate change into a demanding workflow.Limited analytic structures and resources frustrated attempts to monitor changes’ impacts. Variable providerengagement, time allocated to work on changes, and limited collaboration impacted facilitation. iPARIHS constructswere useful in exploring implementation; however, we identified inter-relation of subconstructs, unique conceptsnot captured by the framework, and a need for subconstructs to further describe facilitation.
Conclusions: The PICU environment significantly shaped the implementation. The described process model forimplementation may be useful to guide efforts to integrate changes and select implementation strategies. iPARIHSwas adequate to identify barriers and facilitators of change; however, further elaboration of subconstructs forfacilitation would be helpful to operationalize the framework.
Trial registration: Not applicable, as no health care intervention was performed.
Keywords: Clinical practice change, Implementation, Intensive care unit, Pediatric
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Pediatrics, Division of Pediatric Critical Care Medicine,Stanford University, 770 Welch Road, Suite 435, Palo Alto, CA 94304, USAFull list of author information is available at the end of the article
Steffen et al. Implementation Science (2021) 16:15 https://doi.org/10.1186/s13012-021-01080-9

Contributions to the literature
� This analysis identifies common barriers and facilitators of
practice change in the PICU, which may inform
implementation of future evidence-based interventions in
this care setting.
� Limited research has applied the iPARIHS framework,
although the parent PARIHS is widely cited. This study adds
to the literature by using this new framework to address
implementation planning and strategy selection in the PICU.
� We noted limitations of the iPARIHS framework, particularly
around the facilitation construct, but provide descriptions of
useful activities that may improve understanding and
specification of facilitation.
BackgroundAdvances in care for critically ill children have improvedoutcomes. However, too often modern medical caretrades reduced mortality for increased morbidity inpediatric intensive care units (PICUs) [1]. One contrib-uting reason is that existing evidence-based practices areoften not used as frequently as recommended. As inmany health care settings, implementation of evidencein the intensive care unit (ICU) presents challenges,some of which may be due to patient complexity, stress,and an increased risk for error [2]. Moreover, specificchallenges to implementation related to the pediatricpopulation and environmental context of the PICU mayalso exist.Adult ICU studies provide some insight into ICU-
specific implementation issues, but often focus on imple-mentation of a specific intervention [3–7] such as post-arrest care [8], ICU care bundles [9], or handoffs [10], orutilize a specific implementation approach [2, 5, 11].Prior studies report that identifying and addressing local,contextual implementation barriers may help tooptimize care delivery in the ICU [12–14], which includelack of awareness of the innovation/guideline [7, 15],lack of resources [11], competing priorities [11], appre-hension around change [7], poor formatting of theinnovation for the clinical context [7], and inability toprovide accurate feedback on performance [11]. Sinuffet al. noted a fundamental need for an ICU culture tosupport a new intervention [16]. Other studies identifiedengaging staff, education, providing adequate time andresources, reminders, audit and feedback, and datareporting on performance as being useful implementa-tion strategies [5, 6, 8, 9, 15, 16], with providers in differ-ent roles reporting different implementation strategiesmost useful in effecting change [15].
While adult ICU studies may begin to inform imple-mentation of clinical practice changes in the PICU, toour knowledge, no study has attempted to characterizeunique PICU barriers and facilitators. We sought aframework that would account for the complexity of thisenvironment and identified the integrated PromotingAction on Research Implementation in Health Services(i-PARIHS) framework [17]. This framework and theparent Promoting Action on Research Implementationin Health Services (PARIHS) acknowledge complexity ofimplementation in actual practice. PARIHS is a widelyused conceptual framework designed to explain orpredict success of implementation [18, 19]. i-PARIHSdiffers from PARIHS in that it incorporates a broaderview of evidence and context, acknowledges the functionrecipients play in implementation success, and placesfurther emphasis on the role of facilitation [17]. In iPAR-IHS, the innovation, recipients, and context exist asconstructs that are modified by facilitation in the processof implementation [17].This qualitative study aimed to address a gap in the lit-
erature around PICU-specific implementation barriersand facilitators using the i-PARIHS framework and putsforth a comprehensive process model to understandchange in the PICU. Rather than focusing on a singleintervention, we broadly explore implementation in thiscomplex system. This approach has the potential to in-form adoption, delivery, and sustainability of differenttypes of evidence-based interventions and translate toimplementation benefits across the PICU population[20]. Additionally, we provide insight into using the rela-tively new i-PARIHS framework and comment on utilityin this clinical setting.
MethodsStudy designSemi-structured qualitative interviews were carried outto prepare for a study that will examine prospectiveimplementation of new blood transfusion recommenda-tions for critically ill children. The interviews aimed tounderstand prior experiences with implementing clinicalpractice changes within the PICU. Ethics approval forthe study was obtained from the Stanford University In-stitutional Review Board (IRB-47140). The completedStandards for Reporting Qualitative Research (SRQR)checklist https://www.equator-network.org/reporting-guidelines/srqr/ is included as additional file 1.
Participants and settingWe conducted interviews with health care providersworking in various roles from eight PICUs across theUSA. We selected units to represent variation in PICUtypes (pediatric ICU (excluding cardiac patients, 4 units),pediatric cardiovascular ICU (CVICU) (2 units), and
Steffen et al. Implementation Science (2021) 16:15 Page 2 of 15

combined pediatric/cardiovascular PICU/CVICU (2units)) and overall PICU size (11-32 beds) in the USA.The three types of ICUs are collectively referred to asPICUs, unless specified. A unit representative helped re-cruit participants. The study team and unit representa-tive sent an initial e-mail to solicit volunteers forparticipation. We provided additional information aboutthe study to respondents and contacted them if theyagreed to participate following review of this informa-tion. We selected participants using a stratified, purpose-ful sampling strategy, as described by Palinkas [21] toachieve a sample of participants within each PICU role.One of two authors (KS and MF) conducted interviewseither in person or via telephone. We obtained theparticipant’s verbal consent prior to each interview. In-terviews were audio recorded and transcribed verbatim.We continued interviewing participants in each roleuntil no new information was forthcoming from newparticipants. The qualitative team members (KS, LH,and GL) held meetings to review data and confirm whenvariation in responses was no longer noted.We developed an interview topic guide from the iPAR-
IHS framework [17]; however, added topics that focusedon barriers and facilitators of clinical practice changesand blood transfusion in the intensive care unit toensure we addressed aspects of change that are not ex-plicit in the iPARIHS framework (Additional file 2). Par-ticipants were asked first to describe a clinical practicechange that had been implemented in their ICU as astarting point to discuss the process and impact of theseinitiatives. Additional questioning focused on exploringPICU culture, receptivity to clinical practice change, ini-tiating and sustaining practice changes, and experiencesand perspectives on blood transfusion in the PICU.Qualitative data related to blood transfusion is notreported in this manuscript.
Qualitative analysisWe used a Framework Approach [22] for qualitativeanalysis with the NVivo (Version 12) software package.Framework is an approach to analysis in which case-level data (rows) are summarized along thematic cat-egories (columns) in a matrix and involves five steps offamiliarization, identifying a thematic framework, index-ing, charting, and mapping and interpretation [23]. Thecoding framework was structured around the iPARIHSconstructs (innovation (the evidence-based intervention),recipients, context, and facilitation) with associatedsubconstructs [17]. We applied iPARIHS in this specificsetting to gain insight into the combination of factorsrequired for successful implementation in this clinicalcare environment [20] and move toward precisionimplementation to ultimately better specify and tailorimplementation strategies [24]. Subconstruct definitions
were not available to standardize analysis; therefore, wedeveloped a codebook (Additional file 3) to define subcon-struct items using definitions drawn from the revised PARIHS framework [25], the Consolidated Framework for Im-plementation Research [26], and the Theoretical DomainsFramework [27]. The facilitation construct was codedbroadly to include any data wherein deliberate support orproblem solving was applied to promote implementation.Following coding, review, and organization of data codedwithin the facilitation construct, it became evident that thisdata broadly aligned with the implementation strategies asdescribed in the Expert Recommendations for Implement-ing Change (ERIC) project by Powell et al. [28]; thus, weorganized this data within the ERIC categories. We alsoadded inductive codes while searching for emergentthemes, particularly around implementation barriers andfacilitators to address potential constraints of using theiPARIHS framework to structure our analysis. At the outsetof the analysis, two researchers (KS, LH) selected and codedfived interviews independently using the a priori codes fromiPARIHS, while creating new codes for emergent themes.The researchers met to agree on definitions and interpreta-tions of existing codes, compare coding, and discuss emer-ging themes and integrate into the coding framework. Oneresearcher (KS) coded the remainder of the interviews usingthe established coding strategy. We initially categorizedcoded data within the iPARIHS subconstructs, then, follow-ing the Framework approach, summarized data to retaincontext for ease of comparisons across units and roles.Following summarization, we compared and contrasteddata between roles and clinical units, with careful consider-ation of identifying patterns as well as unique, but inform-ative statements that provided an alternative perspective tocapture variation. Strategies to ensure credibility (internalvalidity) of findings followed guidance by Miles et al. [29]and included linking data to categories in iPARIHS,checking for negative evidence, and checking thatfindings are replicable across the dataset (i.e., acrossmore than one PICU).
ResultsFifty health care providers were interviewed: PICU at-tendings (n = 15), fellow trainees (6), resident trainees(4), nurse practitioners (NPs) or physician assistants (9),nurses (10), and subspecialty physicians/surgeons whosepatients were cared for regularly in a PICU (6), such ashematologists/oncologists, cardiologists, and general andcardiothoracic surgeons. Providers in each role wereinterviewed at each site, with the exception of fellow orresident trainees, as they were not present in some units.Unless specified, the term “providers” refers to these in-dividuals collectively. Interviews lasted a median of 53.5min (range = 37–79 min) and were carried out betweenDecember 2018 and June 2019. Through exploration of
Steffen et al. Implementation Science (2021) 16:15 Page 3 of 15

the iPARIHS framework’s innovation, recipient, context,and facilitation constructs, we identified six themes andnine sub-themes that were important for change in thePICU.
The PICU as a high-risk environment for clinical practicechangeWithin the iPARIHS recipients and context subcon-structs, providers identified unique sub-themes of thePICU environment that increased complexity aroundclinical practice change and had important implicationsfor implementation. These include added complexitywith team-based care, high-stakes care that limited re-ceptivity to change, variable readiness for change, limitedbandwidth, and the emotional toll of the PICU environ-ment; each sub-theme is further described in Table 1. Ofnote, receptivity to change related to providers beingamenable to or interested in change conceptually,whereas readiness to change occurred when providershad the appropriate resources (time, skills, support) tooperationalize the change. When providers were receptiveto or ready for a change to occur, change was facilitated.Conversely, when providers were either not receptive to achange or not ready to integrate the change into practice,this served as a barrier to change.
Three sources of changeProviders reported that the stimulus for change in thePICU, located within iPARIHS innovation and contextconstructs, typically originated from three sources: (1)from a motivated individual or group with a specificinterest working within the unit, (2) from a sourceoutside the unit, or (3) as a result of a negative or sub-optimal clinical outcome (iPARIHS Construct: Context;Sub-constructs: Local level Culture, Local level Pastexperience with innovation and change, Organizationallevel Priorities, Organizational level Culture). Based onprior experience or personal interest, individuals orgroups proposed change initiatives to improve care. Out-side sources included the hospital, hospital system, or,infrequently, a regulatory agency; associated changes wereusually intended for the entire hospital or organization.Often, these changes did not account for PICU workflowor unit dynamics and were more difficult for providers toboth accept and integrate into practice (iPARIHS Con-struct: Innovation; Sub-constructs: Degree of fit with exist-ing practice and values). Providers disliked these changes“imposed” on the PICU and preferred when they weremodified to fit PICU practice. Providers of all professionsnoted that changes were made in response to adverse out-comes with significant or unexpected morbidity or mortal-ity (iPARIHS Construct: Context; Sub-constructs: Locallevel Culture, Local level Past experience with innovationand change). In these cases, clinical practices that were felt
to be causal were often modified or abandoned despiteprior demonstration of safety or success as providers werehighly motivated to avoid future negative events: “There’s alot of anecdote as well. Like there was that one bad caseone time, so we don’t ever want to try that again” (Site 1CVICU, Attending 2). Changes made in response to ad-verse outcomes were often made quickly and sometimeswithout obtaining provider input.
Unit leadership and unit-based processes: decision tomake a change guided by leadershipPrior to initiating change, unit leaders made the decisionto devote resources and pursue a change. Identifiedthrough the iPARIHS recipients and context constructs,there was variation in who made the decision to pursuea change in practice. PICU physician and nursing leaderswere often noted to work together to decide on makingchanges; however, in some cases, nursing or physiciansmade decisions independently without input from otherprofessions (iPARIHS Constructs: Recipients, Context;Sub-constructs: Power and authority, Local level Cul-ture). One NP noted: “A lot of policies and changes tonursing care are driven by nursing leadership. The med-ical team leadership is not necessarily involved in thosechanges…[it’s problematic because] we don’t learn aboutnew standards of care until the nurse actually prints outa new copy of it” (Site 1 Combined PICU/CVICU, NP12). Half of units had unit-based committees (multi-pro-fessional or nursing only) that informed leadership’sdecision to make a change. Other professional groups(respiratory therapists, etc.) and subspecialists wereroutinely omitted in many units from the decision tomake a change, though there was a broad understandingthat obtaining feedback, making modifications, andobtaining buy-in from all professions as change movedforward was essential (iPARIHS Construct: Context;Sub-constructs: Local level Culture, Local level Pastexperience with innovation and change).
Individual determinants: multiple determinants impacteda provider’s decision to accept and adopt changeWhile unit leaders made the decision to institute achange in the unit, in many cases, individual providersmade an independent decision to support the change aspart of their practice. While some changes were notedto be mandatory, providers who did not support achange could avoid using it in many cases, as there wasnot direct accountability. The individual provider’s im-pression of a proposed change impacted their willingnessto comply with or resist the change. This impressionwas determined by four sub-themes within differentiPARIHS constructs: (1) the evidence behind the change(iPARIHS Construct: innovation; Sub-constructs: Under-lying knowledge sources), (2) rationale for change (iPARIHS
Steffen et al. Implementation Science (2021) 16:15 Page 4 of 15

Table
1Descriptio
nof
sub-them
eswith
exam
ples
iPARIHSco
nstruc
t(s)
iPARIHSsub-con
struct
(s)
Them
eSu
b-the
me
Description
Exam
ple
Recipien
tsCon
text
Collabo
ratio
nand
team
work
Locallevel:
Mechanism
sfor
embe
ddingchange
PICUas
ahigh
-risk
environm
entfor
clinicalpractice
change
(sectio
n3.1)
Com
plexity
with
team
-based
care
Careisprovided
bymulti-profession
alteam
s,each
with
different
know
ledg
eand
expe
rtise.Chang
erequ
iredseekingou
tinpu
t,en
surin
gbu
y-in,
orprovidinginform
ation
toallteams,adding
complexity
“whe
neveryouwantto
actuallyeffect
anykind
ofsign
ificant
change
,the
re’sa
lotof
peop
lewho
have
toge
ton
board.
And
ofcourse,assoon
asyouadd
morecooksin
thekitche
nthings
seem
toslow
down”
(Site
1CVICU,A
tten
ding
1).
Recipien
tsCon
text
Motivation
Locallevel:C
ulture
High-stakes
limit
receptivity
tochange
PICUcare
andde
cision
-makingishigh
-risk,with
potentialfor
sign
ificant
morbidity
ormortality.
Providersde
scrib
eda
desire
toavoidne
gative
outcom
esat
allcosts.
“Our
cultu
reisthat
peop
leliketo
usethesame
protocolsbe
causethey’re
proven
,and
nottryto
change…especiallywhenit
comes
tobabies’health
”(Site
2CV
ICU,surgical
subspecialist
34).
Recipien
tsCon
text
Values
andbe
liefs;
Motivation
Locallevel:C
ulture
Variablereadiness
forchang
eCon
tinuo
uschange
sin
patient
status
andne
edforalteratio
nsin
care
plansmakesome
providersreadyto
change
,and
some
resistantto
it.
“Peo
plewho
workin
ICU
tend
tobe
kind
ofconstantlyreadyfora
change
inpatient
cond
ition
,they
arealso
kind
ofhard
wiredor
prepared
for
changesinotherw
ays”(Site
3PICU
,NP23)
“The
unitisa…veryintense
andchaotic
place.Ithink
we
cravestabilityandsomeof
thestabilityiscentered
arou
ndeasy
decisio
nmaking.”(Site
2Co
mbined
PICU
/CVICU
,Attending
44)
Recipien
tsCon
text
Time,resources,supp
ort
Locallevel:C
ulture
Limited
band
width
Unitsoftenfunctio
ned
atlim
itsof
capacity;
providersfelt
overworked,
repo
rted
units
wereun
derstaffed.
Staffandleadership
turnover
andtempo
rary
staff(i.e.traveling
nurses,residen
ttraine
es)
posedchalleng
esto
consistent
useof
new
practicechange
s.
“Inertia
from
being
overworkedisabarrier[to
change
].Peop
lehave
really
high
clinicalloads,so
they
don’twantto
makea
change
.Ifit'sno
talready
partof
your
habit…
gets
pushed
downthepriorities”
(Site
3PICU
,Fellow22)
Con
text
Locallevel:C
ulture
Emotionaltollo
fthePICU
environm
ent
Emotional,ph
ysicaland
men
talexhaustion
noteddu
eto
unpred
ictableand
difficultcases.Em
otions
“Mostkids
dono
thave
any
oftheproced
ures
orou
tcom
esthat
ourpatients
do.Ithinkthat
definitely
flavorsho
wpe
oplereactto
Steffen et al. Implementation Science (2021) 16:15 Page 5 of 15

Table
1Descriptio
nof
sub-them
eswith
exam
ples
(Con
tinued)
iPARIHSco
nstruc
t(s)
iPARIHSsub-con
struct
(s)
Them
eSu
b-the
me
Description
Exam
ple
influen
cedeffortsto
change
practice.
things...Ithink
thestakes
arehigh
erin
manywaysfor
manyof
thethings
that
we
do,orat
leastitfeelsthat
way.”(Site
1Com
bine
dPICU/CVICU,A
tten
ding
9).
Inno
vatio
nUnd
erlyingknow
ledg
esources
Individu
alDeterminants
(sectio
n3.4)
Eviden
cefor
change
Strong
scientific
eviden
ceforchange
was
apo
werfulstim
ulus
toconvince
providersto
change
,particularlyfor
physicians
andNPs.
“For
providers–isit
clinicallyrelevant,d
oesit
provideabe
nefit?How
much?
Wene
edto
see
research.W
ene
edto
see
data
that
show
sthat
thisis
goingto
beworth
the
effort.”(Site
3PICU,N
P24)
Inno
vatio
nRecipien
tsRelativeadvantage
Values
andbe
liefs;
Motivation
Ratio
nalefor
change
Ratio
nale:
Und
erstanding
the
ratio
naleforachange
,go
als,andpo
tential
bene
fitsof
achange
werevitally
impo
rtant
forallp
rovide
rs.
“Som
etim
espe
opledo
n’t
fully
unde
rstand
thereason
fortrying
tomakea
change…
Eitherthatit’sno
trelayedor
explainedinthe
right
manner…
iftherewas
abette
rund
erstanding
they'd
bemorelikelyto
beon
boardwith
it.”(Site
1Co
mbinedPICU
/CVICU
,Attending
11)
Recipien
tsValues
andbe
liefs;
Motivation
Provider
level
factors:provider
expe
rience
App
rehe
nsionarou
ndchange
:Provide
rsno
ted
beingappreh
ensive
abou
tchange
,preferrin
gthe“old
way
todo
things”
“The
hardestthing[abo
utchange
]ispe
oplearejust
soused
todo
ingitacertain
way.Itm
akes
peop
lenervous
tochange
theway
that
they’ve
alwaysdo
nethings.It
may
take
yououto
fyour
comfortzone,and
peop
ledo
n’tlikethat.”(Site
4PICU
,NP35)
Recipien
tsMotivation;skillsand
know
ledg
eDurationof
Expe
rience:
Moresenior
providers
wereofteniden
tifiedas
beingless
receptiveto
change
than
less
senior
providers,ho
wever
theseprovidersalso
influen
cedpracticeand
couldfacilitate
acceptance
ofchange
.
“The
peop
lewho
have
been
here
forthe
long
est,arethe
leastlikelyto
embrace
change…Theearly
adop
ters
aretheyoun
gerp
eople.
Especiallythepeop
lewho
comefro
motherp
lacesand
who
have
seen
itdo
nedifferently.”(Site
1CV
ICU,
Attending
,2)
Recipien
tsValues
andbe
liefs;
Motivation
Provider
level
factors:be
liefs
Perceivedne
ed:C
hang
ewas
perceivedas
“neede
d”if1)
the
“Ithink[thechange
was
easy
because]everyone
was
alittle
bitfrustratedwith
the
lack
ofprocess,or
protocol
Steffen et al. Implementation Science (2021) 16:15 Page 6 of 15

Table
1Descriptio
nof
sub-them
eswith
exam
ples
(Con
tinued)
iPARIHSco
nstruc
t(s)
iPARIHSsub-con
struct
(s)
Them
eSu
b-the
me
Description
Exam
ple
existin
gprocesswas
frustratin
g,2)
the
change
preven
tedabad
outcom
e,or
3)it
aligne
dwith
the
provider’spriorities,
hospitalvalues,or
practices
atothe
rcenters(ben
chmarking
).
previously”(Site1PICU
,Attend
ing6)
Recipien
tsValues
andbe
liefs;
Motivation;Skillsand
know
ledg
e
Potentialfor
negative
outcom
e:Providers
worriedchange
smight
have
ane
gativeim
pact
onou
tcom
esandne
wpractices
may
beless
safe
ininexpe
rienced
hand
s.Sign
ificant
shifts
inpracticeweremore
difficultto
accept.
“It’sno
tjustthatwe’re
stuck
inou
rways.Wewantto
dothings
thatweknow
we’re
good
atandthat
are
effective.Even
ifsomething
[new
]might
besligh
tlymore
safe,isitmoresafeinmy
hand
s?I'm
notsure.”(Site
1PICU
Attending
5)
Recipien
tsValues
andbe
liefs
Com
prom
ised
autono
my:Some
providersfeltcreatio
nof
standard
practices
might
comprom
isetheir
autono
my.
“Som
epe
oplefeellike
they’re
gettingtheir
freed
omtakenaw
ay…
they
aren
’tgo
ingto
have
that
creativefre
edom
tochoo
seho
wthey
wantto
manage
apatient...whe
nthey
feel
liketheiroverallautho
rityis
beingtakenaw
ay,it’s
hard
forsomepe
ople”(Site
4PICU,N
P35)
Recipien
tsValues
andbe
liefs;
Motivation
Provider
level
factors:
Perceivedbenefit/
effort
Costvs.b
enefitof
change
:Manychange
srequ
ireadditio
naltim
eor
adding
atask;the
bene
fitof
thechange
mustexceed
the“cost”
ofchanging
,otherwise
itisless
likelyto
beaccepted
orpe
rform
edconsistently.
“The
re’sprob
ablysome
balanceof
howimpo
rtantis
[thechange]?How
easy
isit?
Ifsomething
’sreally
impo
rtant,even
ifit’sreally
difficultto
do,peoplewilldo
it.Ifsomething
’son
lymod
eratelyimpo
rtant
then
youprob
ablyneed
alow
amou
ntof
resistanceto
doit.”(Site
2CV
ICU,Fellow29)
Recipien
tsCon
text
Time,resources,supp
ort
Locallevel:C
ulture
Com
petin
ginterestsandtim
eChang
esthat
were
unrealistic
dueto
othe
rde
mands/tasks
were
unlikelyto
besupp
orted
orcarriedou
t.
“It’shard
tokeep
adding
all
ofthesechange
s.We
alreadydo
somuchdu
ring
a12-h
perio
d.To
add
something
else
isjust,“Why
arewedo
ing“one
more
thing”.”(Site
1Co
mbined
PICU
/CVICU
,Nurse
13)
Steffen et al. Implementation Science (2021) 16:15 Page 7 of 15

Constructs: innovation, recipients; Sub-constructs; Relativeadvantage, Values and beliefs; Motivation), (3) provider-level factors (iPARIHS Construct: recipients; Sub-constructs: Values and beliefs; Motivation; Skills andknowledge), and (4) competing interests and time (iPAR-IHS Constructs: recipients, context; Sub-constructs: Time,resources, support; Local level Culture) (Table 1). Providerlevel-factors were intrinsic to the individual provider thatinfluenced perception of and receptivity to change. Weidentified three factors within this sub-theme: provider ex-periences, provider beliefs, and balancing benefit with ef-fort. Provider experiences refer to how receptivity tochange and implementation were dependent on a pro-vider’s level of experience or prior experiences working inthe PICU. Provider beliefs were ideas providers held abouttheir own practice or change in the PICU that impactedtheir receptivity to change. Finally, all providers perceivedthat change required an additional investment of time andeffort. Each provider explicitly or implicitly recognizedthat they balanced the “costs” of a change (time, effort)with the perceived benefits of the intervention. Table 1 de-scribes each of these sub-themes and factors in detail andprovides an example of how providers discussed them.
Operationalization of facilitation through implementationstrategiesWe gained perspective on the iPARIHS facilitation con-struct by asking providers about barriers and facilitatorsof change as well as prior experiences with change.Broad coding for this construct yielded a wide range ofdata elements describing actions and strategies used topromote implementation. These data were often linkedwith one or more of the innovation, recipients, and con-text constructs, which made it difficult to characterizeelements within a single iPARIHS construct given theunique PICU context. The actions and strategies thatconstituted facilitation mostly fit within the ERIC cat-egories of planning, restructuring, education, qualitymanagement [30], as detailed in Table 2. These facilita-tion strategies have key features that are unique to thePICU environment which we will describe.Sub-optimal levels of engagement around new evi-
dence and need for practice change (iPARIHS recipients,context) among some providers were an importantbarrier to changing existing clinical practice. This oftenstemmed from professional expectations and require-ments. Nurses were not expected to stay abreast of newevidence which impacted receptivity to change, asdescribed by one nurse: “Not all the nurses have made itpart of their professional practice to stay updated on evi-dence… Practice changes that come from new evidencecan be a little more challenging for that group” (Site 3PICU, Nurse 25). Support given to nurses and othernon-physician providers to spend time working on
practice changes was also limited: “One of the challengesis that they [hospital administration] call our work [onchange] ‘non-productive time’…they don’t allot a lot ofresources to it. Some people are willing to go above andbeyond without getting paid, but it’s not very wellresourced” (Site 3 PICU, Nurse 25). As such, lack of ex-pectations or incentives to work on change in these roleshindered progress.Providers felt identifying a champion within each pro-
fessional role was necessary to ensure a resource existedto support each group (iPARIHS recipients, context).Champions were stated to be knowledgeable about andpromote use of the change, remind and reinforce whychange was being made, and in some cases, assist withimplementation. As in many implementation efforts,achieving buy-in from both leadership and front-linestaff was essential; in addition, for nurses, creating trueownership of change was noted to be particularly power-ful in ensuring consistent application of the change.Informing large and complex PICU teams (iPARIHS
context) of a change was identified as a challenge butwas also noted to be vital to elevate awareness and en-sure that teams worked in concert to use new processes.Multiple modalities of communication (both written andverbal) were needed within multiple settings (meetings,huddles, newsletters, email announcements, computer-based learning modules, etc.) to ensure reach to all pro-viders. Finally, nurses, in particular, preferred advancednotice about upcoming change to allow them to prepareto integrate changes into workflow; they appreciated op-portunities to practice using new skills or techniques ina simulated setting prior to roll-out.Providers emphasized the need to have easy access to
information and tools required for change at all times(iPARIHS innovation, context). Different units had vari-ous established options (electronic, hard copy, signage),but providers differed in their opinions about which ofthese worked best. Because multi-professional educationabout change was often completed at a time remotefrom actual implementation, additional “just-in-time”training at the time of change “roll-out” was viewed asvery helpful, particularly by nurses.Following initial implementation efforts, providers
needed consistent and frequent exposure to a new inter-vention to ensure that it became part of their workflow(iPARIHS innovation). Infrequent opportunities to use achange (i.e., for a rare condition) made it difficult to in-tegrate into practice, as one provider noted: “Sometimeseverybody agrees that there’s going to be a policy changebut it may be six months before you encounter asituation where that change would be implemented andthen nobody remembers.” (Site 2 PICU, medical sub-specialist 18). Any effort to make change automatic orefforts to allow providers to practice using a change to
Steffen et al. Implementation Science (2021) 16:15 Page 8 of 15

Table 2 Implementation strategies important for facilitation in the PICU
Strategy Description Example
Plan strategies
Tailor strategies to overcomebarriers and honor preferencesa
Tailor strategies to overcome barriersand honor preferences
“I think engagementc of the bedsideproviders [helps change occur]...really tryingto understand how a change will affect thework and then modify the proposedchange based on the information that youget from people at bedside.” (Site 3 PICU,Attending 21)
Conduct local consensus discussiona Achieving buy-in from leadership andbedside providers, creating ownershiparound change for those who usechange on a daily basis
“Giving more ownership to the bedsidenurses about the changes that areimpacting the practice helps change to bea little bit easier.” (Site 1 Combined PICU/CVICU, Nurse 13)
Identify and prepare championsa Identifying champions from eachdiscipline impacted by change
“Having people who are champions atmultiple different levels of stakeholders…whoever it may be that’s going to beinvolved to really lead that effort helpschange occur” (Site 4 PICU, Attending 36)
Restructure strategies
Change physical structure,equipment, records systemsa
Embedding change into work systems(including EMR)
I think electronic medical record isprobably the one thing that can help a lotwith [implementation] since there is somuch of our work [that’s done there](Site 4 PICU, Fellow 38)
Educate strategies
Conduct educational meetingsa Multi-professional education aroundchange
“I think that there would have to beeducation [for a proposed change]. Andnot just for physicians, but also for nursepractitioners and for bedside nurses tounderstand why and where this is comingfrom” (Site 1 CVICU, Attending 2)
Make training dynamica Creating ways to reliably inform largePICU teams about change (usingmultiple modes of communication)
I think it is helpful doing [education] in amultitude of ways that are kind ofrepeated, to capture as many people aspossible. (Site 4 PICU, Attending 36)
Time-sensitive training Just in time education around the timeof change roll-out
“For nurses, [change is facilitated by] “bootson the ground” things. The huddles, just-in-time education. (, more responsive tothat sort of environment. (Site 2 PICU,Attending 20)
Develop effective educationalmaterialsa
Creating easy access to informationabout change, tools needed
“[a new protocol/process] would need tobe in a place of easy access… in academicinstitutions where you’re having newrotators come through every several weeks,[you need to] make sure that there is away to introduce it to folks” (Site 2Combined PICU/CVICU, Resident 50)
Advance notice about change Giving providers time to preparefor change
“[Change is hard if] it really greatly impactsour workflow and doesn't come with anypreparation…If I know it’s coming, and Ican personally think about how is this isgoing to affect my practice, and how I’mgoing to mitigate that issue (Site 3 PICU,Nurse 25)
Practice using change Repeated use of change to create“muscle memory” around change(infrequently used changes are muchharder to incorporate)b
“It’s repetition [that helps change “stick”].Whether it’s repetition of practice or justrepetition of education …sometimeseverybody agrees that there’s going to bea policy change but it may be six monthsbefore you encounter a situation wherethat change would be implemented andthen nobody remembers” (Site 2 PICU,medical subspecialist 18)
Steffen et al. Implementation Science (2021) 16:15 Page 9 of 15

create “muscle memory” around the change were alsovaluable.
Sustainability of change in the PICUFollowing initial implementation, sustainability of changein the PICU was a formidable challenge, but of significantinterest, as maintaining the benefits of successful practicemodifications over time is important. While iPARIHSdoes not address sustainability directly, we inferred identi-fied strategies for sustainability through discussions of theiPARIHS context subconstruct “mechanisms for embed-ding change.” Aspects of planning, including ensuringbuy-in from all professional groups, and promoting as-pects of changes that have direct value for providers, wereidentified as being important for ultimate sustainability.While all provider roles saw great value in tracking andproviding data around the impact of change, physicians in
particular saw great benefit in this method to sustain buy-in and increase compliance. Importantly, many providersnoted that their unit lacked resources to collect and reportdata back to unit staff, representing a major limitation tosustainability, and an opportunity for improvement. Oneattending physician involved in quality improvement com-mented: “There’s certainly great efforts to make more ofour interventions data driven, but that hasn’t been empha-sized as much…So creating that whole infrastructure – it’sa big task” (Site 1 CVICU, Attending 1). Providers also feltthat frequent reminders about the rationale for changeand about the change itself promoted sustainability.
A model for implementing change in the PICUThrough exploration of the iPARIHS framework’s con-structs and identification of the themes described above,we developed a model for change implementation in the
Table 2 Implementation strategies important for facilitation in the PICU (Continued)
Strategy Description Example
Quality management strategies
Develop and organize qualitymonitoring systemsa/Audit andprovide feedbacka
Tracking data/evaluation of the impactof change (monitoring compliance,outcomes, safety data)b
I think reporting back…so that peopleknow, “Hey this thing we started this ninemonths ago?...Here’s what happened. That’sobviously an incentive for people to feellike it made a difference” (Site 2 CVICU,Attending 28)
Remind cliniciansa Frequent reminders about existence,importance of/rationale behind newchangeb
“[change is facilitated by] Informalreminders…the way sometimes people willremind you, “All right, let’s make sure weare doing our check lists at the end ofevery patient,” or the way people say, “let’sremember to wash our hands in and out ofevery room.” (Site 2 CVICU, Fellow 29)
Conduct cyclical small testsof changea
Iterative changes made to enhanceuse of change process
“[to make change “stick”] a check-in and afeedback session would probably be good,and if small changes need to be made towhatever protocol that’s established, theycan be made and re-evaluated.” (Site 2PICU, Attending 17)
Other strategies
Ensuring adequate resources Obtaining adequate resources to plan,implement, and sustain change
“Resources [can be a barrier to change] aswell. Most changes require some sort oftime, effort, if not other financial resourcesto implement.” (Site 4 PICU, Attending 36)
Communicating early success Celebrating “successes” of change “One of the ways that we found [to helpmake change] most successful wascelebrating our successes…we put it in thenewsletter, and celebrated it.” (Site 3 PICU,Nurse 25)
Accountability Creating accountability for change(may be from frontline staff)
“There needed to be more accountabilityfor…how do we make sure these thingsget done? So, they developed this littlelist…you had to sign off, you had to turn itin before you left. That went on for 6months, and then people had kind of builta habit into their practice.” (Site 2Combined PICU/CVICU, Nurse 48)
aDenotes described ERIC strategybNoted to be important for sustainability of changecEngagement in this case denotes the process in which a those planning a change solicit feedback from providers who will use a change toprovide insight into how to optimize implementation
Steffen et al. Implementation Science (2021) 16:15 Page 10 of 15

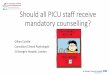
PICU (Fig. 1). This model reflects the iPARIHS con-structs and subconstructs and extends beyond iPARIHSto illustrate the relationships between PICU-specificfactors that influence change, including the hospital andPICU environment that influence change appreciably.These relationships are not reflected in iPARIHS, butlikely crucial to understand when planning implementa-tion in the PICU. As a process model [31], our modeldescribes the manner in which research is translated intopractice within the PICU; this process includes multiplephases.Ideas are initially proposed by individuals or groups
(three sources of change, as described in Section 3.2).The decision to pursue change in the unit is made byunit leadership (unit leadership: Section 3.3). Our inter-views did not explore the factors that influence howleadership selects changes to pursue; however, availableunit resources, unit needs and priorities, and mandatesat the hospital level likely contribute to these decisions.Individual providers also choose to support or resist achange based on multiple factors (individual determi-nants, Section 3.4), including the evidence and rationalefor the change, their own beliefs and experiences, thepotential benefit versus the effort required to change,and time required in light of other competing interests.While initial subthemes such as evidence and rationalefor change are necessary, they are superseded by subse-quent subthemes. As such, regardless of the evidence orrationale for a change, implementation will not occurunless providers perceive that the benefits of a changeexceed the effort required and they have adequate timeto operationalize the change. Change subsequently requires
facilitation (Section 3.5), implementation, and later, effortsto ensure sustainability (Section 3.6).Individual determinants and unit/team processes
interact with one another and influence the selection offacilitation activities which are operationalized primarilyas implementation strategies; likewise, facilitation activitiesimpact these factors and are linked in a bidirectional fash-ion. Facilitation efforts enable implementation; whether ornot a change is implemented is dependent on individualdeterminants and unit leadership and processes. This rela-tionship is unidirectional. Finally, after initial implementa-tion, if a change has been integrated into workflow, it maybe sustained. The PICU environment exerts an influenceon this entire process of change, impacting how individ-uals perceive proposals to change and their ability to inte-grate changes into standard work. To a lesser degree, thehospital may also influence change, often when hospital-wide modifications to practices are also mandated in thePICU. We acknowledge that this model is idealized in thelinear arrangement; in actual practice, implementationsteps are unlikely to be sequential, and implementation ef-forts may stall and require teams to go back to a previousstep before a change is integrated into workflow. Thismodel emphasizes the factors and their relationships thatimpact implementation and may be used for implementa-tion planning in this setting.
DiscussionFrom this qualitative study using the iPARIHS framework,we identified interactions between constructs and shapedthose into a model for change in the PICU, which, to ourknowledge, has not been previously described. Elements
Fig. 1 Model for implementing change in the PICU
Steffen et al. Implementation Science (2021) 16:15 Page 11 of 15

missing from the iPARIHS framework, but relevant inother implementation models [32, 33] have been added.Implications for planning implementation in the PICUexist within each model element and phase. The phases ofchange are shaped by the PICU environment, with anessential need to involve members of large, complexmulti-professional teams, and acknowledge the high-risk,high-stakes nature of the work at near capacity, andapprehension about potentially worsening outcomes thatoften makes providers hesitant to improve care that is ad-equate, but could still be improved significantly. Decisionsto change were made both by unit leadership who sup-ported change at the unit level and individual providerswho made an independent decision to support or resistchanges. Some providers readily embraced change, whileothers sought out stability in this unpredictable environ-ment. Notably, providers who were sometimes identifiedas the least likely to embrace change were also most influ-ential in supporting initiatives and critical for ensuringbuy-in and success; specifically involving these providersin change and ensuring their participation may be usefulfor implementation among other staff looking to these in-dividuals for guidance around use of new changes. Sinuffet al. reported barriers and facilitators in relation to guide-line adherence in adult ICUs and identified several find-ings similar to those in the PICU, notably the need foreffective leaders, tailored education based on learningpreferences, reminders, and data-based evaluation [16].While Sinuff et al. stress the importance of creating a cul-ture that supports guideline use [16], this study highlightssome of the barriers in the PICU environment and culturethat can hinder implementation and ultimately are im-portant to address when creating an implementation plan.
Using iPARIHS to understand PICU implementation effortsThe iPARIHS framework was generally helpful as a de-terminant framework in exploring implementation; wefound the innovation, recipients, and context constructsoverall were a useful scaffold to structure thinking aboutimplementation in the PICU. Harvey and Kitson placefacilitation central to the process of implementation iniPARIHS, as it “activates implementation through asses-sing and responding to characteristics of the innovationand recipients within their contextual setting” [17].While the other main iPARIHS constructs are expandedfor users with detailed subconstructs, facilitation is some-what under-defined. The characteristics of a facilitator aredescribed; however, the actions that constitute facilitationare not detailed, and there is no sub-classification of thetypes of activities or strategies that facilitators might utilizeto enable and support change. Lack of clarity around theaction of facilitation constituted somewhat of a “black box”in the framework, despite the fact that it remains crucialfor implementation. We aimed to further describe
facilitation by identifying activities that “activated imple-mentation” through our interviews and subsequent qualita-tive analysis. While this work does not go as far as topropose a comprehensive set of facilitation subconstructs,we provide insight into facilitation activities that may beuseful in the PICU, which are presented in Table 2. Astrength of our work is the delineation of the activities im-portant for facilitation, which in this PICU environmentconsisted primarily of activities that could be linked withknown implementation strategies. By developing a morecomprehensive and clear understanding of the facilitationconstruct, we aim to advance the framework and poten-tially inform future identification of important facilitationsubconstructs within iPARIHS. We offer this critique basedon our qualitative data and suggest that to further improvethe framework, a more detailed description of componentsor features of facilitation would be useful for frameworkoperationalization and in determining where facilitationbarriers exist. Moreover, identifying these activities may bekey to informing the selection of implementation strat-egies, which continues to be an active area of inquirywithin implementation science [34] and holds practicalvalue to those translating evidence into practice.Implementation strategies identified through assess-
ment of facilitation in our work in the PICU have beendescribed by others in similar ICU environments. de Voset al. and Stevens et al. noted the importance of engagedstaff and adequate resources to facilitate change [5, 15];in our study, facilitation of change was impacted by vari-able provider engagement and the time and personnelallocated to work on change. Other authors have reportedthe utility of some of the same facilitators in the ICUenvironment including the need for multiple educationalmodalities and a team of motivated champions [7, 8].The process model that we have put forth organizes
the iPARIHS constructs to reflect how change occurs inthe PICU setting and potentially informs how groupsmight identify barriers and facilitators and plan imple-mentation strategies. We did, however, find there wereiPARIHS subconstructs that were infrequently discussedby providers (i.e., goals, organizational absorptivecapacity) and may not be as important in this setting.We also identified novel concepts not included in theframework and interplay between constructs that hadimportant implications for implementation.Some of the iPARIHS subconstructs were difficult to
separate from one another in the PICU setting. Withinthe recipients construct, motivation and values and beliefswere often inter-related. Within innovation, usability andclarity were related, and within context, we found that dis-cussions of past experiences with innovation and changewere linked closely to mechanisms for embedding change,as many efforts attempted to integrate changes into PICUworkflow. While this did not complicate our analysis, the
Steffen et al. Implementation Science (2021) 16:15 Page 12 of 15

fact that these and other sub-constructs often “traveledtogether” or were interlinked should be noted.There were a few frequently discussed concepts that did
not easily fit within any of the iPARIHS subconstructs.These findings may reflect the fact that we created aprocess model from the determinant iPARIHS framework,but could potentially be considered useful additions to theframework. Providers’ emotions were conceptually distinctfrom motivation or values and beliefs and had an import-ant influence on the work environment and the stressorsthat might prevent acceptance of change. Another ex-ample was the importance of having regular opportunitiesto use a change in actual or simulated practice for nurses;however, there was no subconstruct within innovationthat captured this concept. We observed a few instanceswhere factors within one construct significantly influencedanother. For example, the concept of loss of autonomywith standardization of care fit within the construct of theinnovation; however, recipients were also impacted. Inexamples like these, factors influencing implementation inthe PICU did not fit neatly within single iPARIHSconstructs; understanding the links between constructshas implications for implementation planning.The iPARIHS framework lacks formal subconstruct
definitions. Guided by other existing frameworks, wedeveloped more explicit subconstruct definitions thatmay be used in future studies to guide a standardapproach to qualitative analysis using this relatively newframework (Additional file 3). To further build on iPAR-IHS, we posit that standard definitions for subconstructsbe developed to ensure consistent use of terms. This isparticularly important for use of the framework withinthe research setting, as the need for uniform definitionshas been noted frequently in implementation science[35]. We also suggest that further exploration of theconcept of facilitation, with potential for development ofsubconstructs to further define components or actions.This will provide users with context to evaluate andoperationalize plans around this critical element of theframework.
LimitationsAn aim of the larger study was to investigate implemen-tation of blood transfusion recommendations, as such,we enrolled participants who ordered or administeredtransfusions but did not include other providers whomay play a role in implementation of other PICU prac-tice changes (respiratory therapists, pharmacists, pa-tients, etc.). While it was not within the scope of thisproject to include the perspectives of all allied healthprofessionals who work in the PICU, we perceive thatour model of change, which is based on a number ofdifferent pediatric ICU models, is likely fairly compre-hensive, but which may benefit from additional nuance
that the inclusion of these groups might offer in futurestudies. While we aimed to ensure that PICUs were rep-resentative of the scope of US practice, it is possible thatnot all variations in PICU culture are represented andthat the data presented is not fully generalizable to otherPICUs; however, using the iPARIHS framework helpedto ensure that we captured characteristics of the changeprocess that are broadly transferable across settings.Barriers, facilitators, and implementation methods notedby interviewees reflect their opinions; in reality, differentelements of the PICU setting may be more important tooptimize implementation; however, this analysis servesas a starting point for guiding and testing implementa-tion in this setting.
ConclusionsThe PICU environment and providers significantly shapethe nature and process of implementing clinical practicechanges, with need for accommodation of large, complexteams, high stakes work, and individual providers whoapproach change in light of their own experiences,beliefs, and capacity to integrate changes into an alreadydemanding workflow. Unit or hospital-based systemsmay not provide resources to optimize facilitation andparticipation in change and often do not have establishedmethods to provide data on the impact of changes. TheiPARIHS framework was adequate to identify barriers andfacilitators of change in this environment; however, furtherelaboration of subconstructs of facilitation was necessaryto operationalize the framework. Our process model forimplementation in the PICU may guide selection of imple-mentation strategies in similar environments and augmentefforts to integrate change into workflow.
Supplementary InformationThe online version contains supplementary material available at https://doi.org/10.1186/s13012-021-01080-9.
Additional file 1.
Additional file 2.
Additional file 3.
AbbreviationsCVICU: Cardiovascular intensive care unit; PICU: Pediatric intensive care unit;ICU: Intensive care unit; iPARIHS: Integrated Promoting Action on ResearchImplementation in Health Services; NP: Nurse practitioner; PARIHS: PromotingAction on Research Implementation in Health Services
AcknowledgementsNot applicable
Authors’ contributionsKS conceptualized the project with LH, conducted provider interviews,analyzed and interpreted the qualitative data, and was a major contributor inwriting the manuscript. LH also analyzed and interpreted the qualitativeinterviews and assisted in writing and editing the manuscript. MF conductedsome of the provider interviews. GL, SA, and EP provided additional support
Steffen et al. Implementation Science (2021) 16:15 Page 13 of 15

in planning the project, interpreting the data, and in framing and editing themanuscript. The authors read and approved the final manuscript.
Authors’ informationNot applicable
FundingResearch reported in this publication was supported by the National Heart,Lung, and Blood Institute of the National Institutes of Health under AwardNumber K12HL137942. The content is solely the responsibility of the authorsand does not necessarily represent the official view of the National Institutesof Health.
Availability of data and materialsThe datasets used and/or analyzed during the current study are availablefrom the corresponding author on reasonable request.
Ethics approval and consent to participateEthics approval for the study was obtained from the Stanford UniversityInstitutional Review Board (IRB-47140). Per the IRB, the participant’s verbalconsent was obtained prior to each interview.
Consent for publicationIndividuals provided verbal consent prior to participating in interviews. Theverbal consent process included reading the following statement: “Yourinterview will be audio recorded and transcribed for analysis. Study findingswill be presented in aggregate; individuals will not be identified in anypresentations or publications. De-identified quotes may also be used inresearch papers or presentations”. We have presented individual quotes thatindicate the individuals’ role and ICU type only. The selected quotes do notreveal any specific details about the individual that could lead to identificationof the individual.
Competing interestsThe authors declare that they have no competing interests.
Author details1Department of Pediatrics, Division of Pediatric Critical Care Medicine,Stanford University, 770 Welch Road, Suite 435, Palo Alto, CA 94304, USA.2Stanford Division of Primary Care and Population Health, Stanford, CA, USA.3Department of Pediatrics, Division of Pediatric Cardiology, StanfordUniversity, Palo Alto, CA, USA. 4Department of Pediatrics, Division of PediatricInfectious Diseases, Stanford University, Palo Alto, CA, USA. 5VA Center forInnovation to Implementation, Stanford Division of Primary Care andPopulation Health, Palo Alto, CA, USA. 6George Warren Brown School ofSocial Work, Washington University in Saint Louis, Saint Louis, MO, USA.
Received: 10 September 2020 Accepted: 1 January 2021
References1. Pollack MM, Holubkov R, Funai T, Clark A, Berger JT, Meert K, et al. Pediatric
intensive care outcomes: development of new morbidities during pediatriccritical care. Pediatr Crit Care Med. 2014;15:821–7.
2. Cavalcanti AB, Machado F, Bozza F, Ibrain J, Salluh F, Campagnucci VP, et al.A cluster randomized trial of a multifaceted quality improvementintervention in Brazilian intensive care units: study protocol. Implement Sci.2015;10:8.
3. Gude WT, Roos-Blom MJ, van der Veer SN, de Jonge E, Peek N, DongelmansDA, et al. Electronic audit and feedback intervention with actionimplementation toolbox to improve pain management in intensive care:protocol for a laboratory experiment and cluster randomised trial.Implement Sci. 2017;12(1):68.
4. Cahill NE, Day AG, Cook D, Heyland DK. Development and psychometricproperties of a questionnaire to assess barriers to feeding critically illpatients. Implement Sci. 2013;8:140.
5. Stevens BJ, Yamada J, Promislow S, Stinson J, Harrison D, Victor JC.Implementation of multidimensional knowledge translation strategies toimprove procedural pain in hospitalized children. Implement Sci. 2014;9:120.
6. Cook D, Meade M, Hand L, McMullin J. Toward understanding evidenceuptake: semirecumbency for pneumonia prevention. Crit Care Med.2002;30:1472–7.
7. Sinuff T, Kahnamoui PK. Cook MsDJ, Giacomini MsM. Practice guidelines asmultipurpose tools: a qualitative study of noninvasive ventilation. Crit CareMed. 2007;35(3):776–82.
8. Dainty KN, Racz E, Morrison LJ, Brooks SC. Implementation of a post-arrestcare team: understanding the nuances of a team-based intervention.Implement Sci. 2016;11:112.
9. Borgert MJ, Goossens A, Dongelmans DA. What are effective strategies forthe implementation of care bundles on ICUs: a systematic review.Implement Sci. 2015;10:119.
10. van Sluisveld PH, Zegers M, Westert GP, van der Hoeven JG, WollersheimHC. A strategy to enhance the safety and efficiency of handovers of ICUpatients: study protocol of the pICUp study. Implement Sci. 2013;8:67.
11. Blom MJ. Improving quality of intensive care: optimizing audit & feedback withactionable indicators and an action implementation toolbox. 2019. https://dare.uva.nl/search?identifier=8141a8d6-2d95-4857-a066-7a18a0d47c06
12. Cochrane LJ, Olson CA, Murray S, Dupuis M, Tooman T, Hayes S. Gapsbetween knowing and doing: understanding and assessing the barriers tooptimal health care. J Contin Educ Health Prof. 2007;27:94–102.
13. Kajermo KN, Boström A-M, Thompson DS, Hutchinson AM, Estabrooks CA,Wallin L. The BARRIERS scale -- the barriers to research utilization scale: asystematic review. Implement Sci. 2010;5:32.
14. Baker R, Camosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, et al.Tailored interventions to overcome identified barriers to change: effects onprofessional practice and health care outcomes. Cochrane Database SystRev. 2010;3:CD005470. https://doi.org/10.1002/14651858.CD005470.pub2.
15. de Vos ML, Van der Veer SN, Wouterse B, Graafmans WC, Peek N, de NF K,et al. A multifaceted feedback strategy alone does not improve theadherence to organizational guideline-based standards: a clusterrandomized trial in intensive care. Implement Sci. 2015;10:95.
16. Sinuff T, Cook D, Giacomini M, Heyland D, Dodek P. Facilitating clinicianadherence to guidelines in the intensive care unit: a multicenter, qualitativestudy. Crit Care Med. 2007;35:2083–9.
17. Harvey G, Kitson A. PARIHS revisited: from heuristic to integrated frameworkfor the successful implementation of knowledge into practice. ImplementSci. 2016;11:33.
18. Balbale SN, Hill JN, Guihan M, Hogan TP, Cameron KA, Goldstein B, et al.Evaluating implementation of methicillin-resistant Staphylococcus aureus(MRSA) prevention guidelines in spinal cord injury centers using the PARIHSframework: a mixed methods study. Implement Sci. 2015;10:130.
19. Förberg U, Unbeck M, Wallin L, Johansson E, Petzold M, Ygge B-M, et al.Effects of computer reminders on complications of peripheral venouscatheters and nurses’ adherence to a guideline in paediatric care—a clusterrandomised study. Implement Sci. 2016;11:10.
20. Brownson RC, Proctor EK, Colditz GA. Future issues in dissemination andimplementation research. In: Brownson RC, Colditz GA, editors.Dissemination and Implementation Research in HealthTranslating Science toPractice: Oxford University Press; 2017. p. 482–4.
21. Palinkas L, Horwitz S, Green C, et al. Purposeful sampling for qualitative datacollection and analysis in mixed method implementation research. AdmPolicy Ment Health. 2015;42:533–44.
22. Ritchie J, Spencer L, O’Connor W. Carrying out qualitative analysis. In: RitchieJ, Lewis J, editors. Qualitative Research Practice: a guide for social sciencestudents and researchers. London: Sage; 2003. p. 219–62.
23. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In:Bryman A, Burgess RG, editors. Analyzing Qualitative Data. London, NewYork: Routledge; 1994. p. 173–94.
24. Tabak RG, Chambers DA, Hook M, Brownson RC. The conceptual basis fordissemination and implementation research lessons from existing modelsand frameworks. In: Brownson RC, Colditz GA, editors. Dissemination andImplementation Research in HealthTranslating Science to Practice: OxfordUniversity Press; 2017. p. 73.
25. Stetler CB, Damschroder LJ, Helfrich CD, Hagedorn HJ. A guide for applyinga revised version of the PARIHS framework for implementation. ImplementSci. 2011;6:99.
26. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC.Fostering implementation of health services research findings into practice:a consolidated framework for advancing implementation science.Implement Sci. 2009;4:50.
Steffen et al. Implementation Science (2021) 16:15 Page 14 of 15

27. Cane J, O’Connor D, Michie S. Validation of the theoretical domainsframework for use in behaviour change and implementation research.Implement Sci. 2012;7:37.
28. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM,Proctor EK, Kirchner JE. A refined compilation of implementation strategies:results from the Expert Recommendations for Implementing Change (ERIC)project. Implement Sci. 2015;10:21.
29. Miles MB, Huberman AM, Saldana J. Qualitative data analysis: a methodssourcebook. 3rd ed. Los Angeles: Sage; 2014.
30. Powell BJ, McMillen JC, Proctor EK, Carpenter CR, Griffey RT, Bunger AC,et al. A compilation of strategies for implementing clinical innovations inhealth and mental health. Med Care Res Rev. 2012;69:123–57.
31. Nilsen P. Making sense of implementation theories, models and frameworks.Implement Sci. 2015;10:53.
32. Kilbourne AM, Neumann MS, Pincus HA, Bauer MS, Stall R. Implementingevidence-based interventions in health care: application of the replicatingeffective programs framework. Implement Sci. 2007;2:42.
33. Aarons G, Aarons G, Hurlburt M, Hurlburt M, Horwitz S, Horwitz S.Advancing a conceptual model of evidence-based practice implementationin public service sectors. Adm Policy Ment Health. 2011;38:4–23.
34. Mitchell R, Parker V, Giles M, White N. Review: toward realizing the potentialof diversity in composition of interprofessional health care teams. Med CareRes Rev. 2010;67:3–26.
35. Proctor EK, Powell BJ, McMillen JC. Implementation strategies:recommendations for specifying and reporting. Implement Sci. 2013;8:139.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Steffen et al. Implementation Science (2021) 16:15 Page 15 of 15