Embed Size (px)
Citation preview
Implementing Mandatory Health Insurance – Lessons from Abu Dhabi
Discussion Material – June 2013
2
Agenda
2
The Abu Dhabi Experience
Potential Lessons for Others
Discussion
3
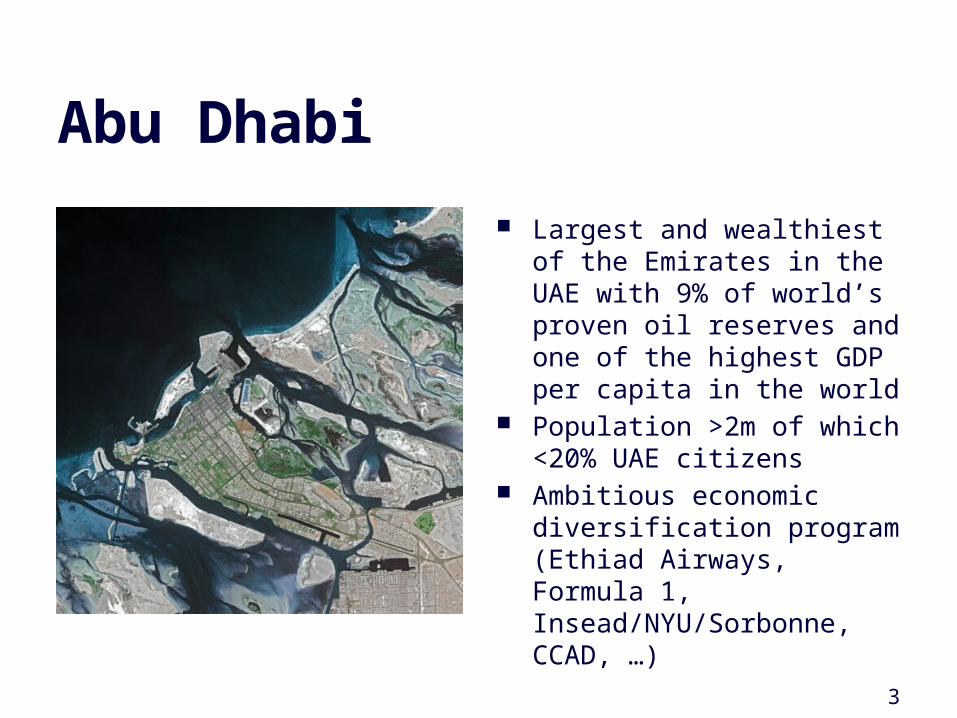
Abu Dhabi
Largest and wealthiest of the Emirates in the UAE with 9% of world’s proven oil reserves and one of the highest GDP per capita in the world
Population >2m of which <20% UAE citizens
Ambitious economic diversification program (Ethiad Airways, Formula 1, Insead/NYU/Sorbonne, CCAD, …)
Health System Challenges Prior to Health Insurance
Lack of access
Lack of clinical and financial transparency
Overreliance on public funding
• Lack of meaningful access especially for low-earning individuals
• Lack of choice for UAE Nationals (public sector free only)
• Limited data without ties between financial and clinical performance (“are we getting value for money?”)
• Public funding not based on activity (block budget)• Perceived lack of customer responsiveness in public sector
as a result• Employers not adequately sharing in cost of providing
health care especially for expatriates
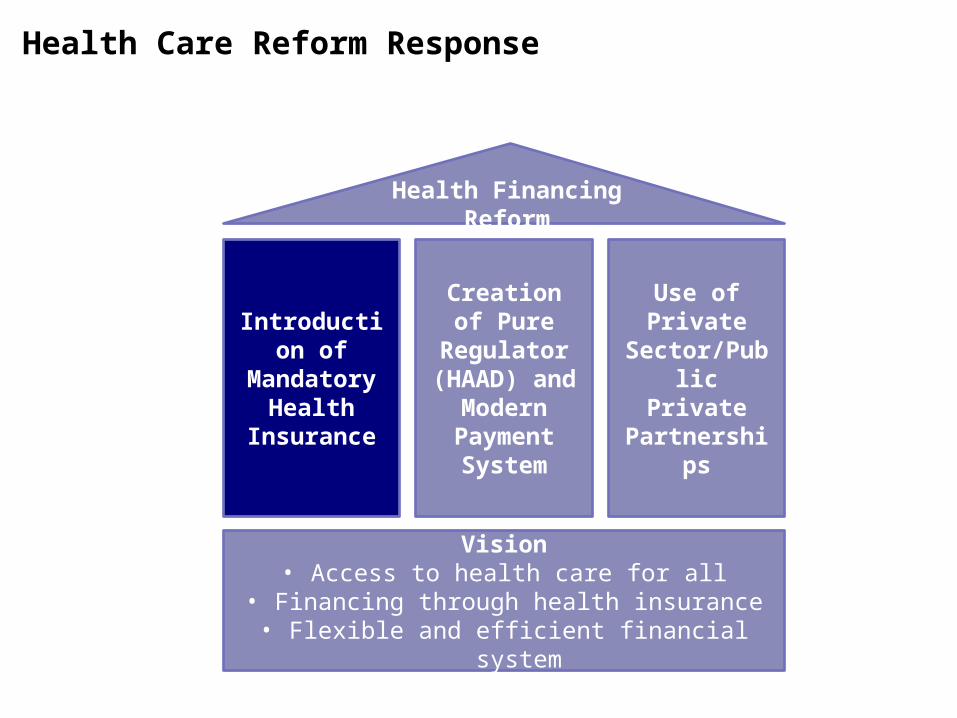
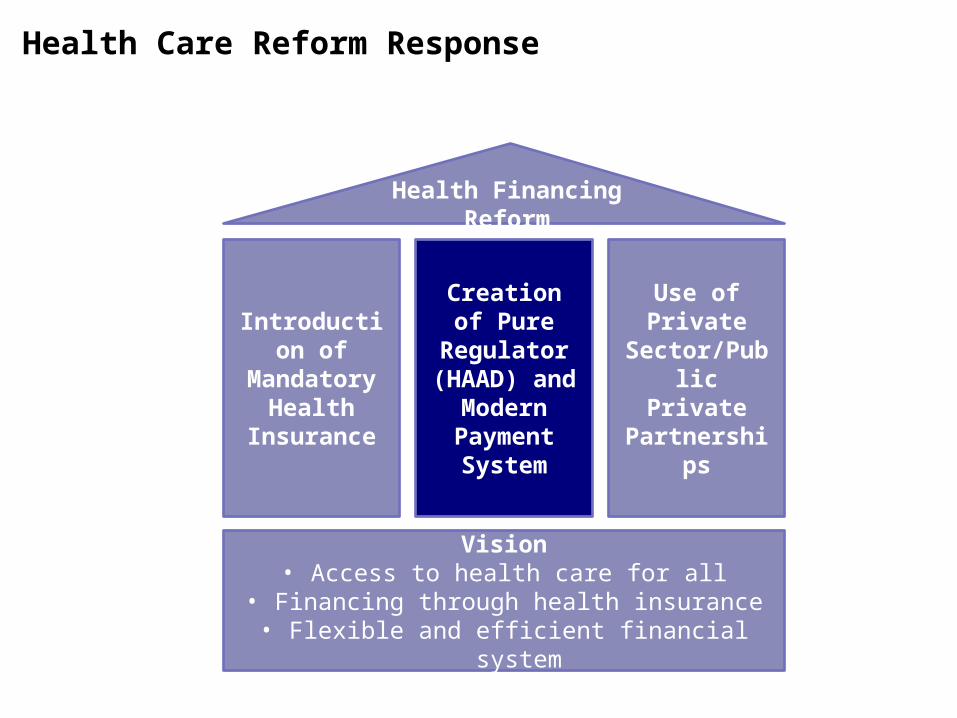
Health Care Reform Response
Introduction of Mandatory
Health Insurance
Creation of Pure Regulator
(HAAD) and Modern Payment System
Use of Private Sector/Public
Private Partnerships
Health Financing Reform
Vision• Access to health care for all
• Financing through health insurance• Flexible and efficient financial system
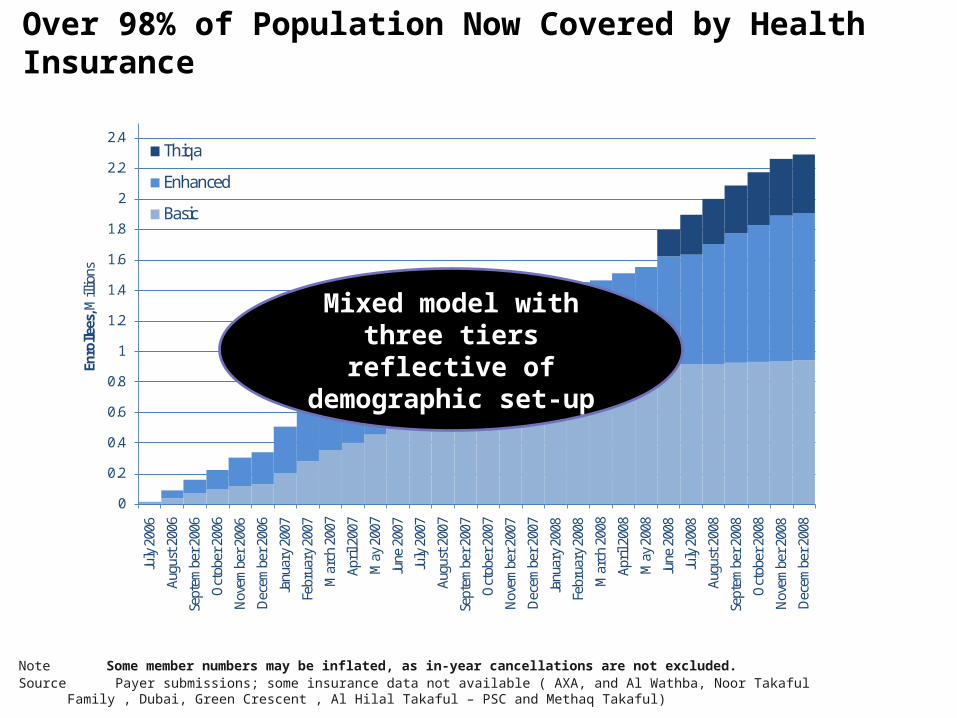
Over 98% of Population Now Covered by Health Insurance
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
2.2
2.4Ju
ly 2
006
Augu
st 2
006
Sept
embe
r 200
6
Oct
ober
200
6
Nov
embe
r 200
6
Dec
embe
r 200
6
Janu
ary
2007
Febr
uary
200
7
Mar
ch 2
007
Apri
l 200
7
May
200
7
June
200
7
July
200
7
Augu
st 2
007
Sept
embe
r 200
7
Oct
ober
200
7
Nov
embe
r 200
7
Dec
embe
r 200
7
Janu
ary
2008
Febr
uary
200
8
Mar
ch 2
008
Apri
l 200
8
May
200
8
June
200
8
July
200
8
Augu
st 2
008
Sept
embe
r 200
8
Oct
ober
200
8
Nov
embe
r 200
8
Dec
embe
r 200
8
Enro
llees
, Mill
ions
Thiqa
Enhanced
Basic
Note Some member numbers may be inflated, as in-year cancellations are not excluded.Source Payer submissions; some insurance data not available ( AXA, and Al Wathba, Noor Takaful Family , Dubai, Green Crescent , Al Hilal Takaful – PSC and
Methaq Takaful)
Mixed model with three tiers reflective of
demographic set-up
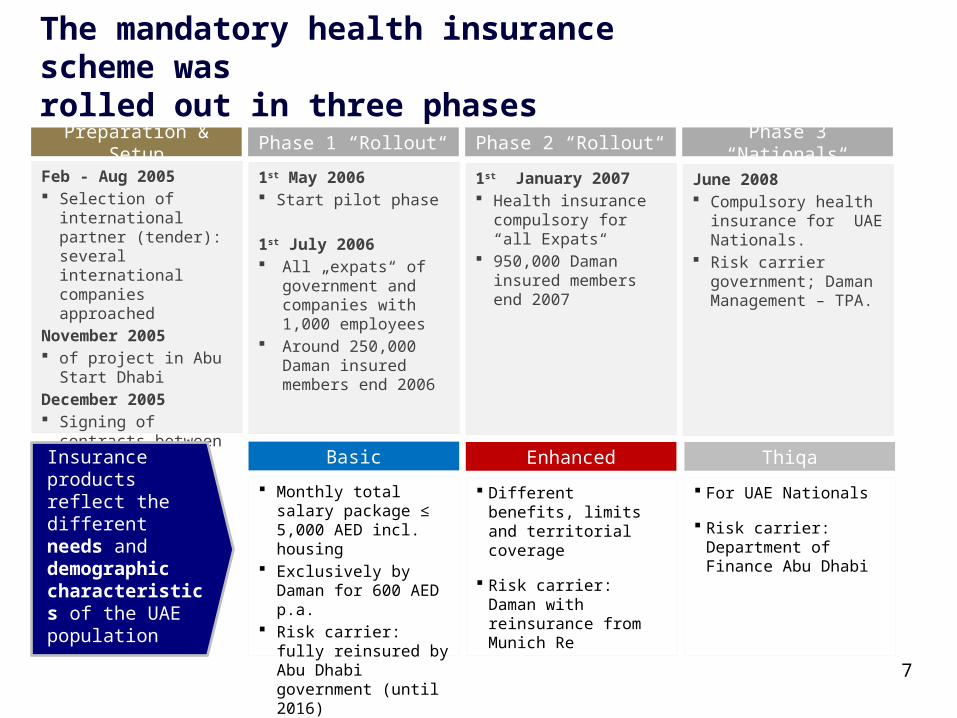
The mandatory health insurance scheme was rolled out in three phases
7
Preparation & Setup
Feb - Aug 2005 Selection of international
partner (tender): several international companies approached
November 2005 of project in Abu Start
DhabiDecember 2005 Signing of contracts
between Daman and Munich Re
Phase 1 “Rollout“
1st May 2006 Start pilot phase
1st July 2006 All „expats“ of
government and companies with 1,000 employees
Around 250,000 Daman insured members end 2006
Phase 2 “Rollout“
1st January 2007 Health insurance
compulsory for “all Expats“
950,000 Daman insured members end 2007
Phase 3 “Nationals“
June 2008 Compulsory health
insurance for UAE Nationals.
Risk carrier government; Daman Management – TPA.
Basic Enhanced Thiqa
Monthly total salary package ≤ 5,000 AED incl. housing
Exclusively by Daman for 600 AED p.a.
Risk carrier: fully reinsured by Abu Dhabi government (until 2016)
Different benefits, limits and territorial coverage
Risk carrier: Daman with reinsurance from Munich Re
For UAE Nationals
Risk carrier: Department of Finance Abu Dhabi
Insurance products reflect the different needs and demographic characteristics of the UAE population
8
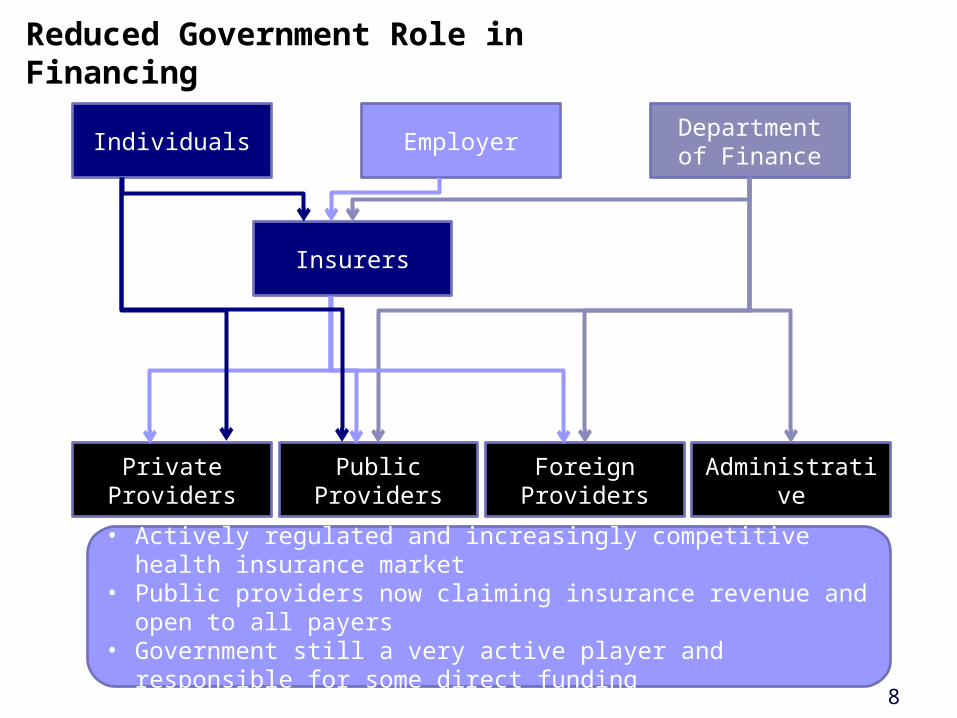
Reduced Government Role in Financing
Individuals Employer Department of Finance
Private Providers Public Providers Foreign Providers Administrative
Insurers
• Actively regulated and increasingly competitive health insurance market• Public providers now claiming insurance revenue and open to all payers• Government still a very active player and responsible for some direct
funding
Health Care Reform Response
Introduction of Mandatory
Health Insurance
Creation of Pure Regulator
(HAAD) and Modern Payment System
Use of Private Sector/Public
Private Partnerships
Health Financing Reform
Vision• Access to health care for all
• Financing through health insurance• Flexible and efficient financial system
10
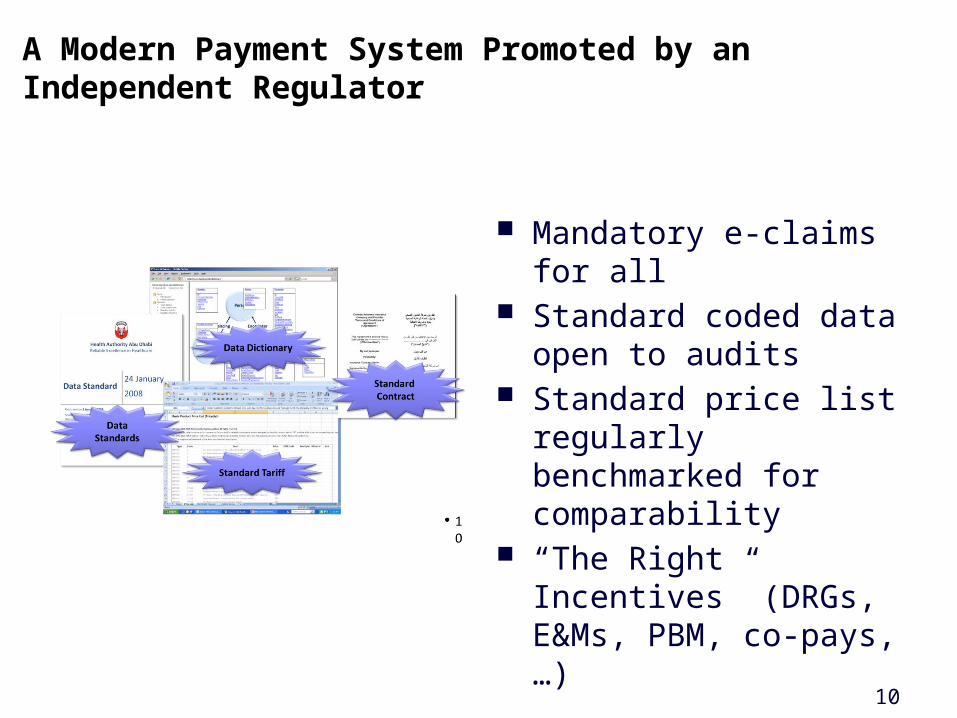
Mandatory e-claims for all Standard coded data open
to audits Standard price list regularly
benchmarked for comparability
“The Right Incentives” (DRGs, E&Ms, PBM, co-pays, …)
A Modern Payment System Promoted by an Independent Regulator
11
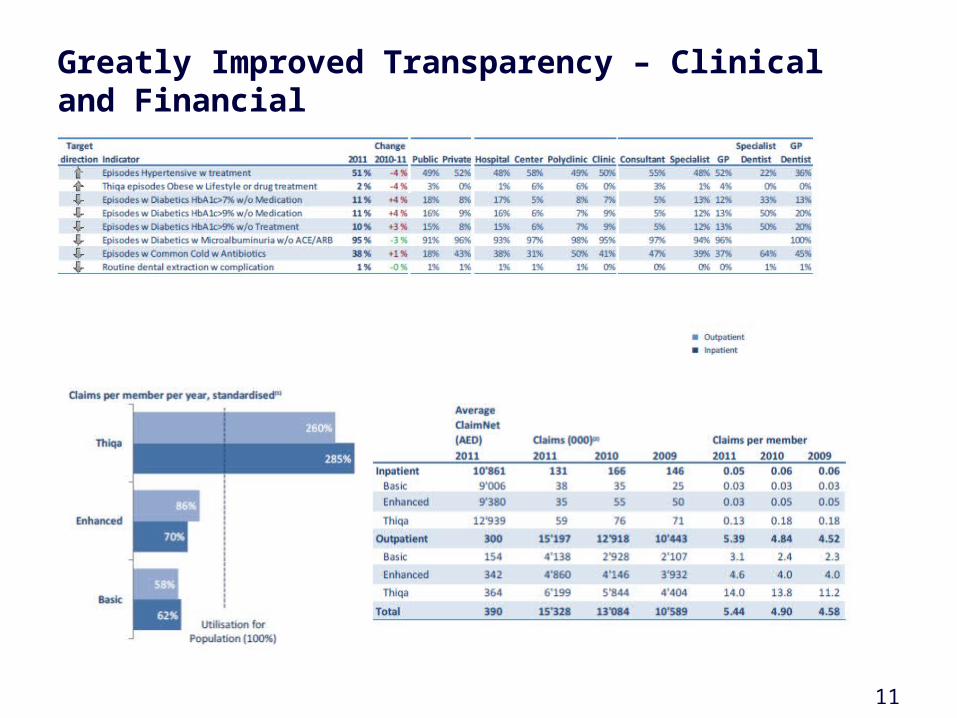
Greatly Improved Transparency – Clinical and Financial
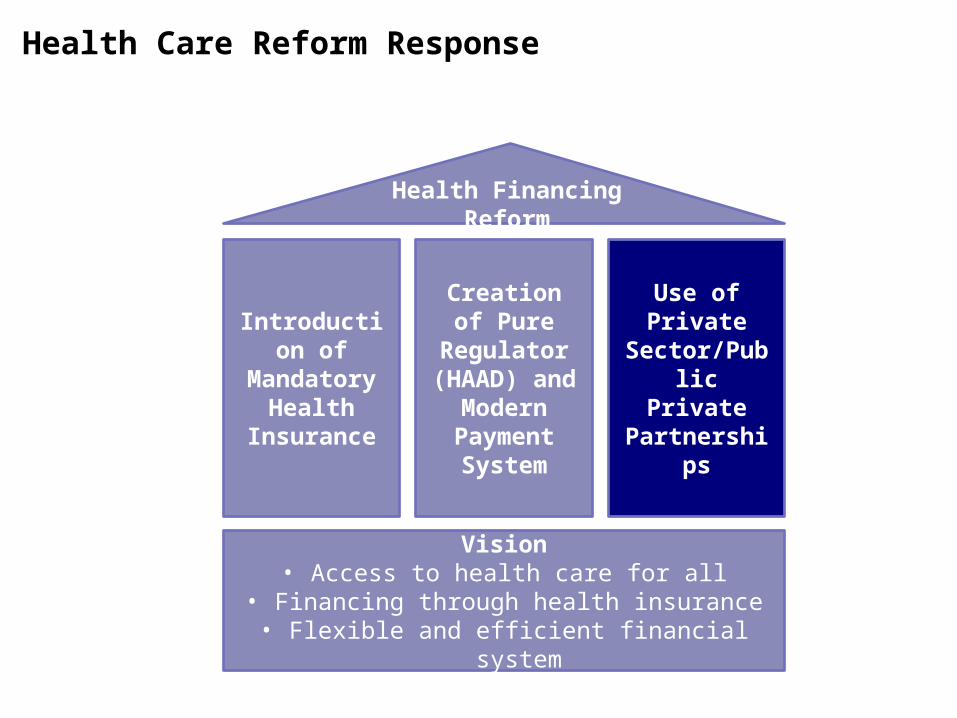
Health Care Reform Response
Introduction of Mandatory
Health Insurance
Creation of Pure Regulator
(HAAD) and Modern Payment System
Use of Private Sector/Public
Private Partnerships
Health Financing Reform
Vision• Access to health care for all
• Financing through health insurance• Flexible and efficient financial system
13
PPP started with MunichRe as an operator of DAMAN providing systems and management
Building trust with the government after successful execution of mandatory health insurance, MunichRe became a shareholder
Now both are jointly expanding locally (broader product range) and regionally (KSA, Qatar, …)
DAMAN – Example for a Successful PPP Model
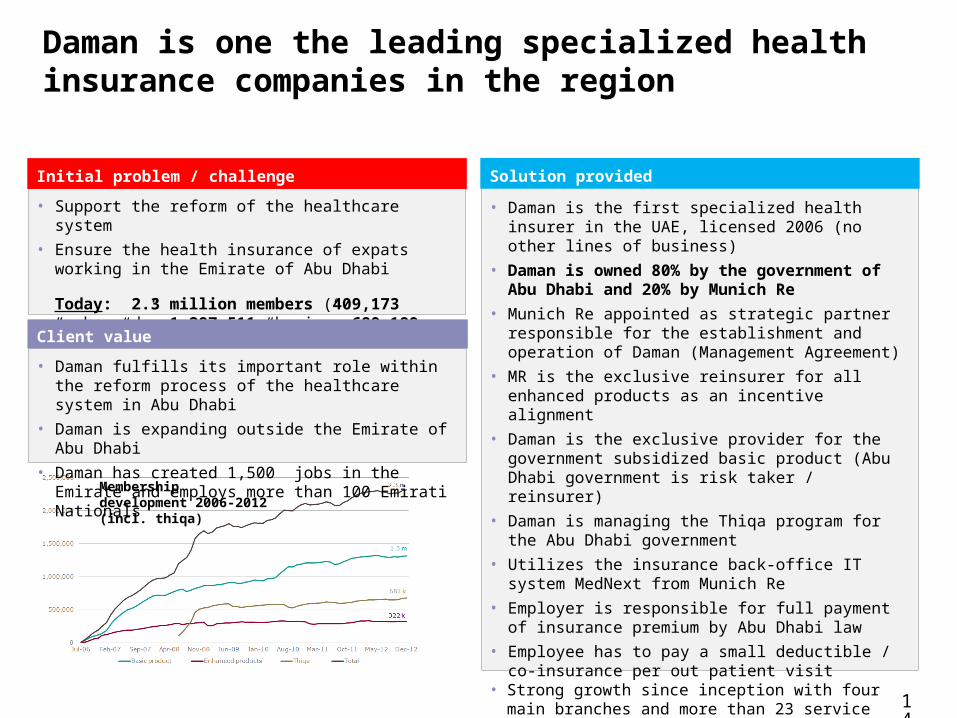
Daman is one the leading specialized health insurance companies in the region
• Support the reform of the healthcare system• Ensure the health insurance of expats working in the Emirate
of Abu Dhabi
Today: 2.3 million members (409,173 “enhanced”; 1,287,511 “basic”; 689,189 “Thiqa”)
Initial problem / challenge
• Daman fulfills its important role within the reform process of the healthcare system in Abu Dhabi
• Daman is expanding outside the Emirate of Abu Dhabi• Daman has created 1,500 jobs in the Emirate and employs
more than 100 Emirati Nationals
Client value
• Daman is the first specialized health insurer in the UAE, licensed 2006 (no other lines of business)
• Daman is owned 80% by the government of Abu Dhabi and 20% by Munich Re
• Munich Re appointed as strategic partner responsible for the establishment and operation of Daman (Management Agreement)
• MR is the exclusive reinsurer for all enhanced products as an incentive alignment
• Daman is the exclusive provider for the government subsidized basic product (Abu Dhabi government is risk taker / reinsurer)
• Daman is managing the Thiqa program for the Abu Dhabi government
• Utilizes the insurance back-office IT system MedNext from Munich Re
• Employer is responsible for full payment of insurance premium by Abu Dhabi law
• Employee has to pay a small deductible / co-insurance per out patient visit
• Strong growth since inception with four main branches and more than 23 service points across the UAE
Solution provided
Membership development 2006-2012 (incl. thiqa)
14
15
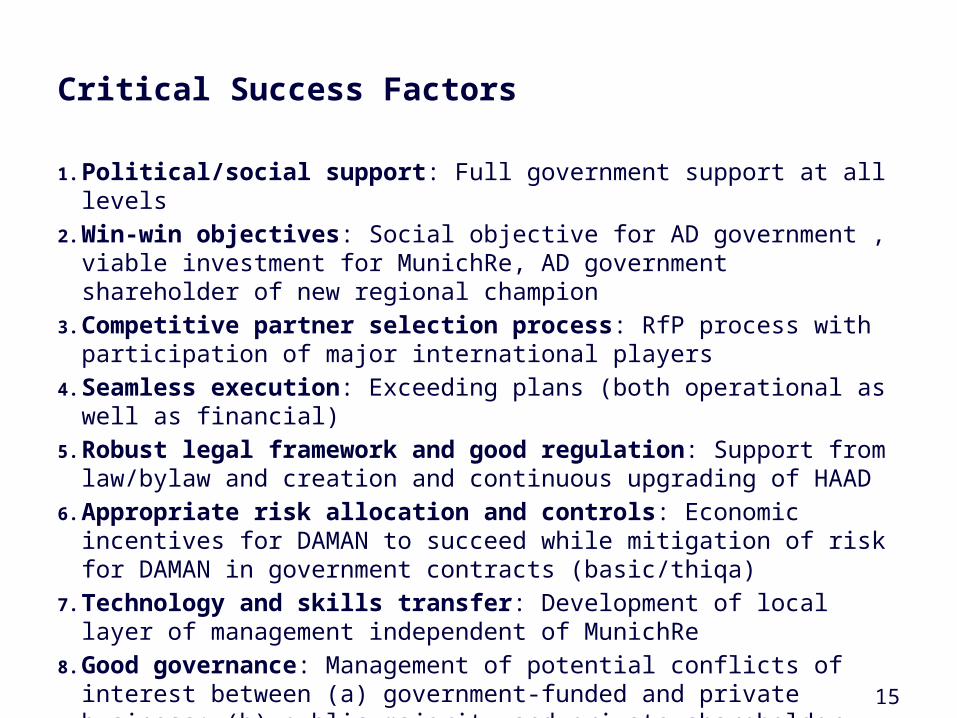
Critical Success Factors
1. Political/social support: Full government support at all levels2. Win-win objectives: Social objective for AD government , viable investment for
MunichRe, AD government shareholder of new regional champion3. Competitive partner selection process: RfP process with participation of major
international players4. Seamless execution: Exceeding plans (both operational as well as financial)5. Robust legal framework and good regulation: Support from law/bylaw and creation
and continuous upgrading of HAAD6. Appropriate risk allocation and controls: Economic incentives for DAMAN to
succeed while mitigation of risk for DAMAN in government contracts (basic/thiqa)7. Technology and skills transfer: Development of local layer of management
independent of MunichRe8. Good governance: Management of potential conflicts of interest between (a)
government-funded and private business; (b) public majority and private shareholder
16
Agenda
16
The Abu Dhabi Experience
Potential Lessons for Others
Discussion
17
Clarify Your Intentions First
Protect against risk of financial ruin and increase access to services?
Shift financing burden from government to employers/employees?
Increase financial/clinical transparency and increase efficiency through better incentives?
Make people happy through more choice (public and private) and increase customer responsiveness of providers (money follows patients)?
What is your ability to stomach potential cost increases as a
result?
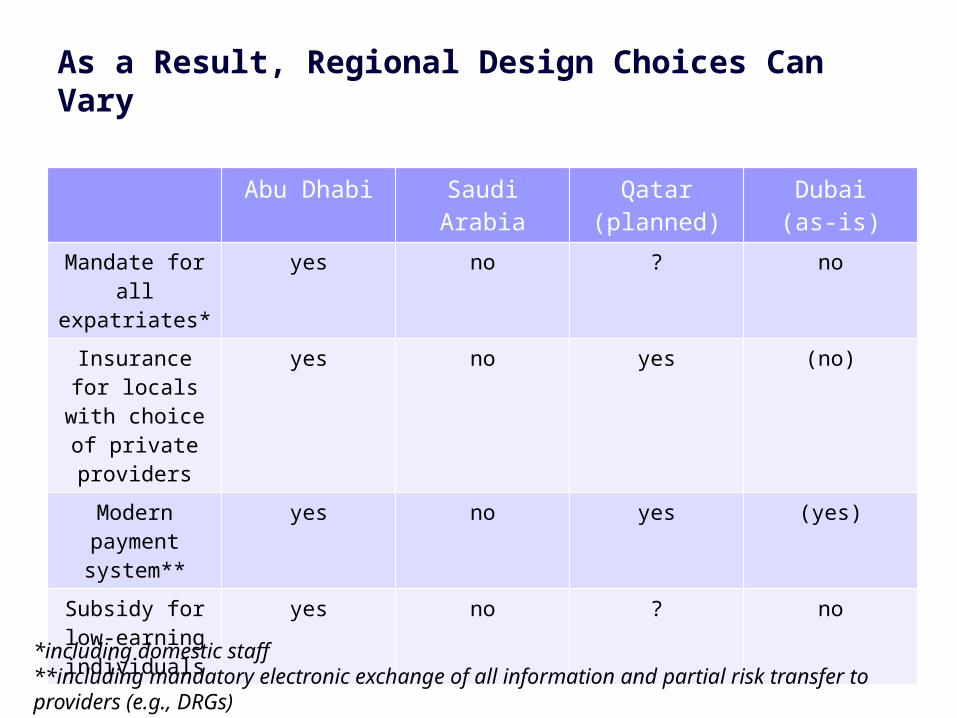
As a Result, Regional Design Choices Can Vary
Abu Dhabi Saudi Arabia Qatar (planned) Dubai(as-is)
Mandate for all expatriates*
yes no ? no
Insurance for locals with choice
of private providers
yes no yes (no)
Modern payment system**
yes no yes (yes)
Subsidy for low-earning
individuals
yes no ? no
*including domestic staff**including mandatory electronic exchange of all information and partial risk transfer to providers (e.g., DRGs)
19
Carefully Prepare for a PPP
Are you ready to accelerate the implementation of health insurance with imported technical skills in a PPP structure
Can you clearly communicate your intentions to an external partner in a PPP venture
Can you manage the complexity inherent in the creation of an able regulator and are you willing to adequately staff and pay for such a function which is needed as a counterpart in any PPP structure
Do you have the contract management skills to set up and monitor a PPP structure with incentives for both sides to succeed
20
Agenda
20
The Abu Dhabi Experience
Potential Lessons for Others
Discussion