Embed Size (px)
DESCRIPTION
Improving prophylactic treatment of gbs positive obstetrical patients. Michelle Blythers Quality Improvement Project Professional Development Perspectives Nursing 3192 January 29, 2014. Group B Streptococcus (GBS). - PowerPoint PPT Presentation
Citation preview

IMPROVING PROPHYLACTIC TREATMENT OF GBS
POSITIVE OBSTETRICAL PATIENTS
Michelle BlythersQuality Improvement Project
Professional Development PerspectivesNursing 3192
January 29, 2014

Group B Streptococcus (GBS)
According to Verani, McGee, and Schrag (2010), GBS is the leading cause of sepsis in the early newborn period, which is defined as the first week of life.
The Centers for Disease Control and Prevention (CDC, 2010), has published revised guidelines for GBS disease prevention.
http://office.microsoft.com/en-us/images/results.aspx?qu=baby&CTT=1#ai:MP900448395

Group B Streptococcus (GBS)
A high priority should be placed on development of a vaccine for GBS as well as an accurate rapid diagnostic test for those patients that present in preterm labor (Valkenburg-van den Burg et al., 2010).
http://www.trcpodcast.com/wp-content/uploads/2013/11/vaccine.gif

• Swab lower vagina and rectum• Collect during 35-37 weeks gestation• Store specimen at 4°C • Process specimen within 24 hours• Intrapartum prophylactic antibiotic
therapy for at least 4 hours before delivery, depending on patient allergy or bacteria resistance
(CDC, 2010)
Current CDC Recommendations

PROBLEMS• Specimens are not collected at the
recommended time
• Specimens are not processed according to the guidelines
1. Sensitivity required if patient has penicillin (PCN) allergy
• Lack of communication among team members1. GBS status2. Patient allergies3. Timely medication orders

PROBLEMS
• Delayed medication administration1. Pharmacy lag time2. Nursing delay
• Lack of education1. Patients should acknowledge importance of
prenatal care at recommended intervals and timely arrival to hospital when in labor
2. Staff should review current guidelines and discuss any updates during each shift report

In an effort to reduce infant morbidity and mortality, we should ensure:
• Proper/timely specimen collection/processing
• No delay in antibiotic therapy/appropriate medication in relation to penicillin allergy and bacteria resistance
• Good communication between obstetrical team members
• Appropriate patient/staff education
Where are improvements needed?

Quality Improvement Team
• Obstetrical Nurses• Obstetrical Providers
1. Obstetricians/Family Practice2. Certified Nurse Midwives
• Residents• Pharmacy • Laboratory

• Committee selected to ensure adherence to guidelines
• Review Laboratory Protocol for GBS culture processing
• Review Clinic Protocol for GBS culture collection
• Ensure all obstetrical team members are educated on current guidelines
• Educate patients on importance of prenatal care and antibiotic therapy when culture is positive
• Audit deliveries monthly to track non-adherence to CDC guidelines
• Committee publishes report with recommendations for improvement
Action Plan

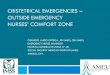
IMPROVING PROPHYLACTIC
TREATMENTOF GBS POSITIVE
OBSTETRICALPATIENTS
SPECIMEN STAFF
GBS PROTOCOL PROCESS IMPROVEMENT
Nurses
Physicians/Midwives/Residents
Processing within 24 hours
Appropriate Storage
Timely Collection
Penicillin
Clindamycin
Vancomycin
MEDICATION
35-37 weeks
4• C
Vaginal/Rectal swab
EDUCATION/COMMUNICATION
Pharmacy
Laboratory
For PCN allergy
For Clindamycin resistance
Current guidelines/Updates
Patient
Team Handoff/ Shift Report
Importance of prenatal care/timely hospital admission
Timely medication delivery
Include sensitivity if PCN allergy Follow processing guidelines
Timely medication administration
Follow protocols/educate patients

Summary
• Surveillance of appropriate prenatal screening for GBS– Timely collection, processing per guidelines
• Antibiotic therapy as recommended– Appropriate alternative as required due to allergy or
sensitivity– Timely administration at appropriate intervals– Reduced number of inadequately treated patients– Reduced number of newborns with GBS infection

Summary
• Education– Current guidelines/updates– Patient acknowledgment
• Communication– Timely/complete status report/plan between all
patient care team members

ReferencesCenters for Disease Control and Prevention. (2010). Prevention of Perinatal Group B Streptococcal Disease. Retrieved from http://www.cdc.gov/mmwr/pdf/rr/rr5910.pdf
Valkenburg-van den Berg, A., Houtman-Roelofsen, R., Oostvogel, P., Dekker, F., Dörr, P., & Sprij, A. (2010). Timing of group B streptococcus screening in pregnancy: a systematic review. Gynecologic And Obstetric Investigation, 69(3), 174-183. doi:10.1159/000265942
Verani, J., McGee, L., & Schrag, S. (2010). Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR. Recommendations And Reports: Morbidity And Mortality Weekly Report. Recommendations And Reports / Centers For Disease Control, 59(RR-10), 1-36.