Embed Size (px)
Citation preview

Improving Transitions in Healthcare Delivering Value and Changing Outcomes Through
Patient Engagement and Technology
A Panel’s Perspective
National Health Leadership Conference June, 2015
Presented by: Helen Brenner, VP & CNE Northumberland Hills Hospital, PATH Executive Lead Maryanne Brown, PATH Gerontology Specialist Wendy Kolodziejczak, PATH Project Manager Moderator, Linda Davis, President and CEO Northumberland Hills Hospital


Marilyn and Jim’s Story
Video

What Makes PATH Different?
(Partners Advancing Transitions in Healthcare)
• A unique and committed community partnership
• Use of Experience Based Co-Design (EBCD) as the improvement methodology
• Authentic engagement of patients/caregivers at every level
• Focused effort that is supported
Learn more about PATH at: http://www.changefoundation.ca/projects/path/

Northumberland Community Partnership
Patients and caregivers recruited from the Northumberland community
Healthcare Providers • Northumberland Hills Hospital
• Northumberland Family Health Team
• NHH Community Mental Health Services
Community Providers • Central East Community Care Access Centre
• Community Care Northumberland
• Golden Plough Lodge Long Term Care Home
• Palisade Gardens Retirement Residence
• YMCA Northumberland
Others • Central East Local Health Integration Network
• Health System Performance Research Network
• Patients’ Canada
• QoC Health (Technology)

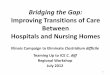
Tier 1: Top 1%
Tier 2: Top 2 - 20%
Tier 3: Bottom 21-100%
Frequent acute care, transitions
• 120 Northumberland residents
Periodic acute care, transitions
• 2,300 Northumberland residents
Very rare acute care, transitions
• 9,600 Northumberland residents
• 66% of all acute services
• 32% of all acute services
• 2% of all acute services
Use of acute
services/
frequency of
transitions
[1] Central East LHIN (2011). Building a Model of Sustainable Access to Community Services. May 2011. [online: web] URL: http://www.centraleastlhin.on.ca/uploadedFiles/Home_Page/Board_of_Directors/Board_Meeting_Submenu/SA_Report_-_FINAL_June_2.pdf, p. 38.
PATH Target Population: Seniors living with chronic health conditions

How Did We Engage Seniors/Caregivers?
Proposal Stage: • Project ideas generated based on feedback from seniors & caregivers
involved – what was most meaningful
Story Gathering Phase: • Research study • Results used to inform to co-design teams
PATH Partnership & Organizational Structure: • PATH Committees & Subcommittees • 5 Co-Design Teams • RISE Team
Pilot Phase: • Testing of new processes & technology solutions
Methodology: Experience Based Co-Design

PATH RISE TEAM Respect, Inform, Support, Empower

Pathwaytoagingwell.com
• Community website with information,
resources, and planning tools all in
one place
Patient/Provider Portal & Mobile Technology • Built by seniors for seniors
Person Centered Care Model • Based on what was important to the seniors/caregivers
• Patient/Family Advisor model
Volunteer Transition Coach Service • Opportunity for broader community engagement
• 31 VTC’s to date
What Did We Create Together?

Physician Perspective
Video

NEEDS
BARRIERS
EXPERIENCE
PATH EBCD AND
RESEARCH
Health System Transformation
Health System Transformation
New Ways of Learning & Evaluating

The EBCD Approach – A Service Improvement Methodology
© NHS Institute for Innovation and Improvement 2010. All rights reserved.


EBCD: ASSUMPTIONS, BELIEFS, and
PIVOTAL POINTS
Assumptions & Beliefs: • Consumers of the system don’t know the solutions
• It is too difficult to work together across the system
Pivotal Points: • The power of the “story”- use of “story” has to be front
and central
• Learning how to create an environment where sharing stories moves providers rather than shuts them down
• Set the environment so that people come as people first
• Meaningful engagement
• When the consumer is involved in co-design they are highly invested and are a rich resource

What Were the Results of This Engagement?
For the Senior/Caregiver :
For the System:
An equal voice
Meaningful engagement
Consumers who use the healthcare system the most are included in and have the solutions for system change
Seniors and caregivers are empowered to be more involved in their own care
Breaking down silos
Working from a systems perspective
Hearing and understanding experiences as the focus for system change- pivotal change
Improvement in efficiencies and costs
Real time feedback

PARTICIPATING IN EBCD
VIDEO


NEEDS: ASSUMPTIONS, BELIEFS, and
PIVOTAL POINTS
Assumptions & Beliefs:
• Patient’s can’t identify their own needs
• Their needs won’t be reasonable or time limited
• Healthcare workers know best
Pivotal Points:
• Hearing the story, understanding the story, and knowing the impact on the persons quality of health and life
• Understanding the waste and inefficiencies in the system
• One size does not fit all – people live with multiple & different types of chronic illnesses


TRANSITIONS: ASSUMPTIONS, BELIEFS, and
PIVOTAL POINTS
Assumptions & Beliefs:
• Seniors can’t bring and share accurate and valuable health information with providers
• The provider can acquire accurate information in stressful health situations
Pivotal Points:
• The patient/caregiver is the only constant in the system
• Patient/caregiver needs to be central in technology solutions
• Reduces duplication, creates efficiencies, reduces costs
• Opportunity for real time feedback after every healthcare encounter


HEALTHCARE CONSUMERS: ASSUMPTIONS,
BELIEFS, and PIVOTAL POINTS
Assumptions & Beliefs:
• Patients/caregivers can’t understand their own health information
• The provider should be the holder of the information
• Seniors can’t use technology
Pivotal Points:
• Patients and caregivers become more engaged and more responsible for their own health when the tools are designed to be meaningful to them
• New IT solutions must be developed together with those who will be using them
• The use of innovative technology can decrease costs to the system


CAREGIVERS: ASSUMPTIONS, BELIEFS,
and PIVOTAL POINTS
Assumptions & Beliefs:
• Caregivers are not an important and integral part of the healthcare circle
• Caregivers are often excluded from the conversation
Pivotal Points:
• Informal caregivers are the coordinators of care
• Caregiver needs must be attended to and supported
• Caregiver burnout must be prevented


VTC’S: ASSUMPTIONS, BELIEFS, and
PIVOTAL POINTS
Assumptions & Beliefs:
• Providers know what is best for patients
• Providers feel the medical perspective is more important than the lived experience
Pivotal Points:
• We have a huge untapped resource in each of our communities
• The design of the role has to be guided by those who will use the service

What Is the Impact for the Senior/Caregiver?
• Engagement in own care
• Empowerment and ownership
• Access to health information
• Ability to monitor conditions from home
• Ability to connect with healthcare providers
• My “needs” matters
• My “experience” matters
• Improved quality of life

What Is the Impact for the System?
• Breaking down silos/working from a systems perspective
• Needs and experiences are central to quality
• Optimizes information for decision making
• Early Intervention and improved responsiveness
• Creates efficiencies by enabling connections to patients without an in person visit
• Improved quality of care
• Provides technology, processes, and models for an integrated system that engages and supports seniors to age well at home

www.changefoundation.ca/projects/path
@NorthlandPATH
www.facebook.com/NorthumberlandPATH
www.pathwaytoagingwell.com
Questions?