Embed Size (px)
DESCRIPTION
In the name of God the compassionate and the merciful. Decentralization of Health System in Islamic Republic of Iran. By Mohammadreza Rahbar MD- MPH [email protected]. Outlines. Definitions Evidences for the necessity of action Indicators Experiences and Analysis 5 Projects - PowerPoint PPT Presentation
Citation preview

Center for Health Network Expansion & Health Promotion
In the name of God the compassionate and the merciful

Center for Health Network Expansion & Health Promotion
Decentralization of Health System in Islamic Republic of Iran
By
Mohammadreza Rahbar

Center for Health Network Expansion & Health Promotion
Outlines
Definitions Evidences for the necessity of action
Indicators
Experiences and Analysis 5 Projects
Lessons should be learnt

Center for Health Network Expansion & Health Promotion
Decentralization
Decentralization is the process of dispersing decision-making closer to the point of service or action.

Center for Health Network Expansion & Health Promotion
Federalism and Decentralisation:
Federalism is often accompanied by decentralisation, but it is not a necessary condition for decentralisation, nor is decentralisation a sufficient condition for federalism.

Center for Health Network Expansion & Health Promotion
Decentralisation and Development
• Decentralized governance, if properly planned and implemented, offers important opportunities for enhanced human development.

Center for Health Network Expansion & Health Promotion
Degrees and Types of Decentralisation by Region
0%20%40%60%80%
100%120%
Sub-SaharanAfrica
East Asiaand
Pacific
SouthAsia
EasternEurope
andCentral
Asia
WesternEurope
MiddleEast andNorthern
Africa
Americas
Fiscal Political None Both

Center for Health Network Expansion & Health Promotion
Decentralization Purposes
Decentralization is a policy pursued for a variety of purposes: Political Administrative Financial.
Many health sector reforms include decentralization as a major component.

Center for Health Network Expansion & Health Promotion
Objectives of Decentralization
Rationale Reasons
EfficacyLocal leaders are better informed about local
problems and can make better decisions
EquityLocal leaders can better target resources to
vulnerable groups
EfficiencyLocal leaders can make more efficient decisions
because they have better information about local conditions
QualityGreater accountability may lead local leaders to
improve quality
Financial Soundness
Local leaders may be more aware of tradeoffs and fiscal constraints.
Local Choice & Priorities
In democratic localities, decentralization can allow more local choice and priority setting

Center for Health Network Expansion & Health Promotion
Areas of decentralization and range of authorities
Range of Choice
Functions Narrow Moderate Wide
FinanceSources of revenue &Allocation of ExpendituresHospital Fees
Service OrganizationRequired Programs Hospital AutonomyInsurance Plans Payment MechanismsContracts with PrivateProviders
Human ResourcesSalariesContractsCivil Service
Access RulesTargeting
Governance RulesLocal accountabilityFacility BoardsDistrict OfficesCommunity Participation
Mapping Decision making for Decentralization

Center for Health Network Expansion & Health Promotion
“Decentralization” of the Iranian Health System - The Challengeable Road From Relative Central plans
to Decentralism
The ChallengeTransition from a relative bureaucratic centralized to a
functional decentralized system

Center for Health Network Expansion & Health Promotion
Network Development Center and Health Promotion Technical OfficesTechnical OfficesM I N I S T R Y O F H E A L T H
CommunityNeedsNeeds
Demands Demands
Insurance Plans
Health Facilities / Providers
Resource Providers
Epidemiologic studies
Utilization Studies
Problem priority
EffectiveInterventions Developing
Resource AllocationBased on
Quality, EfficiencyEquity, Effectiveness
AndOthers
Considerations
Feasibility Study
Integration and
Stratification
New Program Designing
Functional areas in the Health System
Center for Health Network Expansion & Health Promotion
Necessities for Decentralization in Iran
• Local leaders are better informed about local problems and available resources and can make better decisions in Different; • Community health status, • Health related risk factors,• Utilization,• Available resources,• Opportunities and threats and• Weaknesses and strengths

Center for Health Network Expansion & Health Promotion
راهبردهاياقتصادي اجتماعيزيست ومحيط
سيگار
غذايي عادات
جنس ؛ سن وژنتيك
دات عاخواب
ك تحر
سواد
مناسباتجنسي
شرايط زندگي
مخدر مواد
تماسهاينسلي بين
و كشاورزيتغذيه
ترافيك
كار شرايط
الكل
و فرهنگتفريحات
هاي شبكه= اجتماعي خانواده
خدماتبهداشتي
هاي حمايتاجتماعي
اجتماعي رفاه
§ تامين اجتماعي
? بيكاري
Multifactorial complex effects of Health Determinants

Center for Health Network Expansion & Health Promotion
Mortality &
Morbidity
Development Situation
Lit
erac
y
Social structure
capacities
Une
mpl
oym
ent
rat
e
State of welfare
Nut
ritio
n
Uti
liza
tion
Age
Pyramid
Rep
rodu
ctive b
ehaviors

Center for Health Network Expansion & Health Promotion
0
2
4
6
8
10
12
14
" Zscoreمولفهموردمطالعه
عه
طالمرد
موعهاق
ويع
وزت
توزيع نا همگن در سمت صعودي مولفه توزيع نا همگن در سمت صعودي مولفهتوزيع نرمال با پراكندگي زيا د توزيع نرمال در حول ميانگين
Different kinds of distributions of events related to the health

Center for Health Network Expansion & Health Promotion
Some evidences from surveys
For the necessity of decentralization

Center for Health Network Expansion & Health Promotion
Standard
Crude
Crude and standardized registered cases for Non-Intentional accidents for rural and Urban areas for 29 provinces in 2003
for 100000 population

Center for Health Network Expansion & Health Promotion
Standard
Crude
The crude and standardized death rate for cardiovascular disease for 29 provinces- 2004 in
100,000 people

Center for Health Network Expansion & Health Promotion
Standard
Crude
The crude and standardized death rate for Infectious disease for 29 provinces- 2004in 100,000 people

Center for Health Network Expansion & Health Promotion
Standard
Crude
The crude and standardized death rate for cancer of stomach for 29 provinces- 2004 in 100,000 people

Center for Health Network Expansion & Health Promotion
Standard
Crude
The crude and standardized death rate for Diabetes for 29 provinces- 2004in 100,000 people
Center for Health Network Expansion & Health Promotion
Standard
Crude
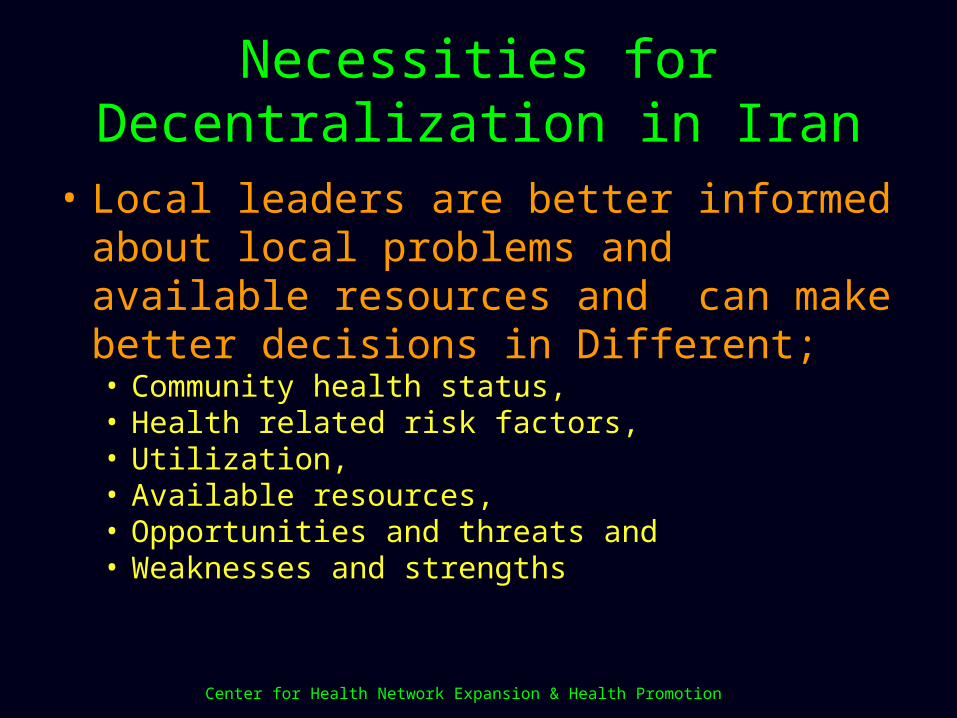
The crude and standardized death rate for Intentional accidents for 29 provinces- 2004 in 100,000 people

Center for Health Network Expansion & Health Promotion
The crude and standardized death rate registered for Traffic accidents for 29 provinces- 2004 in 100,000 people
Standard
Crude

Center for Health Network Expansion & Health Promotion
مراقبت تحت كه سال شش زير دكان كو از نسبتي ( ) گفته) به دارند قرار وورن قد گيري اندازه بهداشتي
سال ( پاييز وروستا شهر تفكيك به مطالعه 1383مادر2انيس
94
91
94
82
74
79
85
77
82
70
65
91
57
84
78
66
76
74
64
77
82
86
77
74
72
79
65
69
65 65
50
60
70
80
90
100
نسمنا
ي
ارتيخلب
حارم
هاچ
هرش
وب
نصفها
ا
قم زدي
نستا
ردك
نمدا
ه
لدبي
را
ندرا
زنما
سراف
نجا
زن
ي
غربن
جااي
ربذ
آ
يكز
رم
ناستگل
الماي
يشرق
نجا
ايربذ
آ
نسا
خرا
)
شدهون
وزم
( ورش
ك
نال
گي
هشاانرمك
نرما
ك
نزوي
ق
يمد
حرا
ويوب
هلوي
هكيك
ناستر
ل
نستا
وزخ
ن
اچست
لونوب
استسي
نهرا
جزتن
هرانت
ستاا
نگامزهر
نهرا
تشهر
روستاشهر
Rural
Urban
The proportion of the children under 6 who utilized by growth monitoring services (assessments of weight and
height) according to the mother's statement in rural and urban areas in 2003- ANIS survey

Center for Health Network Expansion & Health Promotion
يي آنها رشد كارت در رشد منحني ترسيم وضعيتاستان تفكيك به بود شده آنهامشاهده كارت كه
سال انيس 1383پاييز 2مطالعه
0
10
20
30
40
50
60
70
ل حارم
چها
لدبي
را
نسمنا
هرش
وب
زدي
سراف
نستا
ردك
نجا
زن قم
نگامزهر
نصفها
ا
يكز
رم
ندرا
زنما
نزوي
ق
الماي
يشرق
ذرآ
نسا
خرا
ورش
ك
نرما
ك
ي
غربذر
آ
هشاانكرم
نمدا
ه
نستا
رل
نال
گي
ه لوي
هكيك
نستا
گل
نهرا
نتستا
ا
نستا
وزخ
ن
هراتشهر
بون
ستاسي
منحنيرشدكاملترسيمشده قطعترسيمشده يكيدو منحنيرشدبا شدهترسيمشده تكه منحنيرشدناقصوتكه است شده حنيرشدترسيمن Completely drawnمن Relatively complete drawn Incomplete drawn Have not drawn
The situation of drawing growth monitoring chart for those who had checked for it
in 2003- ANIS survey

Center for Health Network Expansion & Health Promotion
اي تغذيه قدي ه كوتا Z برحسب ( STUNTING )توزيعScore سن براي قد اقليم ) ( HAZ ) ؛ دو اقليم سه براي
) پورا مطالعه در اقليم بهترين و طيف انتهايبهار) ( ايران مغذيهاي ريز دروضعيت پژوهشي
كودكان , 1380 سني هه 23تا 15گروه ما
0
5
10
15
20
25
-4.25 -3.75 -3.25 -2.75 -2.25 -1.75 -1.25 -0.75 -0.25 0.25 0.75 1.25 1.75 2.25 2.75 3.25 3.75 4.25
انحرافمعيار
صد
در
استاندارد دران گيالنومازنجنوبخراسانوجنوبكرمانوسيستانوبلوچستان ان بوشهروهرمزگانوجنوبخوزست
Distribution of Stunting for 15 to 23 months children due to nutrition according to Z Score of Height for age (HAZ)
for 3 different climate regions Micronutrients Survey- Spring 2000
Read line= Standard

Center for Health Network Expansion & Health Promotion
اي تغذيه قدي ه كوتا قد Z Score برحسب ( STUNTING )توزيع ؛سن و ) ( HAZ ) براي طيف انتهاي اقليم دو اقليم سه براي
( ) ريز دروضعيت پژوهشي پورا مطالعه ؛ اقليم بهترينبهار ( ايران كودكان , 1380مغذيهاي سني ساله6گروه
0
5
10
15
20
25
-4.25 -3.75 -3.25 -2.75 -2.25 -1.75 -1.25 -0.75 -0.25 0.25 0.75 1.25 1.75 2.25 2.75 3.25 3.75 4.25
انحرافمعيار
صد
در
استاندارد دران گيالنومازنجنوبخراسانوجنوبكرمانوسيستانوبلوچستان ان بوشهروهرمزگانوجنوبخوزست
Distribution of Stunting for 6 yrs children due to nutrition according to Z Score of Height for age (HAZ) for 3 different climate
regions Micronutrients Survey- Spring 2000
Read line= Standard

Center for Health Network Expansion & Health Promotion
وزني كم ؛ Z Score برحسب ( UNDERWEIGHT )توزيعسن براي اقليم ) (WAZ ) وزن سه اقليم چهار براي
) پورا مطالعه در اقليم بهترين و طيف انتهايبهار) ( ايران مغذيهاي ريز دروضعيت پژوهشي
كودكان , 1380 سني هه 23تا 15گروه ما
0
5
10
15
20
25
-4.25 -3.75 -3.25 -2.75 -2.25 -1.75 -1.25 -0.75 -0.25 0.25 0.75 1.25 1.75 2.25 2.75 3.25 3.75 4.25انحرافمعيار
صددر
استاندارد جنوبخراسانوجنوبكرمانوسيستانوبلوچستان ان فارسومركزكرم ان بوشهروهرمزگانوجنوبخوزست
دران گيالنومازن
Distribution of Underweight for 15 to 23 months children due to nutrition according to Z Score of Height for age (HAZ) for 3
different climate regions Micronutrients Survey- Spring 2000
Read line= Standard

Center for Health Network Expansion & Health Promotion
0.1
.2.3
.4.5
.6D
ensi
ty
-1 0 1 2 3 4Permanent income
Iran DHS 2000
Permanent income Province17
0.1
.2.3
.4.5
.6D
ensi
ty
-1 0 1 2 3 4Permanent income
Iran DHS 2000
Permanent income Province12 ايالم استان خانواردر رفاهي امكانات وبلوچستان توزيع سيستان استان خانواردر رفاهي امكانات توزيع
0.1
.2.3
.4.5
.6D
ensi
ty
-1 0 1 2 3 4Permanent income
Iran DHS 2000
Permanent income Province29Permanent Income City of Tehran
0.1
.2.3
.4.5
.6D
ensi
ty
-1 0 1 2 3 4Permanent income
Iran DHS 2000
Permanent income Province11Permanent Income Isfahan Province
Permanent Income Sistan & Baloochestan Province
Permanent Income Ilam Province

Center for Health Network Expansion & Health Promotion
زايمان درصد براي ؛ كشور مختلف استانهاي بين واريانسپوشش ) تحت روستايي جمعيت در نديده دوره فرد توسط
مختلف ( سالهاي تفكيك به بهداشت هاي خانه
103.8
128.2
159.5175.9
212.1226.6
261.9
321.3
354.0
193.3
0
50
100
150
200
250
300
350
400
82818079787776757472سال
سان
اريو
Variation among different provinces for the percentage of deliveries have been done by non-trained attendants for the rural areas being
covered by the Health houses in different years
Year
Variation

Center for Health Network Expansion & Health Promotion
كود مرگ ميزان براي ؛ كشور مختلف استانهاي بين واريانستا يك هاي ) 59كان خانه پوشش تحت روستايي جمعيت در ماه
مختلف ( سالهاي تفكيك به بهداشت
41.0
13.516.7
21.118.2
45.1
39.137.6
58.6
82.9
25.5
0
10
20
30
40
50
60
70
80
90
8281807978777675747372 سال
سيان
ارو
Year
Variation
Variation among different provinces for the 1- 59 months mortality for the rural areas being covered by the Health houses in different
years

Center for Health Network Expansion & Health Promotion
سال در سال پنج زير كودكان مرگ در 1382ميزانكشور بهداشت هاي خانه پوشش تحت روستايي مناطق
55
41
37
33 32 3231 30 30 30 30 29 29 28 28 27 27 26 26
25 24 24 24 24 22 22
18
14
11
0.0
10.0
20.0
30.0
40.0
50.0
60.0
نماكر
نستا
وچبل
ون
ستاسي
نستا
لر
نستا
ردك
نگامز
هر
نسا
راخ
نستا
گل
مدحرا
ويوب
يهلو
گيكه
شاهمان
كر ورش
لکک
ي
ربغن
جابأي
ذرآ
نستا
وزخ
هرش
بو
لدبي
ار
نمدا
ه
يرق
شن
جابأي
ذرآ
سفار
يارختي
وبل
حارم
هاچ
نفها
صا
نويقز
نجا
زن
يکز
مر
نالگي
نمناس زدي
المأي
ندرا
زنما
نراهت
قم
صددر
Under 5 Mortality Rate for the rural areas being covered by the Health houses in 2001

Center for Health Network Expansion & Health Promotion
مرگ ميزان براي ؛ كشور مختلف استانهاي بين واريانسهاي ) خانه پوشش تحت روستايي جمعيت در نوزادان
مختلف ( سالهاي تفكيك به بهداشت
13.8
12.4
10.7
12.3
11.2
15.8
9.6
5.6
9.2
6.9
11.0
0
2
4
6
8
10
12
14
16
18
8281807978777675747372 سال
سيان
ارو
Variation among different provinces for Neonatal Mortality Rate for the rural areas being covered by the Health houses in different years
Year
Variation

Center for Health Network Expansion & Health Promotion
تا يك كودكان مرگ سال 59ميزان در 1382ماههاي خانه پوشش تحت روستايي مناطق در
كشور بهداشت
40
23
14 13 13 13 13 13 12 12 12 12 11 11 11 10 10 10 10 10 10 9 9 8 8 7 7 63
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
نرما
ك
نستا
وچبل
نوستا
سي
نسا
خرا
نستا
وزخ
ي
ربغن
جابأي
ذرآ
ورش
لکک
نستا
لر
شاهمان
كر
مداح
يربو
ويه
لوگي
كه
نستا
گل
نزگا
رمه
سفار
يرق
شن
جابأي
ذرآ
لدبي
ار
يکز
مر
نمدا
ه
يار
ختيوب
لحارم
هاچ
نستا
ردك
المأي
زدي
نمناس
هرش
بو
نفها
صا
نجا
زن
نويقز
ندرا
زنما
نالگي
نهرا
ت
قم
صددر
1- 59 months Mortality Rate for the rural areas being covered by the Health houses in 2001

Center for Health Network Expansion & Health Promotion
y = 0.42 x + 1.01
R2 = 0.53
5
10
15
20
25
30
35
40
10 20 30 40 50 60% نسبتبيسوادي
1000
دراه
م59
تان 1
كاود
كگ
مرت
سبن
ر بها چا
كودكان مرگ نسبت خطي نسبت 59تا 1ارتباط با ماهروستايي مناطق در در 281بيسوادي كشور شهرستان
در- 1381و1380و1379سالهاي شده ثبت اطالعات اساس برومطالعه بهداشت هاي خانه حياتي DHSزيج
شميران ات
نابرابري شاخص بهترين ) ( است بتا خط زوايه ضريب
Vagstaf:2005
Linear relation between 1- 59 months Mortality to Mother's literacy rate in 281 districts between 2000- 2002 according to data on the
Vital Horoscopes in the Health Houses and DHS Surveys
The Literacy Rate
1-5
9 m
on
ths m
orta
lity rate
Inequity IndexVagstaf:2005

Center for Health Network Expansion & Health Promotion
the distribution of percentages of 9 causes of deaths in men by age groups after correcting the garbage codes ,according to
mortality registration among 18 provinces in 2002
CANCERS
CARDIOVASCULAR.D
RESPIRATORY.D
UNINTENTIONAL.ACC
VIOLANC
SUICIDE
OTHERS
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
سن
صددر
OTHERS
SUICIDE
VIOLANC
UNINTENTIONAL.ACC
PERNETAL .D
RESPIRATORY.D
CARDIOVASCULAR.D
CANCERS
INFECTION .D

Center for Health Network Expansion & Health Promotion
The distribution of 9 causes of years life lost in women by separation of age groups after correcting the garbage codes in death registry program between
18 provinces in 2002
CANCERS
CARDIOVASCULAR.D
UNINTENTIONAL.ACC
SUICIDE
OTHERS
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
age
pe
rce
nta
ge
OTHERS
SUICIDE
VIOLANC
UNINTENTIONAL.ACCPERNETAL .D
RESPIRATORY.DCARDIOVASCULAR.DCANCERS
INFECTION .D

Center for Health Network Expansion & Health Promotion
كم تولدنوزادان وقوع بر موثر عوامل از هريك سهمدر - وزن كم نوزاد تولد شيوع تعيين مطالعه 11وزن
مهر -- كشور 1382اقليم
4.9%
1.7%
0.7%
0.5%
47.9%28.0%
21.4%
-1.2%
-1.8%
-2.3%
-3% 7% 17% 27% 37% 47%
ر نوا رفاهي خا وضعيت
وستا سكونت در شهر يا ر
در بيسوادي ما
در آن سكونت دارد اقليمي كه
يراني يا افغاني بودن ا
وقلويي د
د سن مادر در در هنگام تولدنوزا
اد جنس نوز
ري طول باردا
ولد وبت ت ن
The proportional effect of different health determinants on underweight neonates delivery-
The Survey done for prevalence of Underweight neonate deliveries in 11 different regions- Autumn 2003
Birth order
Duration of pregnancy
Sex of neonate
Mother's age
Twin birth
Iranian or Afghani
The area of living
Mother's literacy
Living in Urban or Rural area
Household income

Center for Health Network Expansion & Health Promotion
0.2
5.5
.75
1
Cum
ula
tive p
erc
ent of death
due to s
avaneh
0 .25 .5 .75 1Cumulative percent of dead people ranked by economic status
خطر معنادار تمركزجامعه مرفه غير دربخش
Obs Prob>z (95%) CI5498 0. 0.0281 [-0.1281 -0.0072]
قبال در عمدي غير حوادث از ناشي مرگ توزيعمرگ – ثبت برنامه مشترك كار خانوار رفاه سطح
سال در برابري نا ومطالعه علت 1382برحسب
Distribution of deaths due to Non-Intentional accidents in relation to household income-
The cooperative work of death registration system and inequity survey- 2003
Meaningful concentration for the high income households

Center for Health Network Expansion & Health Promotion
از ناشي مرگ رفاه خودكشيتوزيع سطح قبال درعلت –خانوار برحسب مرگ ثبت برنامه مشترك كار
سال در برابري نا 1382 ومطالعه
0.2
5.5
.75
1
Cum
ula
tive p
erc
ent of death
due to s
uic
ide
0 .25 .5 .75 1Cumulative percent of dead people ranked by economic status
خطر معنادار تمركزجامعه مرفه غير دربخش
Obs Prob>z )95%( CI5498 0.002 [-0.2072 -0.0469]
Meaningful concentration for the low income households
Distribution of deaths due to suicide in relation to household income-
The cooperative work of death registration system and inequity survey- 2003

Center for Health Network Expansion & Health Promotion
0.2
5.5
.75
1
Cum
ula
tive p
erc
ent of death
due to c
ancer
0 .25 .5 .75 1Cumulative percent of dead people ranked by economic status
خطر معنادار تمركزجامعه مرفه دربخش
Obs Prob>z )95%( CI5498 0.0007 [0.037 0.137]
رفاه سطح قبال در طانها سر از ناشي مرگ توزيععلت – برحسب مرگ ثبت برنامه مشترك كار خانوار
سال در برابري نا 1382ومطالعه
Distribution of deaths due to malignancies in relation to household income-
The cooperative work of death registration system and inequity survey- 2003
Meaningful concentration for the high income households

Center for Health Network Expansion & Health Promotion
سرپايي خدمات از مندي بهره توزيعمطالعه – خانوار رفاه سطح قبال در
اسفند مندي 1381بهره
0.2
5.5
.75
1
Cum
ula
tive p
erc
ent of seekin
g_outp
atient_
care
0 .25 .5 .75 1Cumulative percent of people ranked by economic status
N=26750 CCI = .062248 P=0.0000 CI-CCI [0.0464 0.0781]
مندي بهره معنادار تمركزجامعه مرفه دربخش
Meaningful concentration for the high income households
Distribution of utilization from health services in relation to household income-
Utilization survey- 2002

Center for Health Network Expansion & Health Promotion
0.2
5.5
.75
1C
um
ula
tive p
erc
ent of choic
e
0 .25 .5 .75 1Cumulative percent of people ranked by economic status
N=2413 CCI = 0.015196 P=0.0000 CI-CCI [0.0095 0.0209]
توزيع بهره مندي از حق انتخاب به مراجعه سرپايي در قبال سطح رفاه خانوار كنندگان
1381– مطالعه بهره مندي اسفند
انتخاب حق معنادار تمركزجامعه مرفه دربخش
Distribution of utilization for choosing health services provider for ambulatory care in relation to household income-
Utilization survey- 2002
Meaningful concentration for the high income households

Center for Health Network Expansion & Health Promotion
0.2
5.5
.75
1
Cum
ula
tive p
erc
ent of choic
e
0 .25 .5 .75 1Cumulative percent of people ranked by economic status
به انتخاب حق از مندي بهره توزيعكنندگان سطح مراجعه قبال در بستري
اسفند – مندي بهره مطالعه خانوار رفاه1381
N=690 CCI = 0.028351 P=0.0005 CI-CCI [0.0123 0.0444]
انتخاب حق معنادار تمركزجامعه مرفه دربخش
Meaningful concentration for the high income households
Distribution of utilization for choosing health services provider for hospitalization in relation to household income-
Utilization survey- 2002

Center for Health Network Expansion & Health Promotion
خدمات دريافت براي شده انجام هزينه ميانگينهر توسط سال طول در سرپايي درماني بهداشتياز -- مندي بهره مطالعه هزينه نوع تفكيك به فرد
اسفند -- درماني بهداشتي 1381خدمات
2412 3319
65747335
1991
6635
7254
3097
3478
6607
909927426
1564
942
0
5000
10000
15000
20000
25000
30000
صي خشخصو ب تي خشدول ب صي خشدولتيوخصو ب
نوما
ت
هزينهدارو ل ووساي
هزينهاقدامات درماني
هزينهاقدامات شخيصي ت
/ هزينهويزيت / دريافتمستقيم نشيز فرا
رفتوآمد هزينه
تومان20280
تومان6680
تومان26510
Average expenses for receiving ambulatory health services in a year for a person for different type of expenditure
Utilization survey- 2002
Drug and instruments
Curative interventions
Drug and instruments
Direct payments and user fees
Diagnostic tests
Going to the service unit and coming
backPrivate sector Governmental sector Both sectors
Exp
en
ditu
res

Center for Health Network Expansion & Health Promotion
Providers
Service
Ambulatory care
Governmental
Private
Rates of services
34%31% 82%
3524,000 Billion
Tomans
8.4 times of visit per year
for every Iranian
0.061 times of hospitalization
for every Iranian
18% 66%69%
Hospitalization
Revenue from
health Market
ارائه در وخصوصي دولتي بخش سهم درصد نسبت مقايسهمستقيم وبطور دولتي منابع از پول دريافت وسهم خدماتبهرهمندي – مطالعه ايران سالمت بازار در مردم جيب از
اسفند -- درماني بهداشتي خدمات 1381از
The comparison of the ratio of the governmental and private sector in delivering services and revenue from governmental financing and
out of pocket payments by the people in the health marketUtilization survey- 2002

Center for Health Network Expansion & Health Promotion
؛ ماهيانه درآمد بر باربستري يك هزينه پرداخت تاثيريا فرد شدن مقروض و دارايها فروش ؛ انداز پس
مطالعه - بيمارستان نوع تفكيك به خانوادهاسفند -- درماني بهداشتي خدمات از 1381بهرهمندي
5
55
23
3425
22
19
33
37
3026
8
15
13
16
35
12
21
12
21
6 3812 8
0%
20%
40%
60%
80%
100%
خصوصي ميناجتماعي ا ت بهداشتودرمان ه ب وابسته ) سازمانها ساير يا ساير)خيريه بيمارستاني هر
صددر
ناچيز يردرحدهيچيا تاث مصرفبيشاز 50%درآمدماهيانه ز دا آمدماهيانهومجبوربهمصرفپسان در ام مصرفتم ن بهقرضكرد ندازومجبور مامپسا مصرفتها ي روشدارا بهف قرضكردنمجبور عالوهبر
The effect of payments for one time of hospitalization on family wealth, savings, selling family resources and borrowing money for
the service payments Utilization survey- 2002
Every kind of hospitalOther (Charities and other organizations)
Ministry of healthSocial Security OrganizationPrivate
Paying more than 50% of monthly income
Paying more than all of monthly income and loan for it
Paying more which does not affect in the family
Paying more all monthly income and using the savings
Loan and selling properties for payment
Percent

Center for Health Network Expansion & Health Promotion
نسبتي از
DALYsكهريك ه
از گروهها
كوچك يبيماري وآسيب دو درهربه جنس
خود اختصا
مي صبر ؛ دهند
پايه اطالعات
سال 1381
17
9
6
5
4
4
4
4
3
3
3
2
2
2
2
2
2
2
2
1
1
1
1
1
1
0 2 4 6 8 10 12 14 16 18
Traffic injuries
Ischemic Heart Diseases
Depressive disorders
Osteoarthritis
Diabetes mellitus
Cerebrovascular events
Falls
LBW&prematurity
Substance abuse
Other unintentional injuries
Infertility
Psychotic disorders
Rheumatoid arthritis
Asthma
Burns
Cataract
Self-inflicted intentional injuries
Epilepsy
Bipolar disorders
COPD
Leukemia
Iodine deficiency
Stomach cancer
Congenital heart diseases
Hypertention
DALYs for each
of the smaller disease
groups in 2 sexes – According to data
have been
gathered in 2002

Center for Health Network Expansion & Health Promotion
The General Context Goals of the Health System
Health –technical efficiency of medical care in production of health Equity - (includes also efficiency considerations) Cost containment - technical efficiency of medical care in production of health
(and allocative efficiency in consumption of care) Micro-economic efficiency – technical efficiency in the production of quality care Client satisfaction, mainly through accountability
Systemic Functions --subject to devolution and decentralization: Policymaking Financing Organization and Management of Care Consumptions Provision of Care Training and medical education Research and development

Center for Health Network Expansion & Health Promotion
Experience 1 -Current situation of PHC System
Analysis Iranian Governmental PHC Record and Legacy through a Relative Centralized system

Center for Health Network Expansion & Health Promotion
Experience 1 -Current situation in disease prevention area ; Iranian Governmental PHC Record and Legacy
through a Relative Centralized System
Health Eradication of communicable diseases ‘Epidemiological transition’ to non-communicable diseases that
eventually led to superior health outcomes
Equity Relatively wide access to care
Efficiency In spite of low levels of spending, efficient especially when quality of
care is considered
Client satisfaction Relatively high

Center for Health Network Expansion & Health Promotion
Comparative Decision Space: Current Ranges of Choice for Iran in Primary care
Functions Range of Choice
Narrow Moderate Wide
Sources of Revenue *
Expenditures*
Income from Fees*
Service Organization*
Required Programs & Norms *
Hospital Autonomy - -
Insurance Plans*
Payment Mechanisms*
Functions Range of Choice
Narrow Moderate Wide
Salaries*
Contracts*
Civil Service-
Access Rules*
Governance*
Local Government*
Facility Boards*
Health Offices*
Community Participation*
Total Decision Space:

Center for Health Network Expansion & Health Promotion
Causes of Ineffective Government Functions in Preventive health programs
Not setting and maintaining the right priorities over time at local areas
Ineffective distribution in targeting of resources and lack of local resources
Not promoting innovation A lack of responsiveness to the new needs

Center for Health Network Expansion & Health Promotion
Experience 2Construction Board of trustees in
universities
A relative successful experience

Center for Health Network Expansion & Health Promotion
Comparative Decision Space
Functions Range of Choice
Narrow Moderate Wide
Sources of Revenue *
Expenditures*
Income from Fees*
Service Organization*
Required Programs & Norms *
Hospital Autonomy - -
Insurance Plans*
Payment Mechanisms*
Functions Range of Choice
Narrow Moderate Wide
Salaries*
Contracts*
Civil Service-
Access Rules*
Governance*
Local Government*
Facility Boards*
Health Offices*
Community Participation*
Total Decision Space:

Center for Health Network Expansion & Health Promotion
Experience 3Hospital autonomy
A recommended plan but failed because of design and
implementation method

Center for Health Network Expansion & Health Promotion
Comparative Decision Space
Functions Range of Choice
Narrow Moderate Wide
Financing*
Sources of Revenue *
Expenditures*
Income from Fees*
Service Organization*
Required Programs & Norms *
Insurance Plans
*Payment Mechanisms
*
Functions Range of Choice
Narrow Moderate Wide
Salaries*
Contracts*
Access Rules*
Governance*
Local Government*
Facility Boards*
Health Offices*
Community Participation
*Total Decision Space:

Center for Health Network Expansion & Health Promotion
Causes of Ineffective Government Functions in Hospital autonomy
Not thinking about all aspects of decentralization especially in terms of; Utilization of people from different welfare status (Insurance coverage) Training Lack of allocating resource for medical education
Not think about evaluation and monitoring methodology Lack of advocacy in different areas

Center for Health Network Expansion & Health Promotion
Consequences
Decrease equity Increase catastrophic payments Client dissatisfaction Loosing political support Making the plan insufficient

Center for Health Network Expansion & Health Promotion
Social/Cultural Environment
Technological Environment
Futures Scenario
Development
Stakeholder Analysis
Political
Social/Cultural
Demography
Political/Regulatory
Environment
Economic Environment
Health Care
Environment
Response to External Change
Client Orientation
Innovation
Quality
Teamwork
LeadershipVision
/Mission
OrganizationalSubsystem
Resources
Competencies
Capabilities
Value-chainAnalysis
Organizational Objectives
Development
Critical Success Factor Identification
Vision Formulation
Mission Formulation
MeasurementEvaluation
Response
Objectives
Work with Steering
Team to Develop Program Strategies
Hospital Autonomy
)Unsuccessful Program(
Non consideredUncertain Considered

Center for Health Network Expansion & Health Promotion
Experience 4Article 192
An obligatory rule in third national development law for privatization
The Pilot project was conducted in a few areas for only new expansions of health facilities

Center for Health Network Expansion & Health Promotion
Comparative Decision Space
Functions Range of Choice
Narrow Moderate Wide
Sources of Revenue *
Expenditures*
Income from Fees*
Service Organization*
Required Programs & Norms *
Insurance Plans*
Payment Mechanisms*
Functions Range of Choice
Narrow Moderate Wide
Salaries*
Contracts*
Access Rules*
Governance*
Local Government*
Facility Boards*
Health Offices*
Community Participation*
Total Decision Space:

Center for Health Network Expansion & Health Promotion
Experience 5Article 49
A new program for increasing authorities of peripheral management
areas in resource allocation

Center for Health Network Expansion & Health Promotion
It is a new one-year designed plan according to the new tasks for resource managers based on changing the tasks of accountants
Needs conferring authorities to local managers

Center for Health Network Expansion & Health Promotion
Lessons to be learnt Decentralization is like the story of elephant and blind men
Needs a holistic approach It is a scientific planning
Needs methodology All the stakeholders should be engaged in the planning
Bringing stakeholders together to define priorities for projects and programmes increases interest and sense of ownership, which in turn promotes sustainability.
Supporting open dialogue and participation between the local government and civil society can ensure improved self-reliance.
Not all government functions should be entirely decentralised. Decision area is the most important consideration We should consider the risks of political pressures and unilateral
considerations It shouldn't make weakening stewardship ,policy making and leadership of
the headquarter of MOH Some unpredictable events needs centralized financing Decentralization is not the goal we should avoid undesirable
decentralization without health impacts

Center for Health Network Expansion & Health Promotion
Lessons to be learnt- Cont’d
The authorities should be transferred to the most eligible level of system
A centralized and stratified HIS is needed for monitoring and evaluation of the projects
Strategy of change in sequence of time should be clear to policymakers, program planners and local authorities
Resistance of those authorities to relinquish should be thought The plan for ‘denationalization’ should be a real one for all the
experts Technical assistance is needed for local governments More capacity development is needed at all levels of
governance.
Center for Health Network Expansion & Health Promotion
Lessons to be learnt - Cont’d – Risks
Consider Growing regional inequalities Undermining universal access to care Not having mechanisms for system stabilization and long term reform
through innovation Growing inefficiencies due to weak mechanisms to deal with
externalities Not re-defining the roles of different levels of government and
institutions Provide financial and regulatory measures for a federal system

Center for Health Network Expansion & Health Promotion
Priority setting according to
BOD & Burden of Risk Factors
CEA and Choosing the most
appropriate strategies
Policy making tools:
Conduct resources and
plan
Efficient Performance
Modeling Tactical DecisionsBurden of disease- Cost-effectiveness analysis-
Health performance

Center for Health Network Expansion & Health Promotion
CustomerHealth Unit
•BURDEN OF DISEASE•COST•QUALITY•EQUITY•TIME•FLEXIBILITY• MARKET ANALYSIS
Tact
ical
Deci
sions
Policies and
strategies
resultsresults
ProcessOf Design Service Package
Poli
cym
akin
g
Design
standards for
IntegrationStratificati
onEvaluationCoverage
Tech
nic
al
Deci
sion
s
Policy making, Program planningAnd delivering services
Service Packages

Center for Health Network Expansion & Health Promotion
Thank you for your
attention