-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
1/16
In vivo dosimetry in brachytherapyKari Tanderup , Sam Beddar ,
Claus E. Andersen , Gustavo Kertzscher , and Joanna E. Cygler
Citation: Medical Physics 40 , 070902 (2013); doi:
10.1118/1.4810943 View online: http://dx.doi.org/10.1118/1.4810943
View Table of Contents:
http://scitation.aip.org/content/aapm/journal/medphys/40/7?ver=pdfcov
Published by the American Association of Physicists in Medicine
http://scitation.aip.org/search?value1=Kari+Tanderup&option1=authorhttp://scitation.aip.org/search?value1=Sam+Beddar&option1=authorhttp://scitation.aip.org/search?value1=Claus+E.+Andersen&option1=authorhttp://scitation.aip.org/search?value1=Gustavo+Kertzscher&option1=authorhttp://scitation.aip.org/search?value1=Joanna+E.+Cygler&option1=authorhttp://scitation.aip.org/content/aapm/journal/medphys?ver=pdfcovhttp://dx.doi.org/10.1118/1.4810943http://scitation.aip.org/content/aapm/journal/medphys/40/7?ver=pdfcovhttp://scitation.aip.org/content/aapm?ver=pdfcovhttp://scitation.aip.org/content/aapm?ver=pdfcovhttp://scitation.aip.org/content/aapm/journal/medphys/40/7?ver=pdfcovhttp://dx.doi.org/10.1118/1.4810943http://scitation.aip.org/content/aapm/journal/medphys?ver=pdfcovhttp://scitation.aip.org/search?value1=Joanna+E.+Cygler&option1=authorhttp://scitation.aip.org/search?value1=Gustavo+Kertzscher&option1=authorhttp://scitation.aip.org/search?value1=Claus+E.+Andersen&option1=authorhttp://scitation.aip.org/search?value1=Sam+Beddar&option1=authorhttp://scitation.aip.org/search?value1=Kari+Tanderup&option1=authorhttp://oasc12039.247realmedia.com/RealMedia/ads/click_lx.ads/test.int.aip.org/adtest/L23/1354965365/x01/AIP/ScandiDos_MPHCovAd_1640x440Banner_02_05_2014/Scandidos201640x440.jpg/7744715775314c5835346b4141412b4b?xhttp://scitation.aip.org/content/aapm/journal/medphys?ver=pdfcov
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
2/16
In vivo dosimetry in brachytherapyKari Tanderup a) Department of
Oncology, Aarhus University Hospital, Aarhus 8000, Denmark and
Department of Clinical Medicine, Aarhus University, Aarhus 8000,
Denmark
Sam Beddar Department of Radiation Oncology, The University of
Texas MD Anderson Cancer Center, Houston,Texas 77030
Claus E. Andersen and Gustavo KertzscherCenter of Nuclear
Technologies, Technical University of Denmark, Roskilde 4000,
Denmark
Joanna E. Cygler Department of Physics, The Ottawa Hospital
Cancer Centre, Ottawa, Ontario K1H 8L6, Canada
(Received 15 January 2013; revised 12 April 2013; accepted for
publication 16 April 2013;published 25 June 2013)
In vivo dosimetry (IVD) has been used in brachytherapy (BT) for
decades with a number of differentdetectors and measurement
technologies. However, IVD in BT has been subject to certain
difcultiesand complexities, in particular due to challenges of the
high-gradient BT dose distribution and thelarge range of dose and
dose rate. Due to these challenges, the sensitivity and specicity
toward errordetection has been limited, and IVD has mainly been
restricted to detection of gross errors. Giventhese factors,
routine use of IVD is currently limited in many departments.
Although the impact of
potential errors may be detrimental since treatments are
typically administered in large fractions andwith
high-gradient-dose-distributions, BT is usually delivered without
independent verication of thetreatment delivery. This Vision 20/20
paper encourages improvements within BT safety by devel-opments of
IVD into an effective method of independent treatment verication.
2013 American Association of Physicists in Medicine .
[http://dx.doi.org/10.1118/1.4810943 ]
Key words: in vivo dosimetry, brachytherapy, treatment errors,
quality assurance
I. INTRODUCTION
In vivo dosimetry (IVD) has been used in brachytherapy(BT) for
decades and has been referred to in InternationalCommission on
Radiation Units and Measurements (ICRU)recommendations. 1 The
initial motivation for performingIVD in BT was mainly to assess
doses to organs at risk (OAR)by direct measurements, because
precise evaluation of OARdoses was difcult without 3D dose
treatment planning. Withthe introduction of 3D image-guided BT, it
is now possible tocalculate 3D tumor and OAR doses as well as dose
volumehistogram (DVH) parameters by the treatment planning sys-tem
(TPS). 24 Recording and reporting of dose based on 3Dimages is an
important step forward. Current 3D image-baseddose calculations are
often more accurate for assessments of OAR doses than IVD
measurements. However, there are sit-uations with signicant dose
calculation uncertainties, in par-
ticular for low-energy photon-emitting sources and in
hetero-geneous media, where IVD may contribute to more precisedose
reporting. 5 Furthermore, potential organ movement inbetween
imaging and treatment contributes to uncertainties indelivered
dose, and IVD may have a potential role for identi-cation of organ
or applicator movements.
The complexity of BT has increased with the introductionof
remote afterloading and 3D image-based dose planning.However,
independent and patient specic quality assurance(QA) of dose
delivery is not performed systematically, despitethe risk of errors
during the many manual steps involved in
treatment planning and delivery. Furthermore, BT is
typicallyadministered with large doses per fraction ( > 5 Gy),
whichmeans that the consequence of a fractional error may be
sub-stantial when compared to typical external-beam radiother-apy
(EBRT) with delivery of smaller doses per fraction (e.g.,2 Gy).
From this perspective, IVD is very relevant in BT asan independent
method for detection of deviations or errors. 6
Unfortunately, the interest has suffered much from difcul-ties
and uncertainties of dose measurement, in particular thechallenges
of precise detector positioning in the high dosegradient elds.
Error detection sensitivity and specicity of current systems has
been compromised by such uncertainties,and therefore it seems that
current IVD is only able to detectgross errors (Sec. IV.C ), which
happen less frequently. Fur-thermore, there has been a lack of good
infrastructure in termsof commercially available dosimetry systems
with straightfor-ward procedures, which do not require extensive
manpower
and expertise. Substantial progress is needed in dose
measure-ment methodology and infrastructure in order to bring IVD
toits full potential.
Whereas IVD in BT needs further development to becomewell
integrated into routine clinical practice, the situation
isdifferent in EBRT where IVD is more widely used and ac-cepted as
an independent check of dose delivery. 7, 8 Confor-mal EBRT is
characterized by at dose proles and homoge-neous dose in the target
region. Therefore, conformal EBRTIVD for target dose verication has
not suffered from the par-ticular challenge typical for BT, which
is detector positioning
070902-1 Med. Phys. 40 (7), July 2013 2013 Am. Assoc. Phys. Med.
070902-10094-2405/2013/40(7)/070902/15/$30.00
http://dx.doi.org/10.1118/1.4810943http://dx.doi.org/10.1118/1.4810943http://dx.doi.org/10.1118/1.4810943http://dx.doi.org/10.1118/1.4810943http://crossmark.crossref.org/dialog/?doi=10.1118/1.4810943&domain=pdf&date_stamp=2013-06-25http://dx.doi.org/10.1118/1.4810943http://dx.doi.org/10.1118/1.4810943
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
3/16
070902-2 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-2
in high gradient elds. However, due to the heterogeneous u-ence
proles and dose gradients, 9 IVD in IMRT and VMATfor dose
assessments in OARs, for instance, would involvesome of the same
challenges as are seen with BT. The energydependence of detectors
is often more crucial in BT as com-pared to EBRT because of the
lower photon energy appliedin BT. However, most small detectors
that are used for IVDin EBRT, 7 are in principle also suitable in
BT. TransmissionIVD based on, e.g., EPID has much potential for
EBRT, 10 buthas not yet been much exploited for BT. In the
accompanyingVision 20/20 paper, 11 the current and future
justications of performing external beam IVD are discussed, and a
compre-hensive review of detectors used for IVD is provided.
The purpose of the current Vision 20/20 paper is to
discusscurrent and future justications of IVD for BT, and to
iden-tify current challenges that need to be addressed in order
toadvance the eld over the next decade.
II. JUSTIFICATION FOR IN VIVO DOSIMETRY
II.A. Errors and treatment variations in brachytherapy
There is currently no systematic overview of the type
andfrequency of errors which occur in BT. Existing reports of
BTaccidents and errors are mainly based on retrospective
eventcollection since prospectively structured investigations
havenot yet been performed on a multicenter scale.
Furthermore,since current IVD systems suffer from unknown or poor
sen-sitivity and/or specicity (see below), there are an
unknownnumber of BT errors that remain undetected.
The International Commission on Radiological Protection(ICRP)
Report Nos. 86 (Ref. 12) and 97 (Ref. 13) as well asIAEA safety
report series 17 (Ref. 14) describe errors thathave occurred in BT.
BT errors and accidents are mainly
related to human errors, although some errors are causedby
mechanical events related to malfunction of the equip-ment.
Examples of human errors are incorrect medical indi-cation, source
strength, patient identication, diagnosis or siteof treatment,
prescription, data entry, catheter, or applicator.High dose-rate
(HDR) and pulsed dose-rate (PDR) afterload-ing techniques may
introduce source positioning errors whichare related to procedures
specic for afterloading dose plan-ning and treatment delivery.
Source positioning errors mayalso occur in low dose-rate (LDR)
manual loading proceduresdue to manual misplacement or source
migration after theplacement.
Afterloading BT embraces a variety of approaches to treat-
ment planning, each involving specic error scenarios. Treat-ment
planning can be performed without the use of a TPSby directly
dening the target from x-ray image or clinicalndings and applying a
standardized or manually optimizedtreatment plan. An example would
be an esophagus treat-ment where the treatment length, source
offset, step size, anddwell times may be directly dened on site in
some clinicsand followed by a more or less manual entry of
treatment pa-rameters into the afterloader control software. For
this sce-nario, the risk of errors is mainly related to the
denition andmanual entry of parameters. A number of manual steps
are
avoided with 3D image-based treatment planning. However,other
sources of potential errors are introduced in this pro-cedure. With
3D image-based dose planning, both target andsource catheters are
dened with imaging modalities such asultrasound (US), magnetic
resonance imaging (MRI), or com-puted tomography (CT). Mistakes or
uncertainties in identi-cation of source catheters or denition of
applicator lengthcan lead to source positioning errors. Dose
optimization mayinvolve a high degree of dwell time modulation,
which meansthat the consequence of source positioning errors can
lead tosignicant errors throughout the volumetric dose
distribution.The treatment plan is usually directly exported from
the treat-ment planning system to the treatment control station
(TCS)and the afterloader. The automatic transfer reduces the risk
of incorrectly entered parameters, although there is still a risk
that a wrong plan is exported or imported. After treatmentplan
transfer, the afterloader is connected to the applicators;this
process involves a risk of misconnection of the sourcetransfer
guide tubes.
Organ or applicator movement in between imaging andtreatment
represents a limitation on the accuracy of dose de-livery unless
imaging is performed immediately before deliv-ery in a BT suite.
For prostate BT, there have been reportsof needle movements, 15, 16
and for gynecological BT, organmovement has been seen as well as
occasional relocation of the applicator. 17 IVD may be a tool for
detection of such dis-placements and movements. However, direct
inspection of theapplicator (e.g., measurement of free needle
length in prostateBT) or reimaging directly before treatment
delivery may be analternative way to validate that the dose
delivery and doserecording are appropriate. 18 Neither the use of
repeated imag-ing nor IVD has demonstrated wide practical
application fordetection of organ and applicator movement. The
conditionsunder which each of these may be practical and/or
precise
enough for use in clinical practice still remain to be
claried.Certain errors can be identied by the afterloader
safetysystems which include builtin dummy check sources, a
radi-ation detector, and source cable length control. 19
However,afterloader safety systems are only able to detect a subset
of all possible errors that may occur. Additional manual
safetychecks of the treatment planning and delivery procedure maybe
introduced such as verication of applicator reconstruc-tion or
source guide tube connection by a second observer.In addition, as
documented in ICRP and IAEA reports, 1214
there are a number of errors that are not detected by
safetysystems or manual checks. IVD has the potential to
comple-ment other QA and quality control (QC) procedures, as
part
of the greater process of quality management, by providingan
independent overall verication of the treatment delivery(Table
I).
II.B. Recording of dose in individual patients
The increasing use of image-guided BT has been a hugestep
forward for the calculation and recording of tumor andOAR doses. In
most cases, dose calculation is more accuratethan IVD, mainly due
to the challenge of precise detector po-sitioning to measure the
specic OAR or tumor doses (see,
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
4/16
070902-3 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-3
TABLE I. QA and detection of errors and variations occurring
with afterloading BT.
Quality item Typical quality test Role of in vivo dosimetry
Source calibration Independent source calibration in the
department Minor importance, but may in certain situationsreveal
calibration errors (if the in vivo dosimetercalibration is
independent from the actualsource).
Afterloader source positioning and dwell time(nonpatient
specic)
Autoradiography, commissioning of applicators,other source
stepping and dwell time QA
Minor importance, but may in certain situationsreveal errors
which have not been identied with
standard nonpatient specic QA.Afterloader malfunc tion
Unpredictable afterloader malfunction is
difcult to target with general QA.Major relevance, since
afterloader malfunctionmay have signicant impact on dose, and
IVDhas good potential to reveal such errors.
Patient identication Manual check Not relevantCorrect treatment
plan Manual check Relevant since it may detect if a wrong plan
is
used for treatment, if DICOM transports to theafterloader and
dosimeter software areindependent.
Intra- and interfraction organ/applicatormovement
Reimaging performed just before treatmentdelivery can in some
cases be used to assessorgan or tumor dose in image-guided BT.
The relevance depends on detector positioning.If the detector is
xed to the applicator, it willnot reveal applicator movement,
contrary tomeasurements in, e.g., urethra. For the organdose change
detection, there are signicant
challenges to position the detector precisely(reimaging may be
preferred).
Applicator reconstruction and fusion errors Manual check
Relevant. Can detect applicator reconstructionerrors when the
dosimeter is placed in anoptimal geometry.
Applicator length/source-indexer length Manual check Major
relevance, since source-indexer lengtherrors may have signicant
impact on dose, andreal time IVD has good potential to reveal
sucherrors.
Source step size (patient specic) Manual check Major relevance
if source step size is enteredmanually. Otherwise the appropriate
method tocheck source stepping is part of nonpatientspecic QA.
Interchanged guide tubes Manual check Major relevance, since
interchanged guide tubes
may have signicant impact on dose, and IVDhas good potential to
reveal such errors.
Recording of dose General QA related to dose calculation in
theTPS
Relevant when dose recording is not calculatedwith sufcient
accuracy by 3D image based TPScalculation (e.g., lack of
inhomogeneity orradiation scatter corrections).
e.g., Sec. IV.C ). However, for certain clinical situations
TPSbased dose calculations are currently associated with
system-atic deviations due to lack of corrections for
heterogeneitiesand scatter conditions. 20 This is particularly true
for low en-
ergy sources such as 125
I or 103
Pd used in permanent implantsof prostate, lung, and recently
breast. 2123
Some dosimetry systems dene specic points or volumesfor dose
reporting for individual patients such as the ParisSystem for
interstitial implants; 24 ICRU 38, 1 GEC EuropeanSociety for
Radiotherapy and Oncology (ESTRO), 2 and ABSfor cervix BT; 25, 26
as well as ABS (Ref. 27) and GEC ESTRO(Refs. 28 and 29) for
prostate implants. This kind of report-ing is important in
treatment outcome assessments. However,the reporting is mostly
based on treatment planning identi-cation of such points/volumes.
In the situation where the
tumor and OARs move and/or get deformed, as is the caseduring
permanent prostate implants, IVD can provide ad-ditional
information about the dose delivered to the tumorand/or OAR for the
given patient. In particular, for LDR and
PDR treatments that involve long irradiation times, there maybe
anatomical changes such as prostate swelling, applicatormovement,
and organ movement, and IVD may be used tomonitor the treatment
progression. There have been studiesof the point or segment dose
measurements in rectum or ure-thra for gynecological 30, 31 or
prostate implants 3234 or in thetumor. 35, 36 Some results conrm
the agreement between thecalculated and delivered doses, while
others point to discrep-ancies between them. The reasons for these
disagreementsare not always clear and underscore the technical
difcultiesfaced by IVD in BT.
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
5/16
070902-4 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-4
III. CURRENT CLINICAL PRACTICE
Typical sites for IVD are rectum, 3740 and bladder orurethra.
32, 33, 41 Noninvasive detector positioning far from thesource,
e.g., on the skin, make the measurements insensitiveto error
detection because of low signal and difculties toknow precisely the
relation between the source(s) and detec-tor(s). IVD on skin is of
relevance during the treatment of breast cancer 4244 since the skin
is an OAR close to the treated
volume and has signicant dose calculation uncertainties.45
The practice of using IVD varies considerably amongcountries. In
most countries, systematic use of IVD is not of-ten incorporated as
a standard QA or QC procedure. How-ever, there is specic
legislation in a number of countriesmaking IVD obligatory. For
example, France recently intro-duced a law that requires some form
of IVD be performed onall EBRT patients. 46 Unfortunately, there
are no reports avail-able about the value and benet of routine BT
IVD in thesecountries. In patterns-of-care studies from Europe and
LatinAmerica, it has been difcult to collect responses that
homo-geneously represent all countries. 47, 48 However, it seems
thatIVD is available in many institutions because it is
reported
to be used by 20%33% of the centers. 4749 However, it isnot
further described how often, in which disease sites, or inhow many
patients. A recent survey by Sawakuchi et al. 103
on Canadian cancer clinics showed that most of the
clinicsperform some form of IVD for special EBRT
techniques.However, no IVD is performed routinely for BT
treatmentsin Canada. A Japanese patterns-of-care study of cervix
can-cer reports that rectal and bladder IVD was used in 27% and3%
of the BT patients, respectively. 50 IVD was carried out in1.2%
U.S. centers that performed vaginal BT in endometrialcancer
patients. 51 From available literature and institutionalreports, it
seems that IVD most often appears as diode rectaldosimetry
performed during intracavitary BT in gynecolog-ical cancer. There
are a number of groups reporting institu-tional use of IVD in
prostate cancer, but there are no generalreviews or reports that
indicate this technique is commonlyused, or what was the observed
error rate.
IV. CHALLENGES SPECIFIC TO IN VIVO DOSIMETRY IN
BRACHYTHERAPY
IV.A. High dose gradients and detector positioning
The BT dose distributions are characterized by steep
dosegradients that depend strongly on the distance from the
detec-
tor to the source. At a distance of 4 mm from a linear
source,the dose gradient is approximately 50%/mm. The gradient
de-creases to around 6%/mm and 5%/mm at distances of 20 and35 mm,
respectively. Therefore, even small uncertainties indetector
positioning may lead to signicant uncertainties indose
measurements. The ability of IVD to detect errors de-pends
critically on where the detectors can be placed and howwell these
detector positions are known. The optimal regionfor detector
placement balances the favorable signal-to-noiseratio (SNR) with
the smallest possible impact of positionaluncertainties. 35, 36
This optimal region is different and specic
for each detector and patient category due to differences
inpositional uncertainties of the detector as well as
sensitivity,energy dependence, and angular dependence of the
detectorresponse.
The steep dose gradient induces additional challengeswhen IVD is
used for individual measurement of organ dose.The dosimeter needs
to be positioned in a clinically relevantregion, and for the
bladder and rectum, it is a major difcultyto establish a stable
dosimeter position directly adjacent tothe most exposed part of the
organ wall. 52 The anatomy of the urethra is more favorable for
performing accurate IVD inprostate BT since this organ is smaller
and less deformable.Several challenges regarding optimal dosimeter
positioningcould be solved with dedicated clinical components,
e.g., ure-thral catheters and rectal or bladder balloons, that
would bothstabilize and offer accessibility at desired dosimetry
sites (seeSec. VI.A ).
Ease of positioning as well as good detector stability canbe
obtained by insertion of extra invasive catheters or
needles.However, the potential use of such invasive procedures
raisesethical issues because of accompanying risks for the
patientsuch as infection. The extra procedure must be of clear
ben-et to the patient and since IVD still has to demonstrate thatit
adds signicant improvement in terms of safety and qual-ity there is
currently reluctance among clinicians to introduceextra invasive
procedures.
IV.B. Energy dependence of detectors
Another major challenge for IVD in BT is the energy de-pendence
(relative absorber dose sensitivity) (Ref. 53) of ex-isting
detectors in the intermediate-to-the-low energy range of the photon
or gamma energy spectra that are commonly en-
countered (60
Co, 137
Cs down to 103
Pd) covering>
1 to 50%.In order to avoid false alarms, current error decision
cri-
teria are usually high, which means that the error
detectionsensitivity is low. Currently, at error criteria are
mainly usedin clinical practice. However, a at criterion of, e.g.,
10% mayresult in false alarms when the detector is close to the
source,where positional uncertainties of the detector lead to dose
un-certainties larger than 10%. 36 On the other hand, 10% maybe too
large for treatment error detection at larger source-detector
distances where the inuence of positional uncertain-ties is less.
36
V. DETECTORS: STATE OF THE ARTMany dose-measurement systems have
been used in BT
in spite of the practical challenges encountered or the
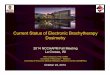
F IG . 1. Rectal IVD in PDR 192 Ir cervix cancer BT with tandem
ring applicator for BT fractions 1 (BT1) and 2 (BT2). Dashed lines
indicate bounds of the 95%prediction interval.
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
7/16
070902-6 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-6
TABLE II I. Characteristics of detectors and dosimetry systems
of importance for precise routine IVD in brachytherapy. The items
are rated according to:advantageous ( ++ ), good ( + ), and
inconvenient ( ).
TLD Diode MOSFET Alanine RL PSD
Size + + / + / ++ ++ ++Sensitivity + ++ + ++ + / ++Energy
dependence + + ++Angular dependence ++ + + ++ ++Dynamic range ++ ++
+ ++ ++
Calibrationprocedures, QA,stability, robustness,size of system,
easeof operation
+ ++ ++ / + + / ++
Commercialavailability
++ ++ ++ ++ +
Online dosimetry ++ + ++ ++Main advantages No cables, well
studied systemCommercialsystems atreasonable price,well studied
system
Small size,commercial systemat reasonable price
Limited energydependence, nocables
Small size, highsensitivity
Small size, noangular and energydependence,sensitivity
Main disadvantages Tedious proceduresfor calibration and
readout, not onlinedosimetry
Angular and energydependence
Limited life of detectors, energy
dependence
Not sensitive to lowdoses, tedious
procedures forcalibration andreadout, not
onlinedosimetry,expensive readoutequipment notavailable in
clinics
Needs frequentrecalibration, stem
effect, notcommerciallyavailable
Stem effect
shortcomings in their physical properties such as en-ergy
response, signal noise ratio, signal stability, read-out precision,
and positional accuracy. 54 In principle, de-tectors that are
commonly used for the EBRT absorbed
dose measurements may be good candidates for appli-cation for
IVD for BT. Few studies have been con-ducted in the past to compare
the performance of thesedetectors for both high dose BT and EBRT.
5860 Ther-moluminescent dosimeters (TLD), 32, 42, 6163
semiconductordiodes, 30, 64 metal-oxide-semiconductor eld-effect
transis-tors (MOSFET), 33, 34, 65 radioluminescence (RL) and
opticallystimulated luminescence (OSL) detectors, 66 plastic
scintil-lation detectors (PSD), 41, 6770 alanine detectors, 39, 71
radio-photoluminescent glass dosimeters (RPLGD) (Refs. 55, 56,and
72) have been used for IVD in BT to measure dosesover an assortment
of disease sites. The characteristics andthe operation of these
detectors are briey described below,
and have also been presented and discussed in the accompa-nying
Vision 20/20 paper for EBRT, 11 in review papers, 73 aswell as in
textbooks. 74, 75
There is no ideal detector for all BT measurements be-cause of
the severe requirements needed and demands ex-pected of the
dosimeters. All currently used detectors exhibitvarying degrees of
artifacts such as volume-averaging, self-attenuation, response
angular anisotropy, energy dependence,and a nonlinear dose
response. Therefore, BT detector se-lection is crucial and is
dictated by the radioactive source inquestion, the spatial
locations of the measurement points with
respect to the source, practical insertion(s) of the
detectors,and the disease site. Only detector designs that can be
easilyinserted within either intraluminal catheters or special
appli-cators inserted into patients should be considered. Table
III
presents an overview of characteristics of the most
relevantdetectors for IVD in BT and an evaluation of their
advantagesand disadvantages.
V.A. TLDs and RPLGDs
TLDs have been used for HDR 192Ir BT to measure thedose to the
urethra and/or rectum during prostate treatments(2428). TLDs come
in a variety of materials and forms andcan be shaped to easily t
into various areas of interest. Thelithium uoride (LiF) TLD rods
are the most widely usedform, because they can be easily inserted
into catheters. How-ever, they require special preparation
(annealing, individual
calibration, careful handling, fading correction, etc.) and
donot provide a direct reading right after the treatment.
Thecombination of these properties places them into a
secondarychoice compared to other dosimetry systems that are
capableof providing reading in real time.
RPLGDs have a similar reading process to TLDs, exceptultraviolet
light (and not heat) is used to stimulate the detec-tor.
Irradiation of the silver-activated phosphate glass convertssilver
ions to stable luminescent centers; when exposed to ul-traviolet
light, the luminescent centers produce uorescencein proportion to
the absorbed radiation dose. These detectors
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
8/16
070902-7 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-7
have been used for IVD (4244) by Nose et al. 55, 56 forHDR
interstitial BT for head-and-neck cancer (61 patients)and pelvic
malignancies (66 patients). In the case of the pelvicpatients, the
RPLGDs were sutured to the anterior wall of therectum or positioned
inside a Foley catheter inside the ure-thra. Deviations greater
than 20% were found between themeasured and calculated doses and
were attributed to the in-dependent movement of the organs and
applicators betweenthe planning and treatment delivery times.
V.B. Semiconductor diodes
Diodes are another type of semiconductor solid-statedosimeters,
typically based on silicon. They are mostly usedfor EBRT but have
been also employed for in vivo verica-tion of BT plans. They have
the advantage of providing userswith an immediate readout, high
sensitivity, good mechan-ical stability, fairly small size.
Unfortunately, they are alsoknown for the undesirable dosimetric
characteristics whichinclude directional dependence, energy
dependence, temper-ature dependence, and changes in sensitivity due
to radiationdamage. As these characteristics affect the accuracy of
thedosimetry system, they must be thoroughly characterized
inphantom before clinical use for the specic radiation sourceor
application. 57, 76
Waldhusl et al. 64 and Seymour et al. 57 both used exiblediode
array manufactured by PTW for IVD for patients un-dergoing HDR
192Ir treatments. Waldhusl et al. 64 evaluatedsuitability of rectal
probes consisting of ve diodes (separatedby 15 mm) and bladder
probes consisting of a single diode forIVD of cervix cancer
patients. Their measurements resulted indifferences between
calculated and measured doses rangingfrom 31% to + 90% (mean 11%)
for the rectum and from 27% to + 26% (mean 4%) for the bladder.
They also re-
ported that shifts in probe position of 2.5 mm for the
rectalprobe and 3.5 mm for the bladder probe caused dose
differ-ences exceeding 10%. Seymour et al. 57 performed a
dosimet-ric evaluation of the ve diode array in the routine
verica-tion of planned dose inside the rectum for prostate (HDR)
BTusing a real-time planning system. The deviations betweenthe
diode measurements and the TPS predicted values rangedfrom 42% to +
35% (with 71% of the measurements within10% of the predicted
values). Waldhusl et al. 64 and Sey-mour et al. 57 estimated that
the overall uncertainty involved inphantom dose measurement, after
correcting for all the factorsaffecting diode response were 7% (SD)
and 10% (SD),respectively.
V.C. MOSFET detectors
MOSFETs are miniature n- or p-type silicon (Si) semicon-ductors.
For dosimetry, mostly p-type detectors are used. Ingeneral, MOSFETs
as all semiconductors, exhibit tempera-ture dependence. However,
this effect has been overcome byspecially designed dual-MOSFET-dual
bias detectors 77 pro-duced by Best Medical Canada. These detectors
can be pro-duced either in standard size, or as micro-MOSFETs. The
lat-ter ones are particularly suitable for BT due to their
small
size (8 2.5 1.3 and 0.2 0.2 5 10 4 mm 3 for ex-ternal and
sensitive volume dimensions, respectively). Theyare also available
in the form of an array of ve detectors.Micro-MOSFETs have almost
isotropic response to radiation.Unlike single dual-MOSFET-dual bias
detectors, MOSFETarrays have some temperature dependence (the
temperaturecoefcient = 0.6%/ C). 34 Most published studies on IVD
inBT involve detectors and dosimetry system from Best Med-ical
Canada. Another MOSFET dosimetry system used inBT comes from the
Centre for Medical Radiation Physics(CMRP), University of
Wollongong. 78 It was found that theirresponse degrades with
exposure to radiation and varies withdistance from a source due to
its dose rate and energy depen-dence. MOSFET system from CMRP is
not yet available inthe market.
The two main disadvantages of MOSFETs for BT mea-surements are:
(1) they are not tissue equivalent, which makestheir dose response
vary with radiation quality and (2) theyhave a rather limited
lifetime. One of their main practicalitieslies in their small size
allowing their insertion inside intra-luminal catheters or even
needles and the possibility of hav-ing multiple MOSFET sensors
along one single line. Recentcoupling of a MOSFET detector with a
sensor capable of de-tecting the position of the MOSFET in 3D
(RADPOS), hasrenewed interest in their use.
MOSFETs have been used to characterize the HDR 192IrLeipzig
surface applicators and found to agree with lms andMonte Carlo
calculations within 3%. 79
Cygler et al. 33 performed in 2006 a feasibility study
usingmicro-MOSFETS (external dimensions: 1 mm diameter by0.5 mm
thickness) during permanent low-dose rate prostateimplants as a
tool for in vivo measurement of the initial doserate within the
urethra and as a mean to help evaluate the over-all quality of the
implant. In this study, IVD in the urethra was
carried out by moving the MOSFET detector along the ure-thra in
1 cm steps. The estimated uncertainty of the MOSFETposition was
within 1 mm. The detector was left at each po-sition to accumulate
dose for 10 min, long enough to providea reasonable measurement
signal.
Bloemen-van Gurp et al. 34, 80 performed two studies in2009
using a linear MOSFET array during permanent prostateimplant. The
overall uncertainty in the measurement proce-dure, determined in a
simulation experiment, was 8.0% andan action level of 16% (2 SD)
for detection of errors in theimplantation procedure is achievable
after validation of thedetector system and measurement conditions.
In their secondstudy, they reported on a technique to monitor the
dose rate in
the urethra and performed IVD in ve patients during and af-ter
implantation of 125I seeds. They concluded that IVD withMOSFET
array during the procedure is a feasible techniqueto evaluate the
dose in the urethra for permanent prostateBT. This study showed the
challenges of performing IVD inBT and the extensive analysis needed
to reach a meaningfulconclusion.
Cherpak et al. 81 performed real-time measurements of ure-thral
dose and position using a RADPOS Array (Best Medi-cal Canada)
during permanent seed implantation for prostateBT. RADPOS Array is
a modied RADPOS detector. 82
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
9/16
070902-8 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-8
Cherpak et al. 81 performed measurements on 17 patients
andconcluded that the modied RADPOS detector with MOS-FET array
instead of a single MOSFET is able to provide ac-curate real-time
dose information which can be used to moni-tor dose rates while
implantation is performed and to estimatetotal integrated dose.
Reniers et al. 83 in 2012, in a feasibilitystudy on a phantom, have
studied the utility of using a RAD-POS system for IVD for
gynecological BT. They reported thatthe RADPOS sensor, if placed,
for example, in the bladderFoley balloon, would detect a 2 mm
motion of the bladder, ata 5% chance of a false positive, with an
action level limit of 9% of the dose delivered. The authors also
found that sourceposition errors caused by, e.g., a wrong rst dwell
position,are more difcult to detect. With a single RADPOS
detectorpositioned in the bladder, dwell position errors below 5
mmand resulting in a dose error within 10% could be detected inthe
tandem but not in the colpostats.
V.D. Alanine
L- -alanine is a nonessential amino acid that has beenused for
electron paramagnetic resonance (EPR) dosimetryin radiation
therapy. Alanine can exist in a form of a whitepowder or can be
formed in the shape of rods, pellets, lms,etc. 84 During
irradiation of alanine, permanent free radicalsare formed. The
concentration of these radicals is proportionalto absorbed dose and
can be measured by EPR spectroscopy.So alanine is a chemical
dosimeter, since dose measurementis based on detection of chemical
species formed during irra-diation. Alanine has some important
advantages as a dosime-ter. Its response is almost independent of
radiation energy anddose rate. It can be formed into small shapes
and requires nobias or wiring. The readout of the radical
concentration is non-destructive and has very little fading with
time.
Unfortunately, it also has disadvantages that limit its
use-fulness in clinical dosimetry. The main disadvantage is a
re-quirement of expensive EPR equipment not easily availablein
clinics. Alanine does not provide an immediate readout of the dose
and it is generally insensitive to doses < 2 Gy. It alsohas some
temperature and humidity dependence. In spite of these limitations,
some feasibility studies were conducted toevaluate its usefulness
in BT. Apart from the phantom stud-ies aimed mostly at the
characterization of the radioactivesources, 8587 few reports exist
on using alanine for IVD of gynecological treatments. 39, 88
Alanine is commercially avail-able, but the tedious readout
procedure needs to be establishedindividually in each department.
At present, use of alanine in
the clinics is very limited due to the readout equipment
beingvery expensive and it is hard to foresee that this will
changein the near future.
V.E. RL and OSL detectors
Recent advances in optically stimulated luminescencedosimeters
(OSLDs) have opened new possibilities for theirapplication in
radiation therapy. 89, 90 OSLDs are gradually re-placing TLDs as
personal radiation monitoring dosimeters forindustry and public
health workers because of their instanta-
neous reading capabilities, faster processing, and the abilityto
store their reading without much degradation of the opticalsignal
(permanent record). To operate in the OSL mode, thecrystals need an
external stimulation (laser or diode) to extractthe reading
postirradiation. The same crystal can also operatein the RL mode
providing the information about the dose rateduring the
irradiation, thus, serving as a true real-time onlinedetector. Al
2O3 :C can be formed as crystals with diameter< 1 mm which can t
inside BT catheters. Even though thesensitive detecting material of
these detectors (Al 2O3 :C) isnot water-equivalent, they have good
potential for IVD in BTdue to their ability to provide feedback in
real time.
RL systems for online dose measurements are not avail-able.
However, a prototype system developed by Andersenet al. 66 in 2009
was investigated to facilitate the preventionand identication of
dose delivery errors in remote afterload-ing BT. The system
consists of a small Al 2O3 :C crystal cou-pled with the optical ber
which carries the light signal gen-erated in the crystal to the
detection system. The system iscapable to operate either in the RL
or OSL mode. The sys-tem allows for automatic online IVD directly
in the tumor re-gion using small detector probes that t into
applicators suchas standard needles or catheters. In the RL mode,
the sys-tem is capable of measuring the absorbed dose rate (with
a0.1 s time resolution) and in the OSL modethe total ab-sorbed
dose. The calibrated system was found to be linearin the tested
dose range. The reproducibility for the RL/OSLmeasurements was
found to be 1.3% (SD). Under certain con-ditions, the RL signal
could be greatly disturbed by the so-called stem signal (i.e.,
unwanted light generated in the bercable upon irradiation). 91 When
taking into account the ef-fect of reproducibility, energy
response, angular dependence,stem effect, instrument and crystal
temperature, light guidetransmission on the reading, and the
calibration uncertainty,
the combined estimated uncertainty budget was found to be8% (SD)
and 5% (SD) for RL and OSL, respectively. Thisinitial study was
followed up with a clinical protocol study onve cervix cancer
patients undergoing PDR BT. 35 For threeof the patients, the
authors found no signicant differences( p > 0.01) between IVD
and TPS calculated reference values(TG 43) at the level of dose per
dwell position, dose per appli-cator, or total dose per pulse. For
the two other patients, theynoted signicant deviations for three
individual pulses and forone dosimeter probe. These differences
could have been dueto applicator movement during the treatment
and/or an incor-rectly positioned probe, respectively.
Kertzscher et al. 36 in 2011 tested the ability of a RL sys-
tem to identify afterloading PDR and HDR gynecological
andprostate BT errors in real time using a novel statistical er-ror
decision criterion. Their phantom studies showed that outof 20
interchanged guide tube errors, time-resolved analysisidentied 17
while accumulated dose identied only two. Ac-cumulated dose
comparisons could leave 10 mm dosimeterdisplacement errors
unidentied and while dose rate compar-isons correctly identied
displacements 5 mm. This phan-tom study demonstrated that Al 2O3:C
real-time dosimetry hasthe potential to detect interchanged guide
tube errors duringPDR and HDR BT and has the ability to identify
applicator
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
10/16
070902-9 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-9
displacements 5 mm. Another important aspect of this studywas to
highlight the shortcoming of using a constant error cri-terion and
instead to recommend using a statistical error cri-terion.
V.F. Plastic scintillation detectors
Plastic scintillation detectors are a promising option forIVD.
PSDs are composed of organic scintillation material(scintillator or
scintillating optical ber) that emits light pro-portionally to the
dose deposited in their detector volume. Thelight produced in the
detector is usually optically coupled toa ber-optic light guide and
transmitted toward a photodetec-tor. The properties of plastic
scintillation detectors have beenstudied for high-energy external
beams. 67, 92 High spatial res-olution, linearity with dose, energy
independence in the mega-voltage energy range, and water
equivalence are among theadvantages that have been demonstrated for
such detectors.Cerenkov light production has also been identied in
the op-tical guide. 67, 92, 93 This light component, often referred
to asstem effect, is produced in the ber when struck by
radiationover a certain energy threshold, which depends on ber
mate-rial, and needs to be removed to perform accurate
dosimetry.Different methods have been proposed to efciently
accountfor this spurious effect. 94, 95 Using these detectors,
possibil-ity of real-time IVD has been demonstrated under
externalbeam radiation 96 and accuracy of better than 1% has
beenachieved. New evidence pointing to possible temperature
de-pendence has recently been reported as a characteristic
beingexhibited by plastic scintillation detectors. 97 An average of
a0.6% decrease in measured dose/ C relative to dose measuredat room
temperature was observed in the range of 1550 C.At the present
time, it is not clear if this thermal dependencecomes from the
construction of the materials used in the de-
sign, the composition of the organic scintillator itself, or
iscoming from the optical train. Since the exact mechanism isnot
well understood, this early communication concluded thatfurther
research is warranted.
PSDs have the capability to perform accurate online IVDduring
HDR 192Ir BT, 58, 68, 69 because they could be cut andshaped in
size that can be easily inserted into catheters orarranged around
applicators that are commonly used in BT.Lambert et al. 58
performed a comparative phantom study of PSDs to other commercially
available detectors (MOSFET,diamond detector, and TLD). Based on
size, accuracy, andreal-time possibilities, the authors claimed
that PSDs showedthe best combination of characteristics to perform
dosimetry
during HDR 192 Ir BT. Because the energy emission spectrumofan
192 Ir radiation source is mainly higher than the
Cerenkovproduction threshold energy, the need for a stem removal
tech-nique has been stressed for clinically relevant situations. 68
Astudy using a prostate phantom was performed by Therriault-Proulx
et al. 69 The authors used a redgreenblue (RGB) pho-todiode as the
photodetection component, allowing for the re-moval of the Cerenkov
component through the polychromaticapproach. Thirteen catheters
were implanted in the phantom:12 for dose delivery and one for the
PSD. The PSD dose rateswere measured in real-time during the
treatment delivery us-
ing a HDR 192Ir source. The average accumulated dose mea-sured
at the PSD location for ve consecutive treatment deliv-eries was
275 14 cGy, in good agreement with the expecteddose of 275 cGy as
calculated by the treatment planning sys-tem. Another phantom study
using an array of 16 PSDs inan insertable applicator that enables
quality assurance of thetreatment delivery and provides an alert to
potential radiationaccidents during HDR BT treatments has been
performed byCartwright et al. 70 The systempresented is capable of
measur-ing doses in a phantom for 1 s exposures with an
uncertaintybetween 2% and 3% for most of the PSDs.
Suchowerska et al. 41 described a plastic scintillator
systemconsisting of a 0.5 mm diameter by 4 mm length BC400
scin-tillator optically coupled to a 0.48 mm core PMMA opticalber
to transmit the signal. They have used a PTW-FreiburgOPTIDOS Reader
to read the signal produced by their scin-tillator detector. 41 The
OPTIDOS reader, consisting of a pho-tomultiplier and an
electrometer unit, was originally designedto measure the dose rate
of 90Sr/ 90 Y beta emitting sources aswell as for 32 P
intravascular BT using different plastic scintil-lator detectors
designed and manufactured by PTW-Freiburg.Note that the
PTW-Freiburg scintillation detectors and OPTI-DOS reader system are
no longer commercially available. Theclinical feasibility of this
study examined urethral dose mea-surements in 24 patients during
HDR prostate BT. The authorsof this study did not report any
temperature dependence fortheir measurement performed inside the
urethra nor any stemeffect when using these PSDs. After the rst 14
patients, im-provements to the dosimeter systemdesign were
implementedthat increased positional accuracy and system
reliability, withthe maximum dose departure from the calculated
dose beingwithin 9% for all of the ten remaining patients and
concludedthat dose to the urethra could be accurately measured
usingthe improved system.
At the present time there are no PSDs or PSD systemsthat are
commercially available for use for in vivo dosime-try for BT. The
only PSD system available commercially isthe EXRADIN W1
Scintillator manufactured by StandardImaging which was designed for
external beam radiother-apy and more specically for the
characterization of smalleld dosimetry (
http://www.standardimaging.com/product_home.php?id=124 ).
VI. DIRECTIONS FOR THE FUTURE
VI.A. Detectors and technology
Most of the development efforts for IVD systems havebeen focused
to the front end of the detection system: the de-tector element(s)
or the sensitive material and their dosimetriccharacteristics to
correct for the effects inuencing their re-sponse. Future
developments would have to be focused on theback end of the
detection system utilized to process the data(i.e., the readings of
the detector) to make the next generationIVD systems user friendly
with automatic data display, re-quiring less manpower, with no
postdata analysis or specialexpertise needed. Furthermore, in order
to be successful forwidespread use, any new technological
innovation for such
Medical Physics, Vol. 40, No. 7, July 2013
http://www.standardimaging.com/product_home.php?id=124http://www.standardimaging.com/product_home.php?id=124http://www.standardimaging.com/product_home.php?id=124http://www.standardimaging.com/product_home.php?id=124
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
11/16
070902-10 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-10
systems will have to be well integrated into the routine
clini-cal application being targeted.
Given existing alternatives for accurate BT dosimeters, fu-ture
requirements will likely be made on IVD systems that canmonitor the
dose in real time, are sensitive to displacementsof all applicators
involved in the treatment, can identify organmotion, and that can
provide immediate alerts of any potentialgross error during ongoing
treatments. Passive detectors, suchas TLDs, OSLDs (when used in the
passive mode), RPLDs,alanine, radiographic and radiochromic lms,
gels, are not ca-pable of monitoring the time-resolved treatment
delivery. Afew studies have introduced the possibility of using the
instan-taneous dose rate for patient QC checks. 31, 35, 36 These
stud-ies indicate that time-resolved dosimetry has potential to
bemore sensitive to error detection than dose verication basedon
integral dose. Therefore, future research will probably fo-cus on
further developing systems that would have the abil-ity to sample
the dose rate in real time while the radiationtreatment is being
delivered to the patient. Currently, goodcandidates for real-time
IVD are RL, 35, 36 PSDs, 69 and MOS-FETs. These detectors are
capable of sampling or measuringthe dose rate which could be useful
for certain applicationsfor which thresholds in dose deviations
could be set and/orupper and lower limits for dose values to
prevent gross errorsand potentially alert the users whether the
treatment shouldor should not be terminated. Although semiconductor
diodesprovide an immediate readout, they are not good candidatesfor
real-time IVD due to their many undesirable
dosimetriccharacteristics (see Table I).
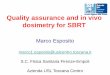
Recently, it has been shown that it is possible to
developdetectors composed of multiple different color PSDs
(mPSD)using a single optical transmission line and capable of
mea-suring the dose accurately (Fig. 2).98 Detectors of this
typecould be used for LDR or HDR interstitial BT applications.
Additional carrier catheters could be sutured within thevicinity
of the implant or nearby a critical structure to monitorthe dose
from the planned implant. The carrier catheters arenot part of the
implant but additional intraluminal cathetersfor the sole purpose
to accommodate the detectors. The read-ings consist of the light
spectrum emitted by each color PSD.The extraction of each
corresponding color from the totalspectrum measured will provide
the dose deposited at corre-sponding color PSD. This type of
detector has the advantageof simultaneous dose rate measurements in
multiple pointswith the potential to improve error detection
capabilities.
F IG . 2. mPSD line detector inserted into a exible
catheter.
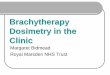
F IG . 3. An example of integrating a detector to a rectal
balloon. In this case,a 0.5 mm diameter by 1.0 mm long plastic
scintillating ber coupled to aclear transmitting ber-optic and an
inatable rectal balloon (upper left) werefully integrated into an
inatable rectal balloon with the detector permanentlymoulded to it
(upper right). Another example illustrating integrating a
com-bination of line detectors and point detectors integrated to an
applicator isshown below. A semicylindrical cut of the rectal
balloon surface onto which,in this case scintillating line and
point probes are attached for detection of dose along the rectal
wall. The individual line and point probes slide intocapillary
tubes permanently attached to the balloon surface.
Stable and clinically relevant detector positioning remainsone
of the most important and critical issues for IVD. Inser-tion of
additional detector catheters may be performed with
the purpose of optimizing detector positioning, e.g., by
in-serting an additional interstitial needle for housing a
dosime-ter probe in the tumor region. A smaller invasive impact
maybe achieved by inserting a sterilized dosimeter in the
urethralcatheter for urethral dose measurements. However, such
in-vasive procedures raise ethical issues as discussed in Sec.IV.A
. Another option is to mould detectors within an appli-cator (see
example in Fig. 3), which has advantages such asxing the sensitive
volume within the geometry of the appli-cator and therefore
reducing the positional uncertainty of thedetector. The applicator
could potentially be designed to con-strain movements of OARs
and/or the target region. Similarmeasures could be achieved with a
urethral catheter with a
closed-end lumen dedicated for housing a dosimeter probe inthe
urethra or along the bladder wall.
Improved integration between afterloader and dosimetrysystem is
warranted. The Bebig Multisource afterloader (byEckert &
Ziegler Bebig GmbH, Berlin, Germany) offers in-tegrated diode IVD
where the dosimetry system can be op-erated from the control unit.
It permits the specication of dose limits and the display of rectum
and bladder doses.A further step forward for integration would be
automatedDICOM import to the dosimeter software and signal
commu-nication between the dosimeter software and the
afterloader.
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
12/16
070902-11 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-11
The communication would help synchronize the dosimeterreadout
with the onset of the treatment, hence, optimize thecomparison
between the delivered treatment with the time andsource coordinates
from the imported DICOM RT plan. An-other attractive solution for
future IVD in BT is the integra-tion of one or several dosimeter
probes into the afterloadingmachinery. Such an afterloader could
offer motorized feedingof dosimeter probes into BT catheters
already inserted intothe patient but unoccupied by the source.
Positioning technol-ogy attached onto both the source wire and
dosimeter probecould both minimize their positional uncertainties
and opti-mize the relative source-to-dosimeter distances. In vivo
de-tector positioning directly inside the source catheters,
e.g.,needles and intracavitary tubes, would in principle alreadybe
possible with sufciently small dosimeter probes as theRADPOS,
MOSFETs and ber-coupled scintillator, and RLprobes.
Recently developed RADPOS system 82, 99, 100 allows for
si-multaneous measurement of dose and position. This detectoris
particularly suited for BT applications and is being exploredto
study not only its sensitivity for error detection during
HDRtreatments 81 but also for applicator movement during
vaginalcylinder treatments and prostate movement during
permanentprostate implants. 81 RADPOS is capable of detecting
prostatemovement during each needle insertion, as well as the
changein the urethral dose after the removal of the ultrasound
probefrom the rectum. 81 Since the RADPOS probe is visible on x-ray
images, it allows to link the coordinates of the point of
measurement before and during the treatment.
VI.B. Error detection criteria
A signicant challenge of future IVD is to dene
relevanterror/decision criteria which take into account that both
sen-
sitivity and specicity of treatment error detection is soundand
robust in a clinical setting. More advanced error deci-sion
criteria could involve a statistical approach where thecomparison
between calculated and measured doses takesinto account the
uncertainty components for both calculatedand measured doses. The
calculated dose is based on assess-ment of both source and detector
positions as they are iden-tied, e.g., in 3D images (US, CT, or
MRI) during treat-ment planning. The identication of both source
and detectorposition is correlated with specic reconstruction
uncertain-ties. The inuence of positional uncertainties on the
calcu-lated dose may be quantied by simulation which incorpo-rates
the source/detector geometry as known from the TPS
and an assumption of a certain distribution of
positioningerrors. 35, 36 Furthermore, dose calculation is
correlated withuncertainties due to the shortcomings of dose
calculation al-gorithms imposed, e.g., by inhomogeneities and
scatter con-ditions. The uncertainty on the measured dose has a
numberof components which are related to the detector
characteris-tics. Based on comparison between calculated and
measureddoses, the measurement should be categorized into Alarmor
No alarm. A certain action level should be dened bybalancing
between sensitivity and false alarms (Table II). Theaction level
can be based on a statistical evaluation of the
incidence of a type 1 error (false alarm), e.g., p = 0.05 or p =
0.01 which means that 5% or 1% of all correct treatmentswill induce
a false alarm, respectively.
The accuracy of the Alarm classication depends on themagnitude
of components in the entire uncertainty budget andas such can be
optimized by reducing uncertainties. These fac-tors relate to the
dosimeter technology, e.g., calibration accu-racy and energy
dependence, and to clinical procedures, e.g.,image reconstruction
and patient-DICOM matching. An op-timized dosimetry integration
into the entire BT workowwould reduce the incidence of false alarms
(type I errors)and/or decrease the failure to detect treatment
errors (typeII errors). This would improve treatment error
detection andminimize the risk of making erroneous decisions
regardingunnecessary treatment interruptions or termination.
An interesting strategy for further improvement of errordecision
criteria could be development of a gamma analysisfor IVD according
to the principles which have been usedin EBRT for comparison of
measured and expected doses,e.g., with EPID dosimetry. 101 With a
gamma analysis an er-ror criterion would be based not only on a
dose difference butcould also combine it with a
distance-to-agreement criterion.In such an analysis, the upfront
knowledge of the geometri-cal uncertainties of the detector and
source positioning couldbe incorporated into the model in order to
decide on relevantdistance-to-agreement criteria.
VI.C. Clinical operation, infrastructure, and workow
Patient involvement should be considered so that the pa-tient is
as comfortable as possible and not stressed by ad-ditional
procedures if possible. Current rectal diode systemsand/or
additional catheter insertion into the urethra/bladderinvolve some
patient discomfort. Reduction of detector size
may contribute to improved patient acceptance. Optimally,the use
of BT source catheters for in vivo detectors, as dis-cussed in Sec.
VI.A , would not require any extra insertion of catheters, and
could potentially make the in vivo system com-pletely invisible for
the patient.
A major barrier for routine implementation of IVD is theadded
workload for the personnel. Developments of new sys-tems should
involve considerations of time consumption, clin-ical robustness,
and ease of use. The Quality ManagementProgram should be optimized
in order to limit the time con-sumption for the personnel. The
measurements should be pre-sented and visualized to the user in
such a way that the evalu-ation and interpretation of the results
is as straightforward as
possible and so that a clear action can be taken from the
mea-surements. The IVD system should also not distract
personnelfrom other important tasks related to treatment planning
anddose delivery.
An example of a general dosimetry integration into an im-age
guided BT workow is shown in the right pane of Fig. 4.Some
potential sources of errors generated during such treat-ment
procedures are specied in the left pane, where thosedetectable with
IVD are highlighted.
An optimal dosimetry integration would involve sourceapplicators
with integrated dosimeter housing, which would
Medical Physics, Vol. 40, No. 7, July 2013
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
13/16
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
14/16
070902-13 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-13
Infrastructure: Is online dosimetry exploited? Is auto-matic
analysis of data incorporated?
Detector position: Is the positional accuracy of the de-tector
addressed and optimized?
Error decision criteria: Fixed level or statistical
ap-proach?
Sensitivity and specicity: Is the sensitivity and speci-city of
the system evaluated?
Communication: Is the dosimetry system able to com-municate with
TPS and/or afterloader?
Prospective IVD: Is IVD used prospectively and system-atically
to evaluate the incidence of errors?
Recent progress of IVD shows that some of these pointshave
already been addressed individually in different publi-cations.
However, the aim and vision for IVD is to create asystem that
embraces all the above aspects.
VII. CONCLUSIONS
The specic role of IVD in BT needs to be dened and es-tablished.
So far, recommendations for BT practice rarely in-clude the
recommendation to perform IVD. This fact is mostlikely mainly
inuenced by the poor ability of current sys-tems to detect errors.
Nevertheless, IVD is used in several de-partments and there is good
potential to improve its utilityand use. Most importantly,
incorporation of routine IVD intoclinical practice requires that
the error detection capability isimproved. Second, streamlined
procedures are needed whichare automatic as far as possible so that
the work load is notexcessive and so that the medical physicist is
not distractedby technical operation. The systems need to be
commerciallyavailable and affordable. Further utilization and
dissemina-tion of IVD will only be feasible if it is cost effective
to as-
sign resources for its infrastructure. Altogether, it should
bedemonstrated that IVD can be developed to become sensitiveto
errors that may have clinical impact and avoidance of errorsshould
be veried.
Proceeding from this, it is crucial to come to a compre-hensive
description of errors in order to make progress withinBT safety.
Systematic IVD in a multicenter setting would be astep forward for
detecting and understanding errors and theirfrequencies. Support of
international databases for error re-porting and for logging user
experiences is important, sincepublications from academic centers
do not reect the major-ity of patient treatments. The Radiation
Oncology Safety In-formation System (ROSIS) database supported by
ESTRO al-
ready supports reporting of BT incidents and the rst reportsfrom
ROSIS include such incidents. 102 Such practice has po-tential to
facilitate signicant improvements in quality for BTby (1) advancing
the use of IVD systems in order to preventand avoid BT errors and
(2) making it possible to focus on themost relevant sources of
errors.
It is the opinion of the authors that IVD in BT is currentlynot
well established in clinical routine to be used for sensitiveand
specic error detection. However, this situation shouldchange over
the coming years by investing in development of IVD with the goal
of establishing an efcient means of inde-
pendent verication of dose delivery in BT. As soon as IVD inBT
becomes better established, there will be a strong need
forrecommendations from professional organizations (e.g., ES-TRO,
ASTRO, AAPM, ABS).
ACKNOWLEDGMENT
The authors have no nancial ties to any of the discussed
detector types and/or to a commercial company.
a) Author to whom correspondence should be addressed. Electronic
mail:[email protected]
1 International Commission on Radiation Units and Measurements,
Doseand volume specication for reporting intracavitary therapy in
gynecol-ogy, ICRU Report No. 38 (ICRU, Bethesta, MD, 1985).
2 R. Ptter et al. , Recommendations from gynaecological (GYN)
GECESTRO working group (II): Concepts and terms in 3D image-based
treat-ment planningin cervix cancer brachytherapy-3D dose volume
parametersand aspects of 3D image-based anatomy, radiation physics,
radiobiology,Radiother. Oncol. 78 , 6777 (2006).
3 T. Major, C. Polgar, K. Lovey, and G. Frohlich, Dosimetric
character-istics of accelerated partial breast irradiation with CT
image-based mul-
ticatheter interstitial brachytherapy: A single institutions
experience,Brachytherapy 10 , 421426 (2011).
4 W. S. Bice, Jr. et al. , Centralized multiinstitutional
postimplant analysisfor interstitial prostate brachytherapy, Int.
J. Radiat. Oncol., Biol., Phys.41 , 921927 (1998).
5 M. J. Rivard, J. L. Venselaar, and L. Beaulieu, The evolution
of brachytherapy treatment planning, Med. Phys. 36 , 21362153
(2009).
6 J. Van Dyk, R. B. Barnett, J. E. Cygler, and P. C. Shragge,
Commission-ing and quality assurance of treatment planning
computers, Int. J. Radiat.Oncol., Biol., Phys. 26 , 261273
(1993).
7 B. Mijnheer, State of the art of in vivo dosimetry, Radiat.
Prot. Dosim.131 , 117122 (2008).
8 AAPM, Report of TG 62 of the Radiation Therapy Committee:
Diodein vivo dosimetry for patients receiving external beam
radiation therapy,AAPM Report No. 87 (Medical Physics Publishing,
Madison, WI, 2005).
9 A. J. Vinall, A. J. Williams, V. E. Currie, E. A. Van, and D.
Huyskens,
Practical guidelines for routine intensity-modulated
radiotherapy veri-cation: Pre-treatment verication with portal
dosimetry and treatment ver-ication with in vivo dosimetry, Br. J.
Radiol. 83 , 949957 (2010).
10 A. Mans et al. , Catching errors with in vivo EPID dosimetry,
Med. Phys.37 , 26382644 (2010).
11 B. Mijnheer, A. S. Beddar, J. Izewska, and C. S. Reft, In
vivo dosimetryin external beam radiotherapy, Med. Phys. 40 (7),
070903 (19pp.) (2013).
12 P. O. Lopez, P. Andreo, J.-M. Cosset, A. Dutreix, and T.
Landberg, Pre-vention of accidental exposures to patients
undergoing radiation therapy,ICRP Publication 86, Annals of the
ICRP (Pergamon, New York, 2000).
13 L. P. Ashton, J.-M. Cosset, V. Levin, A. Martinez, and S.
Nag, Preventionof high-dose-rate brachytherapy accidents, ICRP
Publication 97, Annalsof the ICRP (Pergamon, New York, 2004).
14 IAEA, Lessons learned from accidental exposures in
radiotherapy,IAEA Safety Report Series 17 (IAEA, Vienna, 2000).
15 K. Yoshida et al. , Needle applicator displacement during
high-dose-rate
interstitial brachytherapy for prostate cancer, Brachytherapy
9
, 3641(2010).16 T. Simnor et al. , Justication for
inter-fraction correction of catheter
movement in fractionated high dose-rate brachytherapy treatment
of prostate cancer, Radiother. Oncol. 93 , 253258 (2009).
17 A. A. de Leeuw, M. A. Moerland, C. Nomden, R. H. Tersteeg,J.
M. Roesink, and I. M. Jrgenliemk-Schulz, Applicator
reconstructionand applicator shifts in 3D MR-based PDR
brachytherapy of cervical can-cer, Radiother. Oncol. 93 , 341346
(2009).
18 N. Milickovic et al. , 4D analysis of inuence of patient
movementand anatomy alteration on the quality of 3D U/S-based
prostate HDRbrachytherapy treatment delivery, Med. Phys. 38 ,
49824993 (2011).
19 K. Koedooder, W. N. van, H. N. van der Grient, Y. R. van
Herten,B. R. Pieters, and L. E. Blank, Safety aspects of pulsed
dose rate
Medical Physics, Vol. 40, No. 7, July 2013
http://dx.doi.org/10.1016/j.radonc.2005.11.014http://dx.doi.org/10.1016/j.brachy.2010.12.006http://dx.doi.org/10.1016/S0360-3016(98)90123-7http://dx.doi.org/10.1118/1.3125136http://dx.doi.org/10.1016/0360-3016(93)90206-Bhttp://dx.doi.org/10.1016/0360-3016(93)90206-Bhttp://dx.doi.org/10.1093/rpd/ncn231http://dx.doi.org/10.1259/bjr/31573847http://dx.doi.org/10.1118/1.3397807http://dx.doi.org/10.1118/1.4811216http://dx.doi.org/10.1016/j.brachy.2009.04.006http://dx.doi.org/10.1016/j.radonc.2009.09.015http://dx.doi.org/10.1016/j.radonc.2009.05.003http://dx.doi.org/10.1118/1.3618735http://dx.doi.org/10.1118/1.3618735http://dx.doi.org/10.1016/j.radonc.2009.05.003http://dx.doi.org/10.1016/j.radonc.2009.09.015http://dx.doi.org/10.1016/j.brachy.2009.04.006http://dx.doi.org/10.1118/1.4811216http://dx.doi.org/10.1118/1.3397807http://dx.doi.org/10.1259/bjr/31573847http://dx.doi.org/10.1093/rpd/ncn231http://dx.doi.org/10.1016/0360-3016(93)90206-Bhttp://dx.doi.org/10.1016/0360-3016(93)90206-Bhttp://dx.doi.org/10.1118/1.3125136http://dx.doi.org/10.1016/S0360-3016(98)90123-7http://dx.doi.org/10.1016/j.brachy.2010.12.006http://dx.doi.org/10.1016/j.radonc.2005.11.014
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
15/16
070902-14 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-14
brachytherapy: Analysis of errors in 1300 treatment sessions,
Int. J. Ra-diat. Oncol., Biol., Phys. 70 , 953960 (2008).
20 L. Beaulieu et al. , Report of the Task Group 186 on
model-based dosecalculation methods in brachytherapy beyond the
TG-43 formalism: Cur-rent status and recommendations for clinical
implementation, Med. Phys.39 , 62086236 (2012).
21 J. G. Sutherland, K. M. Furutani, Y. I. Garces, and R. M.
Thomson,Model-based dose calculations for 125 I lung brachytherapy,
Med. Phys.39 , 43654377 (2012).
22 H. Afsharpour et al. , Consequences of dose heterogeneity on
the biologi-cal efciency of 103 Pd permanent breast seed implants,
Phys. Med. Biol.57 , 809823 (2012).23 S. A. White,G. Landry, G. F.
van, F. Verhaegen,and B. Reniers, Inuenceof trace elements in human
tissue in low-energy photon brachytherapydosimetry, Phys. Med.
Biol. 57 , 35853596 (2012).
24 ICRU, International Commission on Radiation Units and
Measurements,Dose and volume specication for reporting interstitial
therapy, ICRUReport No. 58 (ICRU, Bethesta, 1997).
25 S. Nag et al. , The American Brachytherapy Society
recommendations forlow-dose-rate brachytherapy for carcinoma of the
cervix, Int. J. Radiat.Oncol., Biol., Phys. 52 , 3348 (2002).
26 A. N. Viswanathan and B. Thomadsen, American Brachytherapy
Societyconsensus guidelines for locally advanced carcinoma of the
cervix. Part I:General principles, Brachytherapy 11 , 3346
(2012).
27 B. J. Davis et al. , American Brachytherapy Society consensus
guide-lines for transrectal ultrasound-guided permanent prostate
brachytherapy,Brachytherapy 11 , 619 (2012).
28G. Kovacs et al. , GEC/ESTRO-EAU recommendations on
temporarybrachytherapy using stepping sources for localised
prostate cancer, Ra-diother. Oncol. 74 , 137148 (2005).
29 C. Salembier et al. , Tumour and target volumes in permanent
prostatebrachytherapy: A supplement to the ESTRO/EAU/EORTC
recom-mendations on prostate brachytherapy, Radiother. Oncol. 83 ,
310(2007).
30 R. Alecu and M. Alecu, In vivo rectal dose measurements with
diodes toavoid misadministrations during intracavitary high dose
rate brachyther-apy for carcinoma of the cervix, Med. Phys. 26 ,
768770 (1999).
31 K. Tanderup, J. J. Christensen, J. Granfeldt, and J. C.
Lindegaard, Geo-metric stability of intracavitary pulsed dose rate
brachytherapy monitoredby in vivo rectal dosimetry, Radiother.
Oncol. 79 , 8793 (2006).
32 I. A. Brezovich, J. Duan, P. N. Pareek, J. Fiveash, and M.
Ezekiel, In vivourethral dose measurements: A method to verify high
dose rate prostatetreatments, Med. Phys. 27 , 22972301 (2000).
33J. E. Cygler, A. Saoudi, G. Perry, C. Morash, and C. E.,
Feasibility studyof using MOSFET detectors for in vivo dosimetry
during permanent low-dose-rate prostate implants, Radiother. Oncol.
80 , 296301 (2006).
34 E. J. Bloemen-van Gurp et al. , In vivo dosimetry using a
linear MOSFET-array dosimeter to determine the urethra dose in 125
I permanent prostateimplants, Int. J. Radiat. Oncol., Biol., Phys.
73 , 314321 (2009).
35 C. E. Andersen, S. K. Nielsen, J. C. Lindegaard, and K.
Tanderup, Time-resolved in vivo luminescence dosimetry for online
error detection inpulsed dose-rate brachytherapy, Med. Phys. 36 ,
50335043 (2009).
36 G. Kertzscher, C. E. Andersen, F. A. Siebert, S. K. Nielsen,
J. C. Lin-degaard, and K. Tanderup, Identifying afterloading PDR
and HDRbrachytherapy errors using real-time ber-coupled Al 2 O3 :C
dosimetryand a novel statistical error decision criterion,
Radiother. Oncol. 100 ,456462 (2011).
37 D. OConnell, C. A. Joslin, N. Howard, N. W. Ramsey, and W. E.
Liv-ersage, The treatment of uterine carcinoma using the Cathetron.
Part I.
Technique, Br. J. Radiol. 40
, 882887 (1967).38 C. A. Joslin, C. W. Smith, and A. Mallik, The
treatment of cervix cancerusing high activity 60 Co sources, Br. J.
Radiol. 45 , 257270 (1972).
39 K. Schultka, B. Ciesielski, K. Serkies, T. Sawicki, Z.
Tarnawska, andJ. Jassem, EPR/alanine dosimetry in LDR
brachytherapy: A feasibilitystudy, Radiat. Prot. Dosim. 120 ,
171175 (2006).
40 M. Allahverdi, M. Sarkhosh, M. Aghili, R. Jaberi, A. Adelnia,
andG. Geraily, Evaluation of treatment planning system of
brachytherapyaccording to dose to the rectum delivered, Radiat.
Prot. Dosim. 150 , 312315 (2012).
41 N. Suchowerska, M. Jackson, J. Lambert, Y. B. Yin, G. Hruby,
andD. R. McKenzie, Clinical trials of a urethral dose measurement
system inbrachytherapy using scintillation detectors, Int. J.
Radiat. Oncol., Biol.,Phys. 79 , 609615 (2011).
42 J. A. Raf et al. , Determination of exit skin dose for 192 Ir
intracavitaryaccelerated partial breast irradiation with
thermoluminescent dosimeters,Med. Phys. 37 , 26932702 (2010).
43 R. A. Kinhikar et al. , Clinical application of a OneDose
MOSFET forskin dose measurements during internal mammary chain
irradiation withhigh dose rate brachytherapy in carcinoma of the
breast, Phys. Med. Biol.51 , N263N268 (2006).
44 C. A. Mangold, A. Rijnders, D. Georg, L. E. Van, R. Ptter,
andD. Huyskens, Quality control in interstitial brachytherapy of
the breastusing pulsed dose rate: Treatment planning and dose
delivery with an Ir-192 afterloading system, Radiother. Oncol. 58 ,
4351 (2001).
45 M. J. Rivard et al. , Update of AAPM Task Group No. 43
Report: A re-vised AAPM protocol for brachytherapy dose
calculations, Med. Phys.31 , 633674 (2004).
46 R. Bachelot-Narquin, Measures taken by the French Health
Minister toensure safety in radiotherapy treatments, Safety in
External Radiother-apy Treatments (ASN, Paris, 2009), Vol. 185, pp.
57 (available URL:http://www.conference-radiotherapy-asn.com ).
47 F. Guedea et al. , Overview of brachytherapy resources in
Europe: A sur-vey of patterns of care study for brachytherapy in
Europe, Radiother.Oncol. 82 , 5054 (2007).
48 F. Guedea et al. , Overview of brachytherapy resources in
Latin America:A patterns-of-care survey, Brachytherapy 10 , 363368
(2011).
49 R. Ptter, L. E. Van, N. Gerstner, and A. Wambersie, Survey of
the use of the ICRU 38 in recording and reporting cervical cancer
brachytherapy,Radiother. Oncol. 58 , 1118 (2001).
50 T. Toita et al. , Patterns of radiotherapy practice for
patients with cervical
cancer(1999-2001): Patterns of care study in Japan, Int. J.
Radiat. Oncol.,Biol., Phys. 70 , 788794 (2008).
51 W. Small, Jr., B. Erickson, and F. Kwakwa, American
Brachytherapy So-ciety survey regarding practice patterns of
postoperative irradiation for en-dometrial cancer: Current status
of vaginal brachytherapy, Int. J. Radiat.Oncol., Biol., Phys. 63 ,
15021507 (2005).
52 K. S. Kapp, G. F. Stuecklschweiger, D. S. Kapp, and A. G.
Hackl,Dosimetry of intracavitary placements for uterine and
cervical carci-noma: Results of orthogonal lm, TLD, and CT-assisted
techniques, Ra-diother. Oncol. 24 , 137146 (1992).
53 D. W. O. Rogers, General characteristics of radiation
dosimeters and aterminology to describe them, in Clinical Dosimetry
Measurements in Radiotherapy , edited by D. W. O. Rogers and J.
Cygler (Medical PhysicsPublishing, Madison, 2009), pp. 137146.
54 J. F. Williamson and M. J. Rivard, Quantitative dosimetry
methodsfor brachytherapy, in Brachytherapy Physics , edited by B.
Thomadsen,
M. J. Rivard, and W. Butler (Medical Physics Publishing,
Madison, WI,2005).55 T. Nose et al. , In vivo dosimetry of
high-dose-rate brachytherapy: Study
on 61 head-and-neck cancer patients using radiophotoluminescence
glassdosimeter, Int. J. Radiat. Oncol., Biol., Phys. 61 , 945953
(2005).
56 T. Nose et al. , In vivo dosimetry of high-dose-rate
interstitial brachyther-apy in the pelvic region: Use of a
radiophotoluminescence glass dosimeterfor measurement of 1004
points in 66 patients with pelvic malignancy,Int. J. Radiat.
Oncol., Biol., Phys. 70 , 626633 (2008).
57 E. L. Seymour, S. J. Downes, G. B. Fogarty, M. A. Izard, and
P. Met-calfe, In vivo real-time dosimetric verication in high dose
rate prostatebrachytherapy, Med. Phys. 38 , 47854794 (2011).
58 J. Lambert, T. Nakano, S. Law, J. Elsey, D. R. McKenzie, and
N. Suchow-erska, In vivo dosimeters for HDR brachytherapy: A
comparison of adiamond detector, MOSFET, TLD, and scintillation
detector, Med. Phys.34 , 17591765 (2007).
59
A. S. Kirov, J. F. Williamson, A. S. Meigooni, and Y. Zhu,
TLD,diode and Monte Carlo dosimetry of an 192 Ir source for high
dose-ratebrachytherapy, Phys. Med. Biol. 40 , 20152036 (1995).
60 M. Westermark, J. Arndt, B. Nilsson, and A. Brahme,
Comparativedosimetry in narrow high-energy photon beams, Phys. Med.
Biol. 45 ,685702 (2000).
61 G. Anagnostopoulos et al. , In vivo thermoluminescence
dosimetry doseverication of transperineal 192 Ir high-dose-rate
brachytherapy using CT-based planning for the treatment of prostate
cancer, Int. J. Radiat. Oncol.,Biol., Phys. 57 , 11831191
(2003).
62 R. Das, W. Toye, T. Kron, S. Williams, and G. Duchesne,
Thermolumi-nescence dosimetry for in vivo verication of high dose
rate brachyther-apy for prostate cancer, Australas. Phys. Eng. Sci.
Med. 30 , 178184(2007).
Medical Physics, Vol. 40, No. 7, July 2013
http://dx.doi.org/10.1016/j.ijrobp.2007.11.003http://dx.doi.org/10.1016/j.ijrobp.2007.11.003http://dx.doi.org/10.1118/1.4747264http://dx.doi.org/10.1118/1.4729737http://dx.doi.org/10.1088/0031-9155/57/3/809http://dx.doi.org/10.1088/0031-9155/57/11/3585http://dx.doi.org/10.1016/S0360-3016(01)01755-2http://dx.doi.org/10.1016/S0360-3016(01)01755-2http://dx.doi.org/10.1016/j.brachy.2011.07.003http://dx.doi.org/10.1016/j.brachy.2011.07.005http://dx.doi.org/10.1016/j.radonc.2004.09.004http://dx.doi.org/10.1016/j.radonc.2004.09.004http://dx.doi.org/10.1016/j.radonc.2007.01.014http://dx.doi.org/10.1118/1.598598http://dx.doi.org/10.1016/j.radonc.2006.02.016http://dx.doi.org/10.1118/1.1312811http://dx.doi.org/10.1016/j.radonc.2006.07.008http://dx.doi.org/10.1016/j.ijrobp.2008.08.040http://dx.doi.org/10.1118/1.3238102http://dx.doi.org/10.1016/j.radonc.2011.09.009http://dx.doi.org/10.1259/0007-1285-40-480-882http://dx.doi.org/10.1259/0007-1285-45-532-257http://dx.doi.org/10.1093/rpd/nci528http://dx.doi.org/10.1093/rpd/ncr415http://dx.doi.org/10.1016/j.ijrobp.2010.03.030http://dx.doi.org/10.1016/j.ijrobp.2010.03.030http://dx.doi.org/10.1118/1.3429089http://dx.doi.org/10.1088/0031-9155/51/14/N01http://dx.doi.org/10.1016/S0167-8140(00)00270-Xhttp://dx.doi.org/10.1118/1.1646040http://www.conference-radiotherapy-asn.com/http://dx.doi.org/10.1016/j.radonc.2006.11.011http://dx.doi.org/10.1016/j.radonc.2006.11.011http://dx.doi.org/10.1016/j.brachy.2010.12.003http://dx.doi.org/10.1016/S0167-8140(00)00266-8http://dx.doi.org/10.1016/j.ijrobp.2007.10.045http://dx.doi.org/10.1016/j.ijrobp.2007.10.045http://dx.doi.org/10.1016/j.ijrobp.2005.04.038http://dx.doi.org/10.1016/j.ijrobp.2005.04.038http://dx.doi.org/10.1016/0167-8140(92)90372-2http://dx.doi.org/10.1016/0167-8140(92)90372-2http://dx.doi.org/10.1016/j.ijrobp.2004.10.031http://dx.doi.org/10.1016/j.ijrobp.2007.09.053http://dx.doi.org/10.1118/1.3615161http://dx.doi.org/10.1118/1.2727248http://dx.doi.org/10.1088/0031-9155/40/12/002http://dx.doi.org/10.1088/0031-9155/45/3/308http://dx.doi.org/10.1016/S0360-3016(03)00762-4http://dx.doi.org/10.1016/S0360-3016(03)00762-4http://dx.doi.org/10.1007/BF03178424http://dx.doi.org/10.1007/BF03178424http://dx.doi.org/10.1016/S0360-3016(03)00762-4http://dx.doi.org/10.1016/S0360-3016(03)00762-4http://dx.doi.org/10.1088/0031-9155/45/3/308http://dx.doi.org/10.1088/0031-9155/40/12/002http://dx.doi.org/10.1118/1.2727248http://dx.doi.org/10.1118/1.3615161http://dx.doi.org/10.1016/j.ijrobp.2007.09.053http://dx.doi.org/10.1016/j.ijrobp.2004.10.031http://dx.doi.org/10.1016/0167-8140(92)90372-2http://dx.doi.org/10.1016/0167-8140(92)90372-2http://dx.doi.org/10.1016/j.ijrobp.2005.04.038http://dx.doi.org/10.1016/j.ijrobp.2005.04.038http://dx.doi.org/10.1016/j.ijrobp.2007.10.045http://dx.doi.org/10.1016/j.ijrobp.2007.10.045http://dx.doi.org/10.1016/S0167-8140(00)00266-8http://dx.doi.org/10.1016/j.brachy.2010.12.003http://dx.doi.org/10.1016/j.radonc.2006.11.011http://dx.doi.org/10.1016/j.radonc.2006.11.011http://www.conference-radiotherapy-asn.com/http://dx.doi.org/10.1118/1.1646040http://dx.doi.org/10.1016/S0167-8140(00)00270-Xhttp://dx.doi.org/10.1088/0031-9155/51/14/N01http://dx.doi.org/10.1118/1.3429089http://dx.doi.org/10.1016/j.ijrobp.2010.03.030http://dx.doi.org/10.1016/j.ijrobp.2010.03.030http://dx.doi.org/10.1093/rpd/ncr415http://dx.doi.org/10.1093/rpd/nci528http://dx.doi.org/10.1259/0007-1285-45-532-257http://dx.doi.org/10.1259/0007-1285-40-480-882http://dx.doi.org/10.1016/j.radonc.2011.09.009http://dx.doi.org/10.1118/1.3238102http://dx.doi.org/10.1016/j.ijrobp.2008.08.040http://dx.doi.org/10.1016/j.radonc.2006.07.008http://dx.doi.org/10.1118/1.1312811http://dx.doi.org/10.1016/j.radonc.2006.02.016http://dx.doi.org/10.1118/1.598598http://dx.doi.org/10.1016/j.radonc.2007.01.014http://dx.doi.org/10.1016/j.radonc.2004.09.004http://dx.doi.org/10.1016/j.radonc.2004.09.004http://dx.doi.org/10.1016/j.brachy.2011.07.005http://dx.doi.org/10.1016/j.brachy.2011.07.003http://dx.doi.org/10.1016/S0360-3016(01)01755-2http://dx.doi.org/10.1016/S0360-3016(01)01755-2http://dx.doi.org/10.1088/0031-9155/57/11/3585http://dx.doi.org/10.1088/0031-9155/57/3/809http://dx.doi.org/10.1118/1.4729737http://dx.doi.org/10.1118/1.4747264http://dx.doi.org/10.1016/j.ijrobp.2007.11.003http://dx.doi.org/10.1016/j.ijrobp.2007.11.003
-
8/10/2019 In Vivo Dosimetry in Brachytherapy (1)
16/16
070902-15 Tanderup et al. : In vivo dosimetry in brachytherapy
070902-15
63 W. Toye, R. Das, T. Kron, R. Franich, P. Johnston, and G.
Duchesne,An in vivo investigative protocol for HDR prostate
brachytherapy usingurethral and rectal thermoluminescence
dosimetry, Radiother. Oncol. 91 ,243248 (2009).
64 C. Waldhusl, A. Wambersie, R. Potter, and D. Georg, In-vivo
dosimetryfor gynaecological brachytherapy: Physical and clinical
considerations,Radiother. Oncol. 77 , 310317 (2005).
65 J. M. Fagerstrom, J. A. Micka, and L. A. DeWerd, Response of
an im-plantable MOSFET dosimeter to 192 Ir HDR radiation, Med.
Phys. 35 ,57295737 (2008).
66 C. E. Andersen, S. K. Nielsen, S. Greilich, J. Helt-Hansen,
J. C. Linde-
gaard, and K. Tanderup, Characterization of a ber-coupled Al 2
O3 :C lu-minescence dosimetry system for online in vivo dose
verication during192 Ir brachytherapy, Med. Phys. 36 , 708718
(2009).
67 A. S. Beddar, T. R. Mackie, and F. H. Attix, Water-equivalent
plasticscintillation detectors for high-energy beam dosimetry: I.
Physical charac-teristics and theoretical consideration, Phys. Med.
Biol. 37 , 18831900(1992).
68 J. Lambert, D. R. McKenzie, S. Law, J. Elsey, and N.
Suchowerska, Aplastic scintillation dosimeter for high dose rate
brachytherapy, Phys.Med. Biol. 51 , 55055516 (2006).
69 F. Therriault-Proulx, T. M. Briere, F. Mourtada, S. Aubin, S.
Beddar,and L. Beaulieu, A phantom study of an in vivo dosimetry
system us-ing plastic scintillation detectors for real-time
verication of 192 Ir HDRbrachytherapy, Med. Phys. 38 , 25422551
(2011).
70 L. E. Cartwright, N. Suchowerska, Y. Yin, J. Lambert, M.
Haque, andD. R. McKenzie, Dose mapping of the rectal wall during
brachyther-
apy with an array of scintillation dosimeters, Med. Phys. 37 ,
22472255(2010).
71 M. Anton et al. , In vivo dosimetry in the urethra using
alanine/ESR dur-ing 192 Ir HDR brachytherapy of prostate cancer: A
phantom study, Phys.Med. Biol. 54 , 29152931 (2009).
72 S. M. Hsu et al. , Clinical application of
radiophotoluminescent glassdosimeter for dose verication of
prostate HDR procedure, Med. Phys.35 , 55585564 (2008).
73 A. Ismail et al. , Radiotherapy quality assurance by
individualized in vivodosimetry: State of the art, Cancer
Radiother. 13 , 182189 (2009).
74 J. E. Cygler, K. Tanderup, A. S. Beddar, and J.
Perez-Calatayud, In vivodosimetry in brachytherapy, in
Comprehensive Brachytherapy: Physicaland Clinical Aspects , edited
by J. Venselaar, D. Baltas, A. S. Meigooni,and P. Hoskin (Taylor
& Francis, London, 2012), pp. 379397.
75 D. W. O. Rogers and J. Cygler, Clinical Dosimetry
Measurements in Ra-diotherapy (Medical Physics Publishing, Madison,
2009).
76A. Piermattei, L. Azario, G. Monaco, A. Soriani, and G.
Arcovito, p-typesilicon detector for brachytherapy dosimetry, Med.
Phys. 22 , 835839(1995).
77 M. Soubra, J. Cygler, and G. Mackay, Evaluation of a dual
bias dualmetal oxide-silicon semiconductor eld effect transistor
detector as radia-tion dosimeter, Med. Phys. 21 , 567572
(1994).
78 V. O. Zilio, O. P. Joneja, Y. Popowski, A. Rosenfeld, and R.
Chawla,Absolute depth-dose-rate measurements for an 192 Ir HDR
brachytherapysource in water using MOSFET detectors, Med. Phys. 33
, 15321529(2006).
79 H. Niu, W. C. Hsi, J. C. Chu, M. C. Kirk, and E. Kouwenhoven,
Dosi-metric characteristics of the Leipzig surface applicators used
in the highdose rate brachy radiotherapy, Med. Phys. 31 , 33723377
(2004).
80 E. J. Bloemen-van Gurp et al. , In vivo dosimetry with a
linear MOSFETarray to evaluate the urethra dose during permanent
implant brachyther-apy using iodine-125, Int. J. Radiat. Oncol.,
Biol., Phys. 75 , 12661272
(2009).81 A. Cherpak, J. Cygler, and G. Perry, Real-time
measurement of urethraldose and position using a RADPOS array
during permanent seed implan-tation for prostate brachytherapy,
Med. Phys. 38 , 3577 (2011).
82 A. Cherpak, W. Ding, A. Hallil, and J. E. Cygler, Evaluation
of a novel4D in vivo dosimetry system, Med. Phys. 36 , 16721679
(2009).
83 B. Reniers, G. Landry, R. Eichner, A. Hallil, and F.
Verhaegen, In vivodosimetry for gynaecological brachytherapy using
a novel position sen-sitive radiation detector: Feasibility study,
Med. Phys. 39 , 19251935(2012).
84 M. Farahani, F. C. Eichmiller, and W. L. McLaughlin, New
method forshielding electron beams used for head and neck cancer
treatment, Med.Phys. 20 , 12371241 (1993).
85 S. Olsson, E. S. Bergstrand, A. K. Carlsson, E. O. Hole, and
E. Lund,Radiation dose measurements with alanine/agarose gel and
thin alaninelms arounda 192 Ir brachytherapysource, using ESR
spectroscopy, Phys.Med. Biol. 47 , 13331356 (2002).
86 C. S. Calcina, A. A. de, J. R. Rocha, F. C. Abrego, and O.
Baffa, Ir-192 HDR transit dose and radial dose function
determination using ala-nine/EPR dosimetry, Phys. Med. Biol. 50 ,
11091117 (2005).
87 A. C. De, S. Onori, E. Petetti, A. Piermattei, and L. Azario,
Alanine/EPRdosimetry in brachytherapy, Phys. Med. Biol. 44 ,
11811191 (1999).
88 B. Ciesielski, K. Schultka, A. Kobierska, R. Nowak, and Z.
Peimel-Stuglik, In vivo alanine/EPR dosimetry in daily clinical
practice: A fea-sibility study, Int. J. Radiat. Oncol., Biol.,
Phys. 56 , 8