Embed Size (px)
Citation preview

MAIN RESEARCH ARTICLE
Incidence of cervical cancer and age-specific survival ofsmall cell cervical carcinoma in TaiwanCHAO-YUAN HUANG1,6∗, SAN-LIN YOU2,3∗, CHIEN-JEN CHEN2,3, WEN-FANG CHENG4,5, HUI-CHUN LUO2,3
& CHANG-YAO HSIEH4
1Division of Radiation Oncology, Department of Oncology, 4Department of Obstetrics and Gynecology, and 5GraduateInstitute of Oncology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei,Taiwan, 2Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei, Taiwan, 3GenomicsResearch Center, Academia Sinica, Taipei, Taiwan, and 6Department of Radiological Technology, Yuanpei University, Hsinchu,Taiwan
Key wordsCancer, epidemiology, incidence, survival rate,small cell cervical carcinoma, Taiwan
CorrespondenceDr Chao-Yuan Huang, Division of RadiationOncology, Department of Oncology, NationalTaiwan University Hospital and National TaiwanUniversity College of Medicine, Taipei 100,Taiwan. E-mail: [email protected]
Conflict of interestThe authors have stated explicitly that thereare no conflicts of interest in connection withthis article.
Received: 14 December 2010Accepted: 12 August 2011
DOI: 10.1111/j.1600-0412.2011.01261.x
∗ C.-Y. Huang and S.-L. You contributedequally to this work.
Abstract
Objective. To determine the incidence of cervical cancer and the age-specific sur-vival from small cell cervical carcinoma in Taiwan. Design. Retrospective study.Setting. Taiwan. Population. Women diagnosed with cervical cancer from 1991 to2005. Methods. Analysis of data from the National Cancer Registration Systemand National Death Certification System. Main Outcome Measures. Incidence andage at diagnosis of cervical carcinoma and age-specific and overall survival fromsmall cell cervical carcinoma. Results. During the study period, 36 122 women werediagnosed with cervical cancer, and 81.8% had squamous cell carcinoma (SCC).For the periods 1991–1995, 1996–2000 and 2001–2005, the mean age at diagno-sis increased from 53.9±13.3 to 55.0±14.9 and then to 56.7±14.7 years, respec-tively. The incidence of SCC decreased from 1991 to 2005. During the same pe-riod, non-significant increases of adenocarcinoma and small cell carcinoma werenoted. For SCC, occurrence peaked in 1991–1995 in patients 50–59 years of age.From 1996 to 2005, it peaked in patients 40–49 years of age. For cervical ade-nocarcinoma, occurrence peaked in patients 40–49 years of age, with a steadyincrease in this age group from 1991 to 2005. Occurrence of small cell cervicalcarcinoma peaked in the period 1991–1995 in patients 30–39 years of age. Dur-ing the 15 years of the study, the overall mortality rate of the 198 patients withsmall cell cervical carcinoma was 65.7%. Conclusions. In Taiwan, the incidence ofsmall cell cervical carcinoma and adenocarcinoma tended to increase, but the inci-dence of squamous cell cervical carcinoma significantly decreased during the period1991–2005.
Abbreviations: ANOVA, analysis of variance; Pap, Papanicolau; SCC, squamous cellcarcinoma; SD, standard deviation; SEER, Surveillance, Epidemiology and EndResults; TCR, Taiwan Cancer Registry.
Introduction
Incidence of squamous cell carcinoma (SCC) of the uter-ine cervix and mortality rates have decreased significantlyin Nordic and European countries and in the USA over thepast three decades, largely due to comprehensive screeningprograms (1–8). A report by Engholm et al. (5) indicatedthat from 1996 to 2005 the mortality rate from cervical can-cer declined in all Nordic countries, with the exception of
Sweden where the rate remained stable; the highest rate wasseen in Denmark, with 5.8 cervical cancer deaths per 100 000women per year, and the lowest was seen in Finland, with 2.3deaths per 100 000 women per year. Though the impact ofscreening in reducing the incidence of SCC is clear, the im-pact on reducing the mortality due to adenocarcinoma of thecervix has been less significant (3,9,10). Contrary to decreas-ing trends of cervical cancer incidence and mortality seen inmany countries, Arbyn et al. (11) reported rising trends of
1342C© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349
A C TA Obstetricia et Gynecologica

C.-Y. Huang et al. Cervical carcinoma in Taiwan
incidence in Lithuania, Bulgaria and Romania, and increasingmortality due to cervical cancer in Latvia, Lithuania, Bulgariaand Romania.
In Taiwan, an island country of population approximately27million, cervical cancer remains the most frequently di-agnosed neoplasm, with an incidence of 55.66 per 100 000in 1999 (12). This observation may be explained by the Tai-wanese population’s much lower compliance (23.5% in 1999)with Papanicolaou (Pap) smear screening than that reportedfor other developed countries (generally >70%). This lowcompliance remains, despite the Taiwan National Health In-surance System paying for the examination since 1995 (13).Although compliance with guidelines for triennial Pap smearshas increased in Taiwan (51% for 2005–2007) (14), partic-ipation remains lower than in other countries. Since 1996,early cervical cancer detection in screening participants hasresulted in a 54.7% reduction in the incidence of invasivecervical cancer (15). Even so, cervical cancer remains a majorhealth concern in Taiwan.
Recent reports from developed countries describe a grow-ing incidence of non-SCC of the uterine cervix, in contrast todecreasing trends in cervical SCC, a phenomenon highlight-ing the prognostic value of tumor histopathology (16). Ofthe types of cervical non-SCC, small cell cervical carcinomais least reported, but is highly malignant (17). Clear cell ade-nocarcinoma is another unique category of cervical cancerthat shows extremely poor prognosis (3,9,10).
While many countries, like Taiwan, have aggressively pur-sued screening programs for cervical cancer, not all rateshave dropped (9,18). To our knowledge, no population-basedstudies have yet evaluated the incidence and age-specific sur-vival from small cell cervical carcinoma in Taiwan. The objec-tive of the present study was to characterize the mean age atdiagnosis, trend of diagnostic age-specific proportions, age-adjusted incidence and age-specific survival from small cellcervical carcinoma based on national registries in Taiwan.
Material and methods
Patient data from computerized Taiwanese population na-tional registries, including the National Death Certifica-tion System and the National Cancer Registration Sys-tem, were obtained for analyses. Epidemiological data (e.g.incidence rates, patient numbers and population size)were obtained from the Taiwan Cancer Registry (TCR;http://crs.cph.ntu.edu.tw, last accessed on 23 November2010) founded in 1979 by the Department of Health of Tai-wan. The TCR is financially supported by the National De-partment of Health, with the aim of estimating the cancerincidence in Taiwan. It is a population-based cancer registrycovering more than 22million people and an estimated 80%of all cancer cases in Taiwan (19). Hospitals with >50 bedsare obliged to submit information on newly diagnosed can-
cer patients to the TCR, which reimburses the hospitals onthe basis of numbers of cases reported in order to reduce thelikelihood of under-reporting. All cancer registry databases inthe TCR are linked with death certificates from the NationalDeath Database. Persons not identified by this process weretherefore considered to be alive as far as the present studyis concerned (passive follow up). The database was analyzedfor the period from 1991 to 2005 to determine the followingparameters: (1) incidence and age at diagnosis of various his-tological types of cervical carcinoma; and (2) age-specific andoverall survival of small cell cervical carcinoma. Data usedto evaluate the age of onset of cervical cancer by histologi-cal type were grouped into three study periods (1991–1995,1996–2000 and 2001–2005).
Cases of cervical cancer were identified in these reg-istries and categorized according to the InternationalClassification of Disease for Oncology. Classifications in-cluded squamous carcinoma (8050–8130), adenocarcinoma(8140–8490), adenosquamous carcinoma (8560), small cellcarcinoma (8041, 8052) and carcinoma not otherwise spec-ified (8010). The attending physician ultimately made thediagnosis of cervical cancer based on pathological and clin-ical findings, and after diagnosis the data were added to theNational Cancer Registration system.
Statistical analyses
All statistical analyses were performed using SPSS 15.0 (SPSSInc., Chicago, IL, USA). Continuous variables are presentedas the means±SD for each group, and categorical variablesas number (n) and percentage per group. One-way analysisof variance (ANOVA) followed by Tukey’s post hoc multi-ple comparison test was performed to examine patient agein relation to the type of cervical cancer. Linear regressionwas performed to evaluate potential trends in the incidenceof cervical cancer over time. Patient survival following smallcell cervical carcinoma diagnosis was analyzed by age groupby comparing Kaplan–Meier curves using the log-rank test.In the present study, ‘survival’ means overall survival, notdisease-specific survival. Data regarding whether a particularperson was dead were derived from the national death cer-tification system. However, this system does not record thecause of death, only that death occurred. All tests were twosided, where appropriate, and were considered significantwhen p<0.05.
Results
Table 1 summarizes the number of patients diagnosed witheach type of cervical cancer during each year of the studyperiod. During the study period, 36 122 women were diag-nosed with cervical cancer. In each year, more patients werediagnosed with SCC than any of the other cancer types, andoverall 81.8% of patients diagnosed with cervical cancer were
C© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349 1343

Cervical carcinoma in Taiwan C.-Y. Huang et al.
Table 1. Number of patients diagnosed with cervical carcinoma per year in Taiwan and the proportion of different pathological classifications,
1991–2005.
Year Squamous cell Adenocarcinoma Adenosquamous Papillary Small cell Clear cell Othern (%) n (%) n (%) n (%) n (%) n (%) n (%)
1991 1 796 (86.14) 125 (5.99) 50 (2.4) 11 (0.53) 10 (0.48) 3 (0.14) 90 (4.32)1992 1 946 (83.34) 199 (8.52) 46 (1.97) 3 (0.13) 9 (0.39) 7 (0.3) 125 (5.35)1993 1 916 (81.81) 194 (8.28) 56 (2.39) 6 (0.26) 13 (0.55) 6 (0.26) 151 (6.45)1994 1 910 (84.89) 151 (6.71) 55 (2.44) 4 (0.18) 12 (0.53) 4 (0.18) 114 (5.07)1995 1 965 (85.18) 168 (7.28) 44 (1.91) 12 (0.52) 12 (0.52) 3 (0.13) 103 (4.46)1996 2 389 (84.93) 233 (8.28) 69 (2.45) 6 (0.22) 13 (0.46) 4 (0.14) 99 (3.52)1997 2 294 (83.57) 234 (8.53) 62 (2.26) 16 (0.58) 10 (0.36) 4 (0.15) 125 (4.55)1998 2 373 (82.91) 236 (8.25) 83 (2.9) 21 (0.73) 8 (0.28) 8 (0.28) 133 (4.65)1999 2 254 (81.31) 277 (9.99) 64 (2.31) 19 (0.68) 11 (0.4) 6 (0.22) 141 (5.09)2000 2 260 (81.56) 279 (10.07) 64 (2.31) 24 (0.86) 15 (0.54) 3 (0.11) 126 (4.55)2001 1 938 (78.94) 299 (12.18) 52 (2.12) 20 (0.82) 17 (0.69) 3 (0.12) 126 (5.13)2002 1 651 (77.73) 268 (12.62) 55 (2.59) 23 (1.08) 21 (0.99) 9 (0.42) 97 (4.57)2003 1 574 (78.7) 242 (12.1) 62 (3.1) 20 (1) 12 (0.6) 7 (0.35) 83 (4.15)2004 1 766 (77.19) 289 (12.63) 67 (2.93) 46 (2.01) 14 (0.61) 8 (0.35) 98 (4.28)2005 1 525 (77.29) 253 (12.82) 77 (3.9) 16 (0.81) 21 (1.07) 10 (0.51) 71 (3.6)Total 29 557 (81.83) 3 447 (9.54) 906 (2.51) 247 (0.68) 198 (0.55) 85 (0.23) 1 682 (4.66)
Note: Data are shown as n (%) per year by different pathological classifications during the years 1991–2005.
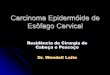
diagnosed with SCC. For SCC, occurrence peaked in1991–1995 in patients 50–59 years of age (Figure 1A). From1996 to 2005, it peaked in patients 40–49 years of age. Thelowest occurrence across all time periods was in patients20–29 years of age. Despite a slight downward trend in occur-rence in patients 60–69 years of age, the incidence in patients70 years or older steadily increased from 1991 to 2005.
For cervical adenocarcinoma, occurrence peaked in pa-tients 40–49 years of age, with a steady increase in this agegroup from 1991 to 2005 (Figure 1B). As for SCC, theyoungest patients (20–29 years of age) also had the lowestrate of cervical adenocarcinoma. In fact, the occurrence ofcervical adenocarcinoma decreased slightly among patients20–29, 30–39 and 60–69 years of age. From 1991 to 2005,the occurrence increased in those 70 years or older. Unlikethe trends noted for SCC and adenocarcinoma, occurrenceof small cell cervical carcinoma peaked in the period from1991–1995 in patients 30–39 years of age (Figure 1C); how-ever, this patient percentage dramatically declined between1996 and 2000, then slightly increased again between 2001and 2005. In opposition to this trend, the occurrence of smallcell cervical carcinoma increased in patients 40–49 years ofage between 1996 and 2000, and this age category remainedthe most prominent between 2001 and 2005. As with othertypes of cervical cancers, occurrence was lowest in patients20–29 years of age. Occurrence trends were variable in theremaining age categories, but generally trended upward be-tween 1991 and 2005.
For the time periods 1991–1995, 1996–2000 and2001–2005, the mean age at diagnosis of cervical cancer
steadily increased from 53.9±13.3 to 55.0±14.9 and thento 56.7±14.7 years, respectively. Table 2 summarizes themean age at diagnosis for all cervical cancer types overtime. ANOVA showed significant differences in the overallmean age of patients at diagnosis by type of cervical cancer(F=93.64, p<0.001). Tukey’s post hoc multiple comparisontests indicated a significantly younger mean age at diagnosisfor those with small cell cervical carcinoma (50.7±15.7 years)compared with those with squamous (55.6±13.9 years) orpapillary carcinoma (61.7±14.6 years). Within-group testsconfirmed these differences (p<0.001 for each cancer type).
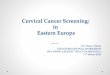
To examine trends over time of the incidence of cervi-cal SCC, adenocarcinoma and small cell carcinoma in Tai-wan, incidence data were plotted across time as scatter plots(Figure 2A–C). Linear regression analysis showed that theincidence of SCC decreased from 1991 to 2005 (Figure 2A;r2=0.67, p<0.001). During the same period, non-significantincreases of adenocarcinoma (Figure 2B; r2=0.11, p=0.23)and small cell carcinoma (Figure 2C; r2=0.15, p=0.16) werenoted.
Patient age at diagnosis has been reported to be a signifi-cant predictor of cervical cancer patient survival in developedWestern nations (16). During the 15 years of the study, theoverall mortality rate of the 198 patients with small cell cervi-cal carcinoma was 65.7%. When stratified by age, the highestmortality rate occurred in patients ≥70 years of age (82.8%).For the patients <70 years of age, the highest mortality rateoccurred in patients 40–49 years of age (71.0%). When ad-justed for varied lengths of follow-up, the overall mortalityrate was 18.1 per 100 person-years. Stratified by age, the
1344C© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349

C.-Y. Huang et al. Cervical carcinoma in Taiwan
Figure 1. Trend of diagnostic age-specific proportions of cervical squamous cell carcinoma (A), cervical adenocarcinoma (B) and cervical small cellcarcinoma (C) per five years in Taiwan, 1991–2005.
highest mortality rate occurred in patients ≥70 years of age(27.4 per 100 person- years). For the patients<70 years of age,the highest mortality rate occurred in patients 40–49 years ofage (20.9 per 100 person- years).
When 15 year survival from diagnosis was evaluated usingKaplan–Meier curves, patients 20–29 years of age at diagnosishad the highest survival rate (44%) (Figure 3). In contrast,patients 40–49 years of age at diagnosis had the lowest survivalrate. Notably, patients 70 years of age or more at diagnosisshowed an abrupt drop in survival after 7 years, and nonesurvived longer than 10 years. When a log-rank test was per-formed to compare survival rates of patients with small cellcervical carcinoma across ages, there was no significant cor-relation of age strata with survival rates (Figure 3; p=0.720).
Discussion
In this population-based study of cervical cancer in Taiwanfrom 1991 to 2005, the occurrence of most types of cervi-cal cancers, including SCC and small cell carcinoma, washighest in women 40–49 years of age and lowest in those
20–29 years of age. Significant differences in mean age of di-agnosis were found between the study periods and betweencancer types. The incidence of adenocarcinoma and smallcell cervical carcinoma tended to increase, but the incidenceof SCC significantly decreased from 1990 to 2005.
Taiwan has been successful in reducing the burden ofdisease from cervical cancer through an aggressive na-tional screening program. The incidence of invasive cancersdropped by 48% during the period from 1995 to 2006, with53.4% of women ≥30 years of age receiving at least one Paptest every three years (15). This finding is similar to decreasesof cervical cancer reported in Asia as a whole, Nordic coun-tries, Europe and the USA (1–8,20).
While screening has been effective in reducing the inci-dence and mortality from SCC of the cervix, the impact onadenocarcinoma of the cervix is less clear (3,9,10). While theincidence rates of adenocarcinoma increased in many Nordicand European countries, the USA and Canada up to themid-1990s, stable or declining trends have been noted (3,9).Possible reasons for the decrease include improved specimen
C© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349 1345

Cervical carcinoma in Taiwan C.-Y. Huang et al.
Tab
le2.
Tren
dof
mea
nag
eat
diag
nosi
sof
cerv
ical
carc
inom
apa
tient
spe
rfiv
eye
ars
inTa
iwan
bydi
ffer
ent
path
olog
ical
clas
sific
atio
ns,1
991–
2005
.
Squa
mou
sce
llA
deno
carc
inom
aA
deno
squa
mou
sPa
pilla
rySm
allc
ell
Cle
arce
llO
ther
sYe
arn
Mea
n(S
D)
nM
ean
(SD
)n
Mea
n(S
D)
nM
ean
(SD
)n
Mea
n(S
D)
nM
ean
(SD
)n
Mea
n(S
D)
p-Va
lue
1991
–199
59
533
54.2
(13.
2)83
750
.7(1
2.5)
251
50.9
(11.
7)36
57.3
(17.
1)56
47.4
(14.
9)23
49.2
(14.
3)58
352
.4(1
4.1)
<0.
001∗
1996
–200
011
570
55.5
(13.
8)†
125
950
.4(1
2.3)
342
50.1
(11.
7)86
62.1
(13.
9)†
5752
.1(1
5.7)
†25
54.6
(13.
9)†
624
53.3
(15.
4)<
0.00
1∗
2001
–200
58
454
57.5
(14.
6)†‡
135
151
.5(1
2.7)
†‡31
350
.3(1
1.7)
†12
562
.7(1
4.2)
†85
51.9
(16.
1)†
3751
.3(1
6.9)
†47
555
.8(1
5.8)
†‡<
0.00
1∗
Tota
l29
557
55.6
(13.
9)3
447
50.9
(12.
5)90
650
.4(1
1.7)
247
61.7
(14.
6)19
850
.7(1
5.7)
8551
.7(1
5.4)
168
253
.7(1
5.1)
–
Not
e:D
ata
are
expr
esse
das
num
ber
(n)a
ndm
ean
(SD
)by
diff
eren
tpa
thol
ogic
alcl
assi
ficat
ions
thro
ugh
aon
e-w
ayA
NO
VAw
itha
post
hoc
test
and
Tuke
y’s
test
for
mul
tiple
com
paris
ons.
∗ p<
0.05
,sig
nific
ant
com
paris
onof
age
amon
gdi
ffer
ent
path
olog
ical
clas
sific
atio
ns.
†p<
0.01
67(0
.05/
3),i
ndic
ated
for
the
sign
ifica
ntre
sult
asco
mpa
ring
with
year
1991
–199
5.‡p
<0.
0167
(0.0
5/3)
,ind
icat
edfo
rth
esi
gnifi
cant
resu
ltas
com
parin
gw
ithye
ar19
96–2
000.
P<0.
0167
(0.0
5/3)
,th
ead
just
sign
ifica
nce
cons
ider
edfo
rth
epo
st-h
ocm
ultip
leco
mpa
rison
,m
ean
age
wer
eco
mpa
red
for
thre
etim
esof
com
paris
ons,
year
1991
–199
5vs
.ye
ar19
96–2
000,
year
1991
–199
5vs
.yea
r20
01–2
005,
and
year
1996
–200
0vs
.yea
r20
01–2
005.
collection, increased recognition of adenocarcinoma precur-sors by histopathologists, and awareness of and testing forhuman papilloma virus infection (3,20,21,22,23).
With the drop in the incidence of cervical cancer, the ageat diagnosis has also decreased, with more than 60% of pa-tients diagnosed with cervical cancer surviving more thanfive years (24). However, despite national funding for cervi-cal cancer screening in Taiwan, cervical carcinoma remains amajor health issue (13,15). Histological subtypes of cervicalcancer carry different mortality risks, which may vary withage. In particular, small cell cervical carcinoma is associatedwith poorer prognosis and higher mortality than most othercancer types (17). Among the rarer forms of cervical cancer,clear cell carcinoma is unique in its association with a poorprognosis owing to its frequent presentation with metastasisand limited treatment options (25).
In our study, the occurrence of small cell cervical carci-noma peaked in the period from 1991 to 1995 in patients30–39 years of age. In contrast, the occurrence of small cellcervical carcinoma increased in patients 40–49 years old be-tween 1996 and 2000 and remained prominent in this agecategory between 2001 and 2005, similar to the trend of SCC.As with other types of cervical cancers, occurrence was lowestin patients 20–29 years old. These data are in line with otherstudies reporting a mean patient age at small cell cervicalcarcinoma diagnosis of 42–47 years (17).
Small cell cervical carcinoma is the least reported of thenon-SCCs of the cervix, most probably owing to its infre-quency and to variability in diagnostic classification. It ac-counts for <1% of all cervical cancers (17). This disease wasrecently reported to be associated with a significantly lower10 year overall survival compared with other types of cervi-cal tumors in a US population (16). Indeed, most patientswith International Federation of Gynecology and Obstetricsstage IIB or higher small cell carcinoma survive 36monthsor less (17). Its aggression may be related to the propen-sity of small cell carcinoma to undergo early lymphatic andhematogenous metastases (17,26). Indeed, we recently foundoverall survival to be closely associated with InternationalFederation of Gynecology and Obstetrics stage and lymphnode metastasis (27).
The mean age at diagnosis was significantly lower for smallcell cervical carcinoma than for SCC or papillary carcinoma.Linear regression analysis showed that the incidence of ade-nocarcinoma and small cell cervical carcinoma increased overtime, but not to a statistically significant degree. By contrast,SCC decreased significantly from 1991 to 2005 (Figure 2A;r2=0.67, p<0.001), which raised the intriguing issue thatyounger women might be at increased risk for small cell cer-vical carcinoma. Further analysis of this subtype is thereforewarranted.
Interestingly, a relatively large proportion of elderly pa-tients (60–69 years old and 70 years or older) were diagnosed
1346C© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349

C.-Y. Huang et al. Cervical carcinoma in Taiwan
Figure 2. Trend of age-adjusted incidence of cervical squamous cell carcinoma (A), cervical adenocarcinoma (B) and cervical small cell carcinoma(C) by year in Taiwan, 1991–2005. The linear regressions are as follows: r2=0.67 and p<0.001 (A); r2=0.11 and p=0.23 (B); and r2=0.11 andp=0.23 (C).
with small cell cervical carcinoma, as well as other types ofcervical cancer (Figure 1). Those with small cell cervical car-cinoma also had lower survival rates than younger womenthroughout the study period (Figure 3); however, the numberwas too small to show statistical variation. At the beginningof the Pap smear program, few Taiwanese women were mo-tivated to be examined. The percentage of those ≥30 years ofage being screened has steadily increased, except for a reduc-tion in 2003 that was possibly related to an outbreak of severeacute respiratory syndrome (15). These results indicate thatcervical cancer screening is likely to be important in olderpopulations (28).
Specific recommendations based on the results of this studyinclude the promotion of community health programs to in-crease the screening rate, that women older than 30 yearsof age should receive Pap smears yearly and that HPV test-ing should be combined with Pap smear screening, with thegovernment subsidizing the cost of both tests.
The study had several limitations. The challenges of usingpopulation-based data, the national registry, did not allow
for analysis of such factors as tumor stage, the presence ofmetastases, surgical margins or other pathological data. Oursurvival analyses were also not adjusted to control for factorssuch as patient age, tumor stage or other types of treatments,such as chemotherapy. Other factors, such as the impact ofage on reproductive hormones, reproductive behavior andlifestyle choices, such as cigarette smoking (16,18) and sexualbehavior, may also have impacted the results. Varying diag-nostic classifications were employed throughout the studyperiod. There is a potential bias from the population-basedcancer registry, with an estimated 80% of all cancer cases inTaiwan.
Conclusions
In this population-based study of small cell cervical cancerin Taiwan from 1991 to 2005, the occurrence increased andremained the most prominent in patients 40–49 years of agebetween 1996 and 2005. As with other types of cervical can-cers, occurrence was lowest in patients 20–29 years of age. Our
C© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349 1347

Cervical carcinoma in Taiwan C.-Y. Huang et al.
Figure 3. Fifteen-year age-specific survivaland overall survival curve of small cellcervical carcinoma in Taiwan, 1991–2005.
study indicated a significantly younger mean age at diagnosisfor small cell cervical carcinoma compared with squamouscell or papillary carcinoma. In Taiwan, the incidence of smallcell cervical carcinoma and adenocarcinoma tended to in-crease, but the incidence of squamous cell cervical carcinomasignificantly decreased during the time period from 1991 to2005. Age at diagnosis had an effect on survival in small cellcervical carcinoma patients in Taiwan. The 15 year survivalrate after diagnosis of small cell carcinoma was highest forpatients 20–29 years old and poor for patients 70 years of ageor more.
Funding
No specific funding.
References
1. Bray F, Loos AH, McCarron P, Weiderpass E, Arbyn M,
Møller H, et al. Trends in cervical squamous cell carcinoma
incidence in 13 European countries: changing risk and the
effects of screening. Cancer Epidemiol Biomarkers Prev.
2005;14:677–86.
2. Sasieni P, Castanon A, Cuzick J. Effectiveness of cervical
screening with age: population based case-control study of
prospectively recorded data. BMJ. 2009;339:b2968.
3. Mathew A, George PS. Trends in incidence and mortality
rates of squamous cell carcinoma and adenocarcinoma of
cervix – worldwide. Asian Pac J Cancer Prev. 2009;10:645–50.
4. Klint A, Tryggvadottir L, Bray F, Gislum M, Hakulinen T,
Storm HH, et al. Trends in the survival of patients diagnosed
with cancer in female genital organs in the Nordic countries
1964–2003 followed up to the end of 2006. Acta Oncol.
2010;49:632–43.
5. Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML,
Klint A, et al. NORDCAN: Cancer incidence, Mortality and
prevalence in the Nordic Countries, Version 3.3. Association
of Nordic Cancer registries. Danish Cancer Society. 2008.
Available online at: www.ancr.nu (accessed March 19, 2011).
6. Gunnell AS, Ylitalo N, Sandin S, Sparen P, Adami HO,
Ripatti S. A longitudinal Swedish study on screening for
squamous cell carcinoma and adenocarcinoma: evidence of
effectiveness and overtreatment. Cancer Epidemiol
Biomarkers Prev. 2007;16:2641–8.
7. American Cancer Society. Cancer prevention & early
detection: Facts & Figures 2009. Atlanta, GA: American
Cancer Society, 2009.
1348C© 2011 The Authors
Acta Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349

C.-Y. Huang et al. Cervical carcinoma in Taiwan
8. Anttila A, Ronco G, Clifford G, Bray F, Hakama M, Arbyn M,
et al. Cervical cancer screening programs and policies in 18
European countries. Br J Cancer. 2004;91:935–41.
9. Bray F, Carstensen B, Moller H, Zappa M, Zakelj MP,
Lawrence G, et al. Incidence trends of adenocarcinoma of the
cervix in 13 European countries. Cancer Epidemiol
Biomarkers Prev. 2005;14:2191–9.
10. Sasieni P, Castanon A, Cuzick J. Screening and
adenocarcinoma of the cervix. Int J Cancer. 2009;125:525–9.
11. Arbyn M, Antoine J, Valerianova Z, Magi M, Stengrevics A,
Smailyte G, et al. Trends in cervical cancer incidence and
mortality in Bulgaria, Estonia, Latvia, Lithuania and
Romania. Tumori. 2010;96:517–23.
12. Department of Health. Public health report 2003. Taipei:
Department of Health, Executive Yuan, 2003.
13. Liao CC, Wang HY, Lin RS, Hsieh CY, Sung FC. Addressing
Taiwan’s high incidence of cervical cancer: factors associated
with the Nation’s low compliance with Papanicolaou
screening in Taiwan. Public Health. 2006;120:1170–6.
14. Wen CP, Tsai SP, Chung WS. A 10-year experience with
universal health insurance in Taiwan: measuring changes in
health and health disparity. Ann Intern Med.
2008;148:258–67.
15. Chen YY, You SL, Chen CA, Shih LY, Koong SL, Chao KY,
et al. Taiwan Cervical Cancer Screening Task Force:
Effectiveness of national cervical cancer screening
programme in Taiwan: 12-year experiences. Br J Cancer.
2009;101:174–7.
16. Vinh-Hung V, Bourgain C, Vlastos G, Cserni G, De Ridder
M, Storme G, et al. Prognostic value of histopathology and
trends in cervical cancer: a SEER population study. BMC
Cancer. 2007;7:164.
17. Chen J, Macdonald OK, Gaffney DK. Incidence, mortality,
and prognostic factors of small cell carcinoma of the cervix.
Obstet Gynecol. 2008;111:1394–402.
18. International Collaboration of Epidemiological Studies of
Cervical Cancer, Appleby P, Beral V, Berrington de Gonzalez
A, Colin D, Franceschi S et al. Carcinoma of the cervix and
tobacco smoking: collaborative reanalysis of individual data
on 13,541 women with carcinoma of the cervix from 23
epidemiological studies. Int J Cancer. 2006;118:1481–95.
19. Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB, eds.
Cancer incidence in five continents, vol. III. Lyon, France:
IARC Scientific Publications, 2002.
20. Qiu D, Marugame T. Comparison of time trends in uterine
cancer incidence (1973–1997) in East Asia, Europe and USA,
from Cancer Incidence in Five Continents, Vols IV–VIII. Jpn J
Clin Oncol. 2007;37:722–4.
21. Sigurdsson K. Cervical cancer: cytological cervical screening
in Iceland and implications of HPV vaccines. Cytopathology.
2010;21:213–22.
22. Kjaer SK. Human papillomavirus (HPV) infection, cervical
cancer and vaccination against HPV: a Nordic perspective.
Acta Obstet Gynecol Scand. 2007;86:1286–9.
23. Sigurdsson K, Sigvaldason H, Gudmundsdottir T, Sigurdsson
R, Briem H. The efficacy of HPV 16/18 vaccines on sexually
active 18–23 year old women and the impact of HPV
vaccination on organized cervical cancer screening. Acta
Obstet Gynecol Scand. 2009;88:27–35.
24. Maher EJ, Denton A. Survivorship, late effects and cancer of
the cervix. Clin Oncol (R Coll Radiol). 2008;20:479–87.
25. Thomas MB, Wright JD, Leiser AL, Chi DS, Mutch DG,
Podratz KC, et al. Clear cell carcinoma of the cervix: a
multi-institutional review in the post-DES era. Gynecol
Oncol. 2008;109:335–9.
26. Chang TC, Lia CH, Tseng, Hsueh S, Huang KG, Chou HH.
Prognostic factors in surgically treated small cell carcinoma
followed by adjuvant chemotherapy. Cancer. 1998;83:
712–8.
27. Huang CY, Chen YL, Chu TC, Cheng WF, Hsieh CY, Lin
MC. Prognostic factors in women with early stage small cell
carcinoma of the uterine cervix. Oncol Res. 2009;18:279–86.
28. Walter LC, Covinsky LE. Cancer screening in elderly patients.
JAMA. 2001;285:2750–6.
C© 2011 The AuthorsActa Obstetricia et Gynecologica Scandinavica C© 2011 Nordic Federation of Societies of Obstetrics and Gynecology 90 (2011) 1342–1349 1349