Embed Size (px)
Citation preview

Ctt
1
SCIENTIFIC ARTICLE
Incidence of Clinically Diagnosed and Surgically
Treated Carpal Tunnel Syndrome in Korea
Young Hak Roh, MD, Moon Sang Chung, MD, PhD, Goo Hyun Baek, MD, PhD, Young Ho Lee, MD, PhD,Seung Hwan Rhee, MD, Hyun Sik Gong, MD, PhD
Purpose Most epidemiologic studies on carpal tunnel syndrome (CTS) have been performedon specific regional or occupational groups, or on general populations in the West. Theauthors undertook to determine the incidence of clinically diagnosed and surgically treatedCTS in the Korean general population.
Methods A retrospective, nationwide cohort study was performed using data collected from2005 to 2007 (inclusive) by the Korean Health Insurance Review Agency, which covers 97%of the population. We analyzed the incidence of clinically diagnosed, electrophysiologicallydiagnosed, and surgically treated CTS in patients aged over 20 years, and the influences ofgender and age on incidence.
Results The incidence of total clinically diagnosed CTS and electrophysiologically diagnosedCTS in patients over 20 years of age was 4.96 and 0.98 per 1,000 person-years, respectively.The incidence of surgically treated CTS was 0.29 per 1,000 person-years. The age-adjustedfemale to male incidence ratio of diagnosed CTS was 2.58 (95% confidence interval,2.56–2.59) and that of surgically treated CTS was 5.82 (95% CI, 5.64–6.00). Women aged50 to 59 years had the highest incidence of CTS (18.11 per 1,000 person-years), whereas menshowed a slow increase in incidence with age, highest at 60 to 69 years.
Conclusions Compared with Western studies, our study of the Korean population shows a similarincidence of CTS but a lower incidence of surgery. Korean women with CTS are more likely tobe treated surgically than men. Further studies may be warranted to identify ethnic, gender, andsocioeconomic factors that influence surgical treatment rates. (J Hand Surg 2010;35A:1410–1417.Copyright © 2010 by the American Society for Surgery of the Hand. All rights reserved.)
Key words Carpal tunnel syndrome, epidemiology, incidence, Korean.
eKhdtantouew
h
ARPAL TUNNEL SYNDROME (CTS) is the mostcommon compressive peripheral neuropathy inthe upper extremity and is characterized by a
ingling sensation and pain over the median nerve dis-ribution, or by weakness of the thenar muscles. The
From the Department of Orthopaedic Surgery, Seoul National University College of Medicine and Na-tional Police Hospital, Seoul, Korea.
Received for publication February 8, 2010; accepted in revised form May 25, 2010.
No benefits in any form have been received or will be received related directly or indirectly to thesubject of this article.
Corresponding author: Hyun Sik Gong, MD, PhD, Department of Orthopaedic Surgery, SeoulNational University Bundang Hospital, Seoul National University College of Medicine, 300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do, 463-707, Korea; e-mail: [email protected].
0363-5023/10/35A09-0002$36.00/0
pdoi:10.1016/j.jhsa.2010.05.020
410 � © ASSH � Published by Elsevier, Inc. All rights reserved.
stimated prevalence of CTS in adults in the Unitedingdom is 7% to 16%, and the number of electiveand surgeries for CTS has almost doubled over theecade from 1990 to 2000.1,2 CTS patients surgicallyreated in the United States number between 400,000nd 500,000 per year and the associated annual eco-omic cost is in excess of $2 billion.3,4 Many studies onhe epidemiology of CTS are from specific regional5–7
r occupational groups,8–10 and studies of general pop-lations have been performed in the West,11–16 but thepidemiology of CTS in Asian countries has not beenell described.Previous studies in Western general populations
ave reported incidences as low as 1.04 per 1,000
erson-years in East Kent (United Kingdom) to as high
INCIDENCE OF CTS IN KOREA 1411
as 3.76 per 1,000 person-years reported in OlmstedCounty (United States).5,12–16 Such differences in theincidence of CTS may be due to different study designs,diagnostic criteria, and true differences in incidenceresulting from different exposures to risk factors. Fur-thermore, ethnic factors and socioeconomic status mayaffect the incidence of CTS.17–20 The purpose of thisstudy was to determine the incidence of clinically di-agnosed and surgically treated CTS in adult Koreans,using data from the Korean Health Insurance ReviewAgency (HIRA), which includes 97% of the population.
MATERIALS AND METHODS
Study setting
We performed a retrospective, nationwide cohort studybased on data collected during a 36-month period fromJanuary 2005 to December 2007 by the Korean HIRA.In Korea, most citizens are enrolled in the Koreannational health insurance program, and all health careproviders submit patient data, including diagnoses andmedical costs, to HIRA to obtain reimbursement of70% of the total medical costs from the government.About 97% of the Korean population is covered by thissystem; the remaining 3% are either covered by a Med-ical Aid Program or are temporary or illegal residents.Therefore, almost all information about patients anddiseases is available from the HIRA database. When aclinic or hospital submits patient data to claim reim-bursement, the Health Care Review and EvaluationCommittee, which is affiliated with HIRA and is com-posed of 630 doctors and other medical specialists,reviews individual patient records to determine whetherthe reimbursement claimed is clinically valid andwhether unnecessary medical services were provided.By doing so, the Health Care Review and EvaluationCommittee aims to maintain the quality of health careand prevent unnecessary or inappropriate use of medi-cal resources. The HIRA database has been used forother epidemiological studies.21,22 For the presentstudy, we used the HIRA database to determine theincidence of diagnosed CTS and of surgically treatedCTS in the Korean general population. Estimates of theKorean general population and in the standardizedworld population were obtained from the Korean Sta-tistical Information Service23 and World Health Orga-nization Statistical Information System.24
Diagnosis of CTS
A diagnosis of CTS is based on symptoms of mediannerve compression, the findings of specific physical
examinations such as Tinel’s sign or Phalen’s test, andJHS �Vol A, Sep
neurophysiologic testing. However, no standardized di-agnostic criteria have been established for CTS, and noconsensus has been reached as to whether CTS is aclinical or an electrophysiologic diagnosis.25 The defi-nition of CTS has varied in the literature according tothe purpose of the study, the available size of the targetgroup, and differences in regional medical service sys-tems.14,15,26 Electrophysiological testing was used asthe reference standard diagnostic tool in some litera-ture,6,14 but this procedure is costly, time consuming,and uncomfortable, and it has been reported to have13% false-negative27 and 18% false-positive rates.11
Additionally, objective confirmation of CTS by thismethod can often be elusive.28 Thus, the method maynot be used routinely in actual medical practice.15,29 Forthe national health system in Korea, confirmatory diag-nosis with electrodiagnostic tests is not necessary be-fore a surgeon can perform carpal tunnel surgery. Ac-cordingly, we tried to estimate both the incidence ofclinically diagnosed CTS by practicing physicians andthat of CTS diagnosed with electrophysiological test-ing; the diagnoses were reviewed and confirmed byHealth Care Review and Evaluation Committeeexperts.
Data obtained from HIRA
The HIRA database uses the diagnostic codes detailedin the International Classification of Diseases (ICD-10code), which differentiate peripheral neuropathies byinvolved nerves and causative factors. The block G56of the ICD-10 classification concerns mononeuropa-thies of the upper limb and is subdivided into codesG56.0 to G56.9. In the present study, we used ICD codeG56.0, which directly addresses CTS. The cases of CTSdiagnosed with electrophysiological testing are ob-tained by using the medical care fee code for electro-physiological testing of the upper extremity and theG56.0 diagnostic code. In cases of surgically treatedCTS, we used a HIRA surgery fee code for carpaltunnel release, and the G56.0 diagnostic code.
We requested data on the number of patients newlydiagnosed as having CTS, the number of electrophysi-ological tests for diagnosed CTS, and the number ofsurgical treatments for CTS conducted from January2005 to December 2007 (inclusive) by age and gender.More recent data were unavailable at the time this studywas begun. We prevented double recording, such asstaged bilateral carpal tunnel surgery, by including onlyone patient record when a patient had more than one inthe HIRA database. Because the HIRA counts patientsmonthly, we could not obtain data on CTS patients who
had both electrophysiological testing and surgery be-tember

1412 INCIDENCE OF CTS IN KOREA
cause only those who had both in the same monthwould be counted. The age categories used were 20 to29, 30 to 39, 40 to 49, 50 to 59, 60 to 69, and 70 orgreater.
Data analysis
The incidence of CTS is described as the incidence rateby using the denominator of person-years, which isdefined as the product of the number of years times thenumber of members of a population who have beenaffected by a certain condition, or the total sum of thenumber of years that each member of a study popula-tion has been under observation. For example, if apopulation initially contains 1,000 nondiseased personsand 30 develop a condition over 2 years of observation,the incidence proportion is 30 cases per 1,000 per-sons—that is, 3%—but the incidence rate is 15 casesper 1,000 person-years, because the incidence propor-tion is divided by the number of years (in this example,2). We calculated 95% confidence intervals (CIs) forincidence rates and incidence rate ratios assuming Pois-son’s distribution. Generally, if confidence intervals donot overlap, the statistics will be statistically significant,and if the incidence rate ratio does not include the valueof 1, the difference is statistically significant. Trendanalysis for incidence of CTS was performed using thechi-square test for trend analysis with Cochran’s andMantel-Haenszel statistics. Statistical significance wasaccepted for p values of less than .05.
RESULTS
Overall incidence of CTS
The number of adults over 20 years of age in Koreawas 35,760,423 in 2005, 36,159,143 in 2006, and36,525,248 in 2007; during these years, a total of164,230, 176,948, and 197,533 cases of CTS were
TABLE 1. Incidence of CTS in Korean General Pop
Year
TotalPopulation
(n)Population
Aged �20 y (n)Diagnosed
CTS (n)
CTS
ElectropTes
2005 48,138,077 35,760,423 164,230 32,080
2006 48,297,184 36,159,143 176,948 35,889
2007 48,456,369 36,525,248 197,533 38,823
*Per 1,000 person-years.†Ratio of electrophysiological testing in diagnosed CTS patients.
documented, respectively; 32,080, 35,889, and 38,823,
JHS �Vol A, Sep
respectively, of these patients were diagnosed withelectrophysiological testing, and, 9,225, 10,458, and11,466, respectively, of diagnosed CTS patients weretreated surgically according to the HIRA database(Table 1). The overall incidence of diagnosed CTSwas 4.96 per 1,000 person-years (95% CI, 4.94–4.98) and that of electrophysiologically diagnosedCTS was 0.98 per 1,000 person-years (95% CI,0.98–0.99). The overall incidence of surgicallytreated CTS was 0.29 per 1,000 person-years (95%CI, 0.28–0.30). The age-standardized incidence rateof total clinically diagnosed, electrophysiologicallydiagnosed, and surgically treated CTS using WorldStandard Population Distribution of the WorldHealth Organization Statistical Information Systemas reference data was 4.83, 0.95, and 0.28 per 1,000person-years, respectively. The proportion of surgeryin patients with overall clinically diagnosed CTS was5.8%.
Gender differences in incidence of CTS
Women had a diagnosed CTS incidence of 7.12 per1,000 person-years (95% CI, 7.11–7.13) and an elec-trophysiologically diagnosed CTS incidence of 1.38 per1,000 person-years (95% CI, 1.37–1.38). Men had adiagnosed CTS incidence of 2.76 per 1,000 person-years (95% CI, 2.74–2.78) and an electrophysiologi-cally diagnosed CTS incidence of 0.58 per 1,000 per-son-years (95% CI, 0.57–0.60). The age-adjustedfemale to male incidence ratio of overall diagnosedCTS and electrophysiologically diagnosed CTS was2.58 (95% CI, 2.56–2.59) (Table 2) and 2.37 (95% CI,2.34–2.40), respectively.
The incidence of surgically treated CTS was 0.08 per1,000 person-years (95% CI, 0.079–0.081) for men and0.49 per 1,000 person-years (95% CI, 0.487–0.493) forwomen. The percentage of patients diagnosed with CTS
ion
osed
ological(n)
SurgicallyTreatedCTS (n)
Annual Incidenceof Diagnosed
CTS*
Annual Incidenceof SurgicallyTreated CTS*
.5%)† 9,225 4.59 0.26
.3%)† 10,457 4.89 0.29
.7%)† 11,466 5.41 0.31
ulat
DiagnWithhysiting
(19
(20
(19
treated surgically was 2.9% for men and 6.9% for
tember
INCIDENCE OF CTS IN KOREA 1413
women, and the female to male ratio for surgicallytreated CTS was 5.82 (95% CI, 5.64–6.00) (Table 2).
Age differences in incidence of CTS
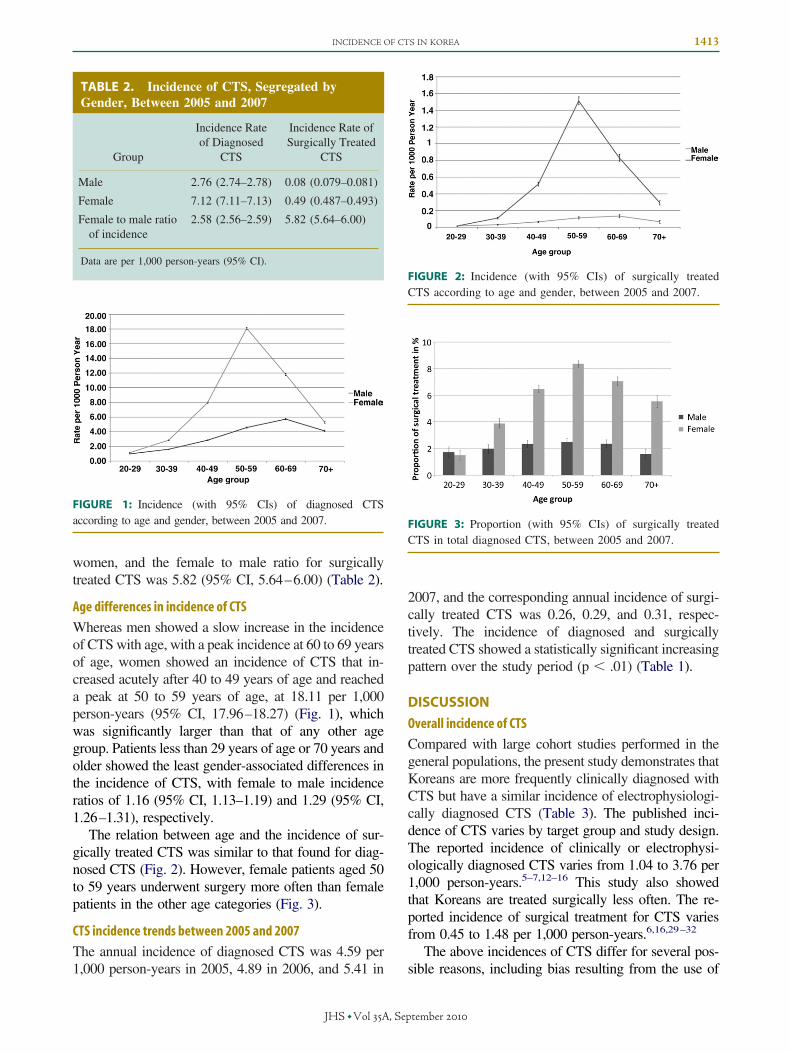
Whereas men showed a slow increase in the incidenceof CTS with age, with a peak incidence at 60 to 69 yearsof age, women showed an incidence of CTS that in-creased acutely after 40 to 49 years of age and reacheda peak at 50 to 59 years of age, at 18.11 per 1,000person-years (95% CI, 17.96–18.27) (Fig. 1), whichwas significantly larger than that of any other agegroup. Patients less than 29 years of age or 70 years andolder showed the least gender-associated differences inthe incidence of CTS, with female to male incidenceratios of 1.16 (95% CI, 1.13–1.19) and 1.29 (95% CI,1.26–1.31), respectively.
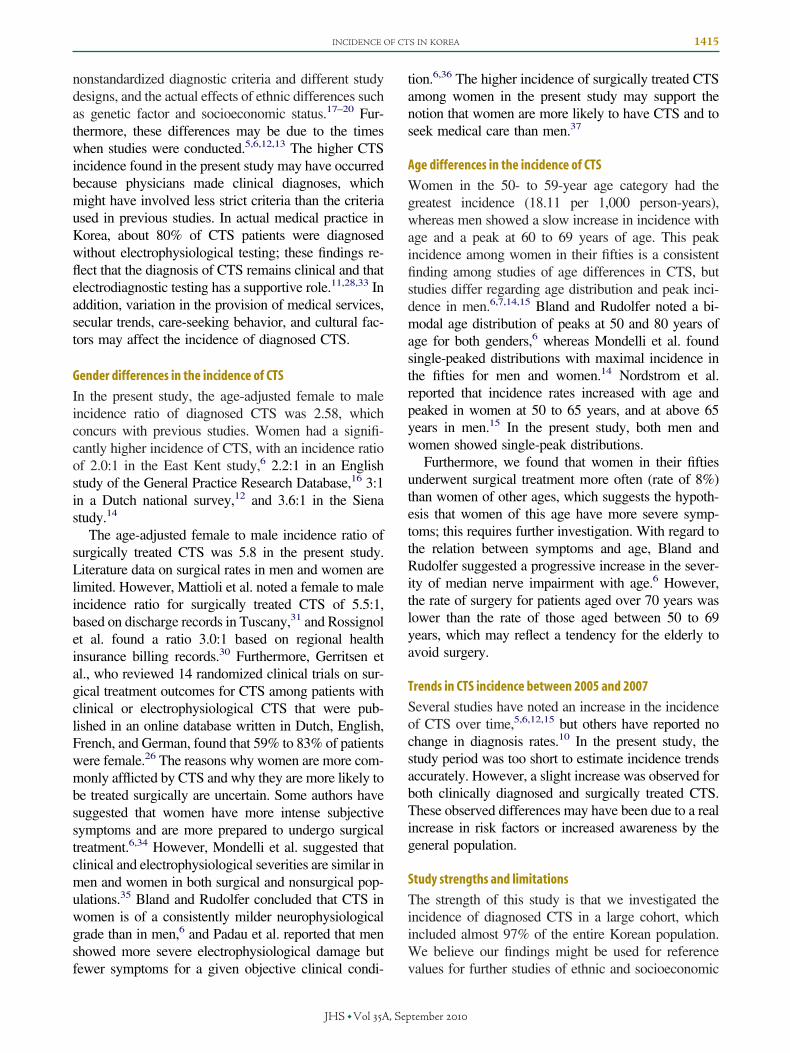
The relation between age and the incidence of sur-gically treated CTS was similar to that found for diag-nosed CTS (Fig. 2). However, female patients aged 50to 59 years underwent surgery more often than femalepatients in the other age categories (Fig. 3).
CTS incidence trends between 2005 and 2007
The annual incidence of diagnosed CTS was 4.59 per
TABLE 2. Incidence of CTS, Segregated byGender, Between 2005 and 2007
Group
Incidence Rateof Diagnosed
CTS
Incidence Rate ofSurgically Treated
CTS
Male 2.76 (2.74–2.78) 0.08 (0.079–0.081)
Female 7.12 (7.11–7.13) 0.49 (0.487–0.493)
Female to male ratioof incidence
2.58 (2.56–2.59) 5.82 (5.64–6.00)
Data are per 1,000 person-years (95% CI).
FIGURE 1: Incidence (with 95% CIs) of diagnosed CTSaccording to age and gender, between 2005 and 2007.
1,000 person-years in 2005, 4.89 in 2006, and 5.41 in
JHS �Vol A, Sep
2007, and the corresponding annual incidence of surgi-cally treated CTS was 0.26, 0.29, and 0.31, respec-tively. The incidence of diagnosed and surgicallytreated CTS showed a statistically significant increasingpattern over the study period (p � .01) (Table 1).
DISCUSSION
Overall incidence of CTS
Compared with large cohort studies performed in thegeneral populations, the present study demonstrates thatKoreans are more frequently clinically diagnosed withCTS but have a similar incidence of electrophysiologi-cally diagnosed CTS (Table 3). The published inci-dence of CTS varies by target group and study design.The reported incidence of clinically or electrophysi-ologically diagnosed CTS varies from 1.04 to 3.76 per1,000 person-years.5–7,12–16 This study also showedthat Koreans are treated surgically less often. The re-ported incidence of surgical treatment for CTS variesfrom 0.45 to 1.48 per 1,000 person-years.6,16,29–32
The above incidences of CTS differ for several pos-
FIGURE 2: Incidence (with 95% CIs) of surgically treatedCTS according to age and gender, between 2005 and 2007.
FIGURE 3: Proportion (with 95% CIs) of surgically treatedCTS in total diagnosed CTS, between 2005 and 2007.
sible reasons, including bias resulting from the use of
tember

TABLE 3. Comparison of Incidence of CTS Reported in the Literature†
Country (Study Author) Region/Time Period Type of Study Diagnostic Definition of CTSIncidence of Diagnosed
CTS*Incidence of Surgically
Treated CTS*
United States (Stevens et al.)5 Rochester, MN 1961–1980 Rochester Epidemiology program project Clinical or electrophysiological CTS(Diagnostic codes from database)
Overall: 1.051961–1965: 0.881976–1980: 1.25
N/A
United States (Hanrahan et al.)32 Wisconsin 1990–1993 Wisconsin occupational CTSsurveillance
(Surgical cases) N/A 1.48
United States (Nordstrom et al.)15 Marshfield 1991–1993 Wisconsin HMO database Clinical or electrophysiological CTS(Diagnostic codes and chartreview)
3.46 N/A
Denmark (Ebskov et al.)29 Whole population1993–1994
Mail survey to medical institute Clinical or electrophysiological CTS(Surgical cases)
N/A 0.61
Canada (Rossignol et al.)30 Montreal 1994–1995 Database of Quebec Health Insuranceplan (ages 20–65 y)
(Surgical cases) N/A 0.9
Italy (Mondelli et al.)14 Siena 1991–1998 Data from regional neurophysiologicalcenter
Electrophysiological CTS 3.29 (2.76‡) N/A
England (Latinovic et al.)16 Not specified 1992–2000 General practice research database (Diagnostic codes from database) 1.36‡ 0.27 (in men)0.62 (in women)
Italy (Mattioli et al.)7,31 Tuscany 1997–2000 Discharge records from all public andprivate hospitals (ages 20–59 y)
(Hospital discharge recorddatabase)
1.06‡ 0.46‡ (in men)2.55‡ (in women)
Netherland (Bongers et al.)12 Whole population 1987–2001
Dutch national survey of general practice Clinical or electrophysiological CTS 1987: 1.32001: 1.8
N/A
England (Bland and Rudolfer)6 East Kent and Huddersfield1991–2001
Data from regional neurophysiologicalcenter
Electrophysiological CTS 1.04 (estimated)1.39 (in women)0.67 (in men)
1991:0.52001:1.0 (estimated)
United States (Gelfman et al.)13 Olmsted County, MN1981–2005
Rochester Epidemiology program project Clinical or electrophysiological CTS(Diagnostic codes from database)
Overall: 3.761981–1985: 2.582000–2005: 4.24
1.09
Korea (current study) Whole population2005–2007
Database of Korean Health InsuranceReview Agency (aged �20 y)
Clinical or electrophysiological CTSElectrophysiological CTS
4.96 (4.83†) 0.29 (0.28†)0.98 (0.95†)
N/A, not available.*Per 1,000 person-years.†Age-standardized rates using World Health Organization World Standard Population.‡Age-standardized rates using World Health Organization European Standard Population.
1414
INCID
ENCEOFCTSIN
KOREA
JHS
�VolA
,September
INCIDENCE OF CTS IN KOREA 1415
nonstandardized diagnostic criteria and different studydesigns, and the actual effects of ethnic differences suchas genetic factor and socioeconomic status.17–20 Fur-thermore, these differences may be due to the timeswhen studies were conducted.5,6,12,13 The higher CTSincidence found in the present study may have occurredbecause physicians made clinical diagnoses, whichmight have involved less strict criteria than the criteriaused in previous studies. In actual medical practice inKorea, about 80% of CTS patients were diagnosedwithout electrophysiological testing; these findings re-flect that the diagnosis of CTS remains clinical and thatelectrodiagnostic testing has a supportive role.11,28,33 Inaddition, variation in the provision of medical services,secular trends, care-seeking behavior, and cultural fac-tors may affect the incidence of diagnosed CTS.
Gender differences in the incidence of CTS
In the present study, the age-adjusted female to maleincidence ratio of diagnosed CTS was 2.58, whichconcurs with previous studies. Women had a signifi-cantly higher incidence of CTS, with an incidence ratioof 2.0:1 in the East Kent study,6 2.2:1 in an Englishstudy of the General Practice Research Database,16 3:1in a Dutch national survey,12 and 3.6:1 in the Sienastudy.14
The age-adjusted female to male incidence ratio ofsurgically treated CTS was 5.8 in the present study.Literature data on surgical rates in men and women arelimited. However, Mattioli et al. noted a female to maleincidence ratio for surgically treated CTS of 5.5:1,based on discharge records in Tuscany,31 and Rossignolet al. found a ratio 3.0:1 based on regional healthinsurance billing records.30 Furthermore, Gerritsen etal., who reviewed 14 randomized clinical trials on sur-gical treatment outcomes for CTS among patients withclinical or electrophysiological CTS that were pub-lished in an online database written in Dutch, English,French, and German, found that 59% to 83% of patientswere female.26 The reasons why women are more com-monly afflicted by CTS and why they are more likely tobe treated surgically are uncertain. Some authors havesuggested that women have more intense subjectivesymptoms and are more prepared to undergo surgicaltreatment.6,34 However, Mondelli et al. suggested thatclinical and electrophysiological severities are similar inmen and women in both surgical and nonsurgical pop-ulations.35 Bland and Rudolfer concluded that CTS inwomen is of a consistently milder neurophysiologicalgrade than in men,6 and Padau et al. reported that menshowed more severe electrophysiological damage but
fewer symptoms for a given objective clinical condi-JHS �Vol A, Sep
tion.6,36 The higher incidence of surgically treated CTSamong women in the present study may support thenotion that women are more likely to have CTS and toseek medical care than men.37
Age differences in the incidence of CTS
Women in the 50- to 59-year age category had thegreatest incidence (18.11 per 1,000 person-years),whereas men showed a slow increase in incidence withage and a peak at 60 to 69 years of age. This peakincidence among women in their fifties is a consistentfinding among studies of age differences in CTS, butstudies differ regarding age distribution and peak inci-dence in men.6,7,14,15 Bland and Rudolfer noted a bi-modal age distribution of peaks at 50 and 80 years ofage for both genders,6 whereas Mondelli et al. foundsingle-peaked distributions with maximal incidence inthe fifties for men and women.14 Nordstrom et al.reported that incidence rates increased with age andpeaked in women at 50 to 65 years, and at above 65years in men.15 In the present study, both men andwomen showed single-peak distributions.
Furthermore, we found that women in their fiftiesunderwent surgical treatment more often (rate of 8%)than women of other ages, which suggests the hypoth-esis that women of this age have more severe symp-toms; this requires further investigation. With regard tothe relation between symptoms and age, Bland andRudolfer suggested a progressive increase in the sever-ity of median nerve impairment with age.6 However,the rate of surgery for patients aged over 70 years waslower than the rate of those aged between 50 to 69years, which may reflect a tendency for the elderly toavoid surgery.
Trends in CTS incidence between 2005 and 2007
Several studies have noted an increase in the incidenceof CTS over time,5,6,12,15 but others have reported nochange in diagnosis rates.10 In the present study, thestudy period was too short to estimate incidence trendsaccurately. However, a slight increase was observed forboth clinically diagnosed and surgically treated CTS.These observed differences may have been due to a realincrease in risk factors or increased awareness by thegeneral population.
Study strengths and limitations
The strength of this study is that we investigated theincidence of diagnosed CTS in a large cohort, whichincluded almost 97% of the entire Korean population.We believe our findings might be used for reference
values for further studies of ethnic and socioeconomictember

1416 INCIDENCE OF CTS IN KOREA
factors affecting the diagnosis and treatment of CTS.However, our study also had its limitations. First andmost important, the diagnosis of CTS was not standard-ized. Physicians used different criteria to diagnose CTS.Second, we did not have access to individual medicalrecords because the HIRA database does not providepersonal data such as occupation, body mass index, andcomorbidities. An analysis of these factors would haveshed light on the reasons for observed differences in theincidence of CTS. Third, we determined the incidenceof CTS by hospital-based cases (including inpatientsand outpatients). Hospital-based cases were selectedaccording to personal characteristics, severity of dis-ease, and associated health conditions.38 Finally, wecannot assume that equal numbers of subjects of diag-nosed and surgical cases will occur each year. Thewaiting period from diagnosis to surgery can be longand may result in different patient datasets of diagnosedand surgical cases.
This study determined the incidence of diagnosedand surgically treated CTS in the Korean general pop-ulation. Compared with Western studies, Koreans havea similar incidence of CTS but are treated surgicallyless often. Korean women with CTS are more likely tobe treated surgically than men. Further studies are war-ranted to identify ethnic, gender, and socioeconomicfactors that influence the incidence of surgical treatmentrates.
REFERENCES1. Wildin C, Dias JJ, Heras-Palou C, Bradley MJ, Burke FD. Trends in
elective hand surgery referrals from primary care. Ann R Coll SurgEngl 2006;88:543–546.
2. Ferry S, Pritchard T, Keenan J, Croft P, Silman AJ. Estimating theprevalence of delayed median nerve conduction in the general pop-ulation. Br J Rheumatol 1998;37:630–635.
3. Palmer DH, Hanrahan LP. Social and economic costs of carpaltunnel surgery. Instr Course Lect 1995;44:167–172.
4. Foley M, Silverstein B, Polissar N. The economic burden of carpaltunnel syndrome: long-term earnings of CTS claimants in Washing-ton State. Am J Ind Med 2007;50:155–172.
5. Stevens JC, Sun S, Beard CM, O’Fallon WM, Kurland LT. Carpaltunnel syndrome in Rochester, Minnesota, 1961 to 1980. Neurology1988;38:134–138.
6. Bland JD, Rudolfer SM. Clinical surveillance of carpal tunnel syn-drome in two areas of the United Kingdom, 1991–2001. J NeurolNeurosurg Psychiatry 2003;74:1674–1679.
7. Mattioli S, Baldasseroni A, Curti S, Cooke RM, Bena A, de GiacomiG, et al. Incidence rates of in-hospital carpal tunnel syndrome in thegeneral population and possible associations with marital status.BMC Public Health 2008;8:374.
8. Gorsche RG, Wiley JP, Renger RF, Brant RF, Gemer TY, SasyniukTM. Prevalence and incidence of carpal tunnel syndrome in a meatpacking plant. Occup Environ Med 1999;56:417–422.
9. Werner RA, Franzblau A, Gell N, Hartigan AG, Ebersole M, Arm-strong TJ. Incidence of carpal tunnel syndrome among automobile
assembly workers and assessment of risk factors. J Occup EnvironMed 2005;47:1044–1050.JHS �Vol A, Sep
10. Wolf JM, Mountcastle S, Owens BD. Incidence of carpal tunnelsyndrome in the US military population. Hand (N Y) 2009;4:289–293.
11. Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, RosenI. Prevalence of carpal tunnel syndrome in a general population.JAMA 1999;282:153–158.
12. Bongers FJ, Schellevis FG, van den Bosch WJ, van der Zee J. Carpaltunnel syndrome in general practice (1987 and 2001): incidence andthe role of occupational and non-occupational factors. Br J Gen Pract2007;57:36–39.
13. Gelfman R, Melton LJ III, Yawn BP, Wollan PC, Amadio PC,Stevens JC. Long-term trends in carpal tunnel syndrome. Neurology2009;72:33–41.
14. Mondelli M, Giannini F, Giacchi M. Carpal tunnel syndrome inci-dence in a general population. Neurology 2002;58:289–294.
15. Nordstrom DL, DeStefano F, Vierkant RA, Layde PM. Incidence ofdiagnosed carpal tunnel syndrome in a general population. Epide-miology 1998;9:342–345.
16. Latinovic R, Gulliford MC, Hughes RA. Incidence of commoncompressive neuropathies in primary care. J Neurol Neurosurg Psy-chiatry 2006;77:263–265.
17. Potocki L, Chen KS, Koeuth T, Killian J, Iannaccone ST, Shapira SK,et al. DNA rearrangements on both homologues of chromosome 17 ina mildly delayed individual with a family history of autosomal dominantcarpal tunnel syndrome. Am J Hum Genet 1999;64:471–478.
18. Hakim AJ, Cherkas L, El Zayat S, MacGregor AJ, Spector TD. Thegenetic contribution to carpal tunnel syndrome in women: a twinstudy. Arthritis Rheum 2002;47:275–279.
19. Elstner M, Bettecken T, Wasner M, Anneser F, Dichgans M, Me-itinger T, et al. Familial carpal tunnel syndrome: further evidence fora genetic contribution. Clin Genet 2006;69:179–182.
20. Tanaka S, Wild DK, Cameron LL, Freund E. Association of occu-pational and non-occupational risk factors with the prevalence ofself-reported carpal tunnel syndrome in a national survey of theworking population. Am J Ind Med 1997;32:550–556.
21. Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM. Fasting serumglucose level and cancer risk in Korean men and women. JAMA2005;293:194–202.
22. Lim S, Koo BK, Lee EJ, Park JH, Kim MH, Shin KH, et al.Incidence of hip fractures in Korea. J Bone Miner Metab 2008;26:400–405.
23. Korean Statistical Information Service. Available at: http://www.kosis.kr. Accessed October 5, 2009.
24. World Health Organization Statistical Information System (WHOSIS).Available at: http://www.who.int/whosis/en/. Accessed October 5, 2009.
25. Keith MW, Masear V, Chung KC, Maupin K, Andary M, AmadioPC, et al. American Academy of Orthopaedic Surgeons ClinicalPractice Guideline on diagnosis of carpal tunnel syndrome. J BoneJoint Surg 2009;91A:2478–2479.
26. Gerritsen AA, Uitdehaag BM, van Geldere D, Scholten RJ, de VetHC, Bouter LM. Systematic review of randomized clinical trials ofsurgical treatment for carpal tunnel syndrome. Br J Surg 2001;88:1285–1295.
27. Concannon MJ, Gainor B, Petroski GF, Puckett CL. The predictivevalue of electrodiagnostic studies in carpal tunnel syndrome. PlastReconstr Surg 1997;100:1452–1458.
28. Finsen V, Russwurm H. Neurophysiology not required beforesurgery for typical carpal tunnel syndrome. J Hand Surg 2001;26B:61– 64.
29. Ebskov LB, Boeckstyns ME, Sorensen AI. Operative treatment ofcarpal tunnel syndrome in Denmark. Results of a questionnaire.J Hand Surg 1997;22B:761–763.
30. Rossignol M, Stock S, Patry L, Armstrong B. Carpal tunnel syn-drome: what is attributable to work? The Montreal study. OccupEnviron Med 1997;54:519–523.
31. Mattioli S, Baldasseroni A, Curti S, Cooke RM, Mandes A, ZanardiF, et al. Incidence rates of surgically treated idiopathic carpal tunnel
syndrome in blue- and white-collar workers and housewives inTuscany, Italy. Occup Environ Med 2009;66:299–304.tember

INCIDENCE OF CTS IN KOREA 1417
32. Hanrahan LP, Higgins D, Anderson H, Smith M. Wisconsin occu-pational carpal tunnel syndrome surveillance: the incidence of sur-gically treated cases. Wis Med J 1993;92:685–689.
33. Redmond MD, Rivner MH. False positive electrodiagnostic tests incarpal tunnel syndrome. Muscle Nerve 1988;11:511–518.
34. Nathan PA, Meadows KD, Doyle LS. Relationship of age and sex tosensory conduction of the median nerve at the carpal tunnel andassociation of slowed conduction with symptoms. Muscle Nerve1988;11:1149–1153.
35. Mondelli M, Aprile I, Ballerini M, Ginanneschi F, Reale F,
Romano C, et al. Sex differences in carpal tunnel syndrome:JHS �Vol A, Sep
comparison of surgical and non-surgical populations. Eur J Neurol2005;12:976–983.
36. Padua L, LoMonaco M, Gregori B, Valente EM, Padua R, Tonali P.Neurophysiological classification and sensitivity in 500 carpal tunnelsyndrome hands. Acta Neurol Scand 1997;96:211–217.
37. Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Genderdifferences in the utilization of health care services. J Fam Pract2000;49:147–152.
38. Masi AT. Potential uses and limitations of hospital data in epidemi-ologic research. Am J Public Health Nations Health 1965;55:658–
667.tember


























![[18'] Carpal](https://img.pdfslide.net/doc/110x75/577d20351a28ab4e1e924083/18-carpal.jpg)

