Embed Size (px)
Citation preview

Accepte
Reprintof Surgenia, 4 ME-mail:
0039-60
� 2012
doi:10.1
186 S
Incidence of venousthromboembolism in patientsundergoing surgical treatmentfor malignancy by type of neoplasm:An analysis of ACS-NSQIP datafrom 2005 to 2010Caroline E. Reinke, MD, MSPH,a,b Giorgos C. Karakousis, MD,a Rachel A. Hadler, MD,c
Jeffrey A. Drebin, MD, PhD,a Douglas L. Fraker, MD,a and Rachel R. Kelz, MD, MSCE,a
Philadelphia, PA
Introduction. This study investigates the incidence, relative risk, and adjusted odds ratio of venousthromboembolism (VTE) among patients with malignant neoplasms compared with those with benignneoplasms, as well as the incidence of outpatient VTE diagnosis.Methods.We performed a retrospective cohort study of patients in the ACS-NSQIP database from 2005 to2010 with a postoperative diagnosis of neoplasm. The incidence of 30-day VTE, post-VTE death, theincidence of postdischarge VTE diagnosis, and the relative risk of postoperative VTE was calculated bycancer site. Logistic regression was used to calculate an independent odds ratio for each neoplasm site,adjusting for age, gender, body mass index, and operative time.Results. Of 208,200 patients, 159,752 had a malignant diagnosis of the sites of interest and 48,448had benign/carcinoma in situ neoplasms. The incidence, relative risk, and odds ratio of 30-day VTEvaried substantially by site of malignancy. The absolute incidence of outpatient VTE diagnosis varied bysite and percent of VTE diagnosed as an outpatient was found to increase over time.Conclusion. Recommendations for VTE prophylaxis and duration of VTE prophylaxis for patientsundergoing operations may benefit from tailoring to the specific type of malignancy. The increasingpercentage of VTE events diagnosed as an outpatient may impact hospitals substantially as financialpenalties for readmission are enacted. (Surgery 2012;152:186-92.)
From the Department of Surgery,a the Center for Health Improvement and Patient Safety,b Department ofMedicine, Perelman School of Medicine at the University of Pennsylvania, and the Perelman School ofMedicine at the University of Pennsylvania,c Philadelphia, PA
THE RELATIONSHIP BETWEEN MALIGNANCY, SURGERY, AND
VENOUS THROMBOEMBOLISM (VTE) is well estab-lished.1-5 VTE is a potentially fatal event, andlong-term consequences of deep venous thrombo-sis can result in substantial disability. Previous stud-ies have reported that the incidence of VTE variesby type of neoplasm,1,6,7 but data regarding VTE bytype of neoplasm for surgical patients are sparse.
d for publication May 10, 2012.
requests: Caroline E. Reinke, MD, MSPH, Departmentry Education, Hospital of the University of Pennsylva-aloney, 3400 Spruce Street, Philadelphia, PA 19104.
60/$ - see front matter
Mosby, Inc. All rights reserved.
016/j.surg.2012.05.003
URGERY
Current guidelines provide recommendationson the use of inpatient pharmacoprophylaxis forsurgical oncology patients, but risk stratification bytype of neoplasm is not available. The practice ofcontinuing pharmacoprophylaxis after discharge isreserved for the ‘‘high-risk’’ patient and the use ofthis practice varies widely. Little is known regard-ing rates of outpatient VTE diagnosis by site ofneoplasm for surgical patients.
The current study was designed to help informsurgeons whendeciding onmethod andduration ofpharmacoprophylaxis for their cancer patients by(1) defining the incidence, relative risk, and ad-justed odds ratio of VTE after surgical interventionby neoplasm site and (2) determining the incidenceof VTE diagnosis after hospital discharge by site ofmalignancy.

SurgeryVolume 152, Number 2
Reinke et al 187
METHODSData source, study design, and cohort. After
exemption by the Institutional Review Board of theUniversity of Pennsylvania, we performed a retro-spective cohort study of adult patients entered intothe 2005–2010 American College of SurgeonsNational Quality Improvement Program Partici-pant Use Data File (ACS-NSQIP PUF) with apostoperative diagnosis of neoplasm (Table I).The ACS-NSQIP PUF is a Health Insurance Porta-bility and Accountability Act–compliant, multi-institutional data source available to researchersaffiliated with ACS-NSQIP hospitals.8 The PUFcontains aggregate data submitted by participatinghospitals with associated patient level information.Data are collected by trained chart reviewers andcompiled by the ACS-NSQIP. It has been welldescribed elsewhere in the literature.9,10
Patients were classified by site (anatomic loca-tion) and type (malignant, carcinoma in situ[CIS], benign, or uncertain) of neoplasm basedon the ICD-9 diagnosis code (Table I). Patientswith CIS and benign neoplasms were combinedfor all analyses and compared with patients withmalignant neoplasms. Patients with neoplasms ofuncertain behavior were excluded from analysis.
Primary outcome measure. The primary out-come measure was the occurrence of a postopera-tive VTE, defined as either a pulmonary embolism(PE) or a deep venous thrombosis, within 30 days ofthe primary procedure. ACS-NSQIP defines PE as alodging of blood clot in the pulmonary artery withsubsequent obstruction of blood supply to the lungparenchyma. A PE was considered to have occurredif the patient had a ventilation–perfusion scaninterpreted as ‘‘high probability’’ of PE, a positivepulmonary arteriogram, or a spiral positive com-puted tomography examination or angiogram.Deep venous thrombosis is defined as the identifi-cation of a new blood clot or thrombus within thevenous system. This diagnosis is confirmed byduplex ultrasonography, venogram, or computedtomography. The patient had to be treated withanticoagulation therapy and/or placement of avena cava filter or clipping of the vena cava.3
Secondary outcome measures. In cancer pa-tients, death after VTE was determined by site ofmalignancy. VTE events were characterized asinpatient or outpatient based on the differencebetween the number of days to discharge and thenumber of days to VTE. A positive difference wasdefined as inpatient, whereas a negative differencewas defined as outpatient. Patients who were miss-ing day of diagnosis of VTE or day of discharge
were excluded. Patients with a day of VTE diagno-sis on the same day as the day of discharge (n = 47)were considered outpatient, because it is unlikelythat patients would be discharged on the sameday as diagnosis of VTE. Because postoperative oc-currences are only tracked for 30 days from theprocedure date, the number of days to dischargewas censored at 30 days. Fewer than 1% of patients(n = 1,974) had a duration of stay >30 days. Pa-tients with a duration of stay >30 days were codedas 30 days in all analyses.
Statistical analysis. Descriptive statistics wereperformed by site and type of neoplasm. Theincidence of 30-day VTE was calculated per 1,000cases for malignant and benign/CIS neoplasms bysite of neoplasm. The relative risk of postoperativeVTE in patients with malignant neoplasms wasdetermined by site of neoplasm using the benign/CIS group as natural control for each malignantneoplasm. For each site of neoplasm, the chi-square test or Fisher exact test was used to deter-mine if the rate of VTE was different between themalignant and benign/CIS patients as appropri-ate. An adjusted odds ratio of VTE in patients withmalignant neoplasms was calculated for each neo-plasm site using logistic regression with the be-nign/CIS group as the reference group. Potentialconfounders were selected based on those readilyavailable using administrative date as well as thosemost frequently associated with VTE outside of themalignancy status. Because the study was focusedon the individual risk of VTE by site of neoplasm,we were interested in all patients regardless of theprocedure type. Operative time was selected in lieuof operative procedure to control for the casecomplexity and duration. In addition to operativeduration, age, and body mass index, were selectedas well-established risk factors for VTE.6,11-13 Be-cause several risk factors for VTE are specific towomen (oral contraceptives, hormone replace-ment therapy), we added gender to the adjustedmodel as well.
Death after a diagnosis of VTE among cancerpatients was also tabulated by site of neoplasm. Forpatients with known malignancies, the median dayof diagnosis withVTEand thepercentage of patientsdiagnosed in the outpatient setting were calculatedby site of neoplasm. The odds of having an outpa-tient diagnosis of VTE in cancer patients wasexamined over time using the Score test for trendof odds and the percent of VTE patients diagnosedas an outpatient was depicted graphically.
All analyses were performed using STATA 11.2(STATA Corp, Houston, TX).
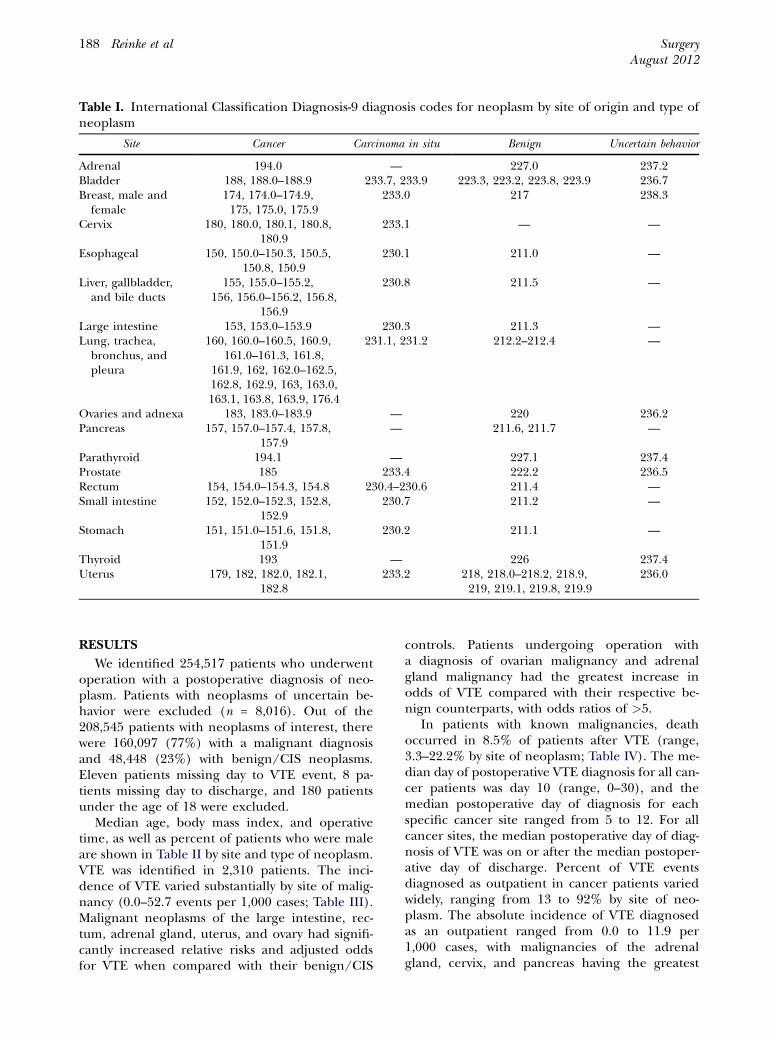
Table I. International Classification Diagnosis-9 diagnosis codes for neoplasm by site of origin and type ofneoplasm
Site Cancer Carcinoma in situ Benign Uncertain behavior
Adrenal 194.0 — 227.0 237.2Bladder 188, 188.0–188.9 233.7, 233.9 223.3, 223.2, 223.8, 223.9 236.7Breast, male and
female174, 174.0–174.9,175, 175.0, 175.9
233.0 217 238.3
Cervix 180, 180.0, 180.1, 180.8,180.9
233.1 — —
Esophageal 150, 150.0–150.3, 150.5,150.8, 150.9
230.1 211.0 —
Liver, gallbladder,and bile ducts
155, 155.0–155.2,156, 156.0–156.2, 156.8,
156.9
230.8 211.5 —
Large intestine 153, 153.0–153.9 230.3 211.3 —Lung, trachea,
bronchus, andpleura
160, 160.0–160.5, 160.9,161.0–161.3, 161.8,
161.9, 162, 162.0–162.5,162.8, 162.9, 163, 163.0,163.1, 163.8, 163.9, 176.4
231.1, 231.2 212.2–212.4 —
Ovaries and adnexa 183, 183.0–183.9 — 220 236.2Pancreas 157, 157.0–157.4, 157.8,
157.9— 211.6, 211.7 —
Parathyroid 194.1 — 227.1 237.4Prostate 185 233.4 222.2 236.5Rectum 154, 154.0–154.3, 154.8 230.4–230.6 211.4 —Small intestine 152, 152.0–152.3, 152.8,
152.9230.7 211.2 —
Stomach 151, 151.0–151.6, 151.8,151.9
230.2 211.1 —
Thyroid 193 — 226 237.4Uterus 179, 182, 182.0, 182.1,
182.8233.2 218, 218.0–218.2, 218.9,
219, 219.1, 219.8, 219.9236.0
SurgeryAugust 2012
188 Reinke et al
RESULTS
We identified 254,517 patients who underwentoperation with a postoperative diagnosis of neo-plasm. Patients with neoplasms of uncertain be-havior were excluded (n = 8,016). Out of the208,545 patients with neoplasms of interest, therewere 160,097 (77%) with a malignant diagnosisand 48,448 (23%) with benign/CIS neoplasms.Eleven patients missing day to VTE event, 8 pa-tients missing day to discharge, and 180 patientsunder the age of 18 were excluded.
Median age, body mass index, and operativetime, as well as percent of patients who were maleare shown in Table II by site and type of neoplasm.VTE was identified in 2,310 patients. The inci-dence of VTE varied substantially by site of malig-nancy (0.0–52.7 events per 1,000 cases; Table III).Malignant neoplasms of the large intestine, rec-tum, adrenal gland, uterus, and ovary had signifi-cantly increased relative risks and adjusted oddsfor VTE when compared with their benign/CIS
controls. Patients undergoing operation witha diagnosis of ovarian malignancy and adrenalgland malignancy had the greatest increase inodds of VTE compared with their respective be-nign counterparts, with odds ratios of >5.
In patients with known malignancies, deathoccurred in 8.5% of patients after VTE (range,3.3–22.2% by site of neoplasm; Table IV). The me-dian day of postoperative VTE diagnosis for all can-cer patients was day 10 (range, 0–30), and themedian postoperative day of diagnosis for eachspecific cancer site ranged from 5 to 12. For allcancer sites, the median postoperative day of diag-nosis of VTE was on or after the median postoper-ative day of discharge. Percent of VTE eventsdiagnosed as outpatient in cancer patients variedwidely, ranging from 13 to 92% by site of neo-plasm. The absolute incidence of VTE diagnosedas an outpatient ranged from 0.0 to 11.9 per1,000 cases, with malignancies of the adrenalgland, cervix, and pancreas having the greatest
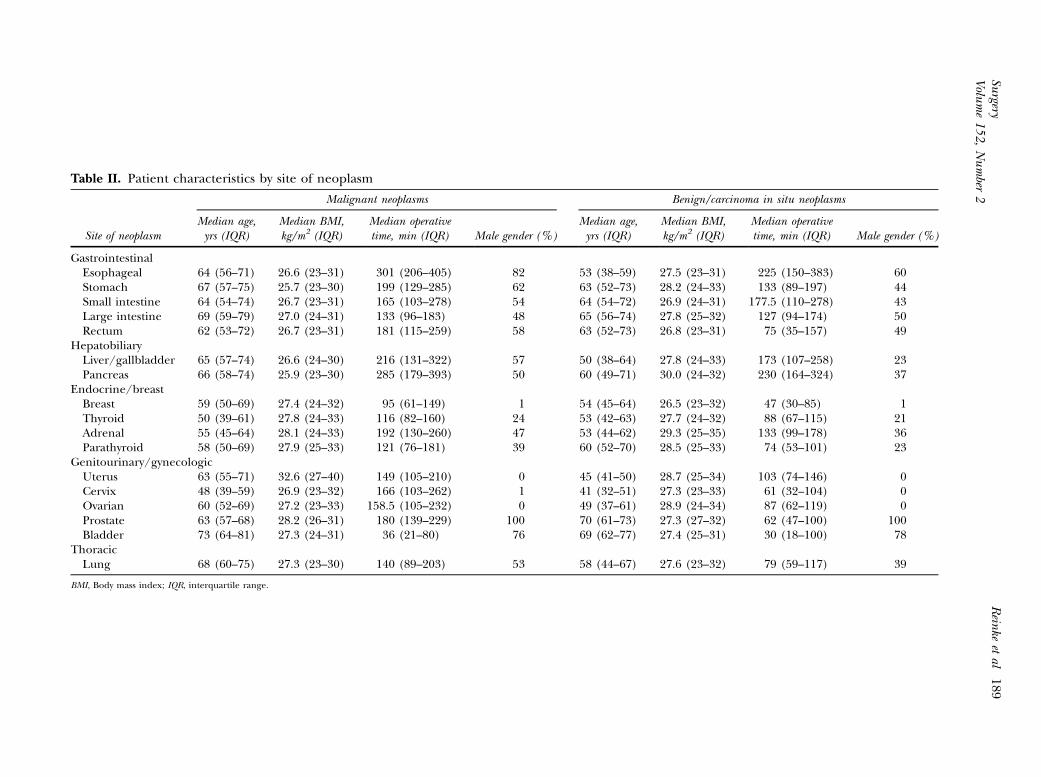
Table II. Patient characteristics by site of neoplasm
Site of neoplasm
Malignant neoplasms Benign/carcinoma in situ neoplasms
Median age,yrs (IQR)
Median BMI,kg/m2 (IQR)
Median operativetime, min (IQR) Male gender (%)
Median age,yrs (IQR)
Median BMI,kg/m2 (IQR)
Median operativetime, min (IQR) Male gender (%)
GastrointestinalEsophageal 64 (56–71) 26.6 (23–31) 301 (206–405) 82 53 (38–59) 27.5 (23–31) 225 (150–383) 60Stomach 67 (57–75) 25.7 (23–30) 199 (129–285) 62 63 (52–73) 28.2 (24–33) 133 (89–197) 44Small intestine 64 (54–74) 26.7 (23–31) 165 (103–278) 54 64 (54–72) 26.9 (24–31) 177.5 (110–278) 43Large intestine 69 (59–79) 27.0 (24–31) 133 (96–183) 48 65 (56–74) 27.8 (25–32) 127 (94–174) 50Rectum 62 (53–72) 26.7 (23–31) 181 (115–259) 58 63 (52–73) 26.8 (23–31) 75 (35–157) 49
HepatobiliaryLiver/gallbladder 65 (57–74) 26.6 (24–30) 216 (131–322) 57 50 (38–64) 27.8 (24–33) 173 (107–258) 23Pancreas 66 (58–74) 25.9 (23–30) 285 (179–393) 50 60 (49–71) 30.0 (24–32) 230 (164–324) 37
Endocrine/breastBreast 59 (50–69) 27.4 (24–32) 95 (61–149) 1 54 (45–64) 26.5 (23–32) 47 (30–85) 1Thyroid 50 (39–61) 27.8 (24–33) 116 (82–160) 24 53 (42–63) 27.7 (24–32) 88 (67–115) 21Adrenal 55 (45–64) 28.1 (24–33) 192 (130–260) 47 53 (44–62) 29.3 (25–35) 133 (99–178) 36Parathyroid 58 (50–69) 27.9 (25–33) 121 (76–181) 39 60 (52–70) 28.5 (25–33) 74 (53–101) 23
Genitourinary/gynecologicUterus 63 (55–71) 32.6 (27–40) 149 (105–210) 0 45 (41–50) 28.7 (25–34) 103 (74–146) 0Cervix 48 (39–59) 26.9 (23–32) 166 (103–262) 1 41 (32–51) 27.3 (23–33) 61 (32–104) 0Ovarian 60 (52–69) 27.2 (23–33) 158.5 (105–232) 0 49 (37–61) 28.9 (24–34) 87 (62–119) 0Prostate 63 (57–68) 28.2 (26–31) 180 (139–229) 100 70 (61–73) 27.3 (27–32) 62 (47–100) 100Bladder 73 (64–81) 27.3 (24–31) 36 (21–80) 76 69 (62–77) 27.4 (25–31) 30 (18–100) 78
ThoracicLung 68 (60–75) 27.3 (23–30) 140 (89–203) 53 58 (44–67) 27.6 (23–32) 79 (59–117) 39
BMI, Body mass index; IQR, interquartile range.
Surgery
Volu
me152,Number
2Rein
keetal
189
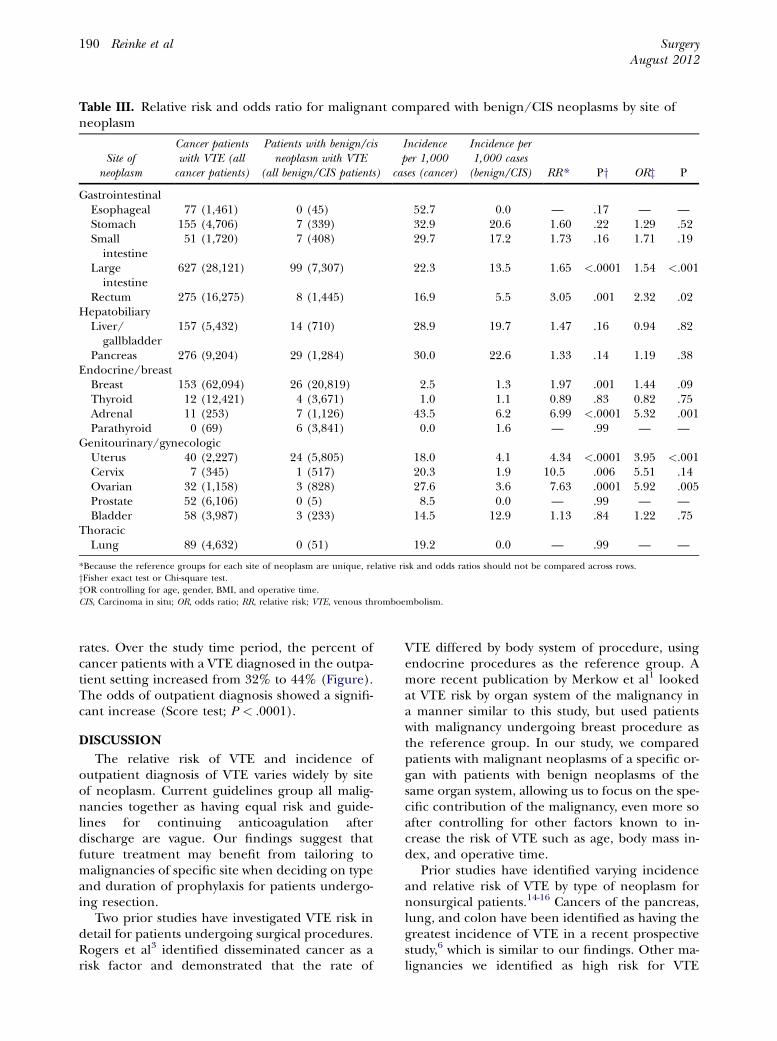
Table III. Relative risk and odds ratio for malignant compared with benign/CIS neoplasms by site ofneoplasm
Site ofneoplasm
Cancer patientswith VTE (allcancer patients)
Patients with benign/cisneoplasm with VTE
(all benign/CIS patients)
Incidenceper 1,000
cases (cancer)
Incidence per1,000 cases(benign/CIS) RR* Py ORz P
GastrointestinalEsophageal 77 (1,461) 0 (45) 52.7 0.0 — .17 — —Stomach 155 (4,706) 7 (339) 32.9 20.6 1.60 .22 1.29 .52Smallintestine
51 (1,720) 7 (408) 29.7 17.2 1.73 .16 1.71 .19
Largeintestine
627 (28,121) 99 (7,307) 22.3 13.5 1.65 <.0001 1.54 <.001
Rectum 275 (16,275) 8 (1,445) 16.9 5.5 3.05 .001 2.32 .02Hepatobiliary
Liver/gallbladder
157 (5,432) 14 (710) 28.9 19.7 1.47 .16 0.94 .82
Pancreas 276 (9,204) 29 (1,284) 30.0 22.6 1.33 .14 1.19 .38Endocrine/breast
Breast 153 (62,094) 26 (20,819) 2.5 1.3 1.97 .001 1.44 .09Thyroid 12 (12,421) 4 (3,671) 1.0 1.1 0.89 .83 0.82 .75Adrenal 11 (253) 7 (1,126) 43.5 6.2 6.99 <.0001 5.32 .001Parathyroid 0 (69) 6 (3,841) 0.0 1.6 — .99 — —
Genitourinary/gynecologicUterus 40 (2,227) 24 (5,805) 18.0 4.1 4.34 <.0001 3.95 <.001Cervix 7 (345) 1 (517) 20.3 1.9 10.5 .006 5.51 .14Ovarian 32 (1,158) 3 (828) 27.6 3.6 7.63 .0001 5.92 .005Prostate 52 (6,106) 0 (5) 8.5 0.0 — .99 — —Bladder 58 (3,987) 3 (233) 14.5 12.9 1.13 .84 1.22 .75
ThoracicLung 89 (4,632) 0 (51) 19.2 0.0 — .99 — —
*Because the reference groups for each site of neoplasm are unique, relative risk and odds ratios should not be compared across rows.yFisher exact test or Chi-square test.zOR controlling for age, gender, BMI, and operative time.CIS, Carcinoma in situ; OR, odds ratio; RR, relative risk; VTE, venous thromboembolism.
SurgeryAugust 2012
190 Reinke et al
rates. Over the study time period, the percent ofcancer patients with a VTE diagnosed in the outpa-tient setting increased from 32% to 44% (Figure).The odds of outpatient diagnosis showed a signifi-cant increase (Score test; P < .0001).
DISCUSSION
The relative risk of VTE and incidence ofoutpatient diagnosis of VTE varies widely by siteof neoplasm. Current guidelines group all malig-nancies together as having equal risk and guide-lines for continuing anticoagulation afterdischarge are vague. Our findings suggest thatfuture treatment may benefit from tailoring tomalignancies of specific site when deciding on typeand duration of prophylaxis for patients undergo-ing resection.
Two prior studies have investigated VTE risk indetail for patients undergoing surgical procedures.Rogers et al3 identified disseminated cancer as arisk factor and demonstrated that the rate of
VTE differed by body system of procedure, usingendocrine procedures as the reference group. Amore recent publication by Merkow et al1 lookedat VTE risk by organ system of the malignancy ina manner similar to this study, but used patientswith malignancy undergoing breast procedure asthe reference group. In our study, we comparedpatients with malignant neoplasms of a specific or-gan with patients with benign neoplasms of thesame organ system, allowing us to focus on the spe-cific contribution of the malignancy, even more soafter controlling for other factors known to in-crease the risk of VTE such as age, body mass in-dex, and operative time.
Prior studies have identified varying incidenceand relative risk of VTE by type of neoplasm fornonsurgical patients.14-16 Cancers of the pancreas,lung, and colon have been identified as having thegreatest incidence of VTE in a recent prospectivestudy,6 which is similar to our findings. Other ma-lignancies we identified as high risk for VTE
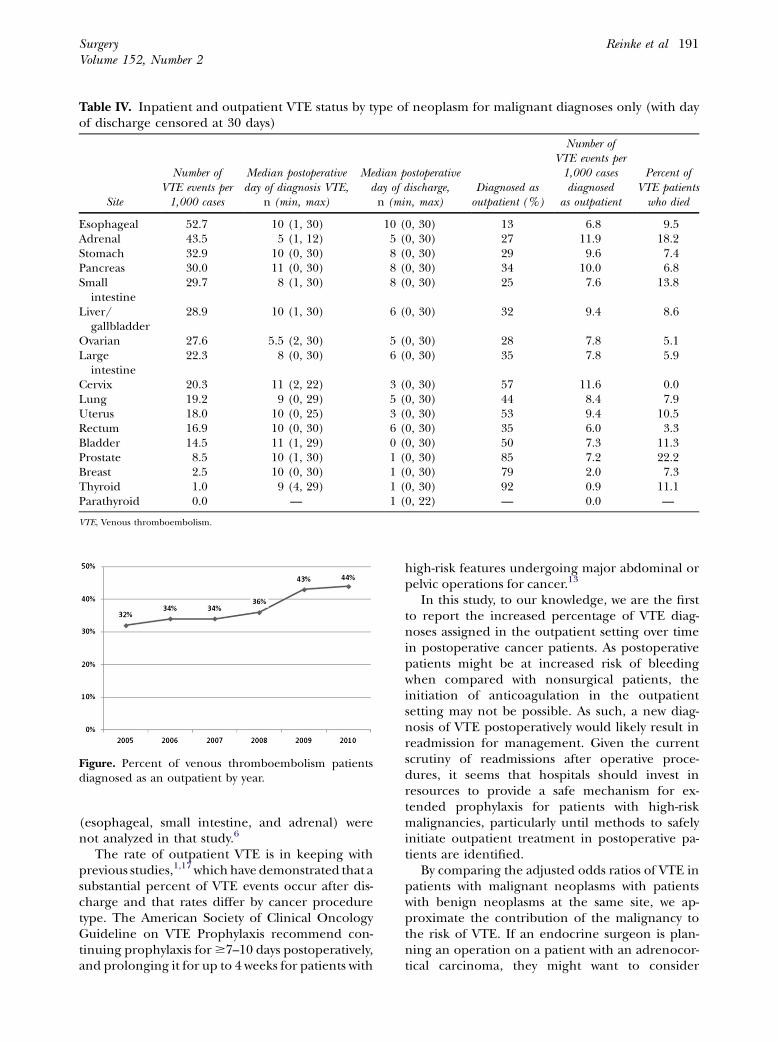
Table IV. Inpatient and outpatient VTE status by type of neoplasm for malignant diagnoses only (with dayof discharge censored at 30 days)
Site
Number ofVTE events per1,000 cases
Median postoperativeday of diagnosis VTE,
n (min, max)
Median postoperativeday of discharge,n (min, max)
Diagnosed asoutpatient (%)
Number ofVTE events per1,000 casesdiagnosed
as outpatient
Percent ofVTE patientswho died
Esophageal 52.7 10 (1, 30) 10 (0, 30) 13 6.8 9.5Adrenal 43.5 5 (1, 12) 5 (0, 30) 27 11.9 18.2Stomach 32.9 10 (0, 30) 8 (0, 30) 29 9.6 7.4Pancreas 30.0 11 (0, 30) 8 (0, 30) 34 10.0 6.8Small
intestine29.7 8 (1, 30) 8 (0, 30) 25 7.6 13.8
Liver/gallbladder
28.9 10 (1, 30) 6 (0, 30) 32 9.4 8.6
Ovarian 27.6 5.5 (2, 30) 5 (0, 30) 28 7.8 5.1Large
intestine22.3 8 (0, 30) 6 (0, 30) 35 7.8 5.9
Cervix 20.3 11 (2, 22) 3 (0, 30) 57 11.6 0.0Lung 19.2 9 (0, 29) 5 (0, 30) 44 8.4 7.9Uterus 18.0 10 (0, 25) 3 (0, 30) 53 9.4 10.5Rectum 16.9 10 (0, 30) 6 (0, 30) 35 6.0 3.3Bladder 14.5 11 (1, 29) 0 (0, 30) 50 7.3 11.3Prostate 8.5 10 (1, 30) 1 (0, 30) 85 7.2 22.2Breast 2.5 10 (0, 30) 1 (0, 30) 79 2.0 7.3Thyroid 1.0 9 (4, 29) 1 (0, 30) 92 0.9 11.1Parathyroid 0.0 — 1 (0, 22) — 0.0 —
VTE, Venous thromboembolism.
Figure. Percent of venous thromboembolism patientsdiagnosed as an outpatient by year.
SurgeryVolume 152, Number 2
Reinke et al 191
(esophageal, small intestine, and adrenal) werenot analyzed in that study.6
The rate of outpatient VTE is in keeping withprevious studies,1,17 whichhave demonstrated that asubstantial percent of VTE events occur after dis-charge and that rates differ by cancer proceduretype. The American Society of Clinical OncologyGuideline on VTE Prophylaxis recommend con-tinuing prophylaxis for$7–10 days postoperatively,and prolonging it for up to 4 weeks for patients with
high-risk features undergoing major abdominal orpelvic operations for cancer.13
In this study, to our knowledge, we are the firstto report the increased percentage of VTE diag-noses assigned in the outpatient setting over timein postoperative cancer patients. As postoperativepatients might be at increased risk of bleedingwhen compared with nonsurgical patients, theinitiation of anticoagulation in the outpatientsetting may not be possible. As such, a new diag-nosis of VTE postoperatively would likely result inreadmission for management. Given the currentscrutiny of readmissions after operative proce-dures, it seems that hospitals should invest inresources to provide a safe mechanism for ex-tended prophylaxis for patients with high-riskmalignancies, particularly until methods to safelyinitiate outpatient treatment in postoperative pa-tients are identified.
By comparing the adjusted odds ratios of VTE inpatients with malignant neoplasms with patientswith benign neoplasms at the same site, we ap-proximate the contribution of the malignancy tothe risk of VTE. If an endocrine surgeon is plan-ning an operation on a patient with an adrenocor-tical carcinoma, they might want to consider

SurgeryAugust 2012
192 Reinke et al
extended prophylaxis, whereas for patients withfunctional, benign neoplasms of the adrenalgland, extended prophylaxis may not be war-ranted. The reported findings do not permit usto compare the role of malignancy as a risk factorfor VTE across sites of neoplasm owing to theunique reference groups; however, because a pa-tient’s cancer status, when known, is usually attrib-utable to a specific site, this information will behelpful in preoperative planning, regardless of thescheduled procedure.
Limitations of this study include an inability toidentify use of preoperative, postoperative inpa-tient, and postoperative outpatient VTE prophy-laxis, which is not possible in the ACS-NSQIPdatabase. Although we did not control for or limitspecific procedure type in this study, by controllingfor operative time we were better able to identifythe contribution of the malignancy to VTE risk forpatients undergoing many different procedures.Unfortunately, we are probably underestimatingthe rate of VTE in this study, because fatal pulmo-nary emboli are frequently suspected but notconfirmed and would, therefore, not be recordedin the ACS-NSQIP PUF. There is no reason tosuspect that these unrecorded events would bemore frequent in patients without malignancy and,therefore, are unlikely to affect our findings.
The incidence of VTE is greater in patients withmalignant neoplasms undergoing surgical proce-dures when compared with their benign counter-parts. The relative risk of VTE varies by type ofneoplasm and is not uniform across patientsundergoing surgical procedures. After controllingfor patient characteristics known to be associatedwith VTE, the odds ratio of VTE remained in-creased for malignancies of specific sites. Recom-mendations for VTE prophylaxis for patientsundergoing surgical procedures may benefit fromtailoring to the specific type of malignancy. Addi-tionally, the results of this study and others suggestthat extended VTE pharmacoprophylaxis shouldbe considered for patients undergoing operationsfor malignancies with a high incidence of VTEdiagnosis after discharge. Future studies to deter-mine the impact of extending VTE prophylaxis onrates of VTE and readmission or complications ofbleeding are needed.
The American College of Surgeons National SurgicalQuality Improvement Program and the hospitals partici-pating in the ACS-NSQIP are the source of the data usedherein; they have not verified and are not responsible
for the statistical validity of the data analysis or theconclusions derived by the authors.
REFERENCES
1. Merkow RP, Bilimoria KY, McCarter MD, et al. Post-discharge venous thromboembolism after cancer surgery:extending the case for extended prophylaxis. Ann Surg2011;254:131-7.
2. Bergqvist D. Venous thromboembolism and cancer: preven-tion of VTE. Thromb Res 2001;102:V209-13.
3. Rogers SO Jr, Kilaru RK, Hosokawa P, et al. Multivariablepredictors of postoperative venous thromboembolic eventsafter general and vascular surgery: results from the patientsafety in surgery study. J Am Coll Surg 2007;204:1211-21.
4. Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignan-cies, prothrombotic mutations, and the risk of venousthrombosis. JAMA 2005;293:715-22.
5. White RH, Zhou H, Romano PS. Incidence of symptomaticvenous thromboembolism after different elective or urgentsurgical procedures. Thromb Haemost 2003;90:446-55.
6. Agnelli G, Bolis G, Capussotti L, et al. A clinical outcome-based prospective study on venous thromboembolism aftercancer surgery: the @RISTOS project. Ann Surg 2006;243:89-95.
7. Lee AY, Levine MN. Venous thromboembolism and cancer:risks and outcomes. Circulation 2003;107(23 Suppl 1):I17-21.
8. Raval M, Caprini J, Esnaola N. ACS NSQIP Best practicesguidelines: prevention and treatment of venous thromboem-bolism. 2009. Available from: http://reports.nsqip.facs.org/acsmain/private/documents/bestpractice/index.jsp.
9. Khuri SF. The NSQIP: a new frontier in surgery. Surgery2005;138:837-43.
10. Khuri SF, Daley J, Henderson W, et al. The Department ofVeterans Affairs’ NSQIP: the first national, validated,outcome-based, risk-adjusted, and peer-controlled programfor the measurement and enhancement of the quality ofsurgical care. National VA Surgical Quality ImprovementProgram. Ann Surg 1998;228:491-507.
11. Caprini J. Venous thromboembolism risk factor assessment[updated 2006]. Available from: http://www.crmhealthcare.net/docs/67450a_CapriniRiskAssesemntTool.pdf.
12. Anderson FA Jr, Spencer FA. Risk factors for venousthromboembolism. Circulation 2003;107(23 Suppl 1):I9-16.
13. Lyman GH, Khorana AA, Falanga A, et al. American Societyof Clinical Oncology guideline: recommendations forvenous thromboembolism prophylaxis and treatment in pa-tients with cancer. J Clin Oncol 2007;25:5490-505.
14. Levitan N, Dowlati A, Remick SC, et al. Rates of initial andrecurrent thromboembolic disease among patients withmalignancy versus those without malignancy. Risk analysisusing Medicare claims data. Medicine (Baltimore) 1999;78:285-91.
15. Heit JA. Cancer and venous thromboembolism: scope ofthe problem. Cancer Control 2005;12(Suppl 1):5-10.
16. Thodiyil PA, Kakkar AK. Variation in relative risk of venousthromboembolism in different cancers. Thromb Haemost2002;87:1076-7.
17. Reinke CE, Hadler RA, Karakousis GC, et al. Does the pres-ence of thyroid cancer increase the risk of venous thrombo-embolism in patients undergoing thyroidectomy? Surgery2011;150:1275-85.