Embed Size (px)
Citation preview

Table of ContentsSupplementary Materials and Methods...............................................................................................................3Included Technology Assessment Groups (TAGs).............................................................................................3Excluded Organizations........................................................................................................................................3Technical Working Group Members (TWG)......................................................................................................3Experts Providing Background Interviews.........................................................................................................4Included Reviews...................................................................................................................................................4Table: Quality Summaries....................................................................................................................................6Supplemental Materials Detailed Summaries.....................................................................................................9AHRQ. Genetic Testing for Developmental Disabilities, Intellectual Disability and Autism Spectrum Disorder, 2015........................................................................................................................................................9AHRQ. Emerging Approaches to Diagnosis and Treatment of Non–Muscle-Invasive Bladder Cancer, 2015........................................................................................................................................................................10AHRQ. Technology Assessment of Molecular Pathology Testing for the Estimation of Prognosis for Common Cancers, 2014.......................................................................................................................................11AHRQ. Testing of CYP2C19 Variants and Platelet Reactivity for Guiding Antiplatelet Treatment, 2013.................................................................................................................................................................................12AHRQ. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: Systematic Review to Update the U.S. Preventive Services Task Force Recommendation, 2013................13AHRQ. PCA3 Testing in the Diagnosis and Management of Prostate Cancer: Future Research Needs, 2013........................................................................................................................................................................14AHRQ. Technology Assessment on Genetic Testing or Molecular Pathology Testing of Cancers with Unknown Primary Site to Determine Origin, 2013..........................................................................................15AHRQ. Fecal DNA Testing in Screening for Colorectal Cancer in Average-Risk Adults, 2013..................16AHRQ. Gene Expression Profiling (GEP) for Predicting Outcomes in Stage II Colon Cancer, 2012........17AHRQ. Systematic Reviews on Selected Pharmacogenetic Tests for Cancer Treatment: CYP2D6 for Tamoxifen in Breast Cancer, KRAS for anti-EGFR antibodies in Colorectal Cancer, and BCR-ABL1 for Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia, 2010...................................................................18BCBS TEC. Special Report: Chromosomal Microarray for the Genetic Evaluation of Patients With Global Developmental Delay, Intellectual Disability, and Autism Spectrum Disorder, 2015......................19BCBS TEC. Noninvasive Prenatal Cell-Free Fetal DNA-Based Screening for Aneuploidies Other Than Trisomy 21, 2014..................................................................................................................................................20BCBS TEC. Gene Expression Analysis for Prostate Cancer Management, 2014.........................................21BCBS TEC. Gene Expression Profiling in Women With Lymph Node‒Negative Breast Cancer to Select Adjuvant Chemotherapy, 2014...........................................................................................................................22BCBS TEC. Fecal DNA Analysis for Colorectal Cancer Screening, 2014.....................................................23BCBS TEC. Special Report: Multiple Molecular Testing of Cancers to Identify Targeted Therapies, 2013.................................................................................................................................................................................24BCBS TEC. Special Report: Exome Sequencing for Clinical Diagnosis of Patients with Suspected Genetic Disorders, 2013.....................................................................................................................................................25BCBS TEC. CYP2D6 Pharmacogenomics of Tamoxifen Treatment, 2013....................................................26

BCBS TEC. Sequencing-Based Tests to Determine Fetal Down Syndrome (Trisomy 21) from Maternal Plasma DNA, 2012...............................................................................................................................................27Cochrane. Cancer genetic risk assessment for individuals at risk of familial breast cancer, 2012..............28Cochrane. Effects of communicating DNA-based disease risk estimates on risk-reducing behaviours, 2010........................................................................................................................................................................29
Supplementary Materials
Included Technology Assessment Groups (TAGs)We first developed a list of potential TAGs based on our review of the literature, and confirmed this list with the TWG. Using our inclusion criteria, we narrowed this to 13 key TAGs: Agency for Healthcare Research and Quality, Blue Cross Blue Shield Association’s Technology Evaluation Center (now called BCBSA Evidence Street), Center for Medical Technology Policy, Centers for Medicare and Medicaid Services, Cochrane Library, Evaluation of Genomic Applications in Practice and Prevention, Institute for Clinical and Economic Review, Lewin Group Center for CER, Medicare Payment Advisory Commission (MEDPAC), National Academy of Medicine (formerly Institute of Medicine), Patient-Centered Outcomes Research Institute (PCORI), US Preventive Services Task Force, and Veteran’s Administration.
Excluded OrganizationsExamples of excluded TAGs and organizations are Up-To-Date, ECRI Institute, and Hayes (these are paid subscription services); Clinical Pharmacogenetics Implementation Consortium (this group publishes guidelines on one type of testing); National Institute for Health and Care Excellence (NICE) (this is a guidelines organization), PROSPERO (International Prospective Register of Systematic Reviews, which is a registry of protocols – not the reviews themselves), and specialty societies (e.g., American Society of Clinical Oncology).
Technical Working Group Members (TWG)The TWG included individuals with expertise in genomic medicine, with a range of disciplinary backgrounds and perspectives: evidence synthesis, comparative effectiveness research, health services research, clinical medicine, genetic epidemiology, public health genomics. Members reviewed results of TAG reviews and provided expert input regarding conclusions, evidence gaps and potential CER studies. The process for obtaining TWG member input involved two group teleconferences, followed by several group and individual calls and online review of materials and drafts. Kathryn A. Phillips PhD, Founding Director UCSF Center for Translational and Policy Research on Personalized Medicine
(TRANSPERS) and Professor of Health Economics and Health Services Research, University of California San Francisco Patricia Deverka, M.D. M.S. M.B.E. Principal Researcher, American Institutes for Research Sean Tunis, M.D. M.Sc. Founder & Chief Executive Officer, Center for Medical Technology Policy Muin J. Khoury, M.D. Ph.D, Director, Office of Public Health Genomics, CDC Lewis Sandy, M.D. F.A.C.P. Senior Vice President, Clinical Advancement, UnitedHealth Group Geoffrey S. Ginsburg, M.D., Ph.D. Director, Center for Applied Genomics & Precision Medicine, Duke University School of
Medicine, Professor of Medicine and Pathology, Duke University Medical Center Lori A. Orlando, M.D., M.H.S. Internal Medicine Physician, Duke Executive Health, Associate Professor of Medicine, Duke
University School of Medicine.

Experts Providing Background Interviews
James P. Evans, M.D., Ph.D., Bryson Distinguished Professor of Genetics and Medicine, UNC School of Medicine. Dr. Evans’ major interests lie within the field of clinical cancer genetics, the use of high-throughput sequencing in clinical medicine and public policy as it relates to genetics. He has been highly active in scientific education of the US judiciary at the State Supreme Court and Federal level, as well as at the Supreme Court level internationally. He was a member of the advisory committee to the US Secretary of Health and Human Services on Genetics, Health and Society and spearheaded that committee’s task force that investigated gene patenting and its effect on patient care.
Robert Nussbaum, M.D. Chief Medical Officer Invitae (formerly Professor, Department of Medicine, and Chief, Division of Medical Genetics, UCSF). Dr. Robert L. Nussbaum, a board certified internist and medical geneticist, specializes in the care of adults with hereditary disorders. Prior to joining UCSF, Nussbaum was chief of the Genetic Disease Research Branch of the National Human Genome Research Institute, one of the National Institutes of Health.
Sharon F. Terry, M.A, President and Chief Executive Officer, Genetic Alliance. Sharon F. Terry is President and CEO of Genetic Alliance, a network of more than 10,000 organizations, of which 1,200 are disease advocacy organizations. In her focus at the forefront of consumer participation in genetics research, services and policy, she serves in a leadership role on many of the major international and national organizations. She is on the editorial boards of several journals and is an editor of Genome. She led the coalition that was instrumental in the passage of the Genetic Information Nondiscrimination Act.
Bruce Quinn, M.D., Ph.D., Bruce Quinn Associates. Bruce Quinn is a national leader on Medicare policy, the impact of health reform on innovation and the crafting of successful business strategies within the U.S. health care reimbursement system. Before joining FaegreBD Consulting, Dr. Quinn was a senior health policy advisor with Foley Hoag and FaegreBD Consulting after serving as the regional Medicare medical director for the California Part B program, where he had authority for final coverage decisions on approximately 15 percent of the U.S. Medicare program.
Included Reviews
1. Black ER, Falzon L, Aronson N. Gene Expression Profiling for Predicting Outcomes in Stage II Colon Cancer. AHRQ: Blue Cross and Blue Shield Association Technology Evaluation Center Evidence-based Practice Center. December 2012.2. Bradley LA, Palomaki G, Gutman S, Samson DJ, Aronson N. PCA3 Testing for the Diagnosis and Management of Prostate Cancer. AHRQ: Blue Cross and Blue Shield Association Technology Evaluation Center Evidence-based Practice Center. April 2013.3. Chou R, Buckley D, Fu R, et al. Emerging Approaches to Diagnosis and Treatment of Non–Muscle-Invasive Bladder Cancer. AHRQ: Pacific Northwest Evidence-based Practice Center. October 25, 2015.4. Dahabreh IJ, Moorthy D, Lamont JL, Chen ML, Kent DM, Lau J. Testing of CYP2C19 Variants and Platelet Reactivity for Guiding Antiplatelet Treatment. AHRQ: Tufts Evidence-based Practice Center. September 25, 2013.5. Glacy J. CYP2D6 Pharmacogenomics of Tamoxifen Treatment. Blue Cross and Blue Shield Technology Evaluation Center. January 2014.6. Glacy J, Chopra RD. Gene Expression Profiling in Women with Lymph Node-Negative Breast Cancer to Select Adjuvant Chemotherapy. Blue Cross and Blue Shield Technology Evaluation Center. October 2014.7. Grant MD, Chopra R. Special Report: Chromosomal Microarray for the Genetic Evaluation of Patients With Global Developmental Delay, Intellectual Disability, and Autism Spectrum Disorder. Blue Cross and Blue Shield Technology Evaluation Center. August 2015.8. Hilgart JS, Coles B, Iredale R. Cancer genetic risk assessment for individuals at risk of familial breast cancer (Review). The Cochrane Collaboration. 2012.9. Lin J, Webber E, Beil T, Goddard K, Whitlock E. Fecal DNA Testing in Screening for Colorectal Cancer in Average-Risk Adults. AHRQ: Oregon Evidence-based Practice Center. February 29, 2012.10. Mark DH, Ratko, T.A. . Special Report: Multiple Molecular Testing of Cancer to Identify Targeted Therapies. Blue Cross and Blue Shield Technology Evaluation Center. June 2013.11. Mark DH. Fecal DNA Analysis for Colorectal Cancer Screening. Blue Cross and Blue Shield Technology Evaluation Center. December 2014.12. Marteau TM, Franch DP, Griffin SJ, et al. Effects of communicating DNA-based disease risk estimates on risk-reducing behaviors (Review). The Cochrane Collaboration. 2010.13. Meleth S, Reeder-Hayes K, Ashok M, et al. Technology Assessment of Molecular Pathology Testing for the Estimation of Prognosis for Common Cancers. AHRQ: RTI International-University of North Carolina at Chapel Hill Evidence-based Practice Center. May 29, 2014.14. Meleth S, Whitehead N, Swinson-Evans T, Lux L. Technology Assessment on Genetic Testing or Molecular Pathology Testing of Cancer with Unknown Primary Site to Determine Origin. AHRQ: RTI International-University of North Carolina at Chapel Hill Evidence-based Practice Center. February 20, 2013.15. Nelson HD, Fu R, Goddard K, et al. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-related Cancer: Systematic Review to Update the U.S. Preventive Services Task Force Recommendation. AHRQ: Pacific Northwest Evidence-based Practice Center. December 2013.

16. Piper M, Grant MD. Special Report: Exome Sequencing for Clinical Diagnosis for Patients with Suspected Genetic Disorders. Blue Cross and Blue Shield Technology Evaluation Center. August 2013.17. Piper MA, Civic D, Grant MD, Lefevre F. Sequencing-Based Tests to Determine Fetal Down Syndrome (Trisomy 21) form Maternal Plasma DNA. Blue Cross and Blue Shield Technology Evaluation Center. April 2013.18. Ratko TA. Gene Expression Analysis for Prostate Cancer Management. Blue Cross and Blue Shield Technology Evaluation Center. January 2015.19. Ratko TA CR. Noninvasive Prenatal Cell-Free Fetal DNA-based screening for Aneuploidies Other Than Trisomy 21. Blue Cross and Blue Shield Technology Evaluation Center. December 2014.20. Sun F, Oristaglio J, Levy S, et al. Genetic Testing for Developmental Disabilities, Intellectual Disability and Autism Spectrum Disorder. AHRQ: ECRI Institute–Penn Medicine Evidence-based Practice Center. June 29, 2015.21. Terasawa T, Dahabreh I, Castaldi PJ, Trikalinos TA. Systematic Reviews on Selected Pharmacogenetic Tests for Cancer Treatment: CYP2D6 for Tamoxifen in Breast Cancer, KRAS for anti-EGFR antibodies in Colorectal Cancer, and BCR-ABL1 for Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia. AHRQ: Tufts Evidence-based Practice Center. June 7, 2010.
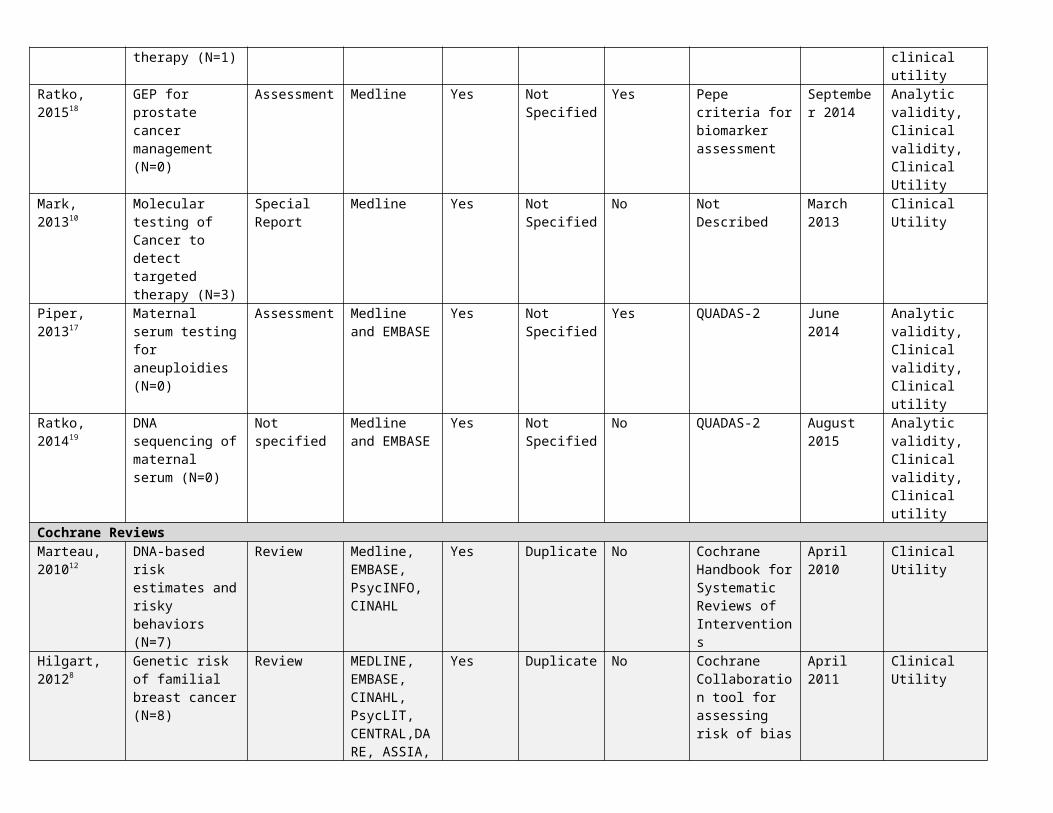
Table: Quality Summaries Author, Year, Reference Number*
Review topic (number of direct studies of clinical outcomes)
Type of Review
Literature searched
Inclusion/ exclusion criteria used
Data extraction protocol
Analytic frameworkused
Risk of Bias instruments used
Date of last search
Type of evidence** looked for in the included studies***
AHRQ ReviewsDahabreh, 20134
CYP2C19 variants and clopidogrel(N=8)
Comparative Effectiveness Review (CER)
Medline, Cochrane, others
Yes Duplicate Yes QUADAS-2AHRQ Methods Guide, others
July 2012 Analytic validity, Clinical validity, Clinical utility
Chou, 20153 Urinary biomarkers in bladder cancer(N=0)
CER Medline, Cochrane, others; gray literature
Yes Duplicate Yes USPSTFQUADAS, AHRQ methods guides
October 2014
Clinical validity,Clinical utility
Bradley, 20132 Prostate cancer antigen 3(no CU studies)
CER Medline, Cochrane; gray literature
Yes Duplicate Yes QUADAS, GRADE
May 2012 Clinical validity, Clinical utility
Lin, 20129 Fecal DNA(N=0)
CER Medline, Cochrane; gray literature
Yes Duplicate Yes QUADAS, geno-mic testing work group, Newcastle Ottawa scale, USPSTF
August 2011 Clinical validity,Clinical utility
Black, 20121 GEP to predict CRC outcomes(N=0)
Technical brief Medline, Cochrane, Embase, others; gray literature
Yes Not Specified
Yes Not Described May 2012 Analytic validity, Clinical validity, Clinical utility
Meleth, 201314 Origin of CUP(N=0)
Technology assessment
Medline, Embase, Cochrane, NIH genetic testing registry, FDA; gray literature
Yes Single abstractor; checked by senior investigator
No (but listed KQs)
QUADAS, EPC strength of evidence, RTI Question Bank
Not specified (report published February 2013)
Analytic validity, Clinical validity, Clinical utility
Sun, 201520 Developmental disabilities (ASD)(N=0)
Technical brief Medline, Embase, Cochrane, gray literature, and National Center for Biotechnology Information
Yes Duplicate No Did not evaluate the strength of the evidence
January 2015
Analytic validity, Clinical validity, Clinical utility
Meleth, 201413 Prognosis in common cancers(N=0)
Technology assessment
Medline, Cochrane, EMBASE; gray literature
Yes Duplicate Yes QUADAS, AHRQ Methods Guide for Medical Tests
November 2013
Analytic validity, Clinical validity, Clinical utility

and for CE Reviews; RTI Question Bank
Terasawa, 201021
Pharmacogenetic tests to detect mutations that could affect cancer treatment with tamoxifen (N=16), anti-EGFR antibodies (N=47) and tyrosine kinase inhibitors (N=32)
Technology assessment
Medline, reference lists of included articles and reviews.
Yes Not Specified.
No (but listed KQs)
No quality standards for pharmaco-genetic tests 2009. Author did abstract information on study quality.
March 2010 Clinical validity, Clinical utility
Nelson, 201315 BRCA-related cancer(N=0)
Systematic Review
Medline, Cochrane Library, others
Yes Duplicate Yes USPSTF standards
December 2012
Clinical validity, Clinical utility
BCBSA TEC ReviewsGrant, August 20157
Developmental delay, including ASD (N=6)
Special Report Medline Yes Not Specified
No Not Described June 2015 Analytic validity, Clinical validity, Clinical utility
Piper, 201316 Whole-exome sequencing for suspected genetic disorders(N=0)
Special Report Medline Yes Not Specified
No Not Described July 2013 Clinical utility
Glacy, 20145 Effects of CYP2D6 testing of tamoxifen metabolism(N=0)
Special Report Medline Yes Not Specified
No Possible sources of bias; misclassification over-fitted models
November 2013
Analytic validity, Clinical validity,Clinical utility
Mark, 201411 Fecal DNA for colon cancer screening(N=0)
Special Report Medline Yes Not Specified
Yes Not Described September 2014
Clinical validity, Clinical utility
Glacy, 20146 GEP in breast cancer to select adjuvant therapy (N=1)
Assessment Medline, Google Scholar
Yes Single Reviewer
No Quality in Prognosis Studies Criteria
May 2014 Analytic validity, clinical validity, clinical utility
Ratko, 201518 GEP for prostate cancer management(N=0)
Assessment Medline Yes Not Specified
Yes Pepe criteria for biomarker assessment
September 2014
Analytic validity, Clinical validity, Clinical Utility
Mark, 201310 Molecular testing of Cancer to detect targeted therapy (N=3)
Special Report Medline Yes Not Specified
No Not Described March 2013 Clinical Utility
Piper, 201317 Maternal serum Assessment Medline and Yes Not Yes QUADAS-2 June 2014 Analytic validity,

testing for aneuploidies(N=0)
EMBASE Specified Clinical validity, Clinical utility
Ratko, 201419 DNA sequencing of maternal serum (N=0)
Not specified Medline and EMBASE
Yes Not Specified
No QUADAS-2 August 2015 Analytic validity, Clinical validity, Clinical utility
Cochrane ReviewsMarteau, 201012
DNA-based risk estimates and risky behaviors(N=7)
Review Medline, EMBASE, PsycINFO, CINAHL
Yes Duplicate No Cochrane Handbook for Systematic Reviews of Interventions
April 2010 Clinical Utility
Hilgart, 20128 Genetic risk of familial breast cancer(N=8)
Review MEDLINE, EMBASE, CINAHL, PsycLIT, CENTRAL,DARE, ASSIA, Web of Science, SIGLE and LILACS.
Yes Duplicate No CochraneCollaboration tool for assessing risk of bias
April 2011 Clinical Utility
*see included reviews list above for corresponding reference number**Definitions adapted from: Methods Guide for Medical Test Reviews. AHRQ Publication No. 12-EC017. Rockville, MD: Agency for Healthcare Research and Quality; June 2012. www.effectivehealthcare.ahrq.gov/reports/final.cfm.
Analytic validity: Ability of a test to conform to technical specifications, e.g. concordance of a genetic test with the true genotype. . Clinical validit y: Ability of a test to classify a patient into a disease/phenotype or prognosis category, e.g., sensitivity, specificity, likelihood ratios, area under the ROC
curve. Clinical utility : Ability of a test to direct clinical management and improve patient outcomes.
***This column indicates the types of validity/utility that the systematic review authors stated that they looked for in the included studies. In many cases, they looked for studies of clinical utility but did not find any, as indicated by the statement “no CU studies” in the second column from the left.
The QUADAS-2 instrument includes questions within 4 domains on the risk of bias, and 3 questions on the applicability of the studies. The domain summary questions and the applicability questions are each assigned a rating of average risk, high risk, or unclear.

Supplemental Materials Detailed SummariesAHRQ. Genetic Testing for Developmental Disabilities, Intellectual Disability and Autism Spectrum Disorder, 2015.Type Technical BriefCondition Autism/Developmental Delay
Condition Category Chronic Conditions other than cancer
Main objective Evaluates use of genetic testing to improve health outcomes in patients with developmental disabilities (DD) compared to standard-of-care diagnostic strategy. This Technical Brief collects and summarizes information on genetic tests clinically available in the United States to detect genetic markers that predispose to DDs. It also identifies, but does not systematically review, existing evidence addressing the tests’ clinical utility.
Comparator For assessing the clinical utility of a genetic test for determining the genetic etiology of ID, an appropriate comparator can be the standard-of-care diagnostic method without genetic testing. The standard-of-care method may include a physical examination by a clinician, a developmental assessment using standardized instruments (e.g., Wechsler Preschool and Primary Scale of Intelligence, Wechsler Intelligence Scales for Children, and Stanford-Binet Intelligence Scales), and other diagnostic tests (e.g., neuroimaging, metabolic studies).
Study Quality Assessment Methods
Described different ways to evaluate clinical utility of tests (RCTs with clinical outcomes; cross-sectional studies of sensitivity and specificity); described different outcome measures; described study design types which the authors seemed to use as a proxy for study quality; Did not evaluate study quality against study-specific pre-defined criteria.
Study Quality A small case-control study was the only one to address the clinical utility of genetic testing; it measured sensitivity and specificity. 20 studies addressed analytical validity (how accurately the test measured the analyte). 129 studies were case series to measure the diagnostic yield of genetic testing.
Primary Conclusions re: Patient Outcomes
The report did not identify any studies that directly assessed the impact of genetic testing on health outcomes. Most of the clinical studies identified for indirect assessment of clinical utility are case series reporting on a test’s diagnostic yield. The systematic review did not directly evaluate the quality of these studies.
Patient-Centeredness beyond Clinical Utility
Patient-centered health outcomes (e.g., functional or symptomatic improvement) and intermediate outcomes (e.g., changes in clinical decisions or family reproductive decisions, the tests’ diagnostic accuracy and analytic validity) are examined.
Scientific & Health Need
DDs are a group of conditions associated with functional impairment in physical, learning, language, or behavior areas. The causes of some developmental disabilities (e.g., Down syndrome, fragile X syndrome, fetal alcohol syndrome) are well understood. However, the underlying causes of many other DDs (e.g., autism spectrum disorder, intellectually disability) are often unclear and may vary substantially across individuals. Genetic abnormalities have been linked to many DDs. Studies suggest that up to 40 percent of DDs may be caused by some genetic aberration.
Illustrative CER Evidence Gaps & Potential Studies
- Small number of studies assessing genetic tests’ value perceived by families affected by DDs or addressing the impact of genetic testing on clinical management or family decisions. (e.g., psychosocial outcomes).
CDC testing tier Not in CDC Tier ListLink to Review http://effectivehealthcare.ahrq.gov/ehc/products/602/2095/genetic-testing-developmental-disabilities-
report-150629.pdf
AHRQ. Emerging Approaches to Diagnosis and Treatment of Non–Muscle-Invasive Bladder Cancer, 2015.Type Systematic ReviewCondition CancerCondition Category
Cancer: tumor profiling
Main objective Non–muscle-invasive bladder cancer (NMIBC) frequently recurs and can progress to muscle-invasive disease.. The purpose of this report is to review the currently available evidence on the comparative effectiveness of diagnostic tests and treatments for NMIBC.
Comparator Urine-based biomarkers have been developed as potential diagnostic alternatives or supplements to cytology, imaging, and cystoscopy. In addition urine-based biomarker tests may also be used to help identify recurrence and need for cystoscopy during surveillance.
Study Quality Assessment Methods
Assessed risk of bias in each study using criteria adapted from US Preventive Services Task Force. Rated diagnostic test study quality with QUADRAS-2 criteria. Two reviewers assessed quality independently. Rated risk of bias as low, medium, or high using criteria for these terms. Did not assess external validity (for which criteria do not exist). Graded strength of evidence using the approach described in the AHRQ Methods Guide (confidence that the evidence represents the true effect: high, moderate, low, insufficient)
Study Quality The over-all risk of bias was rated as medium for nearly all studies. The strength of evidence grade for studies of biomarker test performance were evenly divided between low and moderate. The strength of evidence grades for studies of the effects of intra-vesical treatments on outcomes were mostly low.
Primary Conclusions re: Patient Outcomes
No study evaluated the effectiveness of urinary biomarkers to decrease mortality or improve other outcomes compared with standard diagnostic methods or other urinary biomarkers in surveillance of patients treated for NMIBC. Urinary biomarkers are falsely negative in a substantial proportion of patients with bladder cancer, and additional research is needed to clarify advantages of fluorescent cystoscopy over white light cystoscopy.
Patient-Centeredness beyond Clinical Utility
We also evaluated adverse effects of diagnostic testing (e.g., false-positives, labeling, anxiety, complications of cystoscopy) and adverse effects of treatment (e.g., cystitis, urinary urgency, urinary frequency, incontinence, hematuria, pain, urosepsis, myelosuppression).
Scientific & Health Need
Bladder cancer is the 4th most commonly diagnosed cancer in men and the 10th most commonly diagnosed cancer in women in the United States. Biomarker tests may also be used to help identify recurrence and need for cystoscopy during surveillance.
Illustrative CER Evidence Gaps & Potential Studies
- Studies on how urinary biomarkers with cytology impacts use of cystoscopy and subsequent clinical outcomes- Randomized trials that adequately safeguard against performance bias- Effectiveness of risk-adapted approaches to guide selection of therapy, including use of nontraditional prognostic markers, effects of different surveillance intervals and protocols, and newer techniques such as electromotive administration of intra-vesical therapy
CDC testing tier Not in CDC Tier ListLink to Review http://effectivehealthcare.ahrq.gov/ehc/products/571/2137/bladder-cancer-non-muscle-invasive-report-
151025.pdf

AHRQ. Technology Assessment of Molecular Pathology Testing for the Estimation of Prognosis for Common Cancers, 2014.Type Systematic ReviewCondition CancerCondition Category
Cancer: tumor profiling
Main objective To conduct a systematic review and meta-analysis assessing the prognostic value and test performance (analytic validity, clinical validity, clinical utility, and harms) associated with 11 prognostic molecular pathology tests. Many of these tests are indicated for prediction of therapeutic responses, but this review focuses on their potential use as prognostic factors. Our overarching question was whether there is direct evidence that the addition of these molecular pathology tests changed physician decisionmaking and improved outcomes for adult patients.
Comparator No specific comparators were found in the review.Study Quality Assessment Methods
Assessed risk of bias in each study using criteria from the AHRQ Methods Guide. Rated diagnostic test study quality with QUADRAS-2 criteria. Two reviewers assessed quality independently. Rated risk of bias as low, medium, or high using criteria for these terms. Considered 4 domains: risk of bias, consistency, directness, and precision. Two reviewers independently evaluated quality of evidence. Graded strength of evidence using the approach described in the AHRQ Methods Guide (confidence that the evidence represents the true effect: high, moderate, low, insufficient).
Study Quality Evidence quality was low or insufficient for impact of testing on decision-making, except for MammaPrint and OncotypeDx Breast. Studies of prognostic accuracy had low to moderate risk of bias.
Primary Conclusions re: Patient Outcomes
Modest evidence supports added prognostic value (i.e., clinical validity) for over half of the tests evaluated, and that OncotypeDX Breast leads to changes in treatment decisions, but we found no evidence to determine whether using the tests to estimate prognosis leads to improved outcomes for patients. Even in the cases where the tests seemed to add value in determining prognosis (i.e., evidence of clinical validity), we found no evidence that using the test was related to improved outcomes for patients.
Patient-Centeredness beyond Clinical Utility
Evidence for OncotypeDX Breast showed an overall shift to less-intensive treatment recommendations, with fewer recommendations for chemotherapy (and therefore less exposure to potential harms of chemotherapy), but studies did not follow patients to actually report on harms or to assess the overall balance of clinical benefits and harms.
Scientific & Health Need
Molecular pathology tests that identify pathogenic mutations and cytogenetic translocations help us define the molecular subtypes of common cancers. It is unclear whether these test results can also serve as independent prognostic factors.
Illustrative CER Evidence Gaps & Potential Studies
- Future research should focus on quality of life, survival, and other health outcomes. There is no information on the differential effects of the test by race or cancer subtype (e.g., ductal versus lobular in breast cancer) or location (e.g., proximal versus distal in CRC).- Future research should take into account careful selection of the most appropriate endpoints, both in the context of the existing body of literature and the endpoints of most clinical relevance to doctors and patients. The weight of published research to date in the area of molecular pathology tests has focused on the clinical validity of the tests of interest in giving information about prognosis and little emphasis on how these tests can be integrated into the overall care of cancer patients in terms of measuring changes in management decisions or the effect of those altered decisions on downstream outcomes of value to patients
CDC testing tier OncoTypeDx Breast is Tier 1, others are tier 2 or tier 3 (unspecified)Link to Review http://www.cms.gov/Medicare/Coverage/DeterminationProcess/Downloads/id94TA.pdf

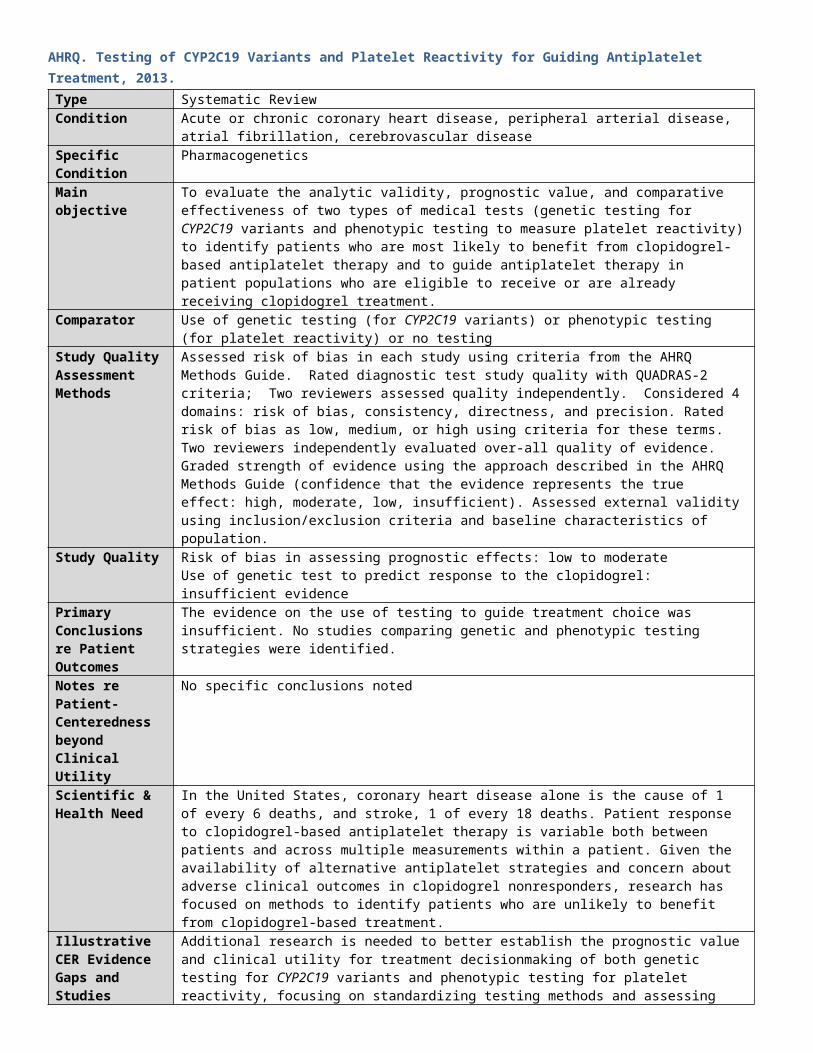
AHRQ. Testing of CYP2C19 Variants and Platelet Reactivity for Guiding Antiplatelet Treatment, 2013.Type Systematic ReviewCondition Acute or chronic coronary heart disease, peripheral arterial disease, atrial fibrillation, cerebrovascular
diseaseSpecific Condition PharmacogeneticsMain objective To evaluate the analytic validity, prognostic value, and comparative effectiveness of two types of medical
tests (genetic testing for CYP2C19 variants and phenotypic testing to measure platelet reactivity) to identify patients who are most likely to benefit from clopidogrel-based antiplatelet therapy and to guide antiplatelet therapy in patient populations who are eligible to receive or are already receiving clopidogrel treatment.
Comparator Use of genetic testing (for CYP2C19 variants) or phenotypic testing (for platelet reactivity) or no testingStudy Quality Assessment Methods
Assessed risk of bias in each study using criteria from the AHRQ Methods Guide. Rated diagnostic test study quality with QUADRAS-2 criteria; Two reviewers assessed quality independently. Considered 4 domains: risk of bias, consistency, directness, and precision. Rated risk of bias as low, medium, or high using criteria for these terms. Two reviewers independently evaluated over-all quality of evidence. Graded strength of evidence using the approach described in the AHRQ Methods Guide (confidence that the evidence represents the true effect: high, moderate, low, insufficient). Assessed external validity using inclusion/exclusion criteria and baseline characteristics of population.
Study Quality Risk of bias in assessing prognostic effects: low to moderateUse of genetic test to predict response to the clopidogrel: insufficient evidence
Primary Conclusions re Patient Outcomes
The evidence on the use of testing to guide treatment choice was insufficient. No studies comparing genetic and phenotypic testing strategies were identified.
Notes re Patient-Centeredness beyond Clinical Utility
No specific conclusions noted
Scientific & Health Need
In the United States, coronary heart disease alone is the cause of 1 of every 6 deaths, and stroke, 1 of every 18 deaths. Patient response to clopidogrel-based antiplatelet therapy is variable both between patients and across multiple measurements within a patient. Given the availability of alternative antiplatelet strategies and concern about adverse clinical outcomes in clopidogrel nonresponders, research has focused on methods to identify patients who are unlikely to benefit from clopidogrel-based treatment.
Illustrative CER Evidence Gaps and Studies
Additional research is needed to better establish the prognostic value and clinical utility for treatment decisionmaking of both genetic testing for CYP2C19 variants and phenotypic testing for platelet reactivity, focusing on standardizing testing methods and assessing the relative impact of testing strategies on patient-relevant clinical outcomes in large well-conducted clinical trials.
CDC testing tier Not in CDC Tier listLink to Review http://effectivehealthcare.ahrq.gov/search-for-guides-reviews-and-reports/?
pageaction=displayproduct&productID=1726

AHRQ. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: Systematic Review to Update the U.S. Preventive Services Task Force Recommendation, 2013.
Type Systematic ReviewCondition CancerCondition Category
Cancer Risk Assessment
Main objective To review new evidence on the benefits and harms of risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women.
Comparator Various general breast cancer risk stratification models were compared, as were various familial risk stratification models to predict individual risk for deleterious BRCA mutations in primary care settings.
Study Quality Assessment Methods
Quality of studies assessed by two independent investigators using the US Preventive Services Task Force predefined criteria for the specific study design. The investigators developed criteria for mutation penetrance. Assessed external validity using inclusion/exclusion criteria and baseline characteristics of population. Two reviewers independently evaluated over-all quality of evidence. Graded strength of evidence using the approach described in the AHRQ Methods Guide (confidence that the evidence represents the true effect: high, moderate, low, insufficient).
Study Quality This background systematic review for a US Preventive Services Task Force practice guideline addressed 5 separate key questions. The authors did not provide a quality rating over the entire body of evidence or for each key question; they did rate the quality of individual studies and systematic reviews.
Primary Conclusions re: Patient Outcomes
There were no studies that answered the question of whether risk assessment, genetic counseling and genetic testing lead to reduced incidence of BRCA-related cancer and reduced cause-specific and all-cause mortality. Risk assessment by nongenetics specialists using familial risk models to determine individual risks for BRCA mutations can accurately guide referrals for genetic counseling. A published systematic review of studies of 13 general breast cancer risk models, such as the Gail model, indicated that they are modest predictors of individual risk (c-statistic, 0.55 to 0.65) Results of genetic testing provide estimates of an individual’s chances of developing BRCA-related cancer depending on the specific test results.
Patient-Centeredness beyond Clinical Utility
Genetic counseling reduces distress, improves patients’ risk perception, and reduces their intentions for genetic testing. Overall, the accuracy of risk perception increased from an average of 42 percent accuracy before counseling to 58 percent after counseling. False-positive rates, unnecessary imaging, and unneeded surgeries were higher in women undergoing intensive screening using MRI versus mammography. Most women experienced no anxiety after breast cancer screening with MRI, mammography, or clinical breast examination.
Scientific & Health Need
Breast cancer is the second most common cancer in women in the United States, and is the second leading cause of cancer death. Ovarian cancer is the fifth leading cause of cancer death in women in the United States. Recent estimates indicate that clinically significant mutations in either of the BRCA genes increase a woman’s risk of breast cancer by age 70 years to 45 to 65 percent.BRCA1 mutations increase ovarian, fallopian tube, or peritoneal cancer risk to 39 percent, and BRCA2 mutations to 10 to 17 percent. These
mutations are estimated to occur in 1 in 300 to 500 women in the general population and account for 5 to 10 percent of breast cancer overall. Mutation testing of appropriate candidates could lead to increased awareness of cancer risk and effective use of interventions to reduce BRCA-related cancer incidence and mortality.
Illustrative CER Evidence Gaps & Potential Studies
- Research has focused on highly-selected women in referral centers and generally reported short-term outcomes. Limitations of studies included lack of predefined quality criteria, inadequate reporting of randomization technique, non-comparable groups at baseline, no specified eligibility criteria, high loss to follow-up and differences between comparison groups .Issues such as access to testing; effectiveness of screening approaches, including risk stratification; use of system supports; and patient acceptance and education require additional study. Additional data from women of varying socioeconomic, racial, and ethnic groups are needed.- Who should perform risk assessment and genetic counseling services, how it should be done, and what skills are needed are unresolved questions. Trials comparing types of providers and protocols could address these issues.- What happens after patients are identified as high-risk in clinical settings is unknown. The consequences of genetic testing for individuals and their relatives require more study. Well-designed investigations that use standardized measures and enroll subjects who reflect the general population, including minority women, are needed.- An expanded database or registry of patients who receive genetic counseling and testing for BRCA mutations would provide essential information about predictors of cancer, response to interventions, and other modifying factors.
CDC testing tier Tier 1Link to Review http://www.ncbi.nlm.nih.gov/books/n/es101/pdf/

AHRQ. PCA3 Testing in the Diagnosis and Management of Prostate Cancer: Future Research Needs, 2013.Type Systematic ReviewCondition CancerCondition Category
Cancer: tumor profiling
Main objective Generate prioritized topics for future research on PCA3 testing (urine based molecular testing) for the diagnosis and management of prostate cancer (conducted for EGAPP)
Comparator Comparators included other measures of PSA (total prostate specific antigen (PSA) elevations, free PSA, PSA density, PSA velocity, externally validated nomograms, complexed PSA, and multivariate models).
Study Quality Assessment Methods
Quality of studies assessed by two independent investigators using the US Preventive Services Task Force AHRQ Methods Guide. Studies of diagnostic accuracy assessed using the QUADAS tool and rated good, fair, or poor. Assessed external validity using inclusion/exclusion criteria and baseline characteristics of population. Strength of evidence for outcomes measured with GRADE criteria, which address risk of bias, consistency, directness, and precision as good, moderate, low, or insufficient. Two reviewers independently evaluated quality of evidence and resolved differences through discussion.
Study Quality Decision about biopsy: poor or insufficient evidenceAccuracy of PCA3 and PSA: low for accuracy comparison and insufficient for impact on health outcomes
Primary Conclusions re: Patient Outcomes
PCA3 is more discriminatory for detecting cancers (i.e., at any sensitivity, the specificity is higher, or at any specificity, the sensitivity is higher) than tPSA elevations; however, strength of evidence was low. For all other diagnostic accuracy comparisons, and all intermediate and long-term health outcomes, the strength of evidence was insufficient. In patients with a positive biopsy for cancer who are being evaluated to distinguish between insignificant/indolent and aggressive disease, the strength of evidence on the effectiveness of PCA3 testing (alone or in combination) was insufficient.
Patient-Centeredness beyond Clinical Utility
The pros and cons of prostate cancer screening are impacted by any diagnostic or demographic information that will help physicians and their patients at risk for prostate cancer to make more informed decisions about biopsy.
Scientific & Health Need
Cancer of the prostate is the second most common cancer and the second leading cause of cancer deaths in men in the United States. Most patients have slow-growing tumors, and may live for years with no or minimal effects, ultimately dying of other causes. A challenge in managing clinically localized disease is distinguishing between men who have aggressive disease and need immediate therapy, and those who have less aggressive disease that can be safely managed by active surveillance.
Illustrative CER Evidence Gaps & Potential Studies
- Questions include: How much improvement in diagnostic accuracy is needed for any new test to impact biopsy decision making? What is the potential of adding PCA3 alone or with other biomarkers to change decision making in practice? How does PCA3 compare with the two more frequently used add-on tests (free PSA, PSA velocity) that have appeared in guidance documents?- Need for matched studies not derived from “convenience” populations (e.g., biopsy referral centers), and more data on how key demographic factors (family history, race) impact on the performance of PCA3 and comparators.- Need for outcome studies to determine how well PCA3 and other comparators used to categorize risk as insignificant/indolent or aggressive to predict the behavior of tumors over time.- Studies should address a range of methodological and statistical questions relating to modeling, assessing impact of verification bias, identifying most effective cutoffs for tests based on ROC analysis, and designs for future studies.
CDC testing tier Not in CDC tier listLink to Review http://effectivehealthcare.ahrq.gov/ehc/products/307/1449/prostate-cancer-antigen-3-gene.pdf

AHRQ. Technology Assessment on Genetic Testing or Molecular Pathology Testing of Cancers with Unknown Primary Site to Determine Origin, 2013.
Type Systematic ReviewCondition CancerCondition Category
Cancer: tumor profiling
Main objective To review the existing literature on commercially available genetic tests that are used to identify the tissue of origin (TOO) of the cancer in patients with cancer of unknown primary (CUP) site. This review focused on analytical and clinical validity of the tests and their utility in guiding the diagnosis and treatment of CUP and improving health outcomes.
Comparator Cytogenetic analysis and three genomic TOO tests (CancerTypeID, miRview, and PathworkDx)Study Quality Assessment Methods
Risk of bias in studies: used the criteria described in AHRQ Methods Guide. Studies of diagnostic accuracy assessed using the QUADAS tool and rated good, fair, or poor. Used Simon criteria to assess the validity of the development of statistical classification algorithms. Assessed clinical applicability using questions from the RTI International Question Bank. Overall quality of evidence judged by two independent investigators using criteria for risk of bias, precision, directness, and consistency.
Study Quality Genomic tests for tissue of origin effect on diagnosis: moderateEffect on treatment decisions or survival of patients: lowEffect on patient outcomes: insufficient
Primary Conclusions re: Patient Outcomes
We reviewed four tests for analytical validity, clinical validity, and clinical utility. The evidence that the TOO tests contributed to the diagnosis of CUP was moderate. There is insufficient evidence to assess the effect of the tests on treatment decision and outcomes.
Patient-Centeredness beyond Clinical Utility
Because tissue-specific therapy would be the standard of care for a patient with a tissue-specific diagnosis, ethical considerations would probably rule out a controlled trial that randomized patients with tissue-specific diagnoses from a TOO test into empiric therapy or tissue-specific therapy.
Scientific & Health Need
Cancer is one of the leading causes of death in the United States. In order to design the most effective treatment regimen for a patient with metastatic cancer, it is important to know the site of the primary tumor or at least the cancer cell type. ACS estimated that there are >30K cases of CUP annually in US.
Illustrative CER Evidence Gaps & Potential Studies
- The most urgent need in the literature is to have the clinical utility of the tests evaluated by research groups that have no evident conflict of interest. Given the difficulty of assessing the accuracy of the TOO in CUP cases, future research should focus on the benefits from the test to the patient in terms of effect on treatment decisions and resulting outcomes.- Studies have small samples, varied study designs and measures of effect on treatment decisions, making it difficult to draw conclusions on any of the tests. Most use historical controls.
CDC testing tier Not in CDC tier listLink to Review http://www.cms.gov/Medicare/Coverage/DeterminationProcess/Downloads/id90TA.pdf
Notes Most studies included in the current review were funded wholly or partially by the manufacturers of the tests

AHRQ. Fecal DNA Testing in Screening for Colorectal Cancer in Average-Risk Adults, 2013.Type Systematic ReviewCondition CancerCondition Category
Cancer Risk Assessment
Main objective To review the evidence on fecal DNA testing to screen for colorectal cancer in adults at average risk for colorectal cancer.
Comparator Fecal DNA testing is intended for individuals who are not eligible (either unable or unwilling) for more invasive CRC screening (i.e., colonoscopy, flexible sigmoidoscopy, or CT colonography). Screening colonoscopy results provided the reference standard for evaluation of fecal DNA testing.
Study Quality Assessment Methods
Study quality judged by two independent investigators using the study design-specific quality of the US Preventive Services Task Force. Also used Evaluation of Genomic Applications in Practice and Prevention for genetic testing, the Newcastle Ottawa Scale for cohort studies, and the QUADAS criteria for diagnostic testing and rated good, fair, or poor.
Study Quality Analytic validity (repeatability, reproducibility, and analytic specificity: poorAcceptability and adherence: fair to poor.Comparison with immunochemical tests for fecal blood: no studies.
Primary Conclusions re: Patient Outcomes
There is insufficient evidence for the harms, analytic validity, and acceptability of testing in comparison to other screening modalities. Existing evidence has little or no applicability to currently available fecal DNA testing.
Patient-Centeredness beyond Clinical Utility
From very limited evidence, it appears that fecal DNA testing is generally acceptable, although an important test attribute for acceptability appears to be the test’s accuracy. No studies have evaluated the relative acceptability or adherence of fecal DNA tests to fecal immunochemical test (FIT) tests.
Scientific & Health Need
Colorectal cancer (CRC) is the third most common cancer in both men and women and is the third
leading cause of cancer deaths in the United States. However, screening rates remain suboptimal. Currently, only one fecal DNA test, ColoSure, is commercially available.
Illustrative CER Evidence Gaps & Potential Studies
- The most critical evidence gap for fecal DNA testing to screen for CRC is the lack of appropriately designed diagnostic accuracy studies applicable to currently available fecal DNA testing.- When better-quality, more-applicable diagnostic accuracy studies in screening populations become available, clinicians and decision makers can use robust models to estimate net benefit of testing and optimal intervals of testing, compared to other currently used or promising screening modalities.- Other important evidence gaps include the relative acceptability of and adherence to fecal DNA testing, compared with FIT (which is a stool based test that does not require dietary or medication restrictions), and issues around fecal DNA testing analytic validity, specifically accuracy, and repeatability and reproducibility.
CDC testing tier Not in CDC Tier ListLink to Review http://effectivehealthcare.ahrq.gov/ehc/products/282/971/CER52_Fecal-DNA-
Testing_FinalReport_20120229.pdf

AHRQ. Gene Expression Profiling (GEP) for Predicting Outcomes in Stage II Colon Cancer, 2012.Type Technical BriefCondition CancerCondition Category
Cancer: tumor profiling
Main objective The objective of this Technical Brief is to provide a summary of the state of the science on use of GEP in predicting outcomes, including benefit from adjuvant chemotherapy, in patients with stage II colon cancer.
Comparator GEP assays are being studied as a better way to identify risk of disease recurrence (prognostic marker) and/or benefit from adjuvant therapy (predictive marker) than existing approaches. The existing approaches generally use information that is routinely obtained from the surgical procedure (presence of bowel perforation) and histological examination of the tumor (e.g., perivascular invasion by tumor). Use of the GEP assays will not replace these standard procedures.
Study Quality Assessment Methods
This study did not assess the quality of the studies
Study Quality Not assessed.
Primary Conclusions re Patient Outcomes (clinical utility/morbidity & mortality)
The clinical utility is uncertain. No prospective studies have reported on what happens to net health outcome, considering both benefits and harms, when GEP results are used in managing patients. Data are also very limited for net reclassification analysis; that is, how the overall risk classification provided by GEP results compares with risk classification using other predictors. Most of the studies have evaluated the GEP assays as a possible prognostic marker for disease recurrence. There is much less information regarding use as a predictive marker for response to adjuvant chemotherapy, which would impact patient management.
Notes re Patient-Centeredness beyond Clinical Utility
Identifying patients who do not need adjuvant chemotherapy because of very low risk of recurrence or predicted lack of benefit from adjuvant chemotherapy would improve the net health outcome by avoiding treatment-related adverse effects. On the other hand, introducing routine testing without a clear understanding of benefits and risks could result in those who would benefit from adjuvant therapy not receiving it.
Scientific & Health Need
Colon cancer is a common malignancy affecting both women and men. The most important prognostic factor for colon cancer is stage at diagnosis. While adjuvant chemotherapy is recommended in patients with stage III colon cancer, its role in stage II disease is unclear.
Illustrative CER Evidence Gaps
- Compared to conventional risk stratification, can prognostic GEP assays identify individual patients at low risk of recurrence who can safely avoid adjuvant chemotherapy? Can GEP assays identify individual patients who will show improved survival with adjuvant chemotherapy or particular adjuvant regimens?- Which patients with stage II colon cancer should be tested using the GEP assay? All stages? Subsets such as those whose tumors do not have microsatellite instability?
CDC testing tier Not on CDC Tier TableLink to Review http://effectivehealthcare.ahrq.gov/ehc/products/434/1366/
TechnicalBrief13_GeneExpressionProfiling_FinalReport_20130110.pdfNotes Vast majority of studies have focused on use of GEP assays as a prognostic marker (relationship between
test result and recurrence of cancer or survival). Predictive assays are especially important in that their use could result in improved survival. Predicting the two types of outcomes may require different GEP signatures.
Test may be add-on vs. substitute for other testing
AHRQ. Systematic Reviews on Selected Pharmacogenetic Tests for Cancer Treatment: CYP2D6 for Tamoxifen in Breast Cancer, KRAS for anti-EGFR antibodies in Colorectal Cancer, and BCR-ABL1 for Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia, 2010.
Type Systematic ReviewsCondition CancerCondition Category
Cancer: tumor profiling OR Pharmacogenetics
Main objective Assesses the evidence on the benefits and harms of three pharmacogenetic tests for treatment: CYP2D6 for Tamoxifen in Breast Cancer, KRAS for anti-EGFR antibodies in Colorectal Cancer, and BCR-ABL1 for Tyrosine Kinase Inhibitors (TKIs) in Chronic Myeloid Leukemia (CML)
Comparator There were no comparators for CYP2D6 for Tamoxifen in Breast Cancer. The comparator for KRAS mutation testing for response to treatment with anti-EGFR antibodies in Colorectal Cancer was not testing. However the design for many of the studies was “retrospective-prospective”, meaning that testing was done on archival samples so it was a typically randomized design. There were no comparators for BCR-ABL1 for TKIs in CML.
Study Quality Assessment Methods
There are no validated quality criteria for pharmacogenetics studies. Authors did abstract information on the design of individual studies (sampling, study design, diagnostic accuracy measures (sensitivity and specificity). Did not use any validated quality criteria sets but did assess study adherence to good statistical and epidemiological practice.
Study Quality This review? was more sophisticated than the others. Without rating the study quality, the analysis conveyed the authors’ analytic skills which increased confidence in their conclusion. Most studies were under-powered. Studies assumed that the genetic abnormality had no effect in untreated patients. There were enough randomized trials of KRAS mutation testing to show that anti-EGFR therapy was more effective in those with the mutation than those without.
Primary Conclusions re: Patient Outcomes
There were no consistent associations between CYP2D6 polymorphisms and outcomes in tamoxifen treated women with breast cancer. When treated with anti-EGFR antibodies, patients with KRAS mutations were less likely to experience treatment benefit, compared to patients whose tumors were wild-type for KRAS mutations, for all outcomes assessed. Although few studies were conducted in the first line setting, for all outcomes and particularly for treatment failure, the predictive ability of KRAS mutations was lower compared to that observed in pre-treated patients. Regarding the two different agents, cetuximab and panitumumab, the predictive ability of KRAS mutations appeared to be similar. The presence of any BCR-ABL1 mutation does not appear to predict differential response to TKI treatments There is consistent evidence that presence of the relatively rare T315I mutation can predict TKI treatment failure, mainly in terms of hematologic and cytogenetic response.
Patient-Centeredness beyond Clinical Utility
There was no evidence of harms associated with testing and its downstream effects.
Scientific & Health Need
Several variant alleles of the CYP2D6 gene have different enzymatic activity and can potentially affect the pathway and metabolite transformation, potentially impacting on patients’ response to tamoxifen treatment. Cetuximab targets epidermal growth factor receptor (EGFR), a member of the subclass I of the receptor tyrosine kinase superfamily, which is overexpressed in up to 80 percent of colorectal cancers. Panitumumab is a similarly acting drug. Specific mutations in BCR-ABL1 have been shown to confer resistance to imatinib both in vitro and in vivo, by affecting the binding of the drug to the tyrosine kinase enzyme.
Illustrative CER Evidence Gaps & Potential Studies
- Studies often had small sample sizes and thus would not be able to reliably identify effects as small as those anticipated for most pharmacogenetic tests or effects determined by rare genetic variations.- Most studies assessed surrogate short term outcomes of treatment failure, as defined by imaging or laboratory measurements. Data on the clinical outcomes of overall or progression-free survival are sparse.- We documented extensive heterogeneity in way genetic factors were grouped and analyzed across the included studies. Adjustments for potential confounding factors were often not based on sound epidemiological principles. Adjustments for multiple comparisons were not documented in the included studies.- Multiple studies on each topic frequently originated from a limited number of specialized centers, posing problems in identifying nonoverlapping populations, and potentially threaten the generalizability of the findings.
CDC testing tier CYP2D6 for Tamoxifen in Breast Cancer – CDC Tier 2; KRAS for anti-EGFR antibodies in Colorectal Cancer - CDC Tier 1; BCR-ABL1 for TKIs in CML – CDC Tier 1 or Tier 2 depending on the chemotherapy agent
Link to Review http://www.cms.gov/medicare-coverage-database/details/technology-assessments-details.aspx?TAId=76&bc=BAAgAAAAAAAA&

BCBS TEC. Special Report: Chromosomal Microarray for the Genetic Evaluation of Patients With Global Developmental Delay, Intellectual Disability, and Autism Spectrum Disorder, 2015.
Type Technology AssessmentCondition Developmental DelayCondition Category
Chronic Conditions other than cancer
Main objective Summarize the evidence on chromosomal microarray testing to identify copy number variations (CNVs) in children with global developmental delay(GDD),intellectual disability (ID), and autism spectrum disorder (ASD).
Comparator There was no comparison to other technologies or methodologies.Study Quality Assessment Methods
Did not use validated, commonly used instruments for evaluating the quality of studies. Did use a specified search strategy.
Study Quality No systematic assessment of the strength of the evidence.
Primary Conclusions re: Patient Outcomes
The studies found identified pathogenic variants can prompt clinical actions potentially impacting morbidity. Less clear is how often outcomes will be improved and in which cases interventions might have occurred in the absence of testing. The strong expert opinion in recommending initial CMA testing over other approaches, together with the indirect evidence for benefit following testing, supports concluding that the net health outcome can be improved.
Patient-Centeredness beyond Clinical Utility
Having a child affected by ASD, and likely GDD/ID, can affect reproductive decision making. For families that desire a genetic diagnosis and what might follow from one, CMA testing can establish a diagnosis more often than other approaches such as karyotyping. Still, other assays will identify some genetic abnormalities not detected by an array. There are also likely circumstances where other family members may be impacted owing to the nature of the variant and subsequent cascade (family member) testing. The downsides to testing can include detecting nonpaternity, an incorrect diagnosis, and findings of uncertain significance.
Scientific & Health Need
Prevalence estimates of GDD and ID range from 1% to 3%. In 2010, the estimated prevalence ASD among 8- year-olds was 14.7 per 1000. The goal of a genetic evaluation is to identify chromosomal imbalances that cause a disorder.
Illustrative CER Evidence Gaps & Potential Studies
- End-to-end cohort studies of children from presentation to outcomes have not been reported. There are considerable challenges conducting studies of sufficient size given the underlying genetic heterogeneity, and including follow-up adequate to observe final health outcomes.- Studies examining clinical utility have reported intermediate outcomes and indirect evidence.
CDC testing tier Not in CDC Tier ListLink to Review Pending Update to BCBSA Website

BCBS TEC. Noninvasive Prenatal Cell-Free Fetal DNA-Based Screening for Aneuploidies Other Than Trisomy 21, 2014.Type Technology AssessmentCondition Prenatal
Condition Category
Prenatal/newborn/children
Main objective To determine whether DNA sequencing based testing for T13, T18, and Sex Chromosome Aneuploidies (SCA) using cell-free fetal DNA improves net health outcomes compared with a traditional combined serum- and ultrasound-based screening strategy
Comparator DNA sequencing based testing for T13, T18, and SCA using cell-free fetal DNA as compared with a traditional combined serum- and ultrasound-based screening strategy.
Study Quality Assessment Methods
The body of the report was about diagnostic accuracy of the tests. Used QUADAS-2 criteria to assess diagnostic test study quality. Used a simple decision model to estimate effects of screening.
Study Quality Most diagnostic test studies had a low risk of bias in the patient flow domain, the index test domain, and the reference test domain. One problem was poorly described processes for selecting the controls for case-control studies, and the diagnostic reference standard domain.
Primary Conclusions re: Patient Outcomes
A decision model showed that the use of sequencing-based cell-free fetal DNA screening increased the number of detected cases of T13 and T18, with commensurate reduction of missed cases, compared with standard integrated screening procedures for those parameters, in high- and average-risk (general obstetric) populations of pregnant women. Evidence is insufficient to determine the clinical benefit of cell-free fetal DNA-based screening for SCA compared with traditional tests
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility
Scientific & Health Need
Fetal chromosomal abnormalities occur in approximately 1 in 160 live births. As early as 8 to 10 weeks of gestation, cell-free fetal DNA fragments may comprise 6% to 10% or more of the total cell-free DNA in a maternal plasma sample. DNA sequencing is highly accurate for prenatal detection of T21. The methods used to screen for T21 have been extended to other less common aneuploidies (primarily T13 and T18), as well as the most common SCA (45, X; 47, XXY;47, XYY).
Illustrative CER Evidence Gaps & Potential Studies
- Studies to compare all potential screening strategies such as serum screening and ultrasound followed by cell-free DNA or cell-free DNA plus subsequent serum screening and ultrasound to examine which might be optimal.
CDC testing tier Not in CDC Tier ListLink to Review Pending Update to BCBSA Website

BCBS TEC. Gene Expression Analysis for Prostate Cancer Management, 2014.Type Technology AssessmentCondition CancerCondition Category
Cancer: Tumor profiling
Main objective To evaluate evidence on gene expression profiling tests, specifically Prolaris and OncotypeDx Prostate
Comparator Gene expression testing compared with clinical criteriaStudy Quality Assessment Methods
Used REMARK (Reporting Recommendations for Tumor Marker Prognostic Studies) to assess tests ability to predict tumor histologic aggressiveness. Found that the US Preventive Services Task Force criteria did not apply to these tests. Instead, they used Pepe’s criteria for evaluating biomarker tests.
Study Quality The article does not describe how well the two tests adhered to the Pepe or REMARK criteria, nor did it make any summary statements about study quality.
Primary Conclusions re: Patient Outcomes
We evaluated published evidence on use of two available tests in combination with current clinical criteria (Gleason score, PSA serum levels, clinical stage) to further stratify biopsy-diagnosed, localized prostate cancer. Such information would assist in initial clinical disease management, specifically to decide whether a patient should proceed to definitive therapy (ie, surgery) or could safely proceed to active surveillance. Published evidence is sparse and insufficient to draw conclusions on the analytic validity, clinical validity, or clinical utility of Prolaris, and is insufficient to determine the clinical validity or utility of OncotypeDx® Prostate in patients under active surveillance program.
Patient-Centeredness beyond Clinical Utility
An individual patient could use the findings to assess his balance of benefits and harms (net benefit) when weighing the choice to proceed immediately to curative treatment with its attendant adverse sequelae, or deciding to enter an active surveillance program. The latter would have an immediate benefit realized by forgoing surgery, but could be associated with greater downstream risks of disease progression and subsequent therapies.
Scientific & Health Need
Prostate cancer is the second most common cancer diagnosed among men in the United States. Given the unpredictable behavior of localized prostate cancer, prognostic tests to guide patient management are under investigation.
Illustrative CER Evidence Gaps & Potential Studies
- Does either test provide actionable patient management information beyond that provided by established clinical criteria to direct patient management? Classification and reclassification must be sufficiently robust to alleviate concerns over balancing uncertain relative risks of treatment related morbidities and rapid disease progression to incurability. It is also unclear whether either test would need to be repeated in patients under active surveillance to evaluate possible changes in cancer behavior based on progressive genotypic and phenotypic alterations.
CDC testing tier CDC Tier 3Link to Review Pending Update to BCBSA Website

BCBS TEC. Gene Expression Profiling in Women With Lymph Node‒Negative Breast Cancer to Select Adjuvant Chemotherapy, 2014.
Type Technology AssessmentCondition CancerCondition Category
Cancer: tumor profiling
Main objective To examine whether, compared with conventional risk assessment tools or when used in conjunction with conventional risk assessment tools, gene expression profiling improves outcomes for women who decide that recurrence risk is low enough to forgo adjuvant chemotherapy for node-negative, HR-positive, early stage breast cancer and for women who otherwise may not have received adjuvant chemotherapy.
Comparator Gene expression profiling, compared with conventional risk assessment tools or when used in conjunction with conventional risk assessment tools. This Assessment evaluates 3 tests that were reviewed in previous TEC Assessments and a fourth test (Prosigna) that has recently received marketing clearance from the U.S. Food and Drug Administration.
Study Quality Assessment Methods
A single reviewer assessed study quality by applying Quality in Prognosis Studies criteria (study participation, study attrition, prognostic factor management, outcome measurement, study confounding, and statistical analysis and reporting).
Study Quality Rated over-all risk of bias as low to moderate; study participation as unbiased; risk of bias moderate for measurement of prognostic factors; adequate for assessment for confounding; and moderate for statistical reporting (due to failure to report confidence intervals for outcomes of interest).
Primary Conclusions re: Patient Outcomes
Retrospective epidemiologic analyses indicated strong, independent associations between Oncotype DX® recurrence score (RS) results and distant disease recurrence or death from breast cancer. Thus, the evidence was judged sufficient to permit conclusions regarding probable health outcomes. The evidence is insufficient to permit conclusions regarding health outcomes for Mammaprint, Breast Cancer Index, and Prosigna.
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility
Scientific & Health Need
For women with early-stage, invasive breast cancer, adjuvant chemotherapy consistently provides an approximate 30% relative risk reduction in 10-year breast cancer mortality regardless of prognosis. However, the magnitude of absolute benefit from chemotherapy depends on baseline risk of recurrence. If these patients could be accurately identified, they could avoid chemotherapy and its toxicity. Current risk classifiers do not accurately identify early-stage patients who are at low risk of recurrence; as a result, more patients receive chemotherapy than can benefit. Several groups have identified panels of gene expression markers (“signatures”) that appear to predict the risk of breast cancer recurrence after surgery, radiation therapy, and hormonal therapy (for HR-positive tumors) in women with node-negative disease.
Illustrative CER Evidence Gaps & Potential Studies
- Among those willing to be guided by the test result, it is unknown what proportion of conventionally estimated intermediate- to high-risk patients will have sufficiently low RS values to change their decision regarding chemotherapy.- How the recurrence risk level below which women might choose to forgo chemotherapy is affected by patient preferences, needs, and values is unknown.- Women reclassified by RS result as intermediate or high risk from conventionally estimated low risk have a much wider range of recurrence risk estimates; women with very high RS values are likely to benefit from accepting chemotherapy; but for the intermediate-risk group, benefits are uncertain.- Because RS is a continuous function with respect to recurrence rates, risk category cutoff values selected by the test developer may not be optimal.
CDC testing tier CDC Tier 2Link to Review Pending Update to BCBSA Website

BCBS TEC. Fecal DNA Analysis for Colorectal Cancer Screening, 2014.Type Technology AssessmentCondition CancerCondition Category
Cancer Risk Assessment
Main objective To evaluate fecal DNA testing as a strategy for colorectal cancer screening. The specific test reviewed (Cologuard) combines both fecal DNA markers and an immunochemical hemoglobin assay, assessed in one study (Imperiale et al, 2014).
Comparator Fecal immunochemical testing (FIT) and screening colonoscopyStudy Quality Assessment Methods
The report describes several desirable characteristics of the sole study. It does not rate them according to QUADAS-2 or another validated set of quality criteria for studies of diagnostic tests, so the word “good” is a subjective judgment rather than reflecting a standard of methodologic rigor that others would necessarily agree with.
Study Quality Rated the sole study of a currently marketed test as “good.” It was a cross-sectional study measure sensitivity and specificity of fecal DNA (the gold standard was colonoscopy) for various precancerous lesions and cancer.
Primary Conclusions re: Patient Outcomes
The diagnostic characteristics of the test (higher sensitivity but lower specificity than FIT) are consistent with reduced colorectal cancer mortality if used in a longitudinal screening program. However, it remains to be determined how effective the test would be when used at a particular frequency within a screening program, and thus its efficacy and impact on resource use compared with established methods are unknown.
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility
Scientific & Health Need
Colorectal cancer is the third most common type of cancer in terms of incidence and mortality in both men and women in the United States. Studies have also shown that colorectal cancer screening is not optimally utilized in the United States, with both under- and overutilization of all cancer screening methods, including more frequent colonoscopy screening than is recommended. Because malignant cells are continuously exfoliated, fecal DNA testing offers the potential for greater sensitivity for detecting cancer than FOBT, which relies on detecting intermittently released occult blood. Various screening methods for colorectal cancer in persons at average risk are available, including several types of fecal DNA tests. Imperiale et al (2014)1 published results of a fecal DNA test study in a large screening population. Their results supported the U.S. Food and Drug Administration approval of a specific test (Cologuard) in August 2014.
Illustrative CER Evidence Gaps & Potential Studies
- An uncertainty regarding the effectiveness of fecal DNA testing is patient adherence to (1) the recommended screening interval and (2) follow-up to positive tests.- Formal modeling studies of the fecal DNA test are needed to estimate the efficacy of the test in preventing colorectal cancer and to help determine the optimal strategy for its use.
CDC testing tier Not in CDC Tier ListLink to Review Pending Update to BCBSA Website

BCBS TEC. Special Report: Multiple Molecular Testing of Cancers to Identify Targeted Therapies, 2013.Type Technology AssessmentCondition CancerCondition Category
Cancer: tumor profiling
Main objective To review important concepts underlying the use of multiple molecular testing to guide cancer treatment, using published studies.
Comparator None notedStudy Quality Assessment Methods
No formal assessment of the quality of the 4 studies that were cited. Two had controls who got “unmatched” treatment. Two did not have controls. The state of the evidence appeared so weak that an assessment against validated criteria sets was beside the point.
Study Quality The report drew conclusions about the sufficiency of the evidence based on the type of studies that had been done to evaluate these tests, but did not describe the quality of the studies other than the presence or absence of controls that did not get therapy matched to the mutation that they had.
Primary Conclusions re: Patient Outcomes
Strong evidence of clinical effectiveness of this approach is not available, and a number of issues remain to be solved, particularly patient selection. It appears that the utility of molecular marker profiling of cancer using multiple molecular markers for the purpose of determining treatment, beyond the few molecular markers that have been established as predictors of treatment, is a story in progress.
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility.
Scientific & Health Need
Cancer poses a substantial health burden in the U.S.. Overall, cancer is the second most common cause of death in the U.S., exceeded only by heart disease, accounting for nearly 25% of deaths annually. There is interest in the utility of measuring a large number of molecular markers at a single time in order to identify a treatment which targets the biological pathway involving that molecular marker.
Illustrative CER Evidence Gaps & Potential Studies
- Studies assessing the efficacy of molecular marker profiling will be challenging, as critical problems in reproducibility of treatment assignment, small numbers of patients in classifiable subgroups, and heterogeneity of patients within studies will need to be solved.- Which patients should be selected for study is an important issue.- A number of practical issues pertinent to application of molecular marker profiling have not been sufficiently resolved to incorporate this strategy into routine clinical care.- Optimal informatics methods to handle large amounts of sequencing data and reconstruct them into clinically actionable information displays remain problematic..
CDC testing tier Multiple CDC Tiers 1-3Link to Review Pending update to BCBSA Website

BCBS TEC. Special Report: Exome Sequencing for Clinical Diagnosis of Patients with Suspected Genetic Disorders, 2013.Type Technology AssessmentCondition Non-SpecificCondition Category
Other
Main objective Compares Sanger sequencing and next-generation sequencing clinical molecular methods targeted on the protein coding region of the genome rather than the entire genome and used for diagnosing disorders that are caused by mutations in a single gene.
Comparator Sanger sequencingStudy Quality Assessment Methods
The study design was case series, in which patients with a disease known to be caused by a mutation in a gene underwent DNA sequencing to discover mutations in different places on the gene. The primary endpoint was the yield of such mutations. The purpose of the studies appeared to be proof of concept. There are no quality criteria developed for exome sequencing, so assessment of study quality was not possible.
Study Quality Not applicable.Primary Conclusions re: Patient Outcomes
Beyond diagnostic yield, occasional anecdotal reports were identified of clinical benefit following molecular diagnosis by exome sequencing. Such potential benefits included a revision of the original diagnosis; a few instances of treatments initiated or discontinued as a result of the known functional consequences of the mutation, and genetic counseling to the affected patient and/or family members. However, no systematic study of clinical outcomes was identified. Studies of exome sequencing compared with traditional Sanger sequencing generally agree that exome sequencing is more efficient and more likely to result in a diagnosis.
Patient-Centeredness beyond Clinical Utility
For some patients, exome sequencing obtained after initial diagnostic evaluation (that may include other genetic testing) has failed may avoid the diagnostic odyssey and return a likely causal variant. Reproductive decisions for parents considering an additional pregnancy may be informed by determining the mode of inheritance.
Scientific & Health Need
Disorders (often early developmental) that present with multiple anomalies suggest a genetic etiology. The number of rare diseases has been estimated at 5,000 to 8,000 (IOM, 2010), and is rapidly growing. These disorders are often clinically difficult to diagnose due to nonspecific presentation, potentially overlapping differential diagnoses (clinical heterogeneity) or a rare disorder, and lack of a clear diagnostic testing path. The search for a clinical diagnosis may result in a long (months to years) diagnostic odyssey comprising several specialist consults and many different individual molecular, cytogenetic and biochemical tests, as well as other types of diagnostic procedures. A relatively unbiased sequencing application that examines most genes without requiring prior knowledge of potential diagnoses would be advantageous. Exome sequencing using next-generation technology has recently become available as a laboratory-developed diagnostic clinical laboratory test.. Currently, the diagnostic yield appears to be no greater than 50% and possibly less for patients with suspected genetic disorder accompanied by multiple anomalies.
Illustrative CER Evidence Gaps & Potential Studies
There are ethical questions about reporting incidental or off-target findings. For example, exome sequencing may be ordered to aid in diagnosis of a developmental syndrome in a young child; in addition to answering the diagnostic question, a medically relevant variant such as a BRCA1/2 gene mutation may be discovered, which predicts a very high risk of breast cancer and ovarian cancer at an adult age.
CDC testing tier CDC Tier 2 and 3Link to Review Pending Update to BCBSA Website
BCBS TEC. CYP2D6 Pharmacogenomics of Tamoxifen Treatment, 2013.Type Technology AssessmentCondition CancerCondition Category
Pharmacogenetics
Main objective Evaluates evidence for CYP2D6 genotyping, compared with no testing, to direct treatment regimen choices for patients at high risk for primary breast cancer or breast cancer recurrence, and to improve survival outcomes.
Comparator CYP2D6 genotyping, compared with no testing, to direct treatment regimen choices for patients at high risk for primary breast cancer or breast cancer recurrence
Study Quality Assessment Methods
Consistency of study populations; thoroughness of CYP2D6 allele genotyping; whether the use of drugs that inhibit CYP2D6 was taken into account; sources of bias; misclassification of metabolizer phenotype, and adjustment for variables that were not considered to be confounders of the genotype-outcome association.
Study Quality Studies relating the CYP2D6 genotype, tamoxifen metabolites, and clinical outcomes were small, leading to confidence intervals that were too wide to prove an association between these variables.
Primary Conclusions re: Patient Outcomes
There is no direct evidence of clinical utility (whether use of CYP2D6 genotype testing for endocrine therapy regimen selection improves recurrence and survival outcomes). Because the available evidence does not clearly support a significant association between CYP2D6 genotype and tamoxifen treatment outcome, a chain of evidence supporting the clinical utility of CYP2D6 genotyping for directing endocrine therapy regimen selection for women at high risk for or with breast cancer cannot be constructed.
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility
Scientific & Health Need
Tamoxifen is prescribed as a component of adjuvant endocrine therapy to prevent hormone receptor positive breast cancer recurrence, as treatment of metastatic breast cancer, and to prevent disease in high-risk populations and in women with ductal carcinoma in situ.
Illustrative CER Evidence Gaps & Potential Studies
Larger studies are needed to determine effect..
CDC testing tier Tier 2Link to Review Pending Update to BCBSA Website

BCBS TEC. Sequencing-Based Tests to Determine Fetal Down Syndrome (Trisomy 21) from Maternal Plasma DNA, 2012.Type Technology AssessmentCondition PrenatalCondition Category
Prenatal/newborn/children
Main objective To determine whether nucleic acid sequencing-based testing for trisomy 21(non-invasive prenatal testing, NIPT) using maternal serum improves outcomes of pregnancies screened for trisomy 21, compared to traditional serum and ultrasound testing strategies. Additionally, the evidence supporting similar objectives for trisomy 18 and 13 will be reviewed.
Comparator Nucleic acid sequencing-based testing for trisomy 21 using maternal serum, compared to traditional serum and ultrasound testing strategies.
Study Quality Assessment Methods
The purpose of the study was to measure the sensitivity and specificity of maternal DNA sequencing for trisomy 13, 18, or 21 by comparing it to definitive tests or the phenotype at birth. Study quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADRAS-2) instrument. The assessment of risk of bias (4 domains) and three applicability questions were assigned ratings of “low risk,” “high risk,” or “unclear: by two independent reviewers.
Study Quality Three studies met all the criteria for low risk of bias. Five studies did not meet all of the patient selection domains because the authors failed to describe how they assembled the study cohort or controls. One study had a high risk of bias owing to having excluded 28 pregnancies that ended in still birth or miscarriage and lacked karyotyping.
Primary Conclusions re: Patient Outcomes
Clinical utility was determined based on a decision model, comparing NIPT with current screening practices and evaluating the outcomes of case detection, invasive confirmatory procedures required and miscarriages resulting from invasive diagnostic procedures.. Based on these analyses, the results met TEC criteria for demonstrating an improvement in net health outcomes in both low and high risk pregnancies.
Patient-Centeredness beyond Clinical Utility
There were no conclusions on patient centeredness beyond clinical utility.
Scientific & Health Need
Fetal chromosomal abnormalities occur in approximately 1 in 160 live births. Both amniocentesis and CVS are invasive procedures and have a small but finite risk of miscarriage. A new screening strategy such as NIPT that reduces unnecessary amniocentesis and CVS procedures (and thus associated miscarriage) and increases detection of trisomy 21 in particular, and potentially trisomy 18 and 13 as well, has the potential to improve outcomes.
Illustrative CER Evidence Gaps & Potential Studies
- Conduct prospective studies in low risk population, given the public health implications of replacing traditional serum screening. Include patient-reported outcome measures in addition to test results and resource utilization.- Assess effectiveness of NIPT for expanded indications, including sex chromosome aneuploidies, microdeletions and single gene disorders
CDC testing tier This is not in the CDC tier listLink to Review Pending Update to BCBSA Website

Cochrane. Cancer genetic risk assessment for individuals at risk of familial breast cancer, 2012.Type Systematic ReviewCondition CancerCondition Category
Cancer Risk Assessment
Main objective To evaluate the impact of cancer genetic risk-assessment services on patients at risk of familial breast cancer. These services can include extended counselling, specialist screening and genetic testing for mutations
Comparator It is possible for risk-assessment services to vary in a variety of ways and a number of pilot projects have explored alternative models of service delivery.
Study Quality Assessment Methods
Used the risk of bias criteria in the Cochrane Handbook for Systematic Reviews of Interventions. These include how to generate the sequence in which the compared interventions were assigned (randomization is the best); allocation concealment (no one knows the intervention to which the patients is assigned until the moment of allocation); Blinding (at least blinding the outcome assessors).
Study Quality None of the 21 studies had a low risk of bias. The reviewers rated that quality of the study as “generally poor.” The main problems seemed to be a lack of clarity in reporting and, when reporting was good, a failure to anticipate sources of bias.
Primary Conclusions re: Patient Outcomes
Cancer genetic risk-assessment services help to reduce distress, improve the accuracy of the perceived risk of breast cancer, and increase knowledge about breast cancer and genetics. The health professional delivering the risk assessment does not appear to have a significant impact on these outcomes. This review found favourable outcomes for patients after risk assessment for familial breast cancer. However, there were too few papers to make any significant conclusions about how best to deliver cancer genetic risk-assessment services.
Patient-Centeredness beyond Clinical Utility
Although limited, the findings of this review suggest that cancer genetic risk-assessment services can help to reduce distress, improve the accuracy of the individual’s perceived risk of breast cancer, and increase knowledge about breast cancer and genetics. Existing evidence suggests that such services do not cause patients any harm and, in the short-term, can have a positive effect by helping to ease distress and decrease cancer worry.
Scientific & Health Need
Advances in genetics have revealed that some cancers have a genetic component and can therefore, be inherited. It is estimated that between 5% and 10% of all incidents of breast cancer can be attributed to hereditary breast cancer susceptibility genes, including BRCA1 and BRCA2. Recognition of the genetic component of breast cancer has led to greater public demand for information, reassurance, screening, and genetic testing, which has consequently led to significant increases in referrals to clinical genetic centres.
Illustrative CER Evidence Gaps & Potential Studies
- The full scope of cancer genetic services and patient journeys through these services needs to be examined, including decisions to undertake predictive genetic testing and the impact on other decision-making such as the uptake of preventive measures such as prophylactic surgery.- Further research is needed assessing the best means of delivering cancer risk assessment, by different health professionals, in different ways and in alternative locations. More research is needed looking at how risk is presented (i.e. verbal, numerical, graphical), the duration of, where and how risk assessment takes place (e.g. face-to-face or videoconferencing), the availability of, and types of support or after care, or both, and the type of information which is available to patients.- Many studies only included patients at average or moderate risk of breast cancer. The impact of cancer genetic risk assessment for those at high risk is an important area for further research, as these women are generally eligible for genetic testing and may have the option for increased screening or prophylactic surgery, or both.- Patient preferences, as well as the psychological impact of all aspects of cancer genetic services on patients should be measured, as should the acceptability of these services to healthcare professionals.- A genetic predisposition is something that an individual carries for the duration of their lifetime; hence there is a need for longitudinal studies to reflect this.
CDC testing tier Tier 1Link to Review http://www.cochrane.org/CD003721/BREASTCA_cancer-genetic-risk-assessment-for-individuals-at-
risk-of-familial-breast-cancer

Cochrane. Effects of communicating DNA-based disease risk estimates on risk-reducing behaviours, 2010.Type Systematic ReviewCondition Non-SpecificCondition Category
Other
Main objective To assess the effects of communicating actual and hypothetical DNA-based disease risk estimates on risk-reducing behaviours and motivation to undertake such behaviours.
Comparator The comparisons considered are as follows:• communicating DNA-based disease risk estimates versus non-DNA based disease risk estimates• communicating both DNA-based disease risk estimates and non-DNA based disease risk estimates versus non-DNA based disease risk estimates only• communicating DNA-based disease risk estimates versus no disease risk estimates
Study Quality Assessment Methods
Used the risk of bias criteria in the Cochrane Handbook for Systematic Reviews of Interventions, as described in the Cochrane review of. cancer genetic risk assessment for individuals at risk of familial breast cancer.
Study Quality None of the studies had a low risk of bias, which may have been due in part to the authors’ failure to communicate clearly. When reporting was satisfactory, the studies often failed to guard against the risk of bias.
Primary Conclusions re: Patient Outcomes
The limited amount and quality of evidence currently available suggests that communicating genetic test based disease risk estimates may have little or no effect on behaviour, but may have a small effect on intentions to change behavior. Studies examined smoking cessation, dietary behavior, physical activity and medication or vitamin use aimed at reducing disease risks. There was no evidence of any unintended detrimental effects on motivation or mood.
Patient-Centeredness beyond Clinical Utility
It was hypothesized that risk estimates derived from genetic tests may motivate people to change their behaviour in order to reduce the identified risks, which could have impacts on patients. There was no evidence that communicating DNA-based disease risk estimates had any unintended adverse effects. Two studies that assessed fear arousal immediately after the presentation of risk information did, however, report greater fear arousal in the DNA-based disease risk estimate groups compared to comparison groups.
Scientific & Health Need
DNA-based disease risk estimates will translate into health benefits only insofar as (a) acting on them actually modifies disease outcomes, and (b) they can be communicated in ways that motivate individuals to undertake the relevant actions. .There are high expectations that communicating DNA-based disease risk estimates may motivate behaviour change more strongly than disease risk estimates based on other types of risk information. Studies of this impact are important given the proliferation of DNA-based tests conferring increased risk of common complex diseases, which claim that receipt of test results motivate behavior change.
Illustrative CER Evidence Gaps & Potential Studies
The evidence available for this review was limited both in quantity and quality. None of the studies were considered to have a low risk of bias, due to either a lack of clarity in reporting, or where details were reported, evidence of a failure to sufficiently safeguard against the risk of bias. Larger and better quality trials are needed. Such designs would be improved by incorporating the following:1. being powered to detect the small effects such information is likely to have on behaviour, with assessments of cost and cost-effectiveness;2. presenting DNA-based risk information as part of evidence based behaviour change interventions, compared with a control group receiving only the latter;3. measuring potential theoretically-driven mediators and moderators of any impact, including separating out the effects of communicating DNA-based risk estimates from the effects of communicating disease risk estimates, and conducting the trial in populations varying, for example, in levels of social deprivation;4. using valid measures of behaviour, assessed over time to measure the impact of risk communication upon sustained behaviour change; and5. more generally conducting and reporting trials cognisant of the risks of bias, such as ensuring use of adequate comparison groups to disentangle the specific effect of the communication of DNA-based information.
CDC testing tier These are not in the CDC Tier ListLink to Review http%3A%2F%2Fwww.ncbi.nlm.nih.gov%2Fpubmed
%2F20927756&usg=AFQjCNGyMIOLg8kQYef4dZiHwLc-abOgnQ&sig2=c4ITu9J_aoouzywlrpCKqA





























