Embed Size (px)
Citation preview
Includes changes from the 2009 Inpatient Prospective Payment Final Rules published in Federal Register August 18, 2008 and
reference to changes made by the Patient Protection and Affordable Care Act of 2010.
Index to Exceptions and Safe Harbors
Academic Medical Centers -- 56
Ambulance Restocking -- 37
Ambulatory Surgery Centers -- 3
Charitable Donations by a Physician -- 64
Community-Wide Health Information Systems -- 65
Cooperative Hospital Service Organizations -- 7
Compliance Training -- 36
Discounts: Buyers Who Submit Claims and Sellers Thereto -- 9
Discounts: Buyers who Submit Cost Reports and Sellers Thereto -- 10
Electronic Health Records Items and Services -- 74
Electronic Prescribing Items and Services -- 72
Employment Relationships -- 11
EPO and Other Dialysis-Related Drugs Furnished in or by an ESRD Facility -- 55
Equipment Leases -- 18
Eyeglasses and Contact Lenses Following Cataract Surgery -- 54
Fair Market Value Compensation -- 12
Federally Qualified Health Centers -- 70
Group Practice Arrangements With a Hospital -- 13
Group Purchasing Organizations – 14
Implants in an ASC -- 56
Increased Coverage, Reduced Cost-Sharing Amounts, or Reduced Premium Amounts Offered by Health Plans -- 43
Indirect Compensation Arrangements -- 36
In-Office Ancillary Services -- 60
Intra-Family Rural Referrals -- 69
Investment Interests -- 48
Investments in Group Practices -- 16
Isolated Transactions -- 18
Joint Ventures in Underserved Areas -- 18
Medical Staff Incidental Benefits -- 34
Non-Monetary Compensation Up to $300 -- 8
Obstetrical Malpractice Insurance Subsidies -- 44
Personal Services and Management Contracts -- 27
Physician Incentive Plans -- 15
Physician Services -- 43
Practitioner Recruitment -- 21
Preventive Screening Tests, Immunizations, and Vaccines -- 54
Price Reductions Offered by Contractors With Financial Risk to Managed Care Organizations -- 48
Price Reductions Offered to Eligible Managed Care Organizations -- 48
Price Reductions Offered to Health Plans -- 31
Professional Courtesy -- 64
Referral Agreements for Specialty Services -- 47
Referral Services -- 29
Retention Payments in Underserved Areas -- 66
Risk Sharing Agreements -- 35
Sale of Practice – 28
Services Furnished by an Organization to Enrollees -- 59
Space Leases -- 20
Unrelated Remuneration -- 69
Waiver of Beneficiary Coinsurance and Deductible Amounts -- 25
Warranties -- 26
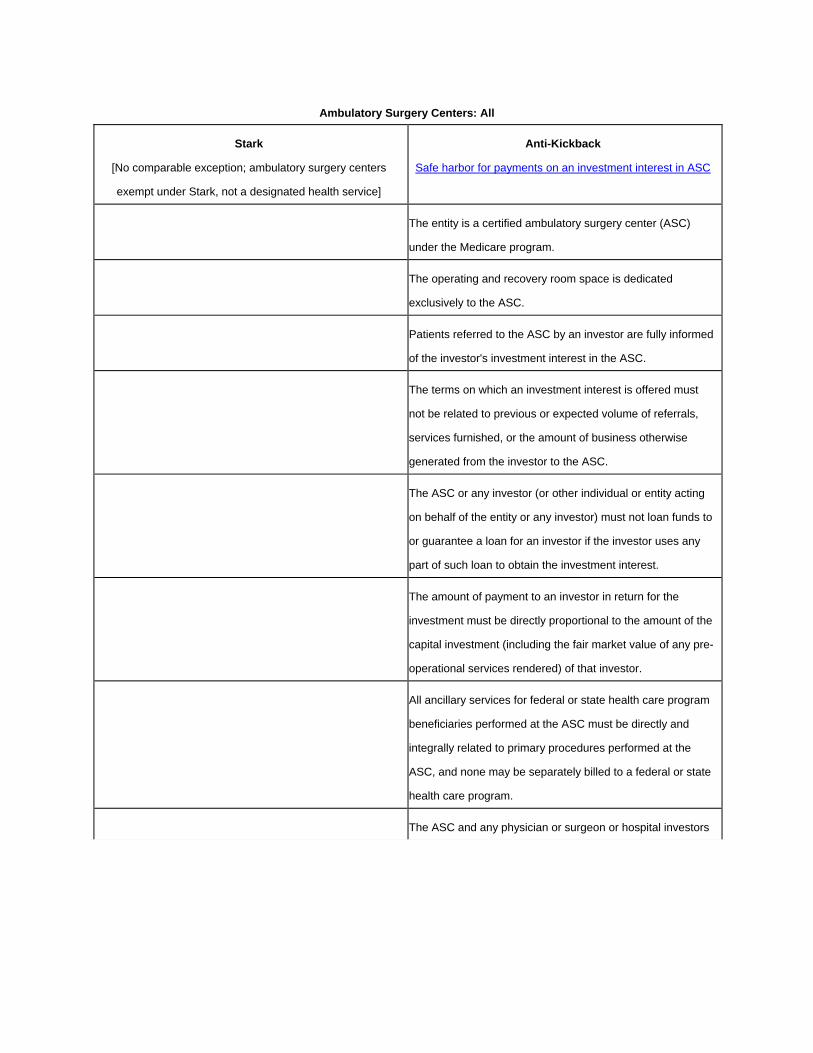
Ambulatory Surgery Centers: All
Stark
[No comparable exception; ambulatory surgery centers
exempt under Stark, not a designated health service]
Anti-Kickback
Safe harbor for payments on an investment interest in ASC
The entity is a certified ambulatory surgery center (ASC)
under the Medicare program.
The operating and recovery room space is dedicated
exclusively to the ASC.
Patients referred to the ASC by an investor are fully informed
of the investor's investment interest in the ASC.
The terms on which an investment interest is offered must
not be related to previous or expected volume of referrals,
services furnished, or the amount of business otherwise
generated from the investor to the ASC.
The ASC or any investor (or other individual or entity acting
on behalf of the entity or any investor) must not loan funds to
or guarantee a loan for an investor if the investor uses any
part of such loan to obtain the investment interest.
The amount of payment to an investor in return for the
investment must be directly proportional to the amount of the
capital investment (including the fair market value of any pre-
operational services rendered) of that investor.
All ancillary services for federal or state health care program
beneficiaries performed at the ASC must be directly and
integrally related to primary procedures performed at the
ASC, and none may be separately billed to a federal or state
health care program.
The ASC and any physician or surgeon or hospital investors
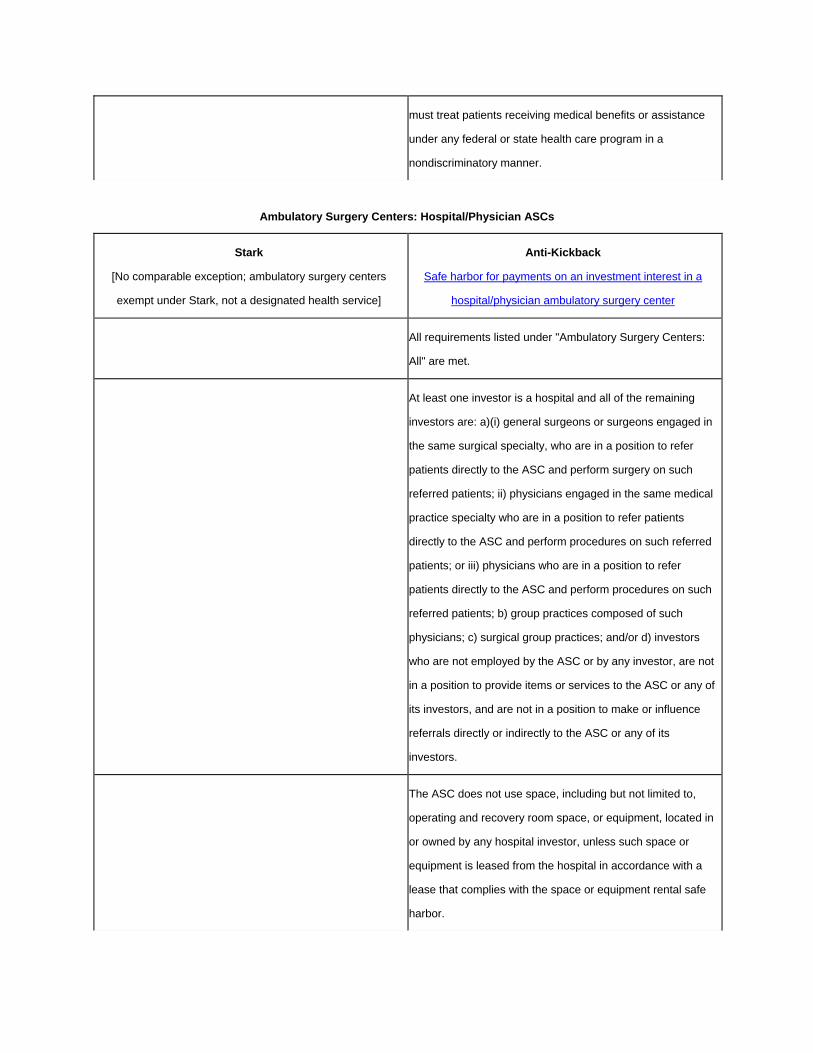
must treat patients receiving medical benefits or assistance
under any federal or state health care program in a
nondiscriminatory manner.
Ambulatory Surgery Centers: Hospital/Physician ASCs
Stark
[No comparable exception; ambulatory surgery centers
exempt under Stark, not a designated health service]
Anti-Kickback
Safe harbor for payments on an investment interest in a
hospital/physician ambulatory surgery center
All requirements listed under "Ambulatory Surgery Centers:
All" are met.
At least one investor is a hospital and all of the remaining
investors are: a)(i) general surgeons or surgeons engaged in
the same surgical specialty, who are in a position to refer
patients directly to the ASC and perform surgery on such
referred patients; ii) physicians engaged in the same medical
practice specialty who are in a position to refer patients
directly to the ASC and perform procedures on such referred
patients; or iii) physicians who are in a position to refer
patients directly to the ASC and perform procedures on such
referred patients; b) group practices composed of such
physicians; c) surgical group practices; and/or d) investors
who are not employed by the ASC or by any investor, are not
in a position to provide items or services to the ASC or any of
its investors, and are not in a position to make or influence
referrals directly or indirectly to the ASC or any of its
investors.
The ASC does not use space, including but not limited to,
operating and recovery room space, or equipment, located in
or owned by any hospital investor, unless such space or
equipment is leased from the hospital in accordance with a
lease that complies with the space or equipment rental safe
harbor.
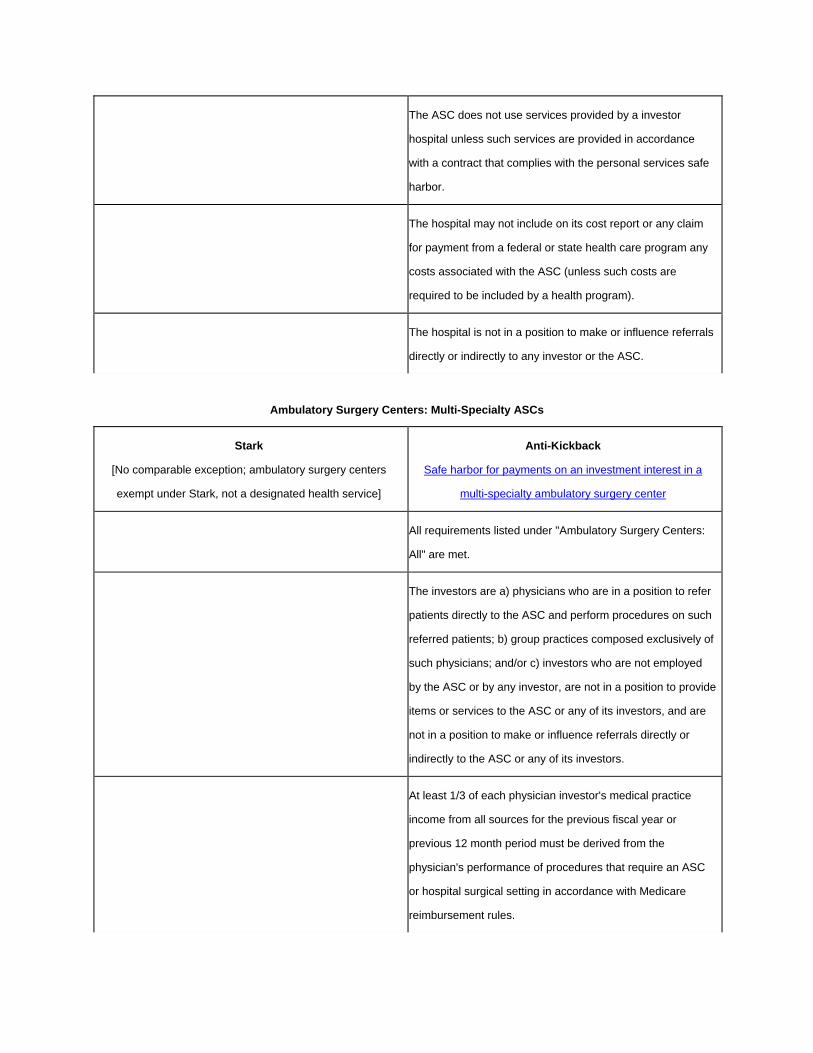
The ASC does not use services provided by a investor
hospital unless such services are provided in accordance
with a contract that complies with the personal services safe
harbor.
The hospital may not include on its cost report or any claim
for payment from a federal or state health care program any
costs associated with the ASC (unless such costs are
required to be included by a health program).
The hospital is not in a position to make or influence referrals
directly or indirectly to any investor or the ASC.
Ambulatory Surgery Centers: Multi-Specialty ASCs
Stark
[No comparable exception; ambulatory surgery centers
exempt under Stark, not a designated health service]
Anti-Kickback
Safe harbor for payments on an investment interest in a
multi-specialty ambulatory surgery center
All requirements listed under "Ambulatory Surgery Centers:
All" are met.
The investors are a) physicians who are in a position to refer
patients directly to the ASC and perform procedures on such
referred patients; b) group practices composed exclusively of
such physicians; and/or c) investors who are not employed
by the ASC or by any investor, are not in a position to provide
items or services to the ASC or any of its investors, and are
not in a position to make or influence referrals directly or
indirectly to the ASC or any of its investors.
At least 1/3 of each physician investor's medical practice
income from all sources for the previous fiscal year or
previous 12 month period must be derived from the
physician's performance of procedures that require an ASC
or hospital surgical setting in accordance with Medicare
reimbursement rules.

At least 1/3 of the procedures that require an ASC or hospital
surgical setting in accordance with Medicare reimbursement
rules performed by each physician investor for the previous
fiscal year or previous 12 month period must be performed at
the ASC.
Ambulatory Surgery Centers: Single Specialty ASCs
Stark
[No comparable exception; ambulatory surgery centers
exempt under Stark, not a designated health service]
Anti-Kickback
Safe harbor for payments on an investment interest in a
single-specialty ambulatory surgery center
All requirements listed under "Ambulatory Surgery Centers:
All" are met.
The investors are a) physicians engaged in the same medical
practice specialty who are in a position to refer patients
directly to the ASC and perform procedures on such referred
patients; b) group practices composed exclusively of such
physicians; and/or c) investors who are not employed by the
ASC or by any investor, are not in a position to provide items
or services to the ASC or any of its investors, and are not in a
position to make or influence referrals directly or indirectly to
the ASC or any of its investors.
At least 1/3 of each physician investor's medical practice
income from all sources for the previous fiscal year or
previous 12 month period must be derived from the
physician's performance of procedures that require an ASC
or hospital surgical setting in accordance with Medicare
reimbursement rules.
Ambulatory Surgery Centers: Surgeon-Owned ASCs
Stark
[No comparable exception; ambulatory surgery centers
exempt under Stark, not a designated health service]
Anti-Kickback
Safe harbor for payments on an investment interest in an
surgeon-owned ambulatory surgery center

All requirements listed under "Ambulatory Surgery Centers:
All" are met.
The investors are a) general surgeons or surgeons engaged
in the same surgical specialty, who are in a position to refer
patients directly to the ASC and perform surgery on such
referred patients; b) surgical group practices composed
exclusively of such surgeons; and/or c) investors who are not
employed by the ASC or by any investor, are not in a position
to provide items or services to the ASC or any of its
investors, and are not in a position to make or influence
referrals directly or indirectly to the ASC or any of its
investors.
At least 1/3 of each surgeon investor's medical practice
income from all sources for the previous fiscal year or
previous 12 month period must be derived from the surgeon's
performance of procedures that require an ASC or hospital
surgical setting in accordance with Medicare reimbursement
rules.
Cooperative Hospital Service Organizations
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for payments between a cooperative hospital
service organization (CHSO) and its patron hospital
Both the CHSO and the patron hospital are described in
§501(e) of the Internal Revenue Code and are tax-exempt
under §501(c)(3.)
The CHSO is wholly owned by two or more patron hospitals.
If the patron hospital makes a payment to the CHSO, it must
be for the purpose of paying for the bona fide operating
expenses of the CHSO; or for the purpose of paying a
distribution of net earnings required to be made under
§501(e)(2) of the Internal Revenue Code.
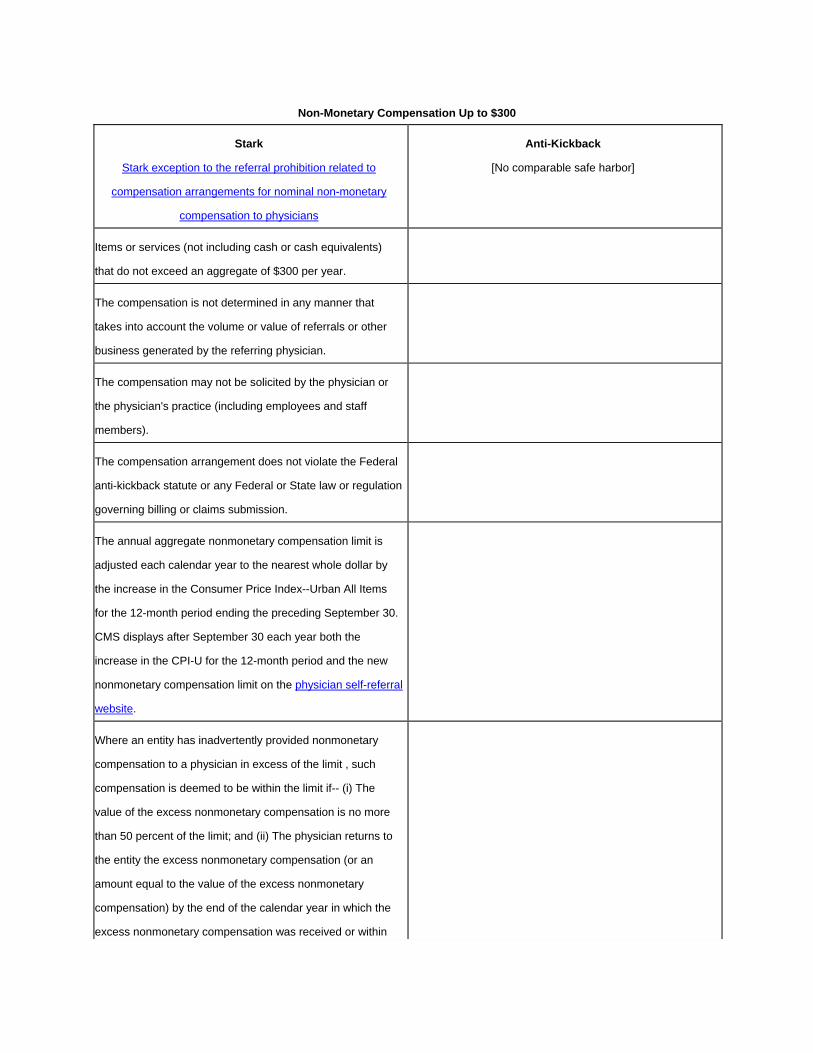
Non-Monetary Compensation Up to $300
Stark
Stark exception to the referral prohibition related to
compensation arrangements for nominal non-monetary
compensation to physicians
Anti-Kickback
[No comparable safe harbor]
Items or services (not including cash or cash equivalents)
that do not exceed an aggregate of $300 per year.
The compensation is not determined in any manner that
takes into account the volume or value of referrals or other
business generated by the referring physician.
The compensation may not be solicited by the physician or
the physician's practice (including employees and staff
members).
The compensation arrangement does not violate the Federal
anti-kickback statute or any Federal or State law or regulation
governing billing or claims submission.
The annual aggregate nonmonetary compensation limit is
adjusted each calendar year to the nearest whole dollar by
the increase in the Consumer Price Index--Urban All Items
for the 12-month period ending the preceding September 30.
CMS displays after September 30 each year both the
increase in the CPI-U for the 12-month period and the new
nonmonetary compensation limit on the physician self-referral
website.
Where an entity has inadvertently provided nonmonetary
compensation to a physician in excess of the limit , such
compensation is deemed to be within the limit if-- (i) The
value of the excess nonmonetary compensation is no more
than 50 percent of the limit; and (ii) The physician returns to
the entity the excess nonmonetary compensation (or an
amount equal to the value of the excess nonmonetary
compensation) by the end of the calendar year in which the
excess nonmonetary compensation was received or within

180 consecutive calendar days following the date the excess
nonmonetary compensation was received by the physician,
whichever is earlier. This option may be used by an entity
only once every 3 years with respect to the same referring
physician.
In addition to nonmonetary compensation up to the limit, an
entity that has a formal medical staff may provide one local
medical staff appreciation event per year for the entire
medical staff. Any gifts or gratuities provided in connection
with the medical staff appreciation event are subject to the
limit.
Discounts: Buyers Who Submit Claims and Sellers Thereto
Stark
[No comparable exemption]
Anti-Kickback
Safe harbor for discounts received by a buyer, which submits
a claim for payment for the good or service for which
payment is made under any federal or state health care plan
and sellers to such buyers
The buyer is an individual or entity (which is not an HMO or
competitive medical plan or a buyer which reports its costs on
a cost report) in whose name a claim or request for payment
is submitted for the discounted item or service and payment
may be made, in whole or in part, under a federal or state
health care program.
The discount must be made at the time of the sale of the
goods or service or the terms of the rebate must be fixed and
disclosed in writing to the buyer at the time of the initial sale
of goods or services.
The buyer, (if submitting the claim) must provide, upon
request, to the Secretary of HHS or a state agency, the
information required to be provided to a buyer by a seller.
Where the seller submits a claim or request for payment on
behalf of the buyer and the item or service is separately

claimed, the seller must provide, upon request by Secretary
of HHS or a state agency information request to be provided
to a seller by an offeror.
Where the buyer submits a claim, the seller must a) fully and
accurately report such discount on the invoice, coupon or
statement submitted to the buyer; b) inform the buyer of its
obligations to report such discount and to provide information
upon request; and c) refrain from doing anything that would
impede the buyer from meeting its obligations.
[Note that discount "offerors" have similar requirements to
sellers; an offeror is an individual or entity who is not a seller
but promotes the purchase of an item or service to a buyer].
Discounts: Buyers Who Submit Cost Reports and Sellers Thereto
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for discounts received by a buyer which submits
a cost report and sellers to such buyers
The buyer is an entity which reports its costs on a cost report
required by the Department of HHS or a state health care
program.
The discount must be earned based on purchases of that
same good or service bought within a single fiscal year of the
buyer.
The buyer must claim the benefit of the discount in the fiscal
year in which the discount is earned or the following year.
The buyer must fully and accurately report the discount in the
applicable cost report.
The buyer must provide, upon request, by the Secretary of
HHS or a state agency, the information required to be
provided to a buyer by a seller.
The seller must a) fully and accurately report such discount
on the invoice, coupon or statement submitted to the buyer;
b) ; b) inform the buyer of its obligations to report such

discount and to provide information upon request; and c)
refrain from doing anything that would impede the buyer from
meeting its obligations.
If the value of the discount is not known at the time of sale,
the seller must a) fully and accurately report the existence of
a discount program on the invoice, coupon or statement
submitted to the buyer; and when the value of the discount
becomes known, provide the buyer with documentation of the
calculation of the discount identifying the specific goods or
services purchased to which to discount will be applied.
[Note that discount "offerors" have similar requirements to
sellers; an offeror is an individual or entity who is not a seller
but promotes the purchase of an item or service to a buyer].
Bona Fide Employment Relationships
Stark
Stark exception to the referral prohibition related to
compensation arrangements for bona fide employment
relationships with physicians (or an immediate family member
of the physician)
Anti-Kickback
Safe harbor for employment relationships
The employment is for identifiable services. The employment is a bona fide employment relationship with
the employer.
The amount of the remuneration under the employment is: a)
consistent with the fair market value of the services; and b) is
not determined in a manner that takes into account (directly
or indirectly) the volume or value of any referrals by the
referring physician. Subparagraph b) herein does not prohibit
payment of remuneration in the form of a productivity bonus
based on services performed personally by the physician (or
immediate family member of the physician).
The remuneration is provided under an agreement that would
be commercially reasonable even if no referrals were made
to the employer.
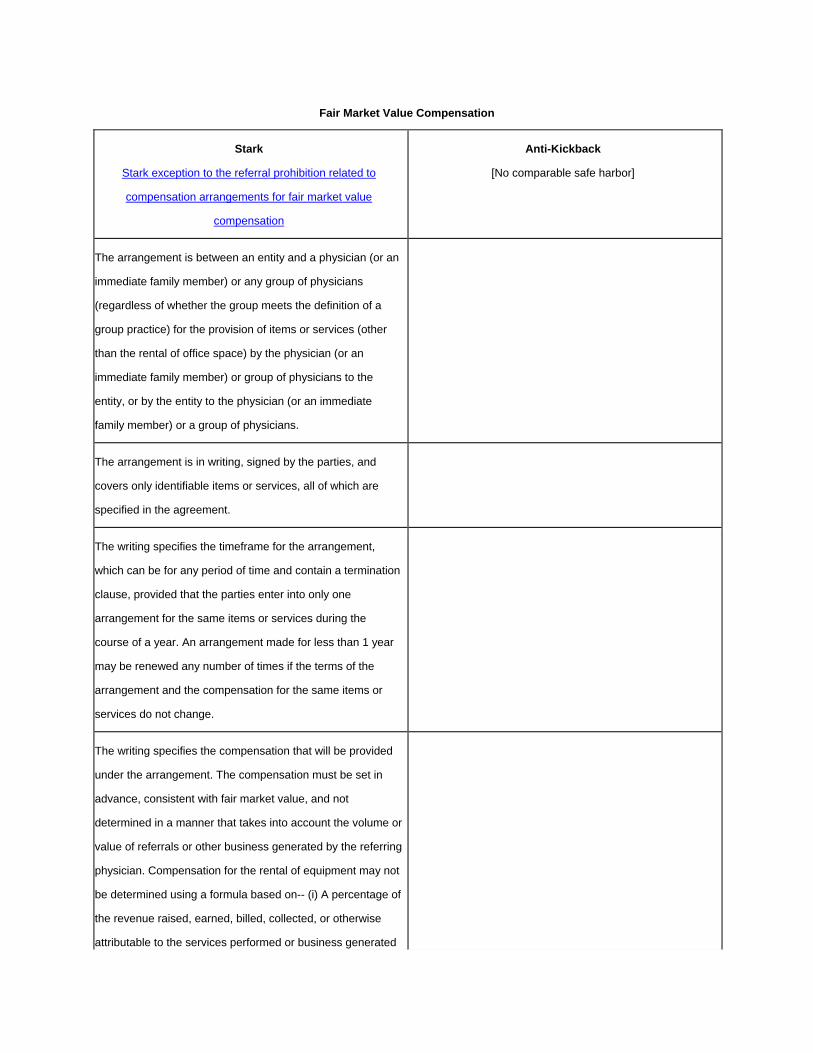
Fair Market Value Compensation
Stark
Stark exception to the referral prohibition related to
compensation arrangements for fair market value
compensation
Anti-Kickback
[No comparable safe harbor]
The arrangement is between an entity and a physician (or an
immediate family member) or any group of physicians
(regardless of whether the group meets the definition of a
group practice) for the provision of items or services (other
than the rental of office space) by the physician (or an
immediate family member) or group of physicians to the
entity, or by the entity to the physician (or an immediate
family member) or a group of physicians.
The arrangement is in writing, signed by the parties, and
covers only identifiable items or services, all of which are
specified in the agreement.
The writing specifies the timeframe for the arrangement,
which can be for any period of time and contain a termination
clause, provided that the parties enter into only one
arrangement for the same items or services during the
course of a year. An arrangement made for less than 1 year
may be renewed any number of times if the terms of the
arrangement and the compensation for the same items or
services do not change.
The writing specifies the compensation that will be provided
under the arrangement. The compensation must be set in
advance, consistent with fair market value, and not
determined in a manner that takes into account the volume or
value of referrals or other business generated by the referring
physician. Compensation for the rental of equipment may not
be determined using a formula based on-- (i) A percentage of
the revenue raised, earned, billed, collected, or otherwise
attributable to the services performed or business generated
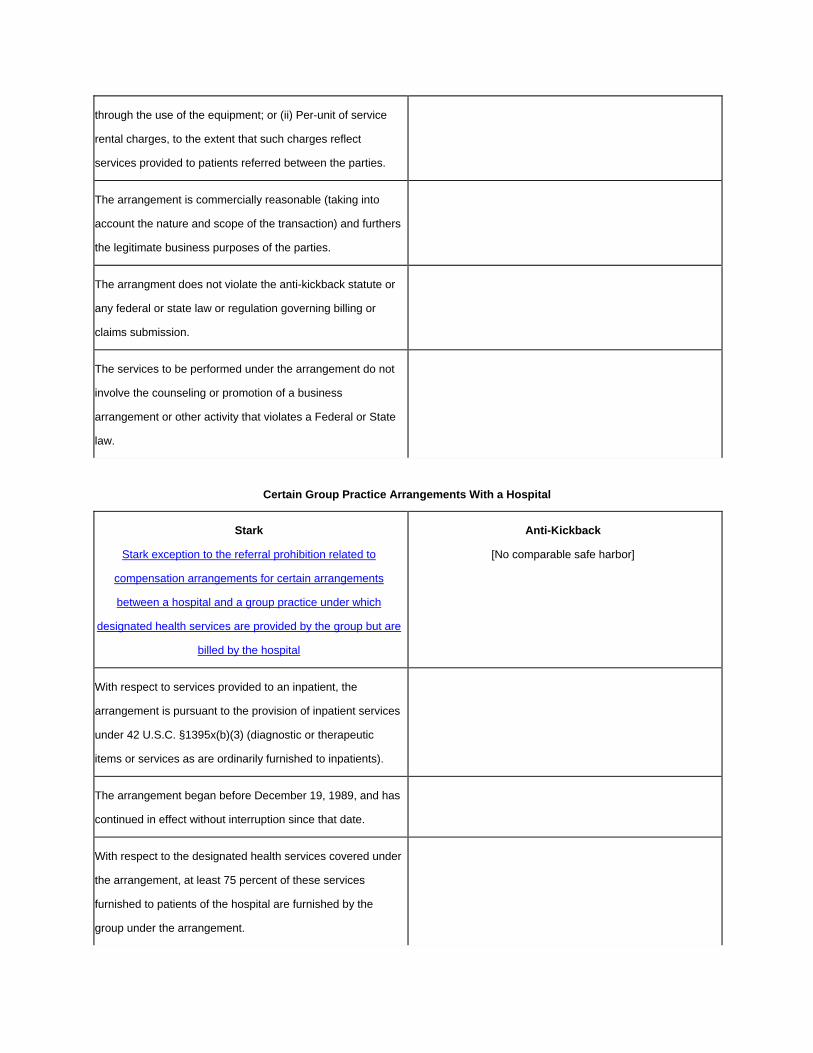
through the use of the equipment; or (ii) Per-unit of service
rental charges, to the extent that such charges reflect
services provided to patients referred between the parties.
The arrangement is commercially reasonable (taking into
account the nature and scope of the transaction) and furthers
the legitimate business purposes of the parties.
The arrangment does not violate the anti-kickback statute or
any federal or state law or regulation governing billing or
claims submission.
The services to be performed under the arrangement do not
involve the counseling or promotion of a business
arrangement or other activity that violates a Federal or State
law.
Certain Group Practice Arrangements With a Hospital
Stark
Stark exception to the referral prohibition related to
compensation arrangements for certain arrangements
between a hospital and a group practice under which
designated health services are provided by the group but are
billed by the hospital
Anti-Kickback
[No comparable safe harbor]
With respect to services provided to an inpatient, the
arrangement is pursuant to the provision of inpatient services
under 42 U.S.C. §1395x(b)(3) (diagnostic or therapeutic
items or services as are ordinarily furnished to inpatients).
The arrangement began before December 19, 1989, and has
continued in effect without interruption since that date.
With respect to the designated health services covered under
the arrangement, at least 75 percent of these services
furnished to patients of the hospital are furnished by the
group under the arrangement.

The arrangement is pursuant to an agreement that is set out
in writing and that specifies the services to be provided and
the compensation for the services provided.
The compensation paid over the term of the agreement is
consistent with the fair market value.
The compensation per unit of service is fixed in advance and
is not determined in a manner that takes into account the
volume or value of any referrals or other business generated
between the parties.
The compensation is provided pursuant to an agreement
which would be commercially reasonable even if no referrals
were made to the entity.
Group Purchasing Organizations
Stark
[No comparable exemption]
Anti-Kickback
Safe harbor for payments made by a vendor of goods or
services to a group purchasing organization (GPO)
The GPO must have a written agreement with each individual
or entity for which items or services are furnished.
The agreement provides for either of the following: a) the
agreement states that participating vendors from which the
individual or entity will purchase goods or services will pay a
fee to the GPO of 3 percent or less of the purchase price of
the goods or services provided by that vendor. or b) in the
event the fee paid to the GPO is not fixed at 3 percent or less
of the purchase price of the goods or services, the agreement
specifies the amount (or if not known, the maximum amount)
the GPO will be paid by each vendor (where such amount
may be a fixed sum or a fixed percentage of the value of
purchases made from the vendor by the members of the
group under the contract between the vendor and the GPO).

Where the entity which receives the goods or service from
the vendor is a health care provider of services, the GPO
must disclose in writing to the entity at least annually, and to
the Secretary upon request, the amount received from each
vendor with respect to purchases made by or on behalf of the
entity.
The term group purchasing organization means an entity
authorized to act as a purchasing agent for a group of
individuals or entities who are furnishing services for which
payment may be made in whole or in part under Medicare or
a State health care program, and who are neither wholly-
owned by the GPO nor subsidiaries of a parent corporation
that wholly owns the GPO (either directly or through another
wholly-owned entity).
Physician Incentive Plan
Stark
Stark exception to the referral prohibition related to
compensation arrangements for incentive plans between an
entity and a physician
Anti-Kickback
[No comparable safe harbor]
The arrangement meets the requirements for of the personal
services safe harbor but the compensation may be
determined in a manner (through a withhold, capitation,
bonus, or otherwise) that takes into account directly or
indirectly the volume or value of any referrals or other
business generated between the parties.
No specific payment is made directly or indirectly under the
plan to a physician or a physician group as an inducement to
reduce or limit medically necessary services furnished with
respect to a specific individual enrolled with the entity.
Upon request of the Secretary of HHS, the entity provides the
Secretary with access to information regarding the plan
(including any downstream subcontractor plans), in order to
permit the Secretary to determine whether the plan is in
compliance with this section.
In the case of a plan that places a physician or a physician
group at substantial financial risk as defined in Sec. 422.208,
the entity (and/or any downstream contractor) complies with
the requirements concerning physician incentive plans set
forth at Sec. 422.208 and Sec. 422.210 of this chapter.
Investments in group practices
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for any payment that is a return on an investment
interest made to a solo or group practitioner investing in his
own practice or group practice
The equity interests in the practice or group must be held by
licensed health care professionals who practice in the
practice of the group.
The equity interests must be in the practice or group practice
itself and not a subdivision of the practice or group.
In the case of a group practice, the practice must be a group
practice and be a unified business with centralized decision-
making, pooling of expenses and revenues, and a
compensation/profit distribution system that is not based on
satellite offices operating substantially as if they were
separate enterprises or profit centers.
Revenues from ancillary services, if any, must be derived
from "in-office ancillary services as defined in section
1877(b)(2) of the Social Security Act.
Joint Ventures in Underserved Areas
Stark Anti-Kickback
[No comparable exception] Safe harbor for payments that constitute return on an
investment interest, such as dividend or interest income,
made to an investor in an entity that possesses investment
interests that are held by either active or passive investors
No more than 50% of the value of the investment interests of
each class of investments may be held in the previous fiscal
year or previous 12 month period by investors who are in a
position to make or influence referrals to, furnish items or
services to, or otherwise generate business for the entity.
The terms on which an investment interest is offered to a
passive investor, if any, who is in a position to make or
influence referrals to, furnish items or services to, or
otherwise generate business for the entity must be no
different from the terms offered to other passive investors.
The terms on which an investment interest is offered to an
investor who is in a position to make or influence referrals to
or generate business for the entity must not be related to the
previous or expected volume of referrals, or the amount of
business generated from the investor to the entity.
Passive investors are not be required to either make referrals
to, or otherwise generate business for the entity as a
condition for remaining as an investor.
The entity or any investor must not market or furnish the
entity's items or services to passive investors differently than
to non-investors.
At least 75% of the dollar volume of the entity's business in
the previous fiscal year or previous 12 month period must be
derived from the service of persons who reside in an
underserved area or are members of medically underserved
populations.
The entity or any investor must not loan funds to or
guarantee a loan for any investor who is in a position to make
or influence referrals to or generate business for the entity if
the investor uses any part of the loan to obtain the
investment interest.
The amount of the payment to an investor in return for the
investment must be directly proportional to the amount of the
capital investment.
Isolated Transactions
Stark
Stark exception to the referral prohibition related to
compensation arrangements for isolated financial
transactions with a physician, such as a one-time sale of
property or a practice
Anti-Kickback
[No comparable safe harbor]
The amount of the remuneration under the transaction is
consistent with the fair market value of the services.
The amount of remuneration under the transaction is not
determined in a manner that takes into account (directly or
indirectly) the volume or value of any referrals by the referring
physician or other business generated between the parties.
The remuneration is provided under an agreement that would
be commercially reasonable even if the physician made no
referrals.
There are no additional transactions between the parties for 6
months after the isolated transaction, except for transactions
which are specifically excepted under the other provisions of
the Stark regulations and except for commercially reasonable
post- closing adjustments that do not take into account
(directly or indirectly) the volume or value of referrals or other
business generated by the referring physician.
Equipment Leases
Stark
Stark exception to the referral prohibition related to
compensation arrangements for rental of equipment between
Anti-Kickback
Safe harbor for payments made by a lessee to a lessor for
the use of equipment
an entity and a referring physician
A rental or lease agreement is set out in writing and signed
by the parties and specifies the equipment covered by the
lease.
The lease agreement is set out in writing and signed by the
parties.
The equipment rented or leased does not exceed that which
is reasonable and necessary for the legitimate business
purposes of the lease or rental and is used exclusively by the
lessee when being used by the lessee and is not shared with
or used by the lessor or any person or entity related to the
lessor.
The lease covers all of the equipment leased between the
parties for the term of the lease and specifies the equipment
covered by the lease.
The lease provides for a term of rental or lease of at least 1
year. If the agreement is terminated during the term with or
without cause, the parties may not enter into a new
agreement during the first year of the original term of the
agreement. A holdover month-to-month rental for up to 6
months immediately following an agreement of at least 1 year
will satisfy this paragraph, provided the holdover rental is on
the same terms and conditions as the immediately preceding
agreement.
If the lease is intended to provide the lessee with use of the
equipment for periodic intervals of time, rather than on a full-
time basis for the term of the lease, the lease specifies
exactly the schedule of such intervals, their precise length,
and the exact rent for such interval.
The rental charges over the term of the agreement are set in
advance, are consistent with fair market value, and are not
determined— (i) In a manner that takes into account the
volume or value of any referrals or other business generated
between the parties; or (ii) Using a formula based on— (A) A
percentage of the revenue raised, earned, billed, collected, or
otherwise attributable to the services performed on or
business generated by the use of the equipment; or (B) Per-
unit of service rental charges, to the extent that such charges
reflect services provided to patients referred between the
parties.
The term of the lease is for not less than one year.
The lease would be commercially reasonable even if no
referrals were made between the parties.
The aggregate rental charge is set in advance, is consistent
with fair market value in arms-length transactions and is not
determined in a manner that takes into account the volume or
value of any referrals or business otherwise generated

between the parties for which payment may be made in
whole or in part under Medicare or a State health care
program.
The aggregate equipment rental does not exceed that which
is reasonably necessary to accomplish the commercially
reasonable business purpose of the rental.
The term fair market value means the value of the equipment
when obtained from a manufacturer or professional
distributor, but shall not be adjusted to reflect the additional
value one party (either the prospective lessee or lessor)
would attribute to the equipment as a result of its proximity or
convenience to sources of referrals or business otherwise
generated for which payment may be made in whole or in
part under Medicare or a State health care program.
Space Leases
Stark
Stark exception to the referral prohibition related to
compensation arrangements for rental of office space
between an entity and a referring physician
Anti-Kickback
Safe harbor for payments made by a lessee to a lessor for
the use of space
The agreement is set out in writing, is signed by the parties,
and specifies the premises it covers.
The lease agreement is set out in writing and signed by the
parties.
The term of the agreement is at least 1 year. To meet this
requirement, if the agreement is terminated during the term
with or without cause, the parties may not enter into a new
agreement during the first year of the original term of the
agreement. A holdover month-to-month rental for up to 6
months immediately following an agreement of at least 1 year
that met the conditions of this paragraph (a) will satisfy this
paragraph (a), provided the holdover rental is on the same
terms and conditions as the immediately preceding
agreement.
The lease covers all of the premises leased between the
parties for the term of the lease and specifies the premises
covered by the lease.
The space rented or leased does not exceed that which is If the lease is intended to provide the lessee with access to

reasonable and necessary for the legitimate business
purposes of the lease or rental and is used exclusively by the
lessee when being used by the lessee (and is not shared with
or used by the lessor or any person or entity related to the
lessor), except that the lessee may make payments for the
use of space consisting of common areas if the payments do
not exceed the lessee's pro rata share of expenses for the
space based upon the ratio of the space used exclusively by
the lessee to the total amount of space (other than common
areas) occupied by all persons using the common areas.
the premises for periodic intervals of time, rather than on a
full-time basis for the term of the lease, the lease specifies
exactly the schedule of such intervals, their precise length,
and the exact rent for such intervals.
The rental charges over the term of the agreement are set in
advance and are consistent with fair market value.
The term of the lease is for not less than one year.
The rental charges over the term of the agreement are not
determined-- (i) In a manner that takes into account the
volume or value of any referrals or other business generated
between the parties; or (ii) Using a formula based on— (A) A
percentage of the revenue raised, earned, billed, collected, or
otherwise attributable to the services performed or business
generated in the office space; or (B) Per-unit of service rental
charges, to the extent that such charges reflect services
provided to patients referred between the parties.
The aggregate rental charge is set in advance, is consistent
with fair market value in arms-length transactions and is not
determined in a manner that takes into account the volume or
value of any referrals or business otherwise generated
between the parties for which payment may be made in
whole or in part under Medicare or a State health care
program.
The agreement would be commercially reasonable even if no
referrals were made between the lessee and the lessor.
The aggregate space rented does not exceed that which is
reasonably necessary to accomplish the commercially
reasonable business purpose of the rental.
The term fair market value means the value of the rental
property for general commercial purposes, but shall not be
adjusted to reflect the additional value that one party (either
the prospective lessee or lessor) would attribute to the
property as a result of its proximity or convenience to sources
of referrals or business otherwise generated for which
payment may be made in whole or in part under Medicare or
a State health care program.
Practitioner Recruitment
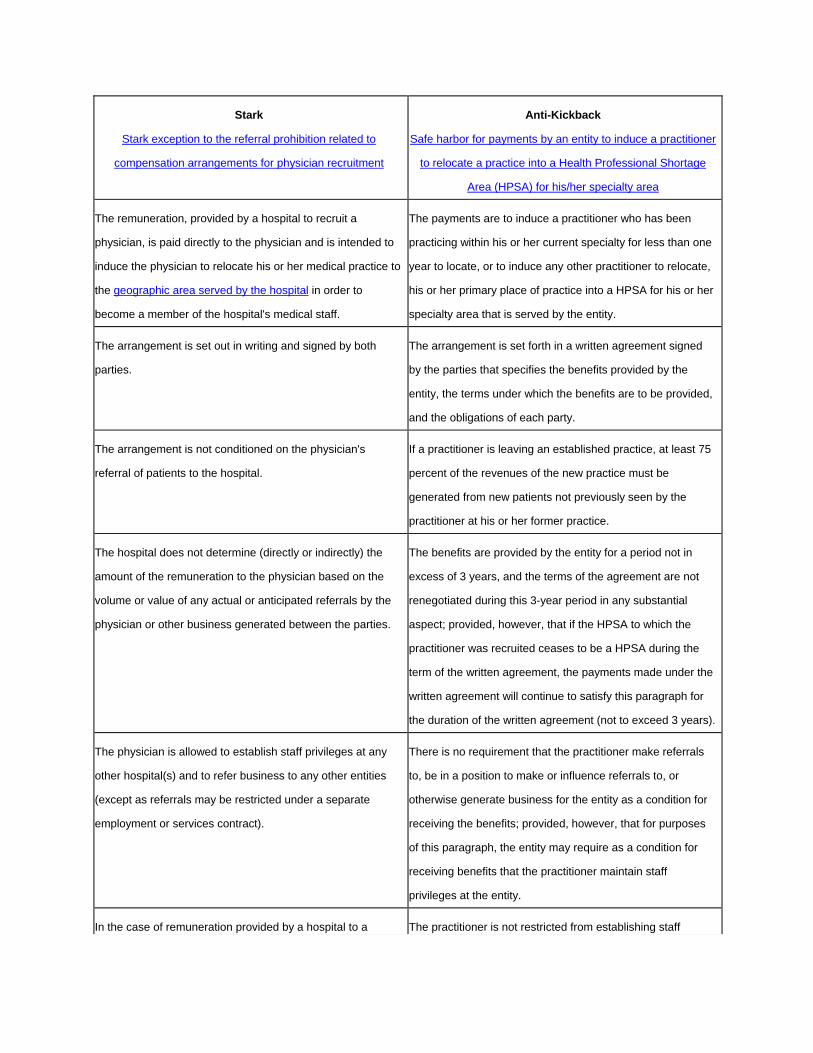
Stark
Stark exception to the referral prohibition related to
compensation arrangements for physician recruitment
Anti-Kickback
Safe harbor for payments by an entity to induce a practitioner
to relocate a practice into a Health Professional Shortage
Area (HPSA) for his/her specialty area
The remuneration, provided by a hospital to recruit a
physician, is paid directly to the physician and is intended to
induce the physician to relocate his or her medical practice to
the geographic area served by the hospital in order to
become a member of the hospital's medical staff.
The payments are to induce a practitioner who has been
practicing within his or her current specialty for less than one
year to locate, or to induce any other practitioner to relocate,
his or her primary place of practice into a HPSA for his or her
specialty area that is served by the entity.
The arrangement is set out in writing and signed by both
parties.
The arrangement is set forth in a written agreement signed
by the parties that specifies the benefits provided by the
entity, the terms under which the benefits are to be provided,
and the obligations of each party.
The arrangement is not conditioned on the physician's
referral of patients to the hospital.
If a practitioner is leaving an established practice, at least 75
percent of the revenues of the new practice must be
generated from new patients not previously seen by the
practitioner at his or her former practice.
The hospital does not determine (directly or indirectly) the
amount of the remuneration to the physician based on the
volume or value of any actual or anticipated referrals by the
physician or other business generated between the parties.
The benefits are provided by the entity for a period not in
excess of 3 years, and the terms of the agreement are not
renegotiated during this 3-year period in any substantial
aspect; provided, however, that if the HPSA to which the
practitioner was recruited ceases to be a HPSA during the
term of the written agreement, the payments made under the
written agreement will continue to satisfy this paragraph for
the duration of the written agreement (not to exceed 3 years).
The physician is allowed to establish staff privileges at any
other hospital(s) and to refer business to any other entities
(except as referrals may be restricted under a separate
employment or services contract).
There is no requirement that the practitioner make referrals
to, be in a position to make or influence referrals to, or
otherwise generate business for the entity as a condition for
receiving the benefits; provided, however, that for purposes
of this paragraph, the entity may require as a condition for
receiving benefits that the practitioner maintain staff
privileges at the entity.
In the case of remuneration provided by a hospital to a The practitioner is not restricted from establishing staff

physician either indirectly through payments made to another
physician practice, or directly to a physician who joins a
physician practice, the following additional conditions must be
met: (a) the written agreement also signed by the party to
whom the payments are directly made; (b) except for actual
costs incurred by the physician practice in recruiting the new
physician, the remuneration is passed directly through to or
remains with the recruited physician; (c) in the case of an
income guarantee of any type made by the hospital to a
recruited physician who joins a physician practice, the costs
allocated by the physician practice to the recruited physician
do not exceed the actual additional incremental costs
attributable to the recruited physician. With respect to a
physician recruited to join a physician practice located in a
rural area or HPSA, if the physician is recruited to replace a
physician who, within the previous 12-month period, retired,
relocated outside of the geographic area served by the
hospital, or died, the costs allocated by the physician practice
to the recruited physician do not exceed either-- (1) the actual
additional incremental costs attributable to the recruited
physician; or (2) the lower of a per capita allocation or 20
percent of the practice's aggregate costs; (d) records of the
actual costs and the passed-through amounts are maintained
for a period of at least 5 years and made available to the
Secretary of HHS upon request; (e) the remuneration from
the hospital under the arrangement is not determined in a
manner that takes into account (directly or indirectly) the
volume or value of any actual or anticipated referrals by the
recruited physician or the physician practice (or any physician
affiliated with the physician practice) receiving the direct
payments from the hospital; (f) the physician practice may not
impose on the recruited physician practice restrictions that
unreasonably restrict the recruited physician's ability to
practice medicine in the geographic area served by the
hospital; and (g) the arrangement does not violate the anti-
privileges at, referring any service to, or otherwise generating
any business for any other entity of his or her choosing.
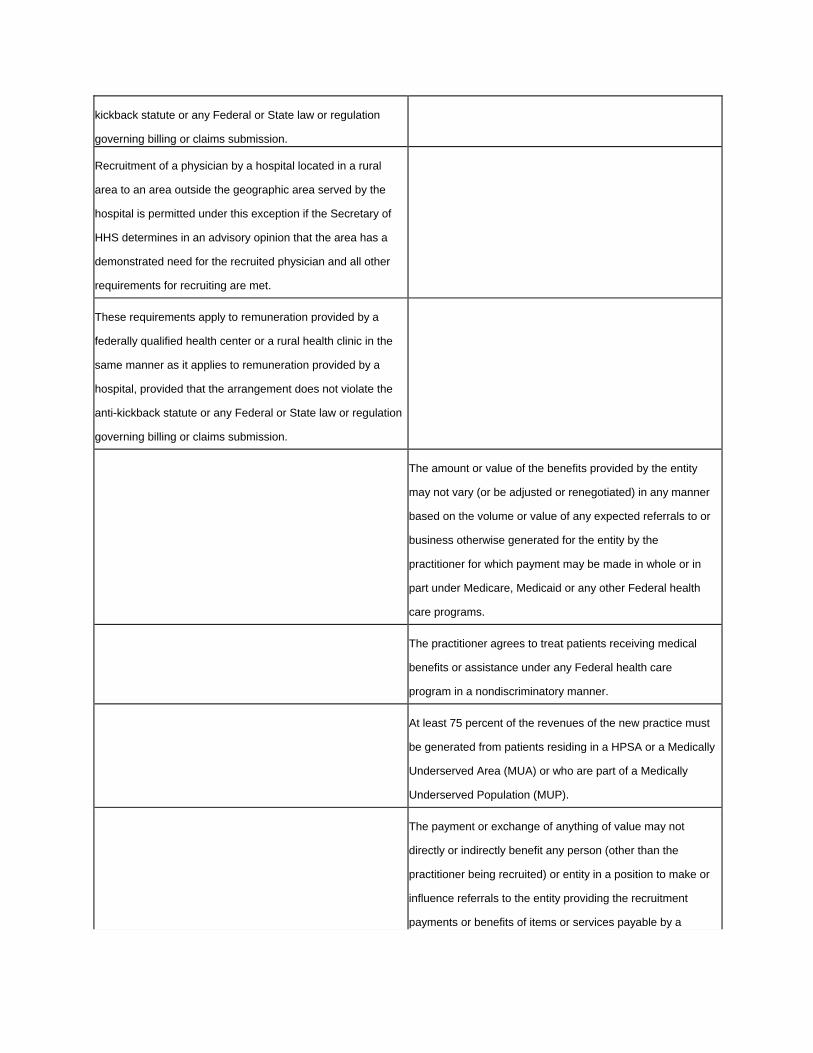
kickback statute or any Federal or State law or regulation
governing billing or claims submission.
Recruitment of a physician by a hospital located in a rural
area to an area outside the geographic area served by the
hospital is permitted under this exception if the Secretary of
HHS determines in an advisory opinion that the area has a
demonstrated need for the recruited physician and all other
requirements for recruiting are met.
These requirements apply to remuneration provided by a
federally qualified health center or a rural health clinic in the
same manner as it applies to remuneration provided by a
hospital, provided that the arrangement does not violate the
anti-kickback statute or any Federal or State law or regulation
governing billing or claims submission.
The amount or value of the benefits provided by the entity
may not vary (or be adjusted or renegotiated) in any manner
based on the volume or value of any expected referrals to or
business otherwise generated for the entity by the
practitioner for which payment may be made in whole or in
part under Medicare, Medicaid or any other Federal health
care programs.
The practitioner agrees to treat patients receiving medical
benefits or assistance under any Federal health care
program in a nondiscriminatory manner.
At least 75 percent of the revenues of the new practice must
be generated from patients residing in a HPSA or a Medically
Underserved Area (MUA) or who are part of a Medically
Underserved Population (MUP).
The payment or exchange of anything of value may not
directly or indirectly benefit any person (other than the
practitioner being recruited) or entity in a position to make or
influence referrals to the entity providing the recruitment
payments or benefits of items or services payable by a

Federal health care program.
Waiver of Beneficiary Coinsurance and Deductible Amounts
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for reduction or waiver of a federal or state
health program beneficiary's obligation to pay coinsurance or
deductible amounts
If the coinsurance or deductible amounts are owed to a
hospital for inpatient hospital services for which Medicare
pays under the prospective payment system, the hospital
must comply with all of the following three standards: a) the
hospital must not later claim the amount reduced or waived
as a bad debt for payment purposes under Medicare or
otherwise shift the burden of the reduction or waiver onto
Medicare, a State health care program, other payers, or
individuals; b) the hospital must offer to reduce or waive the
coinsurance or deductible amounts without regard to the
reason for admission, the length of stay of the beneficiary, or
the diagnostic related group for which the claim for Medicare
reimbursement is filed; c) the hospital's offer to reduce or
waive the coinsurance or deductible amounts must not be
made as part of a price reduction agreement between a
hospital and a third-party payer (including a health plan),
unless the agreement is part of a contract for the furnishing of
items or services to a beneficiary of a Medicare supplemental
policy.
If the coinsurance or deductible amounts are owed by an
individual who qualifies for subsidized services under a
provision of the Public Health Services Act or under titles V or
XIX of the Social Security Act to a federally qualified health
care center or other health care facility under any Public
Health Services Act grant program or under title V of the Act,
the health care center or facility may reduce or waive the
coinsurance or deductible amounts for items or services for
which payment may be made in whole or in part under part B
of Medicare or a State health care program.
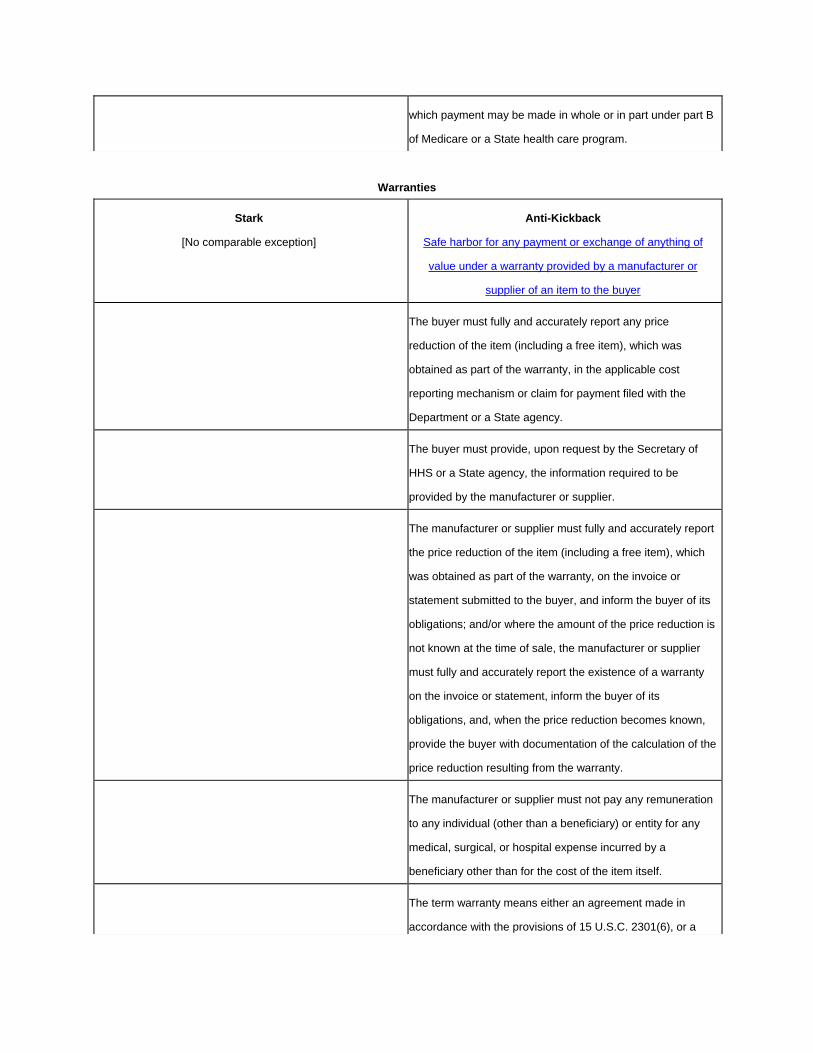
Warranties
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for any payment or exchange of anything of
value under a warranty provided by a manufacturer or
supplier of an item to the buyer
The buyer must fully and accurately report any price
reduction of the item (including a free item), which was
obtained as part of the warranty, in the applicable cost
reporting mechanism or claim for payment filed with the
Department or a State agency.
The buyer must provide, upon request by the Secretary of
HHS or a State agency, the information required to be
provided by the manufacturer or supplier.
The manufacturer or supplier must fully and accurately report
the price reduction of the item (including a free item), which
was obtained as part of the warranty, on the invoice or
statement submitted to the buyer, and inform the buyer of its
obligations; and/or where the amount of the price reduction is
not known at the time of sale, the manufacturer or supplier
must fully and accurately report the existence of a warranty
on the invoice or statement, inform the buyer of its
obligations, and, when the price reduction becomes known,
provide the buyer with documentation of the calculation of the
price reduction resulting from the warranty.
The manufacturer or supplier must not pay any remuneration
to any individual (other than a beneficiary) or entity for any
medical, surgical, or hospital expense incurred by a
beneficiary other than for the cost of the item itself.
The term warranty means either an agreement made in
accordance with the provisions of 15 U.S.C. 2301(6), or a

manufacturer's or supplier's agreement to replace another
manufacturer's or supplier's defective item (which is covered
by an agreement made in accordance with this statutory
provision), on terms equal to the agreement that it replaces.
Personal Services and Management Contracts
Stark
Stark exception to the referral prohibition related to
compensation arrangements for personal services or
management
Anti-Kickback
Safe harbor for remuneration from an entity under an
personal service arrangement or management contract
The arrangement is set out in writing, is signed by the parties,
and specifies the services covered by the arrangement.
The agency agreement covers all of the services the agent
provides to the principal for the term of the agreement and
specifies the services to be provided by the agent.
The arrangement(s) covers all of the services to be furnished
by the physician (or an immediate family member of the
physician) to the entity. This requirement is met if all separate
arrangements between the entity and the physician and the
entity and any family members incorporate each other by
reference or if they cross-reference a master list of contracts
that is maintained and updated centrally and is available for
review by the Secretary of HHS upon request. The master list
must be maintained in a manner that preserves the historical
record of contracts. A physician or family member can
"furnish" services through employees whom they have hired
for the purpose of performing the services; through a wholly-
owned entity; or through locum tenens physicians (as defined
at Sec. 411.351, except that the regular physician need not
be a member of a group practice).
The agency agreement covers all of the services the agent
provides to the principal for the term of the agreement and
specifies the services to be provided by the agent.
The aggregate services contracted for do not exceed those
that are reasonable and necessary for the legitimate
business purposes of the arrangement(s).
If the agency agreement is intended to provide for the
services of the agent on a periodic, sporadic or part-time
basis, rather than on a full-time basis for the term of the
agreement, the agreement specifies exactly the schedule of
such intervals, their precise length, and the exact charge for
such intervals.

The term of each arrangement is for at least 1 year. To meet
this requirement, if an arrangement is terminated during the
term with or without cause, the parties may not enter into the
same or substantially the same arrangement during the first
year of the original term of the arrangement.
The term of the agreement is for not less than one year.
The compensation to be paid over the term of each
arrangement is set in advance, does not exceed fair market
value, and, except in the case of a physician incentive plan
(as defined at Sec. 411.351 of this subpart), is not
determined in a manner that takes into account the volume or
value of any referrals or other business generated between
the parties.
The aggregate compensation paid to the agent over the term
of the agreement is set in advance, is consistent with fair
market value in arms-length transactions and is not
determined in a manner that takes into account the volume or
value of any referrals or business otherwise generated
between the parties for which payment may be made in
whole or in part under Medicare or a State health care
program.
The services to be furnished under each arrangement do not
involve the counseling or promotion of a business
arrangement or other activity that violates any Federal or
State law.
The services performed under the agreement do not involve
the counselling or promotion of a business arrangement or
other activity that violates any state or federal law.
A holdover personal service arrangement for up to 6 months
following the expiration of an agreement of at least 1 year
that met all of the above conditions satisfies the
requirements, provided that the holdover personal service
arrangement is on the same terms and conditions as the
immediately preceding agreement.
The aggregate services contracted for do not exceed those
which are reasonably necessary to accomplish the
commercially reasonable business purpose of the services.
Sale of Practice
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for payments made to a practitioner by another
practitioner where first practitioner is selling a practice to the
second practitioner
The period from the date of the first agreement pertaining to
the sale to the completion of the sale is not more than one

year.
The practitioner who is selling his or her practice will not be in
a professional position to make referrals to, or otherwise
generate business for, the purchasing practitioner for which
payment may be made in whole or in part under Medicare or
a State health care program after one year from the date of
the first agreement pertaining to the sale.
Remuneration under this provision does not include any
payment made to a practitioner by a hospital or other entity
where the practitioner is selling his or her practice to the
hospital or other entity, so long as the following four
standards are met: a) the period from the date of the first
agreement pertaining to the sale to the completion date of the
sale is not more than three years; b) the practitioner who is
selling his or her practice will not be in a professional position
after completion of the sale to make or influence referrals to,
or otherwise generate business for, the purchasing hospital
or entity for which payment may be made in whole or in part
under Medicare or a State health care program; c) the
practice being acquired must be located in a Health
Professional Shortage Area (HPSA), as defined in
Departmental regulations, for the practitioner's specialty area;
d) commencing at the time of the first agreement pertaining
to the sale, the purchasing hospital or entity must diligently
and in good faith engage in commercially reasonable
recruitment activities that may reasonably be expected to
result in the recruitment of a new practitioner to take over the
acquired practice within a one year period and will satisfy the
conditions of the practitioner recruitment safe harbor.
Referral Services
Stark
Stark exception to the referral prohibition related to
compensation arrangements for referral services
Anti-Kickback
Safe harbor for payments between an individual or entity
("participant") and another entity serving as a referral source

("referral service")
Remuneration that meets all of the conditions in the anti-
kickback safe harbor for referral services.
The referral service does not exclude as a participant in the
referral service any individual or entity who meets the
qualifications for participation.
Any payment the participant makes to the referral service is
assessed equally against and collected equally from all
participants, and is only based on the cost of operating the
referral service, and not on the volume or value of any
referrals to or business otherwise generated by either party
for the other party for which payment may be made in whole
or in part under Medicare or a State health care program.
The referral service imposes no requirements on the manner
in which the participant provides services to a referred
person, except that the referral service may require that the
participant charge the person referred at the same rate as it
charges other persons not referred by the referral service, or
that these services be furnished free of charge or at reduced
charge.
The referral service makes the following five disclosures to
each person seeking a referral, with each such disclosure
maintained by the referral service in a written record
certifying such disclosure and signed by either such person
seeking a referral or by the individual making the disclosure
on behalf of the referral service: a) the manner in which it
selects the group of participants in the referral service to
which it could make a referral; b) whether the participant has
paid a fee to the referral service; c) the manner in which it
selects a particular participant from this group for that person;
d) the nature of the relationship between the referral service
and the group of participants to whom it could make the
referral; and e) the nature of any restrictions that would
exclude such an individual or entity from continuing as a
participant.
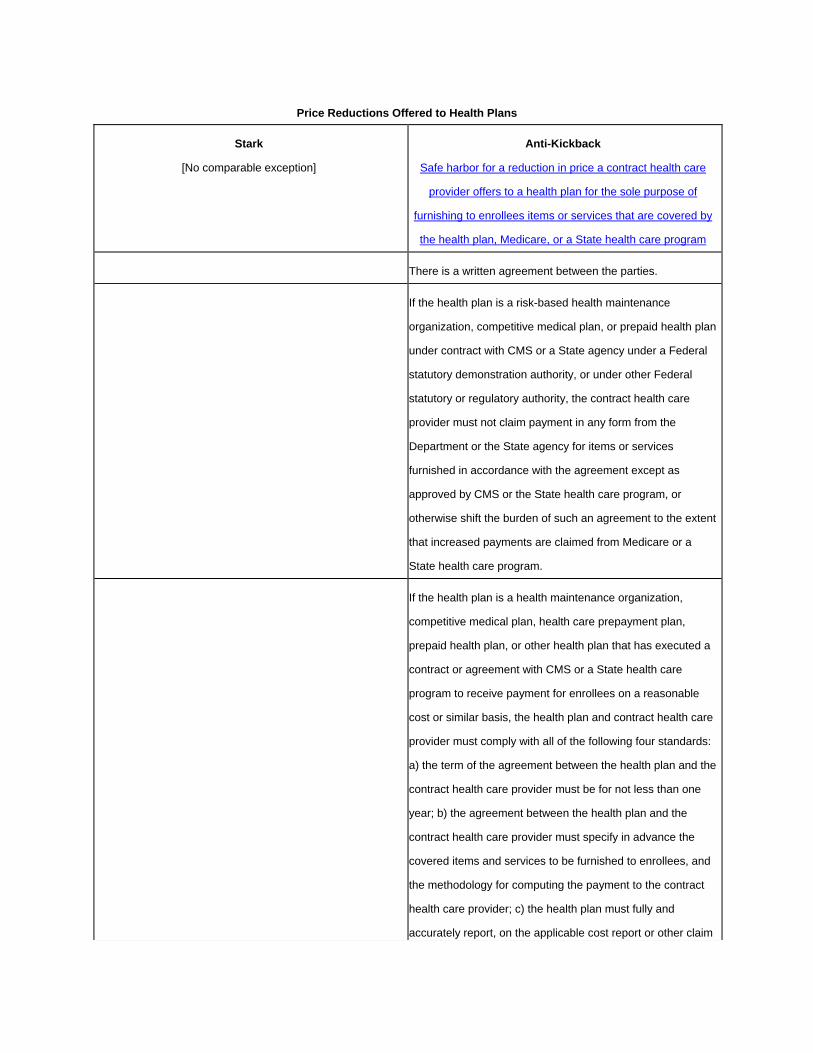
Price Reductions Offered to Health Plans
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for a reduction in price a contract health care
provider offers to a health plan for the sole purpose of
furnishing to enrollees items or services that are covered by
the health plan, Medicare, or a State health care program
There is a written agreement between the parties.
If the health plan is a risk-based health maintenance
organization, competitive medical plan, or prepaid health plan
under contract with CMS or a State agency under a Federal
statutory demonstration authority, or under other Federal
statutory or regulatory authority, the contract health care
provider must not claim payment in any form from the
Department or the State agency for items or services
furnished in accordance with the agreement except as
approved by CMS or the State health care program, or
otherwise shift the burden of such an agreement to the extent
that increased payments are claimed from Medicare or a
State health care program.
If the health plan is a health maintenance organization,
competitive medical plan, health care prepayment plan,
prepaid health plan, or other health plan that has executed a
contract or agreement with CMS or a State health care
program to receive payment for enrollees on a reasonable
cost or similar basis, the health plan and contract health care
provider must comply with all of the following four standards:
a) the term of the agreement between the health plan and the
contract health care provider must be for not less than one
year; b) the agreement between the health plan and the
contract health care provider must specify in advance the
covered items and services to be furnished to enrollees, and
the methodology for computing the payment to the contract
health care provider; c) the health plan must fully and
accurately report, on the applicable cost report or other claim

form filed with the Department or the State health care
program, the amount it has paid the contract health care
provider under the agreement for the covered items and
services furnished to enrollees; and d) the contract health
care provider must not claim payment in any form from the
Department or the State health care program for items or
services furnished in accordance with the agreement except
as approved by CMS or the State health care program, or
otherwise shift the burden of such an agreement to the extent
that increased payments are claimed from Medicare or a
State health care program.
If the health plan is not described in two paragraphs above
and the contract health care provider is not paid on an at-risk,
capitated basis, both the health plan and contract health care
provider must comply with all of the following six standards:
a) the term of the agreement between the health plan and the
contract health care provider must be for not less than one
year; b) the agreement between the health plan and the
contract health care provider must specify in advance the
covered items and services to be furnished to enrollees,
which party is to file claims or requests for payment with
Medicare or the State health care program for such items and
services, and the schedule of fees the contract health care
provider will charge for furnishing such items and services to
enrollees; c) the fee schedule contained in the agreement
between the health plan and the contract health care provider
must remain in effect throughout the term of the agreement,
unless a fee increase results directly from a payment update
authorized by Medicare or the State health care program; d)
the party submitting claims or requests for payment from
Medicare or the State health care program for items and
services furnished in accordance with the agreement must
not claim or request payment for amounts in excess of the
fee schedule; e) the contract health care provider and the
health plan must fully and accurately report on any cost
report filed with Medicare or a State health care program the
fee schedule amounts charged in accordance with the
agreement and, upon request, will report to the Medicare or a
State health care program the terms of the agreement and
the amounts paid in accordance with the agreement; and f)
the party to the agreement, which does not have the
responsibility under the agreement for filing claims or
requests for payment, must not claim or request payment in
any form from the Department or the State health care
program for items or services furnished in accordance with
the agreement, or otherwise shift the burden of such an
agreement to the extent that increased payments are claimed
from Medicare or a State health care program.
If the health plan is not described in the first two paragraphs
above, and the contract health care provider is paid on an at-
risk, capitated basis, both the health plan and contract health
care provider must comply with all of the following five
standards: a) the term of the agreement between the health
plan and the contract health provider must be for not less
than one year; b) the agreement between the health plan and
the contract health provider must specify in advance the
covered items and services to be furnished to enrollees and
the total amount per enrollee (which may be expressed in a
per month or other time period basis) the contract health care
provider will be paid by the health plan for furnishing such
items and services to enrollees and must set forth any
copayments, if any, to be paid by enrollees to the contract
health care provider for covered services; c) the payment
amount contained in the agreement between the health care
plan and the contract health care provider must remain in
effect throughout the term of the agreement; d) the contract
health care provider and the health plan must fully and
accurately report to the Medicare and State health care
program upon request, the terms of the agreement and the
amounts paid in accordance with the agreement; and e) the
contract health care provider must not claim or request
payment in any form from the Department, a State health
care program or an enrollee (other than copayment amounts
described in (b) and the health plan must not pay the contract
care provider in excess of the amounts described in (b) for
items and services covered by the agreement.
Medical Staff Incidental Benefits
Stark
Stark exception to the referral prohibition related to
compensation arrangements from a hospital to a member of
its medical staff
Anti-Kickback
[No comparable safe harbor]
The compensation is in the form of items or services (not
including cash or cash equivalents) from a hospital to a
member of its medical staff when the item or service is used
on the hospital's campus.
The compensation is provided to all members of the medical
staff practicing in the same specialty (but not necessarily
accepted by every member to whom it is offered) without
regard to the volume or value of referrals or other business
generated between the parties.
Except with respect to identification of medical staff on a
hospital Web site or in hospital advertising, the compensation
is provided only during periods when the medical staff
members are making rounds or are engaged in other
services or activities that benefit the hospital or its patients.
The compensation is provided by the hospital and used by
the medical staff members only on the hospital's campus.
Compensation, including, but not limited to, Internet access,
pagers, or two-way radios, used away from the campus only
to access hospital medical records or information or to
access patients or personnel who are on the hospital
campus, as well as the identification of the medical staff on a
hospital web site or in hospital advertising, will meet the "on

campus" requirement.
The compensation is reasonably related to the provision of,
or designed to facilitate directly or indirectly the delivery of,
medical services at the hospital.
The compensation is of low value (that is, less than $25) with
respect to each occurrence of the benefit (for example, each
meal given to a physician while he or she is serving patients
who are hospitalized must be of low value). The $25 limit in
this paragraph (m)(5) will be adjusted each calendar year to
the nearest whole dollar by the increase in the Consumer
Price Index-Urban All Items (CPI-U) for the 12-month period
ending the preceding September 30. CMS intends to display
as soon as possible after September 30 each year both the
increase in the CPI-U for the 12-month period and the new
limits on the physician self- referral Web site.
The compensation is not determined in any manner that
takes into account the volume or value of referrals or other
business generated between the parties.
The compensation arrangement does not violate the anti-
kickback statute or any federal or state law or regulation
governing billing or claims submission.
Other facilities and health care clinics (including, but not
limited to, federally qualified health centers) that have bona
fide medical staffs may provide compensation under this
paragraph on the same terms and conditions applied to
hospitals.
Risk Sharing Arrangements
Stark
Stark exception to the referral prohibition related to a
compensation arrangement that is a risk- sharing
arrangement (including, but not limited to, withholds,
bonuses, and risk pools)
Anti-Kickback [No comparable safe harbor]
The arrangement is between a managed care organization or
an independent physicians association and a physician
(either directly or indirectly through a subcontractor) for
services provided to enrollees of a health plan.
The arrangement does not violate the federal anti-kickback
statute or any law or regulation governing billing or claims
submission.
"Health plan" and "enrollees" have the meanings ascribed to
those terms in the anti-kickback regulations.
Compliance Training
Stark
Stark exception to the referral prohibition related to a
compensation arrangement for compliance training
Anti-Kickback
[No comparable safe harbor]
The training is provided by an entity to a physician (or to the
physician's immediate family member or office staff) who
practices in the entity's local community or service area.
The training is held in the local community or service area.
"Compliance training" means training regarding the basic
elements of a compliance program (for example, establishing
policies and procedures, training of staff, internal monitoring,
or reporting); specific training regarding the requirements of
Federal and State health care programs (for example, billing,
coding, reasonable and necessary services, documentation,
or unlawful referral arrangements); or training regarding other
Federal, State, or local laws, regulations, or rules governing
the conduct of the party for whom the training is provided.
"Compliance training'' also includes programs that offer
continuing medical education credit, provided that
compliance training is the primary purpose of the program.
Indirect Compensation Arrangements
Stark
Stark exception to the referral prohibition related to a
compensation arrangement for indirect compensation
Anti-Kickback
[No comparable safe harbor]

arrangements
The arrangement is an indirect compensation arrangement.
The compensation received by the referring physician (or
immediate family member) described in §411.354(c)(2)(ii) is
fair market value for services and items actually provided and
not determined in any manner that takes into account the
volume or value of referrals or other business generated by
the referring physician for the entity furnishing DHS.
Compensation for the rental of office space or equipment
may not be determined using a formula based on-- (A) A
percentage of the revenue raised, earned, billed, collected, or
otherwise attributable to the services performed or business
generated in the office space or to the services performed or
business generated through the use of the equipment; or (B)
Per-unit of service rental charges, to the extent that such
charges reflect services provided to patients referred
between the parties.
The indirect compensation arrangement is set out in writing,
signed by the parties, and specifies the services covered by
the arrangement, except in the case of a bona fide
employment relationship between an employer and an
employee, in which case the arrangement need not be set
out in a written contract, but must be for identifiable services
and be commercially reasonable even if no referrals are
made to the employer.
The compensation arrangement does not violate the anti-
kickback statute or any laws or regulations governing billing
or claims submission.
Ambulance Restocking: All
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for ambulance restocking programs
The ambulance that is replenished must be used to provide

emergency ambulance services an average of three times
per week, as measured over a reasonable period of time.
Drugs and medical supplies (including linens) initially used by
a first responder and replenished at the scene of the illness
or injury by the ambulance provider that transports the patient
to the hospital or other receiving facility will be deemed to
have been used by the ambulance provider. .
Under no circumstances may the ambulance provider (or first
responder) and the receiving facility both bill for the same
replenished drug or supply. Replenished drugs or supplies
may only be billed (including claiming bad debt) to a Federal
health care program by either the ambulance provider (or first
responder) or the receiving facility.
All billing or claims submission by the receiving facility,
ambulance provider or first responder for replenished drugs
and medical supplies used in connection with the transport of
a Federal health care program beneficiary must comply with
all applicable Federal health care program payment and
coverage rules and regulations. Compliance with this
paragraph will be determined separately for the receiving
facility and the ambulance provider (and first responder, if
any), so long as the receiving facility, ambulance provider (or
first responder) refrains from doing anything that would
impede the other party or parties from meeting their
obligations under this paragraph.
The receiving facility or ambulance provider, or both, must: a)
maintain records of the replenished drugs and medical
supplies and the patient transport to which the replenished
drugs and medical supplies related; b) provide a copy of such
records to the other party within a reasonable time (unless
the other party is separately maintaining records of the
replenished drugs and medical supplies); and c) make those
records available to the Secretary of HHS promptly upon
request. A pre-hospital care report (including, but not limited

to, a trip sheet, patient care report or patient encounter
report) prepared by the ambulance provider and filed with the
receiving facility will meet the requirements of this paragraph,
provided that it documents the specific type and amount of
medical supplies and drugs used on the patient and
subsequently replenished. For purposes of this paragraph,
documentation may be maintained and, if required, filed with
the other party in hard copy or electronically. If a replenishing
arrangement includes linens, documentation need not be
maintained for their exchange. If documentation is not
maintained for the exchange of linens, the receiving facility
will be presumed to have provided an exchange of
comparable clean linens for soiled linens for each ambulance
transport of a patient to the receiving facility. Records
required under this section must be maintained for 5 years.
The replenishing arrangement must not take into account the
volume or value of any referrals or business otherwise
generated between the parties for which payment may be
made in whole or in part under any Federal health care
program (other than the referral of the particular patient to
whom the replenished drugs and medical supplies were
furnished.
The receiving facility and the ambulance provider otherwise
comply with all Federal, State, and local laws regulating
ambulance services, including, but not limited to, emergency
services, and the provision of drugs and medical supplies,
including, but not limited to, laws relating to the handling of
controlled substances.
The arrangement must satisfy all of the standards in one of
three categories: general replenishing, fair market value
replenishing, or government-mandated replenishing.
A receiving facility is a hospital or other facility that provides
emergency medical services. An ambulance provider is a
provider or supplier of ambulance transport services that

provides emergency ambulance services. The term does not
include a provider of ambulance transport services that
provides only non-emergency transport services. A first
responder includes, but is not limited to, a fire department,
paramedic service or search and rescue squad that responds
to an emergency call (through 911 or other emergency
access number) and treats the patient, but does not transport
the patient to the hospital or other receiving facility. An
emergency ambulance service is a transport by ambulance
initiated as a result of a call through 911 or other emergency
access number or a call from another acute care facility
unable to provide the higher level care required by the patient
and available at the receiving facility. Medical supplies
includes linens, unless otherwise provided.
Ambulance Restocking: General Replenishing
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for ambulance restocking programs
The arrangement meets all of the requirements for applicable
to all ambulance restocking arrangements.
The receiving facility must replenish medical supplies or
drugs on an equal basis for all ambulance providers that
bring patients to the receiving facility in any one of the
following categories: a) all ambulance providers that do not
bill any patient or insurer (including Federal health care
programs) for ambulance services, regardless of the payor or
the patient's ability to pay (i.e., ambulance providers, such as
volunteer companies, that provide ambulance services
without charge to any person or entity); b) all not-for-profit
and State or local government ambulance service providers
(including, but not limited to, municipal and volunteer
ambulance services providers); or c) all ambulance service
providers.
A receiving facility may offer replenishing to one or more of
the categories and may offer different replenishing
arrangements to different categories, so long as the
replenishing is conducted uniformly within each category. For
example, a receiving facility may offer to replenish a broader
array of drugs or supplies for ambulance providers that do no
not charge for their services than for ambulance providers
that charge for their services. Within each category, the
receiving facility may limit its replenishing arrangements to
the replenishing of emergency ambulance transports only.
The replenishing arrangement must be conducted in an open
and public manner. A replenishing arrangement will be
considered to be conducted in an open and public manner if
one of the following two conditions are satisfied: a) a written
disclosure of the replenishing program is posted
conspicuously in the receiving facility's emergency room or
other location where the ambulance providers deliver patients
and copies are made available upon request to ambulance
providers, Government representatives, and members of the
public (subject to reasonable photocopying charges). The
written disclosure can take any reasonable form and should
include the category of ambulance service providers that
qualifies for replenishment; the drugs or medical supplies
included in the replenishment program; and the procedures
for documenting the replenishment. No written contracts
between the parties are required; or b) the replenishment
arrangement operates in accordance with a plan or protocol
of general application promulgated by an Emergency Medical
Services (EMS) Council or comparable entity, agency or
organization, provided a copy of the plan or protocol is
available upon request to ambulance providers, Government
representatives and members of the public (subject to
reasonable photocopying charges). While parties are
encouraged to participate in collaborative, comprehensive,
community-wide EMS systems to improve the delivery of
EMS in their local communities, nothing in this paragraph

shall be construed as requiring the involvement of such
organizations or the development or implementation of
ambulance replenishment plans or protocols by such
organizations.
Disclosure of confidential proprietary or financial information
related to the replenishing arrangement (including, but not
limited to, information about cost, pricing or the volume of
replenished drugs or supplies) to ambulance providers or
members of the general public is not required.
Ambulance Restocking: Fair Market Value Replenishing
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for ambulance restocking programs
The arrangement meets all of the requirements for applicable
to all ambulance restocking arrangements
The ambulance provider must pay the receiving facility fair
market value, based on an arms-length transaction, for
replenished medical supplies.
If payment is not made at the same time as the replenishing
of the medical supplies, the receiving facility and the
ambulance provider must make commercially reasonable
payment arrangements in advance.
Ambulance Restocking: Government Mandated Replenishing
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for ambulance restocking programs
The arrangement meets all of the requirements for applicable
to all ambulance restocking arrangements.
The replenishing arrangement is undertaken in accordance
with a State or local statute, ordinance, regulation or binding
protocol that requires hospitals or receiving facilities in the
area subject to such requirement to replenish ambulances
that deliver patients to the hospital with drugs or medical

supplies (including linens) that are used during the transport
of that patient.
Physician Services
Stark
Stark exception to the referral prohibition related to both
ownership/investment and compensation arrangements for
certain physician services
Anti-Kickback
[No comparable safe harbor
The services are physicians' services, including diagnosis,
therapy, surgery, consultations, and home, office, and
institutional calls.
The services are provided a) personally by another physician
who is a member of the referring physician's group practice
or is a physician in the same group practice as the referring
physician; or b) under the supervision of another physician
who is a member of the referring physician's group practice
or is a physician in the same group practice as the referring
physician, provided that the supervision complies with all
other applicable Medicare payment and coverage rules for
the physician services.
"Physician services'" includes only those "incident to"
services ( the services or supplies are furnished as an
integral, although incidental, part of the physician's personal
professional services in the course of diagnosis or treatment
of an injury or illness) that are physician services. All other
"incident to'" services (for example, diagnostic tests, physical
therapy) are outside the scope of this section.
Increased Coverage, Reduced Cost-Sharing Amounts, or Reduced Premium Amounts Offered by Health Plans
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for increased coverage, reduced cost-sharing
amounts, or reduced premium amounts offered by health
plans

If the health plan is a risk-based health maintenance
organization, competitive medical plan, prepaid health plan,
or other health plan under contract with CMS or a State
health care program and operating under a Federal statutory
demonstration authority, or under other Federal statutory or
regulatory authority, it must offer the same increased
coverage or reduced cost-sharing or premium amounts to all
Medicare or State health care program enrollees covered by
the contract unless otherwise approved by CMS or by a State
health care program.
If the health plan is a health maintenance organization,
competitive medical plan, health care prepayment plan,
prepaid health plan or other health plan that has executed a
contract or agreement with CMS or with a State health care
program to receive payment for enrollees on a reasonable
cost or similar basis, it must comply with both of the following
two standards: a) the health plan must offer the same
increased coverage or reduced cost-sharing or premium
amounts to all Medicare or State health care program
enrollees covered by the contract or agreement unless
otherwise approved by CMS or by a State health care
program; and b) the health plan must not claim the costs of
the increased coverage or the reduced cost-sharing or
premium amounts as a bad debt for payment purposes under
Medicare or a State health care program or otherwise shift
the burden of the increased coverage or reduced cost-
sharing or premium amounts to the extent that increased
payments are claimed from Medicare or a State health care
program.
Obstetrical Malpractice Insurance Subsidies
Stark
Stark exception to the referral prohibition related to
compensation arrangements for obstetrical malpractice
insurance subsidiaries
Anti-Kickback
Safe harbor for obstetrical malpractice insurance subsidies
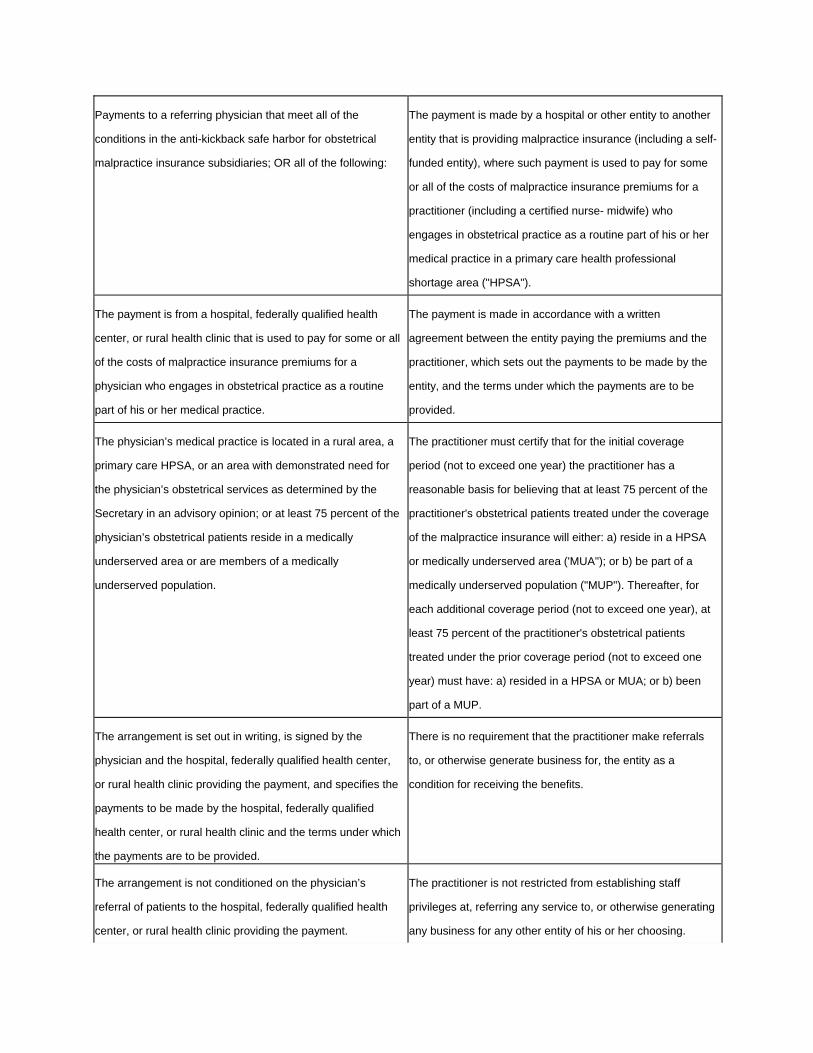
Payments to a referring physician that meet all of the
conditions in the anti-kickback safe harbor for obstetrical
malpractice insurance subsidiaries; OR all of the following:
The payment is made by a hospital or other entity to another
entity that is providing malpractice insurance (including a self-
funded entity), where such payment is used to pay for some
or all of the costs of malpractice insurance premiums for a
practitioner (including a certified nurse- midwife) who
engages in obstetrical practice as a routine part of his or her
medical practice in a primary care health professional
shortage area ("HPSA").
The payment is from a hospital, federally qualified health
center, or rural health clinic that is used to pay for some or all
of the costs of malpractice insurance premiums for a
physician who engages in obstetrical practice as a routine
part of his or her medical practice.
The payment is made in accordance with a written
agreement between the entity paying the premiums and the
practitioner, which sets out the payments to be made by the
entity, and the terms under which the payments are to be
provided.
The physician’s medical practice is located in a rural area, a
primary care HPSA, or an area with demonstrated need for
the physician’s obstetrical services as determined by the
Secretary in an advisory opinion; or at least 75 percent of the
physician’s obstetrical patients reside in a medically
underserved area or are members of a medically
underserved population.
The practitioner must certify that for the initial coverage
period (not to exceed one year) the practitioner has a
reasonable basis for believing that at least 75 percent of the
practitioner's obstetrical patients treated under the coverage
of the malpractice insurance will either: a) reside in a HPSA
or medically underserved area ('MUA"); or b) be part of a
medically underserved population ("MUP"). Thereafter, for
each additional coverage period (not to exceed one year), at
least 75 percent of the practitioner's obstetrical patients
treated under the prior coverage period (not to exceed one
year) must have: a) resided in a HPSA or MUA; or b) been
part of a MUP.
The arrangement is set out in writing, is signed by the
physician and the hospital, federally qualified health center,
or rural health clinic providing the payment, and specifies the
payments to be made by the hospital, federally qualified
health center, or rural health clinic and the terms under which
the payments are to be provided.
There is no requirement that the practitioner make referrals
to, or otherwise generate business for, the entity as a
condition for receiving the benefits.
The arrangement is not conditioned on the physician’s
referral of patients to the hospital, federally qualified health
center, or rural health clinic providing the payment.
The practitioner is not restricted from establishing staff
privileges at, referring any service to, or otherwise generating
any business for any other entity of his or her choosing.
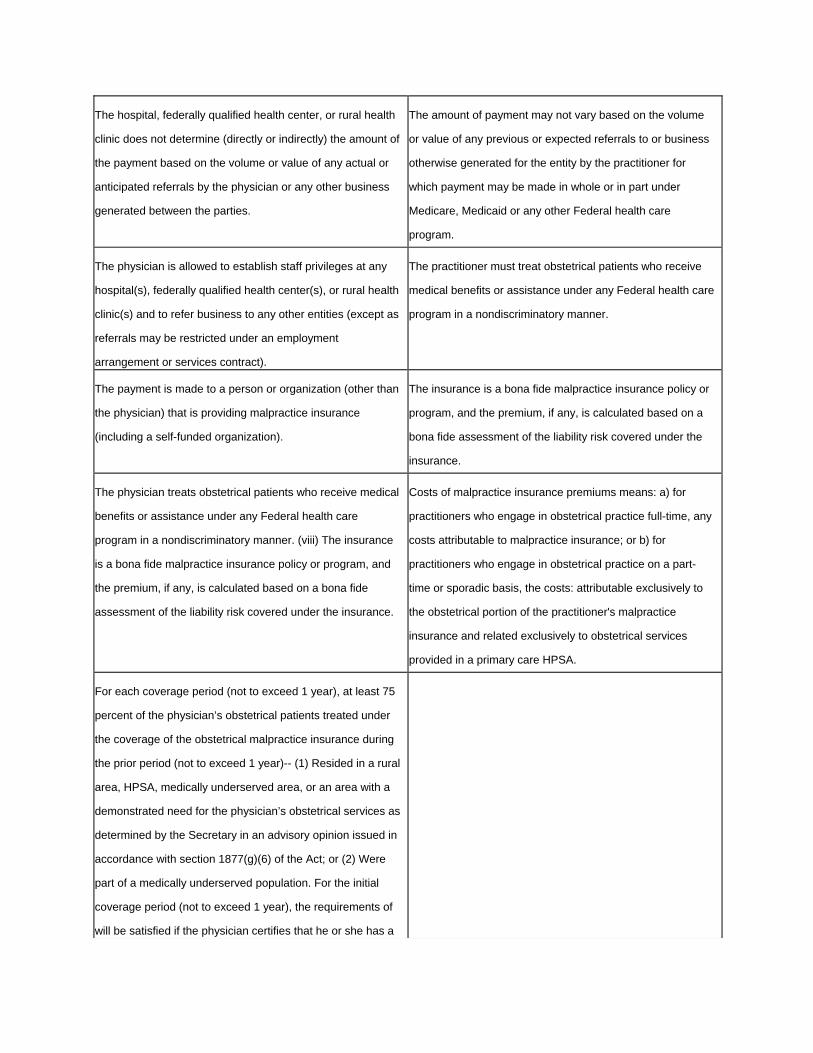
The hospital, federally qualified health center, or rural health
clinic does not determine (directly or indirectly) the amount of
the payment based on the volume or value of any actual or
anticipated referrals by the physician or any other business
generated between the parties.
The amount of payment may not vary based on the volume
or value of any previous or expected referrals to or business
otherwise generated for the entity by the practitioner for
which payment may be made in whole or in part under
Medicare, Medicaid or any other Federal health care
program.
The physician is allowed to establish staff privileges at any
hospital(s), federally qualified health center(s), or rural health
clinic(s) and to refer business to any other entities (except as
referrals may be restricted under an employment
arrangement or services contract).
The practitioner must treat obstetrical patients who receive
medical benefits or assistance under any Federal health care
program in a nondiscriminatory manner.
The payment is made to a person or organization (other than
the physician) that is providing malpractice insurance
(including a self-funded organization).
The insurance is a bona fide malpractice insurance policy or
program, and the premium, if any, is calculated based on a
bona fide assessment of the liability risk covered under the
insurance.
The physician treats obstetrical patients who receive medical
benefits or assistance under any Federal health care
program in a nondiscriminatory manner. (viii) The insurance
is a bona fide malpractice insurance policy or program, and
the premium, if any, is calculated based on a bona fide
assessment of the liability risk covered under the insurance.
Costs of malpractice insurance premiums means: a) for
practitioners who engage in obstetrical practice full-time, any
costs attributable to malpractice insurance; or b) for
practitioners who engage in obstetrical practice on a part-
time or sporadic basis, the costs: attributable exclusively to
the obstetrical portion of the practitioner's malpractice
insurance and related exclusively to obstetrical services
provided in a primary care HPSA.
For each coverage period (not to exceed 1 year), at least 75
percent of the physician’s obstetrical patients treated under
the coverage of the obstetrical malpractice insurance during
the prior period (not to exceed 1 year)-- (1) Resided in a rural
area, HPSA, medically underserved area, or an area with a
demonstrated need for the physician’s obstetrical services as
determined by the Secretary in an advisory opinion issued in
accordance with section 1877(g)(6) of the Act; or (2) Were
part of a medically underserved population. For the initial
coverage period (not to exceed 1 year), the requirements of
will be satisfied if the physician certifies that he or she has a

reasonable expectation that at least 75 percent of the
physician's obstetrical patients treated under the coverage of
the malpractice insurance will— (1) Reside in a rural area,
HPSA, medically underserved area, or an area with a
demonstrated need for the physician’s obstetrical services as
determined by the Secretary in an advisory opinion; or (2) Be
part of a medically underserved population.
The arrangement does not violate the anti-kickback statute of
the Act), or any Federal or State law or regulation governing
billing or claims submission.
The costs of malpractice insurance premiums means: (i) For
physicians who engage in obstetrical practice on a full-time
basis, any costs attributable to malpractice insurance; or (ii)
For physicians who engage in obstetrical practice on a part-
time or sporadic basis, the costs attributable exclusively to
the obstetrical portion of the physician's malpractice
insurance, and related exclusively to obstetrical services
provided-- (A) In a rural area, primary care HPSA, or an area
with demonstrated need for the physician’s obstetrical
services, as determined by the Secretary in an advisory
opinion; or (B) In any area, provided that at least 75 percent
of the physician's obstetrical patients treated in the coverage
period (not to exceed 1 year) resided in a rural area or
medically underserved area or were part of a medically
underserved population.
Referral Agreements for Specialty Services
Stark
[No comparable exemption]
Anti-Kickback
Safe harbor for specialty service referral agreements
The agreement is for one party to refer a patient to the other
party for the provision of a specialty service payable in whole
or in part under Medicare or a State health care program in
return for an agreement on the part of the other party to refer
that patient back at a mutually agreed upon time or
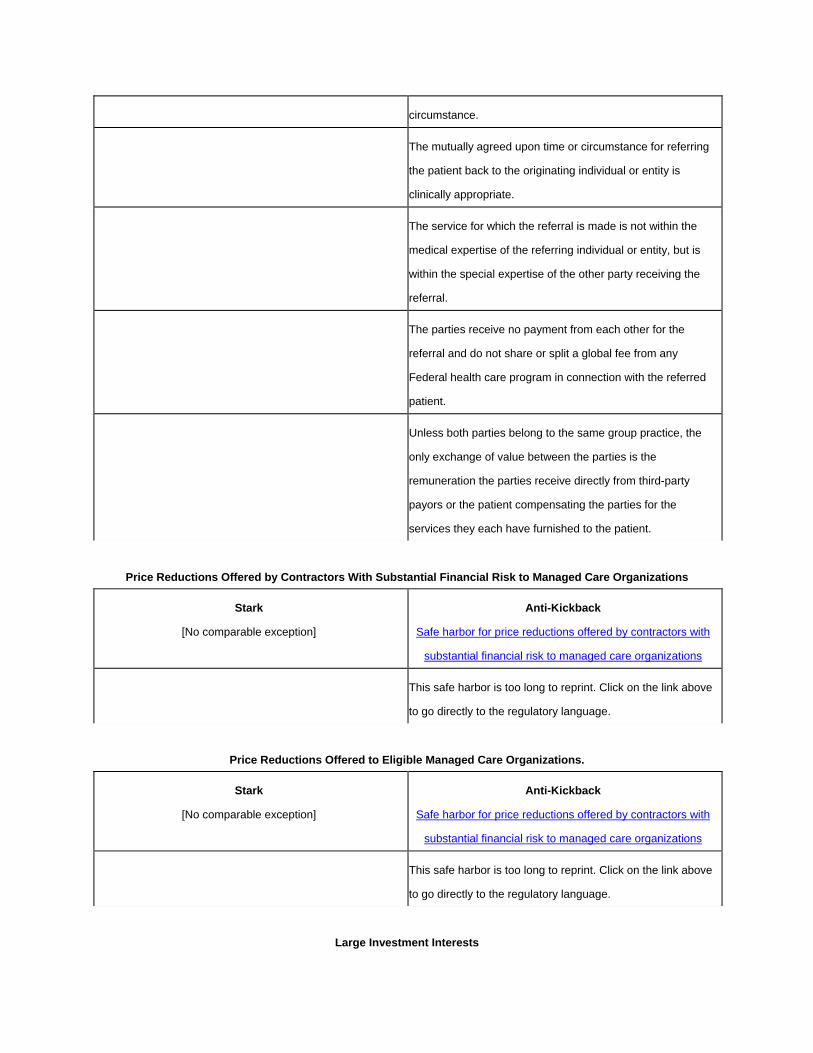
circumstance.
The mutually agreed upon time or circumstance for referring
the patient back to the originating individual or entity is
clinically appropriate.
The service for which the referral is made is not within the
medical expertise of the referring individual or entity, but is
within the special expertise of the other party receiving the
referral.
The parties receive no payment from each other for the
referral and do not share or split a global fee from any
Federal health care program in connection with the referred
patient.
Unless both parties belong to the same group practice, the
only exchange of value between the parties is the
remuneration the parties receive directly from third-party
payors or the patient compensating the parties for the
services they each have furnished to the patient.
Price Reductions Offered by Contractors With Substantial Financial Risk to Managed Care Organizations
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for price reductions offered by contractors with
substantial financial risk to managed care organizations
This safe harbor is too long to reprint. Click on the link above
to go directly to the regulatory language.
Price Reductions Offered to Eligible Managed Care Organizations.
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for price reductions offered by contractors with
substantial financial risk to managed care organizations
This safe harbor is too long to reprint. Click on the link above
to go directly to the regulatory language.
Large Investment Interests

Stark
Stark exception to the referral prohibition related to
ownership or investment interests
Anti-Kickback
Safe harbor for certain investment interests
The ownership of must be of investment securities (including
shares or bonds, debentures, notes, or other debt
instruments) that at the time the designated health service
referral was made could be purchased on the open market.
The investment is in an entity with more than $50,000,000 in
undepreciated net tangible assets (based on the net
acquisition cost of purchasing such assets from an unrelated
entity) related to the furnishing of health care items and
services.
The investment securities are a) listed for trading on the New
York Stock Exchange, the American Stock Exchange, or any
regional exchange in which quotations are published on a
daily basis, or foreign securities listed on a recognized
foreign, national, or regional exchange in which quotations
are published on a daily basis; or b) traded under an
automated interdealer quotation system operated by the
National Association of Securities Dealers.
With respect to an investment interest that is an equity
security, the equity security must be registered with the
Securities and Exchange Commission.
The investment securities are in a corporation that had
stockholder equity exceeding $75 million at the end of the
corporation's most recent fiscal year or on average during the
previous 3 fiscal years. "Stockholder equity" is the difference
in value between a corporation's total assets and total
liabilities.
The investment interest of an investor in a position to make
or influence referrals to, furnish items or services to, or
otherwise generate business for the entity must be obtained
on terms (including any direct or indirect transferability
restrictions) and at a price equally available to the public
when trading on a registered securities exchange, such as
the New York Stock Exchange or the American Stock
Exchange, or in accordance with the National Association of
Securities Dealers Automated Quotation System.
The entity or any investor must not market or furnish the
entity's items or services (or those of another entity as part of
a cross referral agreement) to passive investors differently
than to non- investors.
The entity or any investor (or other individual or entity acting
on behalf of the entity or any investor in the entity) must not
loan funds to or guarantee a loan for an investor who is in a
position to make or influence referrals to, furnish items or
services to, or otherwise generate business for the entity if

the investor uses any part of such loan to obtain the
investment interest.
The amount of payment to an investor in return for the
investment interest must be directly proportional to the
amount of the capital investment of that investor.
Mutual Funds
Stark
Stark exception to the referral prohibition related to
ownership or investment interests for mutual funds
Anti-Kickback
[No comparable safe harbor]
Investment or ownership of shares in a regulated investment
company as defined in section 851(a) of the Internal
Revenue Code of 1986, if the company had, at the end of its
most recent fiscal year, or on average during the previous 3
fiscal years, total assets exceeding $75 million.
Investment Interests in Entity With Investment Interests Held by Either Active or Passive Investors
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for certain investment interests
The investment is in an entity which possesses investment
interests that are held by either active or passive investors.
No more than 40 percent of the value of the investment
interests of each class of investment interests may be held in
the previous fiscal year or previous 12 month period by
investors who are in a position to make or influence referrals
to, furnish items or services to, or otherwise generate
business for the entity. Equivalent classes of equity
investments may be combined, and equivalent classes of
debt instruments may be combined.
The terms on which an investment interest is offered to a
passive investor, if any, who is in a position to make or
influence referrals to, furnish items or services to, or
otherwise generate business for the entity must be no

different from the terms offered to other passive investors.
The terms on which an investment interest is offered to an
investor who is in a position to make or influence referrals to,
furnish items or services to, or otherwise generate business
for the entity must not be related to the previous or expected
volume of referrals, items or services furnished, or the
amount of business otherwise generated from that investor to
the entity.
There is no requirement that a passive investor, if any, make
referrals to, be in a position to make or influence referrals to,
furnish items or services to, or otherwise generate business
for the entity as a condition for remaining as an investor.
The entity or any investor must not market or furnish the
entity's items or services (or those of another entity as part of
a cross referral agreement) to passive investors differently
than to non- investors.
No more than 40 percent of the entity's gross revenue related
to the furnishing of health care items and services in the
previous fiscal year or previous 12-month period may come
from referrals or business otherwise generated from
investors.
The entity or any investor (or other individual or entity acting
on behalf of the entity or any investor in the entity) must not
loan funds to or guarantee a loan for an investor who is in a
position to make or influence referrals to, furnish items or
services to, or otherwise generate business for the entity if
the investor uses any part of such loan to obtain the
investment interest.
The amount of payment to an investor in return for the
investment interest must be directly proportional to the
amount of the capital investment (including the fair market
value of any pre- operational services rendered) of that
investor.
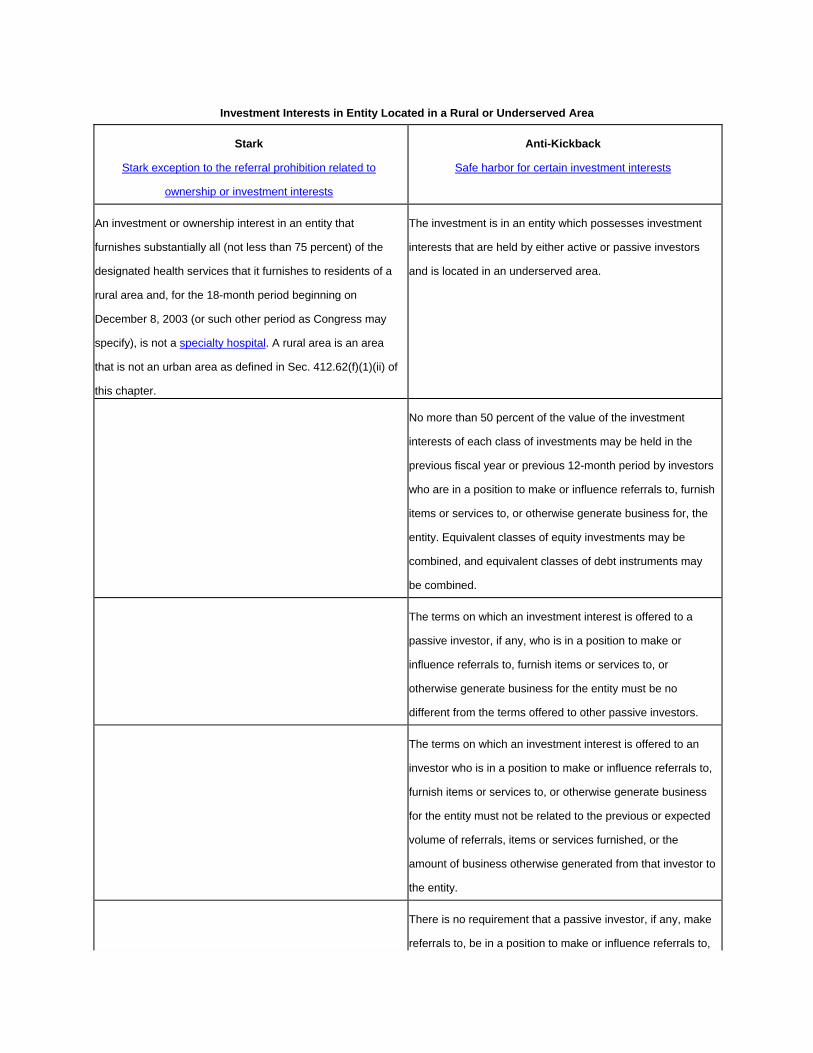
Investment Interests in Entity Located in a Rural or Underserved Area
Stark
Stark exception to the referral prohibition related to
ownership or investment interests
Anti-Kickback
Safe harbor for certain investment interests
An investment or ownership interest in an entity that
furnishes substantially all (not less than 75 percent) of the
designated health services that it furnishes to residents of a
rural area and, for the 18-month period beginning on
December 8, 2003 (or such other period as Congress may
specify), is not a specialty hospital. A rural area is an area
that is not an urban area as defined in Sec. 412.62(f)(1)(ii) of
this chapter.
The investment is in an entity which possesses investment
interests that are held by either active or passive investors
and is located in an underserved area.
No more than 50 percent of the value of the investment
interests of each class of investments may be held in the
previous fiscal year or previous 12-month period by investors
who are in a position to make or influence referrals to, furnish
items or services to, or otherwise generate business for, the
entity. Equivalent classes of equity investments may be
combined, and equivalent classes of debt instruments may
be combined.
The terms on which an investment interest is offered to a
passive investor, if any, who is in a position to make or
influence referrals to, furnish items or services to, or
otherwise generate business for the entity must be no
different from the terms offered to other passive investors.
The terms on which an investment interest is offered to an
investor who is in a position to make or influence referrals to,
furnish items or services to, or otherwise generate business
for the entity must not be related to the previous or expected
volume of referrals, items or services furnished, or the
amount of business otherwise generated from that investor to
the entity.
There is no requirement that a passive investor, if any, make
referrals to, be in a position to make or influence referrals to,
furnish items or services to, or otherwise generate business
for the entity as a condition for remaining as an investor.
The entity or any investor must not market or furnish the
entity's items or services (or those of another entity as part of
a cross-referral agreement) to passive investors differently
than to non- investors.
At least 75 percent of the dollar volume of the entity's
business in the previous fiscal year or previous 12-month
period must be derived from the service of persons who
reside in an underserved area or are members of medically
underserved populations.
The entity or any investor (or other individual or entity acting
on behalf of the entity or any investor in the entity) must not
loan funds to or guarantee a loan for an investor who is in a
position to make or influence referrals to, furnish items or
services to, or otherwise generate business for the entity if
the investor uses any part of such loan to obtain the
investment interest.
The amount of payment to an investor in return for the
investment interest must be directly proportional to the
amount of the capital investment (including the fair market
value of any pre- operational services rendered) of that
investor.
If an entity that otherwise meets all of the above standards is
located in an area that was an underserved area at the time
of the initial investment, but subsequently ceases to be an
underserved area, the entity will be deemed to comply with
this section for a period equal to the lesser of: a) the current
term of the investment remaining after the date upon which
the area ceased to be an underserved area; or b) three years
from the date the area ceased to be an underserved area.
Hospital Investment or Ownership

Stark
Stark exception to the referral prohibition related to
ownership or investment interests for certain hospital
investments
Anti-Kickback
[No comparable safe harbor]
NOTE: This exception has been significantly changed by
the Patient Protection and Affordable Care Act. Review
the changes
Investment or ownership in a hospital if: a) the referring
physician is authorized to perform services at the hospital; b)
effective for the 18-month period beginning on December 8,
2003 (or such other period as Congress may specify), the
hospital is not a specialty hospital; and c) the ownership or
investment interest is in the entire hospital and not merely in
a distinct part or department of the hospital.
Preventive Screening Tests, Immunizations, and Vaccines
Stark
Stark exception related to both ownership/investment and
compensation
Anti-Kickback
[No comparable safe harbor
The preventive screening tests, immunizations, and vaccines
must be covered by Medicare and must be listed as eligible
for this exception on the List of CPT/HCPCS Codes.
The preventive screening tests, immunizations, and vaccines
are subject to CMS-mandated frequency limits.
The arrangement for the provision of the preventive
screening tests, immunizations, and vaccines does not
violate the anti-kickback statute.
All billing and claims submission for the preventive screening
tests, immunizations, and vaccines does not violate any
federal or state law or regulation governing billing or claims
submission.
Eyeglasses and Contact Lenses Following Cataract Surgery
Stark
Stark exception related to both ownership/investment and
compensation
Anti-Kickback
[No comparable safe harbor]
The eyeglasses and contact lenses are covered by Medicare
when furnished to patients following cataract surgery.
The eyeglasses or contact lenses are provided in accordance
with the coverage and payment provisions set forth in Sec.
410.36(a)(2)(ii) and Sec. 414.228.
The arrangement for the furnishing of the eyeglasses or
contact lenses does not violate the federal anti-kickback
statute.
Billing and claims submission for the eyeglasses or contact
lenses complies with all federal and state laws and
regulations.
EPO and Other Dialysis-Related Drugs Furnished in or by an ESRD Facility
Stark
Stark exception related to both ownership/investment and
compensation
Anti-Kickback
[No comparable safe harbor
The EPO and other dialysis-related drugs are furnished in or
by an ESRD facility. " EPO and other dialysis-related drugs"
means certain outpatient prescription drugs that are required
for the efficacy of dialysis and identified as eligible for this
exception on the List of CPT/HCPCS Codes; and "furnished"
means that the EPO or dialysis-related drugs are
administered to a patient in the ESRD facility, or, in the case
of EPO or Aranesp (or equivalent drug identified on the List
of CPT/HCPCS Codes) only, are dispensed by the ESRD
facility for use at home.
The arrangement for the furnishing of the EPO and other
dialysis-related drugs does not violate the anti-kickback
statute.
All billing and claims submission for the EPO and other
dialysis-related drugs does not violate any Federal or State
law or regulation governing billing or claims submission.
This exception does not apply to any financial relationships
between the referring physician and any entity other than the
ESRD facility that furnishes the EPO and other dialysis-
related drugs to the patient.
Implants in an ASC
Stark
Stark exception related to both ownership/investment and
compensation
Anti-Kickback
[No comparable safe harbor]
Implants are furnished by an ambulatory surgery center and
include, but are not limited to, cochlear implants, intraocular
lenses, and other implanted prosthetics, implanted prosthetic
devices, and implanted DME.
The implant is implanted by the referring physician or a
member of the referring physician's group practice in a
Medicare-certified ASC with which the referring physician has
a financial relationship.
The implant is implanted in the patient during a surgical
procedure paid by Medicare to the ASC as an ASC
procedure.
The arrangement for the furnishing of the implant does not
violate the federal anti-kickback statute.
All billing and claims submission for the implants does not
violate any federal or state law or regulation governing billing
or claims submission.
This exception does not apply to any financial relationships
between the referring physician and any entity other than the
ASC in which the implant is furnished to, and implanted in,
the patient.
Academic Medical Centers
Stark
Stark exception related to both ownership/investment and
compensation for services provided by an academic medical
center
Anti-Kickback
[No comparable safe harbor]
The referring physician a) is a bona fide employee of a
component of the academic medical center on a full-time or
substantial part-time basis. (A ``component'' of an academic
medical center means an affiliated medical school, faculty
practice plan, hospital, teaching facility, institution of higher
education, departmental professional corporation, or
nonprofit support organization whose primary purpose is
supporting the teaching mission of the academic medical
center. The components need not be separate legal entities);
b) is licensed to practice medicine in the State(s) in which he
or she practices medicine; c) has a bona fide faculty
appointment at the affiliated medical school or at one or more
of the educational programs at the accredited academic
hospital; and d) provides either substantial academic services
or substantial clinical teaching services (or a combination of
academic services and clinical teaching services) for which
the faculty member receives compensation as part of his or
her employment relationship with the academic medical
center. Parties should use a reasonable and consistent
method for calculating a physician's academic services and
clinical teaching services. A physician will be deemed to meet
this requirement if he or she spends at least 20 percent of his
or her professional time or 8 hours per week providing
academic services or clinical teaching services (or a
combination of academic services or clinical teaching
services). A physician who does not spend at least 20
percent of his or her professional time or 8 hours per week
providing academic services or clinical teaching services (or
a combination of academic services or clinical teaching
services) is not precluded from qualifying.
The total compensation paid by all academic medical center

components to the referring physician is set in advance and,
in the aggregate, does not exceed fair market value for the
services provided, and is not determined in a manner that
takes into account the volume or value of any referrals or
other business generated by the referring physician within the
academic medical center.
All transfers of money between components of the academic
medical center must directly or indirectly support the missions
of teaching, indigent care, research, or community service.
The relationship of the components of the academic medical
center must be set forth in written agreement(s) or other
written document(s) that have been adopted by the governing
body of each component. If the academic medical center is
one legal entity, this requirement will be satisfied if transfers
of funds between components of the academic medical
center are reflected in the routine financial reports covering
the components.
All money paid to a referring physician for research must be
used solely to support bona fide research or teaching and
must be consistent with the terms and conditions of the grant.
The referring physician's compensation arrangement does
not violate the anti-kickback statute, or any federal or state
law or regulation governing billing or claims submission.
The "academic medical center" consists of: a) an accredited
medical school (including a university, when appropriate) or
an accredited academic hospital (as defined at Sec.
411.355(e)(3)); b) 0ne or more faculty practice plans affiliated
with the medical school, the affiliated hospital(s), or the
accredited academic hospital; and c) one or more affiliated
hospital(s) in which a majority of the physicians on the
medical staff consists of physicians who are faculty members
and a majority of all hospital admissions are made by
physicians who are faculty members.

A faculty member is a physician who is either on the faculty
of the affiliated medical school or on the faculty of one or
more of the educational programs at the accredited academic
hospital. Faculty from any affiliated medical school or
accredited academic hospital education program may be
aggregated, and residents and non- physician professionals
need not be counted. Any faculty member may be counted,
including courtesy and volunteer faculty.
An accredited academic hospital means a hospital or a health
system that sponsors four or more approved medical
education programs.
Services Furnished by an Organization to Enrollees
Stark
Stark exception related to both ownership/investment and
compensation
Anti-Kickback
[No comparable safe harbor]
The services are furnished by an organization (or its
contractors or subcontractors) to enrollees of one of the
following prepaid health plans (not including services
provided to enrollees in any other plan or line of business
offered or administered by the same organization): a) an
HMO or a CMP in accordance with a contract with CMS,
which set forth qualifying conditions for Medicare contracts;
enrollment, entitlement, and disenrollment under Medicare
contracts; Medicare contract requirements; and change of
ownership and leasing of facilities: effect on Medicare
contracts; b) a health care prepayment plan in accordance
with an agreement with CMS; c) an organization that is
receiving payments on a prepaid basis for Medicare enrollees
through a demonstration project; d) a qualified HMO; e) a
coordinated care plan offered by an organization in
accordance with a contract with CMS; f) a managed care
organization (MCO) contracting with a State; g) a prepaid
inpatient health plan or prepaid ambulance health plan

contracting with a State; h) a health insuring organization
(HIO) contracting with a State; and i) an entity operating
under a demonstration project under sections 1115(a),
1915(a), 1915(b), or 1932(a) of the Act.
In-Office Ancillaries
Stark
Stark exception related to both ownership/investment and
compensation for in-house ancillary services
Anti-Kickback
[No comparable safe harbor]
NOTE: This exception has been modified by the Patient
Protection and Affordable Care Act. Review the changes.
Services are all designated health services and can include
certain items of durable medical equipment (DME), and
infusion pumps that are DME (including external ambulatory
infusion pumps), but excluding all other DME and parenteral
and enteral nutrients, equipment, and supplies (such as
infusion pumps used for PEN))
The services are furnished personally by one of the following
individuals: a) the referring physician.; b) a physician who is a
member of the same group practice as the referring
physician; or c) an individual who is supervised by the
referring physician or by another physician in the group
practice, provided the supervision complies with all other
applicable Medicare payment and coverage rules for the
services
They are furnished in one of the following locations:
The same building, but not necessarily in the
same space or part of the building, in which one of the
following conditions are satisfied:
a. The referring physician or his or her
group practice (if any) has an office that is
normally open to the physician's or group's
patients for medical services at least 35 hours per

week; and the referring physician or one or more
members of the referring physician's group
practice regularly practices medicine and
furnishes physician services to patients at least
30 hours per week. (The 30 hours must include
some physician services that are unrelated to the
furnishing of designated health services payable
by Medicare, any other federal health care payer,
or a private payer, even though the physician
services may lead to the ordering of designated
health services; or
b. the patient receiving the designated
health services usually receives physician
services from the referring physician or members
of the referring physician's group practice (if any)
and the referring physician or the referring
physician's group practice owns or rents an office
that is normally open to the physician's or group's
patients for medical services at least 8 hours per
week; and the referring physician regularly
practices medicine and furnishes physician
services to patients at least 6 hours per week.
(The 6 hours must include some physician
services that are unrelated to the furnishing of
designated health services payable by Medicare,
any other federal health care payer, or a private
payer, even though the physician services may
lead to the ordering of designated health services;
or
c. the referring physician is present
and orders the designated health services during
a patient visit on the premises or the referring
physician or a member of the referring physician's
group practice (if any) is present while the
designated health service is furnished during

occupancy of the premises; and the referring
physician or the referring physician's group
practice owns or rents an office that is normally
open to the physician's or group's patients for
medical services at least 8 hours per week; and
the referring physician or one or more members
of the referring physician's group practice
regularly practices medicine and furnishes
physician services to patients at least 6 hours per
week. The 6 hours must include some physician
services that are unrelated to the furnishing of
designated health services payable by Medicare,
any other federal health care payer, or a private
payer, even though the physician services may
lead to the ordering of designated health services.
A centralized building that is used by the group
practice for the provision of some or all of the group
practice's clinical laboratory services; or
A centralized building that is used by the group
practice for the provision of some or all of the group
practice's DHS (other than clinical laboratory services).
The services must be billed by one of the following: a) the
physician performing or supervising the service; b) the group
practice of which the performing or supervising physician is a
member under a billing number assigned to the group
practice; c) the group practice if the supervising physician is a
"physician in the group" under a billing number assigned to
the group practice; d) an entity that is wholly owned by the
performing or supervising physician or by that physician's
group practice under the entity's own billing number or under
a billing number assigned to the physician or group practice;
e) an independent third party billing company acting as an
agent of the physician, group practice, or entity under a billing
number assigned to the physician, group practice, or entity,

provided the billing arrangement meets the requirements of
Sec. 424.80(b)(6) of this chapter. A group practice may have,
and bill under, more than one Medicare billing number,
subject to any applicable Medicare program restrictions
DME covered by the in-office ancillary services exception
means canes, crutches, walkers and folding manual
wheelchairs, and blood glucose monitors, that meet the
following conditions:
The item is one that a patient requires for the
purposes of ambulating, uses in order to depart from
the physician's office, or is a blood glucose monitor
(including one starter set of test strips and lancets,
consisting of no more than 100 of each). A blood
glucose monitor may be furnished only by a physician
or employee of a physician or group practice that also
furnishes outpatient diabetes self- management training
to the patient.
The item is furnished in a building that meets the
"same building" requirements in the in-office ancillary
services exception as part of the treatment for the
specific condition for which the patient-physician
encounter occurred.
The item is furnished personally by the physician
who ordered the DME, by another physician in the
group practice, or by an employee of the physician or
the group practice.
A physician or group practice that furnishes the
DME meets all DME supplier standards located in Sec.
424.57(c) of this chapter.
The arrangement does not violate the anti-
kickback statute or any federal or state law or
regulation governing billing or claims submission.
All other requirements of the in-office ancillary

services exception are met.
In the case of a referring physician whose principal medical
practice consists of treating patients in their private homes,
the "same building" requirements are met if the referring
physician (or a qualified person accompanying the physician,
such as a nurse or technician) provides the designated health
services contemporaneously with a physician service that is
not a designated health service provided by the referring
physician to the patient in the patient's private home. A
private home does not include a nursing, long-term care, or
other facility or institution, except that a patient may have a
private home in an assisted living or independent living
facility.
Charitable Donations by a Physician
Stark
Stark exception related to compensation arrangements for
charitable donations
Anti-Kickback
[No comparable safe harbor]
The donations are bona fide charitable donations made by a
physician (or immediate family member) to an entity.
The charitable donation is made to an organization exempt
from taxation under the Internal Revenue Code (or to a
supporting organization).
The donation is neither solicited, nor offered, in any manner
that takes into account the volume or value of referrals or
other business generated between the physician and the
entity.
The donation arrangement does not violate the anti-kickback
statute or any federal or state law or regulation governing
billing or claims submission.
Professional Courtesy
Stark Anti-Kickback
Stark exception related to compensation arrangements for
professional courtesies
[No comparable safe harbor]
Professional courtesy that is offered by an entity with a formal
medical staff to a physician or a physician's immediate family
member or office staff.
The professional courtesy is offered to all physicians on the
entity's bona fide medical staff or in such entity's local
community or service area without regard to the volume or
value of referrals or other business generated between the
parties.
The health care items and services provided are of a type
routinely provided by the entity.
The entity has a professional courtesy policy that is set out in
writing and approved in advance by the entity's governing
body.
The professional courtesy is not offered to a physician (or
immediate family member) who is a Federal health care
program beneficiary, unless there has been a good faith
showing of financial need.
The arrangement does not violate the anti-kickback statute or
any federal or state law or regulation governing billing or
claims submission.
Community-Wide Health Information Systems
Stark
Stark exception related to compensation arrangements for
health information systems
Anti-Kickback
[No comparable safe harbor]
Items or services of information technology are provided by
an entity to a physician to allow access to, and sharing of,
electronic health care records and any complementary drug
information systems, general health information, medical
alerts, and related information for patients served by
community providers and practitioners, in order to enhance

the community's overall health.
The items or services are available as necessary to enable
the physician to participate in a community-wide health
information system, are principally used by the physician as
part of the community-wide health information system, and
are not provided to the physician in any manner that takes
into account the volume or value of referrals or other
business generated by the physician.
The community-wide health information systems are
available to all providers, practitioners, and residents of the
community who desire to participate.
The arrangement does not violate the anti-kickback statute or
any federal or state law or regulation governing billing or
claims submission.
Retention Payments in Underserved Areas
Stark
Stark exception related to compensation arrangements for
retention payments in underserved areas
Anti-Kickback
[No comparable safe harbor]
Remuneration is provided by a hospital directly to a physician
on the hospital's medical staff to retain the physician's
medical practice in the geographic area served by the
hospital.
The physician has a bona fide firm, written recruitment offer
or offer of employment from a hospital, academic medical
center or physician organization that is not related to the
hospital making the payment, and the offer specifies the
remuneration being offered and requires the physician to
move the location of his or her medical practice at least 25
miles and outside of the geographic area served by the
hospital making the retention payment.
In lieu of a bona fide written offer, the physician furnishes to
the hospital before the retention payment is made a written
certification that the physician has a bona fide opportunity for
future employment by a hospital, academic medical center or
physician organization that requires the physician to move
the location of his or her medical practice at least 25 miles
and outside the geographic area served by the hospital and
the certification contains at least the following-- (A) Details
regarding the steps taken by the physician to effectuate the
employment opportunity; (B) Details of the physician's
employment opportunity, including the identity and location of
the physician's future employer or employment location or
both, and the anticipated income and benefits (or a range for
income and benefits); (C) A certification that the future
employer is not related to the hospital making the payment;
(D) The date on which the physician anticipates relocating his
or medical practice outside of the geographic area served by
the hospital; and (E) Information sufficient for the hospital to
verify the information included in the written certification; and
the hospital takes reasonable steps to verify that the
physician has a bona fide opportunity for future employment
that requires the physician to relocate outside the geographic
area served by the hospital.
All requirements of the Stark exception for physician
recruitment are met.
Any retention payment is subject to the same obligations and
restrictions, if any, on repayment or forgiveness of
indebtedness as the written recruitment offer or offer of
employment. This requirement does not apply in the case of
a certification of employment.
In the case of a bona fide written offer, the retention payment
does not exceed the lower of-- (A) The amount obtained by
subtracting the physician's current income from physician and
related services from the income the physician would receive
from comparable physician and related services in the written
recruitment or employment offer, provided that the respective

incomes are determined using a reasonable and consistent
methodology, and that they are calculated uniformly over no
more than a 24-month period; or (B) The reasonable costs
the hospital would otherwise have to expend to recruit a new
physician to the geographic area served by the hospital to
join the medical staff of the hospital to replace the retained
physician.
In the case of a certification of employment, the retention
payment does not exceed the lower of-- (A) An amount equal
to 25 percent of the physician's current income (measured
over no more than a 24-month period), using a reasonable
and consistent methodology that is calculated uniformly; or
(B) The reasonable costs the hospital would otherwise have
to expend to recruit a new physician to the geographic area
served by the hospital to join the medical staff of the hospital
to replace the retained physician.
The physician's current medical practice is located in a rural
area or HPSA (regardless of the physician's specialty) or is
located in an area with demonstrated need for the physician
as determined by the Secretary of HHS in an advisory
opinion; or (B) At least 75 percent of the physician's patients
reside in a medically underserved area or are members of a
medically underserved population.
The hospital does not enter into a retention arrangement with
a particular referring physician more frequently than once
every 5 years.
The amount and terms of the retention payment are not
altered during the term of the arrangement in any manner
that takes into account the volume or value of referrals or
other business generated by the physician.
The arrangement does not violate the anti-kickback statute or
any federal or state law or regulation governing billing or
claims submission.

The above requirements apply to remuneration provided by a
federally qualified health center or a rural health clinic in the
same manner as it applies to remuneration provided by a
hospital.
Intra-Family Rural Referrals
Stark
Stark exception related to both ownership/investment and
compensation for intra-family referrals in rural areas
Anti-Kickback
[No comparable safe harbor]
Services are provided pursuant to a referral from a referring
physician to his or her immediate family member or to an
entity furnishing designated health services with which the
immediate family member has a financial relationship.
The patient who is referred resides in a rural area.
No other person or entity is available to furnish the services
in a timely manner in light of the patient's condition within 25
miles of the patient's residence; except in the case of
services furnished to patients where they reside (for example,
home health services or in-home DME), no other person or
entity is available to furnish the services in a timely manner in
light of the patient's condition.
The financial relationship does not violate the anti-kickback
statute or any federal or state law or regulation governing
billing or claims submission
The referring physician or the immediate family member must
make reasonable inquiries as to the availability of other
persons or entities to furnish the designated health services.
However, neither the referring physician nor the immediate
family member has any obligation to inquire as to the
availability of persons or entities located farther than 25 miles
from the patient's residence.
Unrelated Remuneration

Stark
Stark exception related to compensation arrangement for
unrelated remuneration
Anti-Kickback
[No comparable safe harbor]
Remuneration provided by a hospital to a physician that does
not relate, directly or indirectly, to the furnishing of designated
health services. Remuneration relates to the furnishing of
designated health services if it: a) is an item, service, or cost
that could be allocated in whole or in part to Medicare or
Medicaid under cost reporting principles; b)is furnished,
directly or indirectly, explicitly or implicitly, in a selective,
targeted, preferential, or conditioned manner to medical staff
or other persons in a position to make or influence referrals;
or c) otherwise takes into account the volume or value of
referrals or other business generated by the referring
physician.
The remuneration must be wholly unrelated to the furnishing
of DHS and must not in any way take into account the
volume or value of a physician's referrals.
Federally Qualified Health Centers
Stark
[No comparable exception]
Anti-Kickback
Safe harbor for payments and other transfers made to a
Federally Qualified Health Center
The transfer is made pursuant to a contract, lease, grant,
loan, or other agreement that-- (A) is set out in writing; (B) is
signed by the parties; and (C) covers, and specifies the
amount of, all goods, items, services, donations, or loans to
be provided by the individual or entity to the FQHC.
The amount of goods, items, services, donations, or loans
specified in the agreement may be a fixed sum, fixed
percentage, or set forth by a fixed methodology.
The amount may not be conditioned on the volume or value
of federal health care program business generated between
the parties.
The goods, items, services, donations, or loans are medical
or clinical in nature or relate directly to services provided by
the FQHC as part of the scope of the FQHC section 330
grant (including, by way of example, billing services,
administrative support services, technology support, and
enabling services, such as case management, transportation,
and translation services, that are within the scope of the
grant).
The FQHC reasonably expects the arrangement to contribute
meaningfully to the FQHC's ability to maintain or increase the
availability, or enhance the quality, of services provided to a
medically underserved population served by the FQHC, and
the FQHC documents the basis for the reasonable
expectation prior to entering the arrangement. The
documentation must be made available to the Secretary upon
request. At reasonable intervals, but at least annually, the
FQHC must re-evaluate the arrangement to ensure that the
arrangement is expected to continue to satisfy the standards,
and must document the re-evaluation contemporaneously.
The documentation must be made available to the Secretary
upon request. Arrangements must not be renewed or
renegotiated unless the FQHC reasonably expects the
standard to be satisfied in the next agreement term.
Renewed or renegotiated agreements must comply with the
requirements of this paragraph.
The individual or entity making the payment or transfer does
not (i) require the FQHC (or its affiliated health care
professionals) to refer patients to a particular individual or
entity, or (ii) restrict the FQHC (or its affiliated health care
professionals) from referring patients to any individual or
entity.
Individuals and entities that offer to furnish goods, items, or
services without charge or at a reduced charge to the FQHC

must furnish such goods, items, or services to all patients
from the FQHC who clinically qualify for the goods, items, or
services, regardless of the patient's payor status or ability to
pay. The individual or entity may impose reasonable limits on
the aggregate volume or value of the goods, items, or
services furnished under the arrangement with the FQHC,
provided such limits do not take into account a patient's payor
status or ability to pay.
The agreement must not restrict the FQHC's ability, if it
chooses, to enter into agreements with other providers or
suppliers of comparable goods, items, or services, or with
other lenders or donors. Where a FQHC has multiple
individuals or entities willing to offer comparable
remuneration, the FQHC must employ a reasonable
methodology to determine which individuals or entities to
select and must document its determination.
The FQHC must provide effective notification to patients of
their freedom to choose any willing provider or supplier. In
addition, the FQHC must disclose the existence and nature of
an agreement to any patient who inquires. The FQHC must
provide such notification or disclosure in a timely fashion and
in a manner reasonably calculated to be effective and
understood by the patient.
The FQHC may, at its option, elect to require that an
individual or entity charge a referred FQHC patient the same
rate it charges other similarly situated patients not referred by
the FQHC or that the individual or entity charge a referred
FQHC patient a reduced rate (where the discount applies to
the total charge and not just to the cost-sharing portion owed
by an insured patient).
Electronic Prescribing Items and Services
Stark
Stark exception related to compensation arrangements
Anti-Kickback
Safe harbor for payments made for electronic prescribing

items and services
The remuneration is nonmonetary and consists of items and
services in the form of hardware, software, or information
technology and training services necessary and used solely
to receive and transmit electronic prescription information.
The remuneration is nonmonetary and consists of items and
services in the form of hardware, software, or information
technology and training services necessary and used solely
to receive and transmit electronic prescription information.
The items and services are provided by a (i) a hospital to a
physician who is a member of its medical staff; (ii) a group
practice to a physician who is a member of the group; or (iii)
a PDP sponsor or MA organization to a prescribing physician.
The items and services are provided by a (i) hospital to a
physician who is a member of its medical staff; (ii) group
practice to a prescribing health care professional who is a
member of the group practice; and (iii) PDP sponsor or MA
organization to pharmacists and pharmacies participating in
the network of such sponsor or organization and to
prescribing health care professionals.
The items and services are provided as part of, or are used
to access, an electronic prescription drug program that meets
the applicable standards under Medicare Part D at the time
the items and services are provided.
The items and services are provided as part of, or are used
to access, an electronic prescription drug program that meets
the applicable standards under Medicare Part D at the time
the items and services are provided.
The donor (or any person on the donor's behalf) does not
take any action to limit or restrict the use or compatibility of
the items or services with other electronic prescribing or
electronic health records systems.
The donor (or any person on the donor's behalf) does not
take any action to limit or restrict the use or compatibility of
the items or services with other electronic prescribing or
electronic health records systems.
For items or services that are of the type that can be used for
any patient without regard to payor status, the donor does not
restrict, or take any action to limit, the physician's right or
ability to use the items or services for any patient.
For items or services that are of the type that can be used for
any patient without regard to payor status, the donor does not
restrict, or take any action to limit, the physician's right or
ability to use the items or services for any patient.
Neither the physician nor the physician's practice (including
employees and staff members) makes the receipt of the
items or services, or the amount or nature of the items or
services, a condition of doing business with the donor.
Neither the recipient nor the recipient's practice (or any
affiliated individual or entity) makes the receipt of items or
services, or the amount or nature of the items or services, a
condition of doing business with the donor.
Neither the eligibility of a physician for the items or services,
nor the amount or nature of the items or services, is
determined in a manner that takes into account the volume or
value of referrals or other business generated between the
parties.
Neither the eligibility of a physician for the items or services,
nor the amount or nature of the items or services, is
determined in a manner that takes into account the volume or
value of referrals or other business generated between the
parties.
The arrangement is set forth in a written agreement that (i) is
signed by the parties; (ii) specifies the items and services
being provided and the donor's cost of the items and
services; and (iii) covers all of the electronic prescribing items
and services to be provided by the donor. This requirement
will be met if all separate agreements between the donor and
the physician (and the donor and any family members of the
physician) incorporate each other by reference or if they
cross-reference a master list of agreements that is
maintained and updated centrally and is available for review
by the Secretary of HHS upon request. The master list should
be maintained in a manner that preserves the historical
record of agreements.
The arrangement is set forth in a written agreement that (i) is
signed by the parties; (ii) specifies the items and services
being provided and the donor's cost of the items and
services; and (iii) covers all of the electronic prescribing items
and services to be provided by the donor (or affiliated
parties). This requirement will be met if all separate
agreements between the donor (and affiliated parties) and
the recipient incorporate each other by reference or if they
cross-reference a master list of agreements that is
maintained and updated centrally and is available for review
by the Secretary of HHS upon request. The master list should
be maintained in a manner that preserves the historical
record of agreements.
The donor does not have actual knowledge of, and does not
act in reckless disregard or deliberate ignorance of, the fact
that the physician possesses or has obtained items or
services equivalent to those provided by the donor.
The donor does not have actual knowledge of, and does not
act in reckless disregard or deliberate ignorance of, the fact
that the recipient possesses or has obtained items or
services equivalent to those provided by the donor.
Electronic Health Records Items and Services
Stark
Stark exception related to compensation arrangements
Anti-Kickback
Safe harbor for payments made for electronic health records
The remuneration is nonmonetary and consists of items and
services in the form of software or information technology
and training services necessary and used predominantly to
create, maintain, transmit, or receive electronic health
records.
The remuneration is nonmonetary and consists of items and
services in the form of software or information technology
and training services necessary and used predominantly to
create, maintain, transmit, or receive electronic health
records.
The items and services are provided by an entity to a
physician.
The items and services are provided to an individual or entity
engaged in the delivery of health care by (i) an individual or
entity that provides services covered by a Federal health care
program and submits claims or requests for payment, either
directly or through reassignment, to the Federal health care
program; or (ii) a health plan.
The software is interoperable at the time it is provided to the
physician. Software is deemed to be interoperable if a
The software is interoperable at the time it is provided to the
recipient. Software is deemed to be interoperable if a

certifying body recognized by the Secretary of HHS has
certified the software no more than 12 months prior to the
date it is provided to the physician.
certifying body recognized by the Secretary of HHS has
certified the software within no more than 12 months prior to
the date it is provided to the recipient.
The donor (or any person on the donor's behalf)
does not take any action to limit or restrict the use,
compatibility or interoperability of the items or
services with other electronic prescribing or
electronic health records systems.
The donor (or any person on the donor's behalf)
does not take any action to limit or restrict the use,
compatibility or interoperability of the items or
services with other electronic prescribing or
electronic health records systems.
Before receipt of the items and services, the
physician pays 15 percent of the donor's cost for the
items and services. The donor (or any party related
to the donor) does not finance the physician's
payment or loan funds to be used by the physician
to pay for the items and services.
Before receipt of the items and services, the
recipient pays 15 percent of the donor's cost for the
items and services. The donor (or any affiliated
individual or entity) does not finance the recipient's
payment or loan funds to be used by the recipient to
pay for the items and services.
Neither the physician nor the physician's practice
(including employees and staff members) makes the
receipt of items or services, or the amount or nature
of the items or services, a condition of doing
business with the donor.
Neither the recipient nor the recipient's practice (or
any affiliated individual or entity) makes the receipt
of items or services, or the amount or nature of the
items or services, a condition of doing business with
the donor.
Neither the eligibility of a physician for the items or services,
nor the amount or nature of the items or services, is
determined in a manner that directly takes into account the
volume or value of referrals or other business generated
between the parties. For purposes of this paragraph, the
determination is deemed not to directly take into account the
volume or value of referrals or other business generated
between the parties if any one of the following conditions is
met: (i) the determination is based on the total number of
prescriptions written by the physician (but not the volume or
value of prescriptions dispensed or paid by the donor or billed
to the program); (ii) the determination is based on the size of
the physician's medical practice (for example, total patients,
total patient encounters, or total relative value units); (iii) the
determination is based on the total number of hours that the
Neither the eligibility of a recipient for the items or services,
nor the amount or nature of the items or services, is
determined in a manner that directly takes into account the
volume or value of referrals or other business generated
between the parties. For the purposes of this paragraph, the
determination is deemed not to directly take into account the
volume or value of referrals or other business generated
between the parties if any one of the following conditions is
met: (i) the determination is based on the total number of
prescriptions written by the recipient (but not the volume or
value of prescriptions dispensed or paid by the donor or billed
to a Federal health care program); (ii) the determination is
based on the size of the recipient's medical practice (for
example, total patients, total patient encounters, or total
relative value units); (iii) the determination is based on the

physician practices medicine; (iv) the determination is based
on the physician's overall use of automated technology in his
or her medical practice (without specific reference to the use
of technology in connection with referrals made to the donor);
(v) the determination is based on whether the physician is a
member of the donor's medical staff, if the donor has a formal
medical staff; (vi) the determination is based on the level of
uncompensated care provided by the physician; or (vii) the
determination is made in any reasonable and verifiable
manner that does not directly take into account the volume or
value of referrals or other business generated between the
parties.
total number of hours that the recipient practices medicine;
(iv) the determination is based on the recipient's overall use
of automated technology in his or her medical practice
(without specific reference to the use of technology in
connection with referrals made to the donor); (v) the
determination is based on whether the recipient is a member
of the donor's medical staff, if the donor has a formal medical
staff; (vi) the determination is based on the level of
uncompensated care provided by the recipient; or (vii) the
determination is made in any reasonable and verifiable
manner that does not directly take into account the volume or
value of referrals or other business generated between the
parties.
The arrangement is set forth in a written agreement that (i) is
signed by the parties; (ii) specifies the items and services
being provided, the donor's cost of the items and services,
and the amount of the physician's contribution; and (iii)
covers all of the electronic health records items and services
to be provided by the donor. This requirement will be met if
all separate agreements between the donor and the
physician (and the donor and any family members of the
physician) incorporate each other by reference or if they
cross-reference a master list of agreements that is
maintained and updated centrally and is available for review
by the Secretary of HHS upon request. The master list should
be maintained in a manner that preserves the historical
record of agreements.
The arrangement is set forth in a written agreement that (i) is
signed by the parties; (ii) specifies the items and services
being provided, the donor's cost of those items and services,
and the amount of the recipient's contribution; and (iii) covers
all of the electronic health records items and services to be
provided by the donor (or any affiliate). This requirement will
be met if all separate agreements between the donor (and
affiliated parties) and the recipient incorporate each other by
reference or if they cross-reference a master list of
agreements that is maintained and updated centrally and is
available for review by the Secretary of HHS upon request.
The master list should be maintained in a manner that
preserves the historical record of agreements.
The donor does not have actual knowledge of, and does not
act in reckless disregard or deliberate ignorance of, the fact
that the physician possesses or has obtained items or
services equivalent to those provided by the donor.
The donor does not have actual knowledge of, and does not
act in reckless disregard or deliberate ignorance of, the fact
that the recipient possesses or has obtained items or
services equivalent to those provided by the donor.
For items or services that are of the type that can be used for
any patient without regard to payor status, the donor does not
restrict, or take any action to limit, the physician's right or
For items or services that are of the type that can be used for
any patient without regard to payor status, the donor does not
restrict, or take any action to limit, the recipient's right or

ability to use the items or services for any patient. ability to use the items or services for any patient.
The items and services do not include staffing of physician
offices and are not used primarily to conduct personal
business or business unrelated to the physician's medical
practice.
The items and services do not include staffing of the
recipient's office and are not used primarily to conduct
personal business or business unrelated to the recipient's
clinical practice or clinical operations.
The electronic health records software contains electronic
prescribing capability, either through an electronic prescribing
component or the ability to interface with the physician's
existing electronic prescribing system that meets the
applicable standards under Medicare Part D at the time the
items and services are provided.
The electronic health records software contains electronic
prescribing capability, either through an electronic prescribing
component or the ability to interface with the recipient's
existing electronic prescribing system, that meets the
applicable standards under Medicare Part D at the time the
items and services are provided.
The arrangement does not violate the anti-kickback statute or
any Federal or State law or regulation governing billing or
claims submission.
The donor does not shift the costs of the items or services to
any Federal health care program.
The transfer of the items or services occurs and all conditions
are satisfied on or before December 31, 2013.
The transfer of the items and services occurs, and all
conditions have been satisfied, on or before December 31,
2013.
![FY 2020 Inpatient Rehabilitation Facility PPS Final Rule ... · Medicare Inpatient Rehabilitation Facility Prospective Payment System for FY 2020 [CMS-1710-F] Summary of Final Rule](https://img.pdfslide.net/doc/110x75/5e152d886e3b54465b2e79a7/fy-2020-inpatient-rehabilitation-facility-pps-final-rule-medicare-inpatient.jpg)




























