Embed Size (px)
Citation preview
STATE OFNEW YORK - WORKERS' COMPENSATION BOARD
INDEPENDENT EXAMINER'S REPORT OF INDEPENDENT MEDICAL EXAMINATIONA copy of each report of Independent Medical Examination shall be submitted on the same dav and In the same manner ir> .
e'<amlne'r,CHECK ONE: PHYSICIAN PODIATRIST ICHIROPRACTOR Ij |PSYCHOLOGIST"]
THIS EXAMINATION WAS REQUESTED BY; | pCcARRlER.'EMPLOYERCLAIMANT
V/CB CASE NO. CARRIER CASE NO, (IFKNOWN) DATE OF IN.)1JRY INJURED PERSON'SDATE OF EXAMINATION
lovastoS 1!pW00292 02/25/IB 04/i4/ib •INJURED
PERSON
IMHJCB intual) JLaslName)
JAMES KEATING
ADDRESS(IncludeApLNO,) P.O. BOX 34
REMSEHBUR6. NV 11960
Efi^PLOYER
SCPD
INSURANCE
CARRIERSUFFOLK COUNTY RISK MGMT
>.0. BOX 6100
HAUPPAOGE, NY 11783-
WoS^S-bVwIi'ETsATiON BOARD RE^T^lloNNUMBER OM 0" ARRANGEMSNl Wl 1H AN IME COMPANY, STATE NAmTaHoMedical Management Group of NY, Inc. 010029
Results ofExamination (continue on reverse orattach additional sheets, If necessary}
Attached please find my report regarding theabove referenced injured person,
RE
i nU-A-»
Copies of this report have been furnished to the followingparties as required under the workers' compensation law;
KEATING, JAMESMCINTYRE DONOHUE ACCARDI
WORKERS COMPENSATION BOARD
SUFFOLK COUNTY RISK MGMT
CHERRY, EDSON & KELLYDR. JONATHAN RAANAN
Ihereby certify that this report Is afull and truthful representation of ect to the claimant's condition' that noperson or entity has caused, directed or encouragedme tq subnyit areviewed the report and attest to its accuracy.
differs substantially f m my professional opinion; and I have
SHEBAIRO, RAYMOND, MD
Independent Examiner's Name Exam Dale
independent Examiner's Address IME Authorization No.NO INDEPENDENT EXAMINER EXAMINING OR EVALUATING A CLAIMANT UNDER THE WORKERS' COMPENSATION IAW KiriR amv c:i iocp\>igiM>-l
IME-4(7-14)
NYS Workers'Compensation Board, Centralized Mailing, PQ Box 5205, Binghamton, NY 13902-5205
State of New YorkWORKERS' COMPENSATION BOARD
INDEPENDENT EXAMINER'S REPORT OF REQUEST FOR INFORMATION/RESPONSE
1. INDEPENDENT EXAMINER'S NAMEAND ADDRESS
SHEBAIRO, RAYMOND, MD •OF LONG ISLAND, PC86-11 LEFFERTS BLVD LL LEVELp T PtJA/inMr> tj T T T _• n .11 o
2. NAME AND ADDRESS OF PARTY REQUESTING INFORMATION
SUFFOLK COUNTY RISK MGMTP.O. BOX 6100
HAUPPAUGE, NY 11788-
3. INDtPtMJENTEXTXMINER^TMt AoTRORIZATtONTlO.
122681-OB 1
4. IMEENTITY REGISTRATION NO. (If AppficaWs)
>10029
5. DATE OF INDEPENDENT MEDICAL EXAMINATION
04/14/166. CLAIMANTS NAME
KEATING, JAMES
7. CLAIMANTS WCB CASE NO.
31078858
8. DATE OF iNJUR\L
02/25/15 19. DATE OF THIS REPORT
independent medical examination of a workers' compensation claimant receives a request for information regarding the claimant, Including faxedor elecfronicaliy-transrnitted requests, the Independent examiner must submit a copy of the request for information to the Workers'Compensation Board within ten days of the receipt of the request, in addition, copies of all responses to such requests, shall be submitted by theresponding Independent examiner tothe Board within ten days ofthesubmission oftheresponse totherequester.
PLEASE NOTE: Do not use this form tofile documents, records, reports oritems that are part of the official Board file. Any such itemsthat are not part of the Board file atthe time the IME is scheduled, should be submitted lo the Board atthe time of scheduling. The iME-3 shouldnot be used for such submissions.
ifthe requestfor information Is limited to a request for scheduling ofan independent medical examination, you neednotfile thisform.However, you must send a copy of Form IME-5 {"Claimant's Notice of Independent Medical Examination") to the Workers'Compensation Board.
Instructions:
Complete all identifying information, items 1-9 above.To report a request for information, complete ilem 10-A below, sign, date and mail to the Workers' Compensation Board within ten days ofreceiptof request. Acopyof the request must be attached.To report independent examiner's response to a request for Information, complete Item 10-B below, sign, date and mail lo the Workers'Compensation Board within tendays ofsubmission ofresponse totherequester. Acopy ofthe response must beattached.If the independent examiner responds to the requester within ten days ofthe receipt of the request, complete, sign and date items 10-A and10-B and mail to the Workers' Compensation Board within ten days of receipt of the request, with copies of the request and responseattached. Otherwise, submit separate forms toreport request andyour response within the lime limits given in b.andc. above,NOTE: The independent examiner's release of medical and/or workers' compensation records to,the Board and/or to the requesting party issubject to applicable laws regarding the confidentiality of such records, including but ^t; limited to Section 110-a of the Workers'Compensation Law, Section 18 of the Public Health Law, and other applicable state and feder^lpws.
HIPAA Notice: In order to adjudicate a workers' compensation claim, WCL Sections 13-a and 137 permit an employer orcarrier to have aclaimant examined by a health care provider. Pursuant to 45 CFR 512 a health care provider who has been retained by an employer orcarrierto evaluate a workplaceInjury Is exempt from HIPAA's restrictions on disclosure of health information.
INDEPENDENT EXAMINERS WHO FAIL TO FILE REQUIRED FORMS MAY BE SUBJECT TO DISCIPLINE,INCLUDING REMOVAL OFAUTHORIZATION TOPERFORM INDEPENDENT MEDICAL EXAMINATIONS.
10-A. INDEPENDENT EXAMINER'S REPORT OF REQUEST FOR INFORMATION REGARDING INDEPENDENT MEDICAL EXAMINATION
Daterequest receivedAlta^d is a copy ofa request for information received
Independent Examiner's Name
10-B. INDEPENDENT EXAMINER'S REPORT OFRESPONSE t6 REQUEXAMINATION '
Date response submittedto requesterAttached is a copy of my response to a request fto thej;equester which are not already part of
Independent Examiner's Name
IME-3 (7-14)
Date
JDING INDEPENDENT MEDICAL
Ir^teiyed In^e case IdentifijEi'd above, and all materials suppliedbase record/.. ,
Date
www.wcb.ny.gov
04/14/2016
Raymond A. Shebairo^ M.D.Diplomate American Board of Orthopedic Surgery
10 55 Portion Road. Suite IIWFarmingviiie, NY 11738
Medical Management Group, Inc. of New York1 Corporate Drive, Suite 104Bohemia, NY 11716
Claimant: Keating, James J.Claim #: 15W00292WCB#: G1078858
MMG#: P124944-O-02Emp. Name: SCPDDOA: 02/25/2015
To Whom It May Concern:
As you requested, I have performed an orthopedic independent medicalevaluation regarding the above-named claimant, Mr. James J. Keating, on04/14/2016 In the Suffolk office. His New York State commercial driverlicense was presented prior to this examination. David, a female chaperone,was present at the time of this examination. My findings are as follows:
ACCIDENT AND TREATMENT HISTORY:
The history was obtained from Mr. Keating who reports that he was involvedin a work-related accident on 02/25/2015. The claimant explains that he fellin parking lot and injured his neck, bilateral shoulder, left wrist, and left hip.
Mr. Keating reports that he went to the Emergency Room of Peconic BayMedical Center the next day for an evaluation and treatment. He states thatX-rays of his left shoulder, left wrist, pelvis and left hip was performed. Hestates that he was released that same day from the.Emergency Room withprescriptions for Ibuprofen, Tramadol, Cyclpbenzaprine, Zaieplon,Oxycodone, and Ambien.
Subsequently, Mr. Keating states that he came under the care of variousphysicians. As per the review of medical records, he was then started on acourse of physical therapy. He states that diagnostic tests consisting of MRIsof his neck, right shoulder, and left wrist were pditfbrmed. He states that herequired the use of rubber bands and TENS machine. He reports undergoingleft shoulder surgery on 06/29/2015. He states i-hat he is receiving triggerpoint injections.
>^iaMiiaiiL. i\caLiii97~Jciineb~j;
Claim #: 15W00292MMG#: P124944-O-02
Emp. Name: SCPDDOA: 02/25/2015
iMt KeportPage 2
MEDICAL HISTORY:
Mr. Keating reports history of prior motor vehicle accident in 2012; howeverhe has not provided any information regarding injuries. He reports a historyof prior Worker's Compensation accident, however he did not elaboratefurther. He does not disclose any information regarding diabetes andhypertension.
SURGICAL HISTORY!
Mr. Keating reports undergoing prior gailbiadder removal in 2010.
MEDICATIONS:
Mr. Keating reports that currently he is taking Ibuprofen, Tramadoi,Cyciobenzaprine, and Zaleplon.
ALLERGIES:
Mr. Keating does not disclose any information regarding allergies.
EMPLOYMENT HISTORY:
Mr. Keating states that he was employed as a detective at the time of theaccident. He states that currently he is not working.
PRESENT COMPLAINTS!
At the time of this examination, Mr. Keating states that he has complaints ofpain in the neck, bilateral shoulder, left elbow, bilateral wrist, and left hip.He states that his left shoulder is partially frozen.
REVIEW OF AVAILABLE RECORDS:
1. The following medical records were available at the time of theexamination for my review:
2. C-4.2 forms.
3. Foiiow-up visit report, from New York Sports medicine Institute., dated07/07/2015 through 02/23/2016.
4. Physical therapy progress notes, from Ail Star Physical Therapy., dated06/12/2015 through 08/12/2015.
5. SOAP notes dated 03/13/2015 through 07/30/2015 by Peter M Piscina,PT.
6. OT/PT-4 forms.7. Operative report, dated 06/29/2015, operation: "Left shoulder
arthroscopic subacromial decompression. Left shoulder arthroscopic
uaimant: : Keating, James J.Claim #: 15W00292MMG#: P124944-O-02Emp. Name: SCPDDOA: 02/25/2015
IME ReportPage 3
lysis of adhesions. Left shoulder arthroscoplc distal clavicle resection(AC joint resection). Left shoulder arthroscoplc debrldement,extensive. Left shoulder manipulation under anesthesia", performed byNell Roth, M.D., assisted by Dr. Tammy Hamzavl, preoperatlvediagnosis: Left shoulder adhesive capsulltis secondary to superiorlabral tear. Left shoulder Impingement syndrome. Left shouldersubacromlal bursltls. Left shoulder AC joint arthrosls., postoperativediagnosis: Left shoulder adheislve capsulltis secondary to superiorlabral tear. Left shoulder Impingement syndrome. Left shouldersubacromlal bursltls. Left shoulder AC joint arthrosls.
8. SOAP notes dated 04/15/2015 and 06/22/2015 by Kerry Murphy, M.D.9. Examination report dated 05/26/2015 by Nell Roth, M.D.10.EC-4NARR forms.
11.Office visit report, from Orthopedic Associates of Long Island, LLP.,dated 03/02/2015 through 04/06/2015.
12.MRI report of the cervical spine, by Brett Helfner, M.D., dated04/03/2015, Impression: Broad-based disc hernlatlon at C4-5 mildlyflattens the cord without high-grade cord compression or cord signalabnormality. Multilevel foramlnal stenosis, severe at C4-C5 withcompression of the exiting C5 nerve roots.
13.Invoice dated 12/09/2014.14.MRI 3T report of the left shoulder, by Brett Helfner, M.D., dated
03/03/2015, Impression: Attenuated and scarred anterolnferlorlabrum suggesting chronic Injury. Blunting and fraying of thesuperlor/posterosuperlor labrum with 3 mm paralabral cyst at the10:00 position. Moderate subscapularls tendlnosis without rotator cufftear.
15.MRI 37 report of the left wrist , by Brett Helfner, M.D., dated03/03/2015, Impression: Large full-thickness central TFC tear, chronicIn appearance. No acute fracture or tendon tear. Intact scapholunateand lunotrlquetral ligaments.
16.MRI 37 report of the right shoulder, by Brett Helfner, M.D., dated03/03/2015, Impression: Mild suprasplnatus tendlnosis with smallpartial-thickness Interstitial tear at the Insertion. No high-grade partialor full-thickness rotator cuff tear. Minimal fraying of theposterosuperlor labrum. Benlgn-appearing chondrold lesion In theproximal humeral shaft spanning 5.6 cm In cc dimension, likely achondroma. Consider comparison with any outside prior studies versussurveillance Imaging In 6 months to ensure stability.
17.Emergency department medical record, from Peconic Bay MedicalCenter., dated 02/26/2015.
IS.X-ray report of the left wrist, from Peconic Bay Medical Center., dated02/26/2015, Impression: no acute fracture or dislocation of right onleft wrist.
19.X-ray report of the pelvis and left hip, from Peconic Bay MedicalCenter., dated 02/26/2015, Impression: no acute fracture or pelvis orleft hip.
Claimant: Keating, James J.Claim #: 15W00292MMG#: P124944-O-02Emp. Name: SCPDDOA: 02/25/2015
20.X-ray report of the left shoulder, from Peconic Bay Medical Centerdated 02/26/2015
21.C-3 form.
22.First report of Injury report type (MTC) OO-Orlginal dated 04/21/2015.23.Subsequent report of Injury report type (MTC) EP-Employer paid dated
05/15/2015.24.MG-2 forms dated 07/28/2015 through 02/25/2016 by Nell Roth.25.MG-2 forms dated 03/16/2016 by Jonathan Raanan, M.D.26.Progress notes dated 03/08/2016 by Jonathan Raanan, M.D.27.Fax dated 03/16/2016.28.C-8.1 form.
29.Health Insurance Claim forms.
PHYSICAL EXAMINATION!
Examination reveals a 53-year-old right-handed male. He is 6 feet 2 inchestall, weighs 210 pounds, and he has bionde/grey hair with blue eyes. Heappears in no acute distress and is able to understand and cooperate duringthe examination.
ORTHOPEDIC EXAMINATION;
Cervical Spine: There is no muscle spasm upon palpation. There is nocomplaint of tenderness upon palpation. Range of motion is flexion at 50degrees (50 degrees normal), extension at 55 degrees (60 degrees normal),right lateral flexion at 40 degrees (45 degrees normal) and left lateral flexionat 40 degrees (45 degrees normal), and right rotation at 75 degrees (80degrees normal) and left rotation at 80 degrees (80 degrees normal).
Neurological examination of the bilateral upper extremities shows as foilows:There is no atrophy. Muscle strength in each range is at 5/5. Deep tendonreflexes, biceps and triceps, are at 2+.
Right Shoulder: There is no heat, swelling, effusion, erythema, or crepitusappreciated. Range of motion is forward flexion at 170 degrees (170-180degrees normal), extension at 20 degrees (40 degrees normal), abduction at120 degrees (170-180 degrees normai), adduction at 30 degrees (45degrees normal), internal rotation at 90 degrees (80-90 degrees normal),and external rotation at 90 degrees (80-90 degrees normal).
The following orthopedic test is performed:
• Impingement - negative.
Left Shoulder: There is an arthroscopic scar noted. There is no heat,swelling, effusion, erythema, or crepitus appreciated. Range of motion isforward flexion at 90 degrees (170-180 degrees normal), extension at 20
Claimant:" Keating, James J. i- IME ReportPage 5Claim #: 15W00292
MMG#: P124944-0-02Emp. Name: SCPD
DOA: 02/25/2015
degrees (40 degrees normal), abduction at 70 degrees (170-180 degreesnormal), adduction at 10 degrees (45 degrees normal), internal rotation at80 degrees (80-90 degrees normal), and external rotation at 40 degrees (80-90 degrees normal).
• Impingement - not performed.
Tenodesis surgery and arthroscopic surgery were performed.
Right Elbow: Range of motion is flexion at 125 degrees (135-145 degreesnormai), pronation 80 degrees (80-90 degrees normal), supination 80degrees (80-90 degrees normal) and extension at 0 degrees (0 degreesnormal).
Left Elbow: There is no heat, sweiling, effusion, erythema, or crepitusappreciated. Range of motion is flexion at 105 degrees (135-145 degreesnormal), pronation 80 degrees (80-90 degrees normai), supination 80degrees (80-90 degrees normai) and extension at 20 degrees (0 degreesnormal).
The following orthopedic tests are performed:
• Tinel's - negative.Apiey's - negative.
Right Wrist/Hand: There is no heat, sweiling, effusion, erythema, orcrepitus appreciated. Range of motion reveals palmar flexion to 60 degrees(80-90 degrees normal), dorsiflexion to 60 degrees (70-85 degrees normal),pronation to 80 degrees (80-90 degrees normal) and supination to 80degrees (80-90 degrees normal), radial-lateral motion to 20 degrees (20degrees normal), and ulnar motion to 30 degrees (30 degrees normal).
• Tinel's - negative.• Phalen's - negative.
Left Wrist/Hand: There is no heat, swelling, effusion, erythema, orcrepitus appreciated. Range of motion reveals palmar flexion to 60 degrees(80-90 degrees normal), dorsiflexion to 60 degrees (70-85 degrees normal),pronation to 80 degrees (80-90 degrees normai) and supination to 80degrees (80-90 degrees normal), radial-lateral motion to 20 degrees (20degrees normal), and ulnar motion to 30 degrees (30 degrees normal).
• Tinel's - negative.• Phaien's - negative.
The claimant reports numbness in the ieft ring and middle fingers.
Claimant: - '^ Keating, James J. — IME ReportClaim #: 15W00292 Page 6MMG#: P124944-O-02
Emp. Name: SCPD
DOA: 02/25/2015
Right Hip: There is no heat, swelling, or redness appreciated. There Is nocomplaint of tenderness upon palpation. Range of motion Is forward flexionat 90 degrees (120 degrees normal), extension at 25 degrees (25-30degrees normal), abduction at 45 degrees (45 degrees normal), adduction at40 degrees (35 degrees normal), external rotation at 70 degrees (50 degreesnormal), and Internal rotation at 10 degrees (40 degrees normal).
Left Hip: There Is no heat, swelling, or redness appreciated. Range ofmotion Is forward flexion at 90 degrees (120 degrees normal), extension at25 degrees (25-30 degrees normal), abduction at 45 degrees (45 degreesnormal), adduction at 30 degrees (35 degrees normal), external rotation at70 degrees (50 degrees normal), and Internal rotation at 10 degrees (40degrees normal).
DIAGNOSES;
1. Cervical spine spraln/strain - resolving.2. Right shoulder spraln/strain - resolved.3. Status post left shoulder surgery on 06/29/2015.
vx4. Left elbow spraln/strain - resolving.5. Bilateral wrist spraln/strain - resolved.6. Left hip spraln/strain - resolved.
DISABILITY:
There Is evidence of a moderate partial disability.
TREATMENT;
Based on my physical examination, Mr. Keatlng's condition warrants furthertreatment and has not reached maximum medical Improvement in myspecialty. Orthopedics. Therefore,.! recommend further treatment Includingphysical therapy administered for the.duration of six weeks at the rate of twotimes per week with a re-evaluatlon upon completion that would bereasonable, related, and necessary at this time.
Upon completion of the examination, Mr. Keating offers no complaints as aresult of this examination and left the examining area stable and unchanged.
ATTESTATION:
I, Raymond A. Shebairo, M.D., being an orthopedic surgeon, duly licensed topractice medicine In the State of NY, pursuant to the applicable provisions ofthe Civil Practice Law and Rules section 2106, hereby affirm that Mr. Keatingwas examined according to the restricted rules concerning an Independentmedical examination. It Is, therefore, understood that no doctor/patientrelationships exists or is Implied by this examination. Mr. Keating was
Glalmaht:Claim #;MMG#:
Emp. Name:DOA:
Keating, James J.15W00292
P124944-O-02SCPD
02/25/2015
IME ReportPage 7
examined with reference to the specific complaint emanating from theoriginal injury. Any other medical conditions, which were either unreportedor felt to be unrelated to the original injury, are considered to be beyond thisexamination.
This report is a full and truthful representation of the independent medicalexaminer's professional opinion with respect to the claimant's condition inaccordance with Workers' Compensation Law Sections 13-a (4)(e)(i), 13-k(3)(e)(i), 13-1 (3)(e)(l) or 13-m (4)(e)(i). No person or entity has caused,directed or encouraged me to submit a report that differs substantially frommy professional opinion. I have reviewed the report and attest to itsaccuracy.
Sincerely,
Raymond A. Shebairo, M.D.WCB License No: 122681-OB
RAS/OKS/MO/st
AVAILABILITY TO TESTIFY:
I will be available to testify by appointment only with four weeks advancednotice.
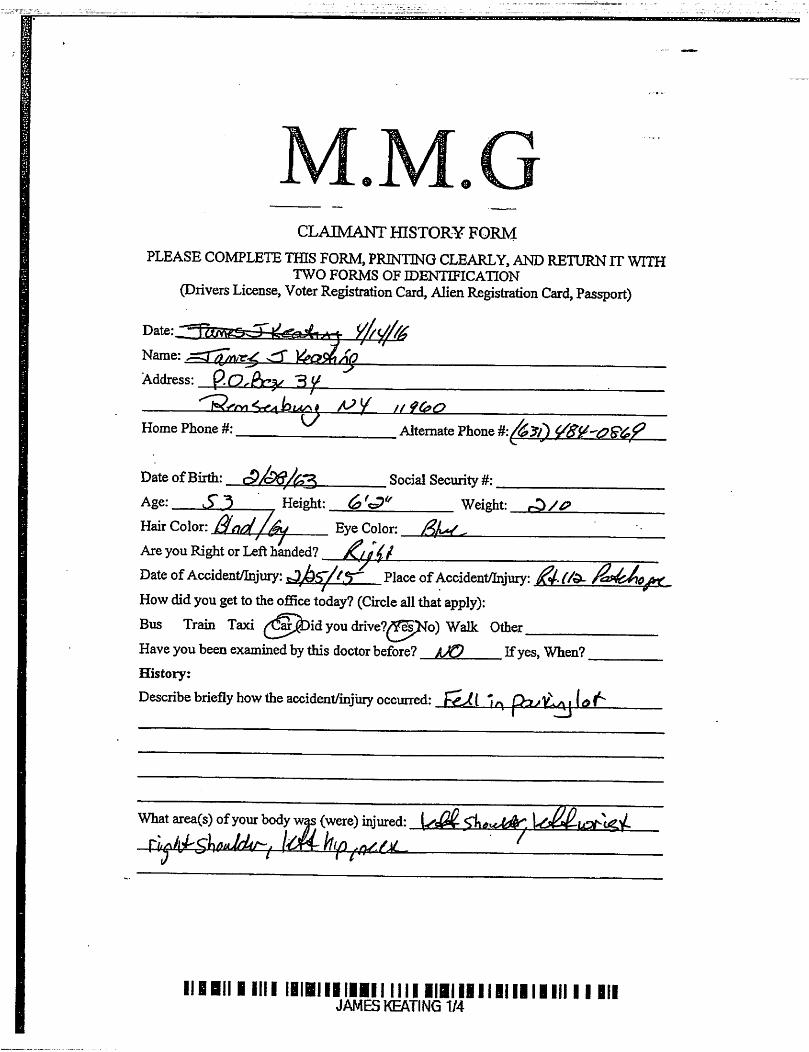
CLAIMANT HISTORY FORM
PLEASE COMPLETE THIS FORM, PRINTING CLEARLY, AND RETURN IT WITHTWO FORMS OF IDENTXFICATION
(Drivers License, Voter Registration Card, Alien Registration Card, Passport)
Name: sTT Vffi^AoAddress:
Home Phone #: Alternate Phone
Date ofBirth: Social Security #:Age: Height: Weight:Hair Color: Sn/J //^ Eve Color: f,L/. ^Are you Right or Left handed? _
Date ofAccident/Injury: Place ofAccident/Injury:
How didyougetto theoffice today? (Circle allthatapply):
Bus Train Taxi you drive?^^pNo) Walk OtherHave you been examined by this doctor before? kJQ Ifyes. When?History:
Describebrieflyhowthe accident/injiiiy occurred:
What area(s) ofyour body was (were) injured:
IIBBIII ill! IBIBIIIIIIII nil IIBiililliilllill 11 IIIJAMES KEATING 1/4
iM'i
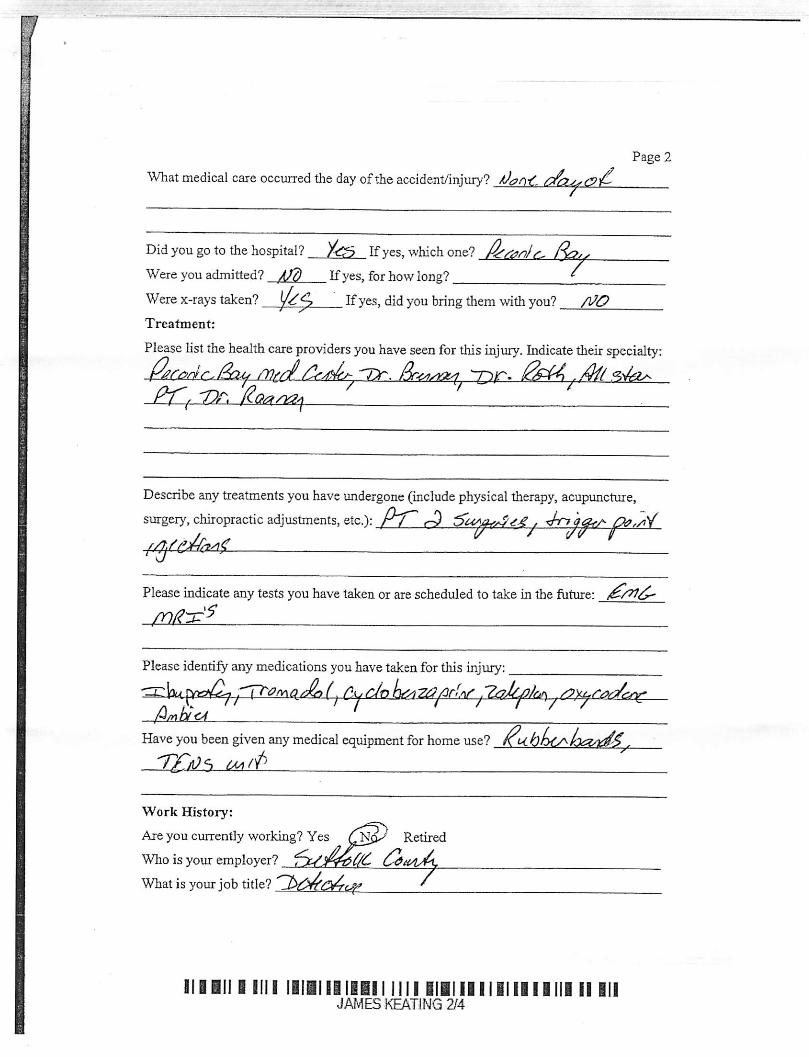
What medical care occurred the day oftheaccident/injury? /Jj?/
Did you go to the hospital? Ay? Ifyes, which one?
Were you admitted? A/d Ifyes, for how long? ^Were x-rays taken? If yes, didyoubringthemwithyou? /}/0
Treatment:
Page 2
Please listthe health care providers you have seen forthis injury. Indicate their specialty:
Please indicate any tests you have taken or are scheduled to take in the future:
wss^
Have you been given any medical equipment for home use?
— • it-
Work History:
Are you currently working? Yes Retired
Who is your employer?
What is your job title? '
ill III 1 nil liiiiiiiiEii nil iliiiiiiiiiiiiiii 11 IIIJAMES KEATING 2/4
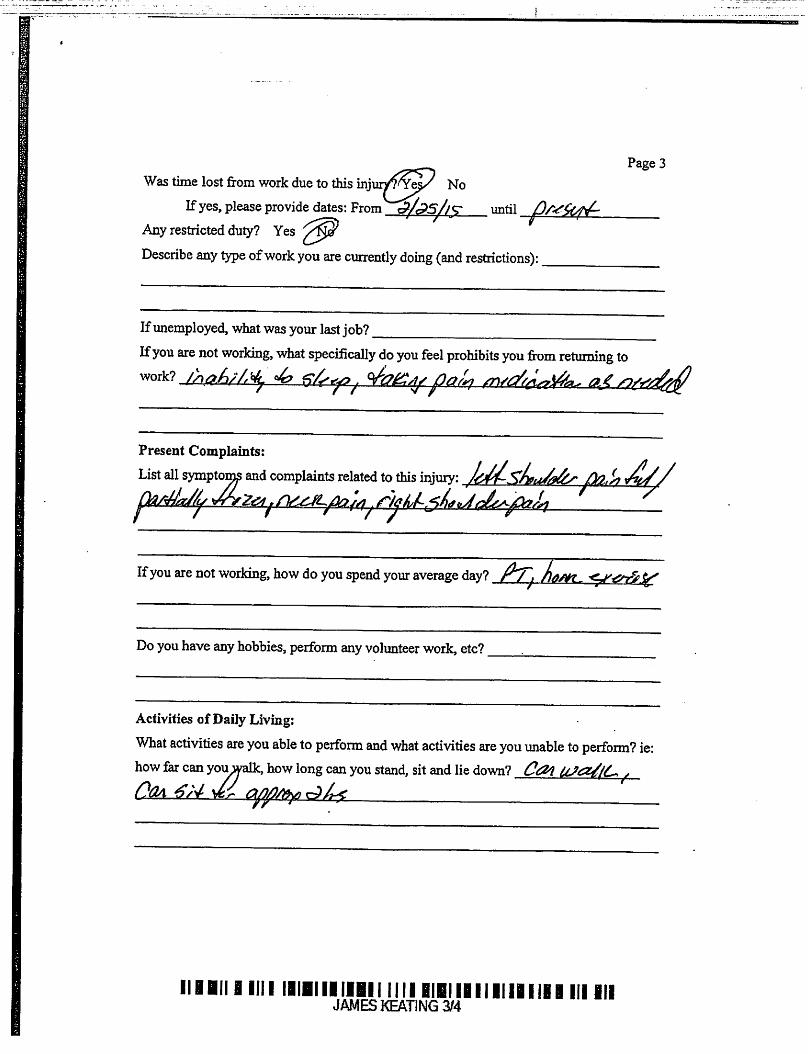
Page 3Was time lost from work due to this mjiiiVTYe^ No
Ifyes, please provide dates: From cP/^5//<r untilAny restricted duty? Yes
Describe any type ofwork you are currently doing (and restrictions):
If unemployed, whatwasyourlastjob?
Ifyou are not working, what specifically do you feel prohibits you from returning to
Present Complaints:
Ifyou are notworking, how doyou spend your average day?
Doyouhave anyhobbies, perform anyvolunteer work,etc?
Activities of Daily Living:
What activities are you able to perform and what activities are you unable to perform? ie:how far can yoi^alk, how long can you stand, sit and lie down? COl. .
llllll Bnil IIIHIiiiiBil iili BIBIiiililililil III illJAMES KEATING 3/4
Page 4What daily activities are you capable/incapable ofperfonning? ie: cooking, cleaning,tending to personal hygiene, taking care ofchildren, shopping for groceries, runningmiscellaneous errands: ^ /nA'
WA
Medical Management Groupof New York, Inc.
1 Corporate DriveSuite 104
Bohemia, NY 11716
www.medicalmanagementime.com
NY 631.467.7766NJ 732.885.5850
Fax 631.589.2331
Claimant's Name KEATING, JAMESMMG File # P124944-0 -03Date Of Exam 04/14/16IME Practitioner's Name..SHEBAIRO, RAYMOND, MDCarrier's File # 15W00292A copy of this report was sent to the following parties on
Carrier: ATTN: MS. JESSICA CARUSOSUFFOLK COUNTY RISK MGMTP.O. BOX 6100
HAUPPAUGE, NY 11788-
Claimant KEATING, JAMESP.O. BOX 34
REMSENBURG, NY 11960
Claimant's Attorney: MCINTYRE DONOHUE ACCARDI8 EAST MAIN STREET
WCB:
Treating Physician:
Other Parties
BAYSHORE, NY 11706
Downstate Centralized MailingPO Box 5205
Binghamton, NY 13902-5205
DR. JONATHAN RAANAN54 COMMERCE DRIVE STERIVERHEAD, NY 11901-
CHERRY, EDSON & KELLY1 OLD COUNTRY ROADSUITE 410
CARLE PLACE, NY 11514-1852










![WINSFORD NEIGHBOURHOOD PLAN INDEPENDENT EXAMINATION · WINSFORD NEIGHBOURHOOD PLAN INDEPENDENT EXAMINATION ... Act 2011, to enable those ... 2 Town and ountry Planning Act [ ^T PA]](https://img.pdfslide.net/doc/110x75/5ac693147f8b9aa0518eb34d/winsford-neighbourhood-plan-independent-neighbourhood-plan-independent-examination.jpg)


















