Embed Size (px)
Citation preview

Individualizing Therapy for T2DM Management:
New options and Opportunities
CH Choi

Targets

Target
• A: Age
• B: Body weight
• C: Complications
• D: Duration
• E: Life Expectancy
• E: Expense

Target (elderly)

Lifestyle
“Not everything that can be counted counts, and not everything that counts can be counted”

思慮 --諸國亮
故欲思其利,必慮其害
(Complications/ SE);
欲思其成,必慮其敗。(Disease progression)
故仰高者,不可忽其下,(Hypoglycemia)
瞻前者不可忽其后。(Metabolomics)
君子視微知著,見始知終,
禍無從起,此思慮之政也。

Guideline: AES & EASD
Diabetes Care 2015; 38:S1-S94



Metformin
• Cost-effective
• Long safe data
• Low hypoglycemic risk
• Weight neutral
• Extra-glycemic effect
• Combination therapy

Metformin
• GI disturbance
• Twice or three times/day
• Risk of lactic acidosis in significant renal/liver/heart failure

Sulphonylurea
• Diamicron/ Minidiab/ Daonil/ Amaryl
• Cost-effective, daily dose
• SU receptor insulin secretion
• Hypoglycemia
• Weight gain
• Tolerance
• ? Adverse cardiovascular events


Role of pioglitazone

SE of pioglitazone
• Edema and weight gain (+3.6 kg)
• CHF
• Bone fracture (0.5/100 pt yr)
• Macular edema (combined with insulin)

Pioglitazone & Cancer
• Bladder cancer (FDA 10-yr prospective observational)– 2 yr: HR 1.4 (1.03-2.0)– 5 yr: HR 1.17 (0.79-1.49)– 8 yr: HR 1.07 (0.87-1.30)
• Liver cancer: OR 0.83 (0.72-0.95)• Bladder cancer (meta-analysis): HR 1.23, NNH:
5/100000• Colorectal cancer: OR 0.86 (0.79-0.94)• Lung cancer: RR 0.67 (0.51-0.87)


Role of pioglitazone
• Insulin resistant patients
– Large waist circumference
– Low HDL
– Fatty liver
• High risk or history of CVD (PROactive)

GLP-1 secretion & action

Food
GLP-1GIP
Promotes
Insulin secretionInhibits
gluconeogenesis
Vasodilates
perfusing beds Reduces
appetiteDPP-IV
Inhibits background
Glucagon secretion
Increases
Hypo-dependent
Glucagon secretion
Guyton and Hall. Textbook of Medical Physiology.

“Regular minds find
similarities in stories; finer
minds detect difference”


Glycemic parameters for DPP-4i as add-on to MET+SU: A1C reduction
DPP-4i Duration
A1C (%)
Reference
N BL ∆ VS BL
Vildagliptin50 mg BD
24 157 8.8 -1.0 Galvus PI
Sitagliptin100 mg QD
24 115 8.3 -0.6 Januvia PI
Linagliptin5mg QD
24 778 8.2 -0.7 Tradjenta PI
Saxagliptin5mg QD
24 127 8.4 -0.7 Onglyza PI
Alogliptin25mg QD
26 197 8.1 -0.5 Nesina PI
Note: This is not a head-to-head study

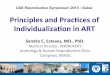
-1.34
-2.44
-3.77
-1.07
-1.49
-3.16
-1.21
-1.83
-3.41
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
Me
an d
iffe
ren
ce f
rom
bas
elin
e (
95
% C
I)
Vildagliptin
Sitagliptin
Saxagliptin*
*
HbA1C FBP 2hBG
In this randomized, open-label, parallel clinical trial, 207 T2DM patients inadequately controlled by dual combination ofmetformin and another traditional oral hypoglycemic agent (glimepiride, acarbose or pioglitazone) were randomized to add-on 5mg saxagliptin group or 100 mg sitagliptin once daily group, or 50 mg vildagliptin twice daily group for 24 weeks. * p < 0.01 forthe between-treatment difference from Vildagliptin.
Li CJ, et al. Diabetol Metab Syndr. 2014 May 31;6:69.
Mean Baseline: 8.75 8.54 8.86 8.79 8.22 8.36 11.98 10.98 11.77
Superior Fasting Blood Glucose Control of Vildagliptin - Comparison from a head-to-head study

Microvascular complications

Microvascular complications

Macrovascular complications

Primary Results
8th June 2015

Sitagliptin: Primary Composite Cardiovascular Outcome* PP Analysis for Non-inferiority
* CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352

Sitagliptin:Hospitalization for Heart Failure*ITT Analysis
* Adjusted for history of heart failure at baseline
Green JB et al. NEJM 2015; DOI: 10.1056/NEJMoa1501352

TECOS: Sitagliptin
• Pragmatic study, aiming similar A1c
• Non-inferior for primary composite MACE & secondary hospitalization for CHF
• Different inclusion criteria comparing to SAVOR-TIMI (saxagliptin) & EXAMINE (alogliptin)



Hospitalisations for heart failure, DPP-4i class effect? - Combined analysis
Analysis DPP-4i’s Placebo HR (95%CI) P value
SAVOR TIMI(n=16,492)
289 (3.5%) 228 (2.8%) 1.27 (1.07,1.51) 0.009
EXAMINE(n=5380)
106 (3.9%) 89 (3.3%) 1.19 (0.89, 1.58) 0.238
TECOS(n=14,671)
228 (3.1%) 229 (3.1%) 1.00 (0.83, 1.20) 0.983
COMBINED ANALYSIS
623 (3.4%) 546 (3.0%)1.14 (0.97, 1.34)
Test for heterogeneity for 3 trials:p=0.178, I2= 42%
Presented at ADA2015 on June 8th, unpublished data

• CV safety data collected during Phase II and Phase III clinical trials have been pooled and used
in meta-analyses to show the CV safety of the individual DPP-4 inhibitors
FDA Recommendations on Evaluating CV Risk in Drugs Intended to T2DM
FDA recommendation Sitagliptin Saxagliptin Linagliptin Alogliptin Vildagliptin
Trial duration ≥2 years
Duration of trials 12−104 weeks 24 weeks 18−52 weeks 12−26 weeks 12−104 weeks
Independent verification
of CV events
RR ≤1
Upper bound of 95% CI <1.3
Schweizer A et al. Diabetes Obes Metab 2010;12:485–94.

Vildagliptin is not associated with increased risk of MACE* and its individual components vs comparators
0. 1 1.0 10.0 100.00.01
Vildagliptin
n/N (%)
0.82 (0.61–1.11)85/7102 (1.20)83/9599 (0.86)MACE composite endpoint
0.87 (0.56–1.38)35/7102 (0.49)38/9599 (0.40)Myocardial infarction
0.84 (0.47–1.50)25/7102 (0.35)24/9599 (0.25)Stroke
0.77 (0.45–1.31)28/7102 (0.39)25/9599 (0.26)CV death
Comparators
n/N (%)
M-H RR
(95% CI)
Vildagliptin better Comparator better
*MACE, major adverse cardiovascular (CV) events–non-fatal myocardial infarction, non-fatal stroke or CV death
Vildagliptin = 50 mg qd/bid; M-H RR, Mantel-Haenszel risk ratio
Adapted from McInnes G et al. Poster no 891 presented at the 50th EASD Annual Meeting, Sep 15–19, 2014, Vienna, Austria.

Vildagliptin is not associated with increased risk of hospitalization of heart failure vs comparators
Vildagliptin 50 mg qd/bid
Vildagliptin 50 mg qd
Vildagliptin 50 mg bid
Vildagliptin
n/N (%)
1.08 (0.68-1.70)32/7102 (0.45)41/9599 (0.43)
1.19 (0.63-2.26)19/2451 (0.78)20/2201 (0.91)
0.99 (0.55-1.77)24/6229 (0.39)21/7398 (0.28)
0. 1 1.0 10.0 100.00.01
Comparators
n/N (%)
M-H RR
(95% CI)
Vildagliptin better Comparator better
*new onset or requiring hospitalization for worsening heart failure.
M-H RR, Mantel-Haenszel risk ratio
Adapted from Evans M et al. Poster no 888 presented at the 50th EASD Annual Meeting, Sep 15–19, 2014, Vienna, Austria.
Vildagliptin 50 mg bid
Incidence and relative risk for vildagliptin vs all comparators (meta-analysis)

Possible SE of DPP4ISAVOR
SaxagliptinRx Vs Plac
EXAMAlogliptinRx Vs Plac
TECOSSitagliptinRx Vs Plac
VildagliptinRx Vs Plac
(combined)
Pancreatitis 24 Vs 21 12 Vs 8 23 Vs 12 9 Vs 13
CA pancreas 5 Vs 12 0 Vs 0 9 Vs 14 0 Vs 0
Severe hypo 53 Vs 43 18 Vs 16 160 Vs 143 85 Vs 184
Hosp CHF 290 Vs 2303.5% Vs 2.8%HR 1.27 (1.07-
1.51)
160 Vs 89 3.9% Vs 3.3%
228 Vs 2293.1% Vs 3.1%
41 Vs 320.43 Vs 0.45%
Inclusion criteria
Hx or high risk AMI/ACS within 15-90days
Hx of vascular disease
All DM patients

SGLT2 inhibitor



Advantages of SGLT2 inhibitors
• Glycemic control through another mechanism
• Oral medication
• Weight loss
• May have advantages in lower SBP & FBS


Avoid using SGLT2 inhibitors…
• High risk of ketosis– Type 1 DM
– Ketosis-prone type 2 DM
• High risk of dehydration/hypovolumeia– Elderly, especially high fall risk
– Postural hypotension
– On long term diuretics
• High risk of genital infection– Recurrent infection

GLP-1 analogues

GLP-1 analogues
• Exenatide (Byetta)
• Liraglutide (Victoza)
• Lixisenatide (Lyxumia)
• …..
• Weekly preparation

GLP-1 analogues
• Lower A1c 1.0-1.5%
• Significant weight loss
• Combined with insulin
• GI side effects
• ? Increase pulse
• ? Pancreatitis
• ? Durability

Insulin



Basal analogues
• Glargine/ Detemir
• Bio-similar glargine
• Degludec
• Peglispro
• …


有連續血糖檢測功能的胰島素泵 – pump with CGMS
數據傳送器
胰島素泵
感應器
輸注器
整合血糖檢測/胰島素泵系統
配合血糖儀校正和電腦下載圖表
胰島素泵 遙控器
電腦
血糖儀
感應器/ 數據傳送器
紅外數據傳送

Individualize therapy
• Metformin• DPP-4 inhibitor• Pioglitazone/ SGLT-2 inhibitor/ SU• Acarbose
• Insulin – basal ± bolus• GLP-1 analogues• Combinations• Insulin pump


Conclusion