Embed Size (px)
Citation preview

ARTICLE
Infant Walker–Related Injuries in the United StatesAriel Sims, MS, a, b Thitphalak Chounthirath, MS, a Jingzhen Yang, PhD, MPH, a, c Nichole L. Hodges, PhD, a, c Gary A. Smith, MD, DrPHa, c, d
OBJECTIVES: To investigate the epidemiologic characteristics of infant walker–related injuries among children <15 months old who were treated in US emergency departments and to evaluate the effect of the 2010 federal mandatory safety standard on these injuries.METHODS: National Electronic Injury Surveillance System data from 1990 to 2014 were analyzed.RESULTS: An estimated 230 676 children <15 months old were treated for infant walker–related injuries in US emergency departments from 1990 to 2014. Most of the children sustained head or neck injuries (90.6%) and 74.1% were injured by falling down the stairs in an infant walker. Among patients who were admitted to the hospital (4.5%), 37.8% had a skull fracture. From 1990 to 2003, overall infant walker–related injuries and injuries related to falling down the stairs decreased by 84.5% and 91.0%, respectively. The average annual number of injuries decreased by 22.7% (P = .019) during the 4-year period after the implementation of the federal mandatory safety standard compared with the 4-year period before the standard.CONCLUSIONS: Infant walker–related injuries decreased after the implementation of the federal mandatory safety standard in 2010. This decrease may, in part, be attributable to the standard as well as other factors, such as decreased infant walker use and fewer older infant walkers in homes. Despite the decline in injuries, infant walkers remain an important and preventable source of injury among young children, which supports the American Academy of Pediatrics’ call for a ban on their manufacture and sale in the United States.
abstract
aCenter for Injury Research and Policy, The Research Institute at Nationwide Children’s Hospital, Columbus, Ohio; bCollege of Medicine and Life Sciences, University of Toledo, Toledo, Ohio; cDepartment of Pediatrics, College of Medicine, The Ohio State University, Columbus, Ohio; and dChild Injury Prevention Alliance, Columbus, Ohio
Ms Sims conducted the data analysis and drafted and revised the manuscript; Mr Chounthirath assisted in the data analysis and revised the manuscript; Drs Yang and Hodges critically reviewed and revised the manuscript; Dr Smith conceptualized the study, assisted in the data analysis, and critically reviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
DOI: https:// doi. org/ 10. 1542/ peds. 2017- 4332
Accepted for publication Jun 13, 2018
Address correspondence to Gary A. Smith, MD, DrPH, Center for Injury Research and Policy, The Research Institute at Nationwide Children’s Hospital, 700 Children’s Dr, Columbus, OH 43205. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
PEDIATRICS Volume 142, number 4, October 2018:e20174332
WHAT’S KNOWN ON THIS SUBJECT: Infant walkers provide young children with increased mobility, which can expose them to hazardous situations, especially falls down the stairs. Although infant walker–related injuries have decreased since the mid-1990s, they continue to be a source of child injury.
WHAT THIS STUDY ADDS: Infant walker–related injuries decreased after the implementation of the federal safety standard in 2010. This decrease may, in part, be attributable to the standard and other factors, such as decreased infant walker use and fewer older infant walkers in homes.
To cite: Sims A, Chounthirath T, Yang J, et al. Infant Walker– Related Injuries in the United States. Pediatrics. 2018;142(4): e20174332
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

Infant walkers are designed for use by young children generally 5 to 15 months of age before they develop the ability to walk independently.1 Infant walkers provide this young age group with increased mobility, which often exposes them to hazardous situations.1 The majority of infant walker–related injuries occur when the child falls down the stairs in the walker.1 –8 However, infant walkers also give young children access to environments and objects that they might not otherwise be able to reach. This can result in proximity injuries from such actions as touching a hot oven door, grabbing sharp objects, or ingesting household poisons.5, 9
Infant walker–related injuries can be severe and can include skull fracture, brain injury, burns, poisoning, and drowning.1, 10 – 16 From 2004 to 2008, infant walkers were associated with 8 pediatric fatalities.17 Despite product warning labels, campaigns to educate parents, and the recommendation by the American Academy of Pediatrics (AAP) for a ban on the manufacture and sale of infant walkers, many families continue to purchase and use these devices.1, 8, 10, 18 –20
The number of infant walker–related injuries in the United States decreased markedly after (1) the introduction of stationary activity centers in 1994, which are devices without wheels that support children who are preambulatory similar to an infant walker, and (2) the revision of the infant walker voluntary safety standard, ASTM F977-96, which became effective in 1997 and required that infant walker frames be wider than a standard 36-in doorway or have a braking feature to stop the device if ≥1 wheels drop over the edge of a step.1 – 4, 9, 20 The authors of a number of studies evaluated the effect of these changes in the mid-1990s and demonstrated a decreased but persistent number of infant walker–related injuries.2 – 4 However, there has not been an evaluation of these injuries since
a mandatory safety standard for infant walkers was established by the US Consumer Product Safety Commission (CPSC) under section 104(b) of the Consumer Product Safety Improvement Act (CPSIA) in June 2010. The CPSIA is the most significant federal product safety legislation passed during the last 2 decades, and the resulting infant walker mandatory safety standard (16 CFR 1216) modified ASTM F977-07 and added more stringent requirements.7, 21
In this study, we examine the characteristics and trends associated with infant walker–related injuries in children who were treated in US emergency departments (EDs) from 1990 to 2014, and we are the first to investigate the effect of the CPSC’s 2010 mandatory safety standard on infant walker–related injuries.
METHODS
Data Source
The National Electronic Injury Surveillance System (NEISS) is managed by the CPSC and collects data on the injuries of patients who are treated in US EDs. The NEISS obtains data from ∼100 hospitals, representing a stratified probability sample of >5300 hospitals with a 24-hour ED and at least 6 beds in the United States and its territories.22, 23 Data are weighted to provide national injury estimates.
Case Selection Criteria
In this study, we retrospectively examined infant walker–related injuries among children <15 months old who were treated in US EDs from January 1, 1990, to December 31, 2014. Injuries that involved infant walkers were identified by using the NEISS product code 1508 for “baby walkers and jumpers.” Injuries that were not directly related to the infant walker, such as “fell off couch and struck walker, ” were excluded. Injuries involving non–infant walker
products, such as “baby bouncer, ” “baby jumper, ” “stroller, ” or “infant swing, ” were excluded.
Variables
NEISS case narratives were used to identify the mechanism of injury and, when applicable, the number of steps that the child fell down. The mechanism of injury was classified as (1) fell down the stairs (including fell from any elevated height, such as porches or decks), (2) fell out of infant walker (including tipped over, flipped over, and climbed out), (3) proximity mechanism (including pulled on object and direct thermal contact), and (4) other (including struck surface, struck by object or person, entanglement, product malfunction, removed from infant walker by person, and other specified mechanisms). If multiple injury mechanisms were referenced in the narrative, the first mechanism in the sequence of events was coded as the mechanism of injury. For example, if a child fell out of an infant walker and struck the edge of a table, the injury mechanism was coded as fell out of infant walker rather than struck object or person. The number of steps that the child fell down was grouped into 2 categories: ≤10 steps or >10 steps. For narratives specifying a range for the number of steps (eg, 4–10 steps), the median number of steps was used.
Body region that was injured was categorized as (1) head or neck (including head, neck, face, eyeball, mouth, and ear), (2) upper extremity (including shoulder, upper arm, elbow, lower arm, wrist, hand, and finger), (3) lower extremity (including upper leg, knee, lower leg, ankle, foot, and toe), and (4) other (including all remaining NEISS body region categories). Diagnoses were grouped as (1) concussion or closed-head injury (CHI) (including internal organ injury to the head), (2) laceration (including laceration, amputation,
SIMS et al2 by guest on July 13, 2020www.aappublications.org/newsDownloaded from

puncture, and nondental avulsion), (3) burn (all types), (4) soft-tissue injury (including contusion, abrasion, crush injury, hematoma, and strain or sprain), (5) fracture (including skull fracture), and (6) other (including all remaining NEISS diagnoses). If a patient sustained multiple injuries to multiple body regions, only the most severe injury and the most seriously injured body region were included in the data set. Disposition from the ED was classified as (1) treated and released (including examined and released without treatment), (2) admitted (including treated and transferred to another hospital, treated and transferred for hospitalization, treated and admitted for hospitalization within the same facility, and held for observation), and (3) left against medical advice.
Injury location was categorized as (1) home (including house, apartment or condo, farm or ranch, and mobile or manufactured home) and (2) other (including street or highway, industrial place, school or day care, sports or recreational place, and other public property). Other variables included patient age and sex.
Statistical Analysis and Ethical Statement
Data were analyzed by using IBM SPSS Statistics for Windows version 21.0 (IBM Corporation, Armonk, NY) and SAS Enterprise Guide version 7.15 (SAS Institute Inc, Cary, NC). To account for the NEISS sampling design, complex survey procedures were used to calculate national estimates, and the Taylor series linearization method was used to calculate the variance of estimates. All estimates reported in this study are stable national estimates unless stated otherwise. An estimate is potentially unstable if the sample size is <20 cases, the estimate is <1200 cases, or the coefficient of variation is >33.0%. Preliminary analyses of scatter plots
indicated that the number of infant walker–related injuries peaked in 1991 and then decreased through 2014, with the rate of the decrease changing in 2002 for the number of concussions or CHIs and in 2003 for infant walker–related injuries overall. Therefore, trend analyses were performed by using piecewise linear regression with breakpoints at 2002 for concussions or CHIs and at 2003 for infant walker–related injuries overall. The estimated slope from the regression model was reported along with the associated P value. To assess the effectiveness of the 2010 federal safety standard, a t test was used to compare the average annual number of injuries during a 4-year period before (2006–2009) and after (2011–2014) the standard went into effect. Other statistical analyses included the Rao–Scott χ2 test for association and calculation of relative risks (RRs) with 95% confidence intervals (CIs). Statistical significance was determined at α = .05. This study was judged exempt by the institutional review board of the authors’ institution.
RESULTS
General Characteristics
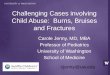
From 1990 to 2014, an estimated 230 676 (95% CI: 189 808–271 544) children <15 months old were treated in US EDs for infant walker–related injuries, averaging 9227 (95% CI: 7592–10 862) children annually. The median age of children who were injured was 8.2 months (interquartile range: 6.9–9.7), with children 7 to 10 months old accounting for 68.3% of infant walker–related injuries (Fig 1). Most (59.1%) of the reported injuries were among boys, and 98.8% of the injuries occurred at home (Table 1).
Body Region Injured, Diagnosis, and Disposition From ED
The majority (90.6%) of children sustained an injury to the head or neck, and 4.5% of children sustained an injury to the upper extremities (Table 1). Most of the injuries were a soft-tissue injury (50.5%), concussion or CHI (26.5%), or laceration (10.1%). Fractures accounted for 5.1% of the injuries, and of these, 55.4% were skull fractures. Most (95.4%) of the children who were
PEDIATRICS Volume 142, number 4, October 2018 3
FIGURE 1Estimated number of infant walker–related injuries among children <15 months old treated in US EDs by age and sex (NEISS 1990–2014).
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

injured were treated and released, and 4.5% were admitted. Among those admitted, 37.8% had a skull fracture, and 29.2% had a concussion or CHI.
Mechanism of Injury
Almost three-fourths (74.1%) of infant walker–related injuries resulted from a fall down the
stairs (Table 1). The percentage of injuries associated with falling down the stairs decreased from 80.4% during 1990–1996 to 66.4% during 1997–2009 and to 40.6% during 2010–2014. Most (95.9%) of the children who fell down the stairs sustained injuries to the head or neck and were diagnosed with a soft-tissue injury (54.0%) or concussion
or CHI (29.8%). The number of steps that the child fell down was available for 78 270 children who fell down the stairs, and among these, 66.3% of children fell down ≤10 steps, and the median number of steps was 5.7 (interquartile range: 2.9–11.8). Among the 6539 children who were diagnosed with a skull fracture, 91.4% fell down the stairs. Patients who fell down >10 steps were more likely to be diagnosed with a fracture (RR: 2.51; 95% CI: 1.69–3.72), especially a skull fracture (RR: 5.04*; 95% CI: 3.06–8.29), compared with those who fell down ≤10 steps.
A fall out of an infant walker was the second most common mechanism of injury, accounting for 14.7% of injuries. Similar to falling down the stairs, most of these injuries occurred to the head or neck (95.1%) and were diagnosed as a soft-tissue injury (48.1%), concussion or CHI (21.4%), or laceration (21.2%). Although proximity mechanisms accounted for only 2.8% of infant walker–related injuries, 74.0% of these were burn injuries and occurred mostly to the upper extremities (42.8%) or head or neck (39.8%). Among children who were injured via proximity mechanisms, 14.5%* were admitted, and all were admitted for burns.
Injury Trends
The annual number of infant walker–related injuries decreased significantly by 84.5% (slope: −1766.5; P < .001), from 20 650 injuries in 1990 to 3201 injuries in 2003 followed by a nonsignificant 37.5% decline from 2003 to 2014 (slope: −66.0; P = .556) (Fig 2). The overall reduction in injuries was primarily a result of a decline in falls down the stairs. The number of injuries associated with this mechanism decreased significantly by 91.0% (slope: −1500.8; P < .001) from 1990 (16 386 injuries) to 2003 (1473 injuries)
* Potentially unstable estimates.* Potentially unstable estimates.
SIMS et al4
TABLE 1 Characteristics of Infant Walker–Related Injuries Among Children <15 Months Old Treated in US EDs (NEISS 1990–2014)
Characteristics National Estimate, n (%a) 95% CI
Study total 230 676 (100) 189 808–271 544Sex Male 136 214 (59.1) 111 599–160 830 Female 94 293 (40.9) 77 776–110 809 Subtotal 230 507 (100.0) 189 917–271 097Location Home 169 312 (98.8) 137 361–201 264 Other 1996 (1.2) 1324–2668 Subtotal 171 308 (100.0) 139 231–203 386Body region injured Head or neck 206 709 (90.6) 168 563–244 856 Upper extremity 10 244 (4.5) 8327–12 160 Lower extremity 4595 (2.0) 3425–5765 Other 6599 (2.9) 4939–8258 Subtotal 228 146 (100.0) 187 764–268 528Diagnosis Soft-tissue injury 115 897 (50.5) 94 575–137 220 Concussion or CHI 60 967 (26.5) 41 561–80 373 Laceration 23 259 (10.1) 19 042–27 477 Fracture 11 798 (5.1) 8435–15 160 Burn 5397 (2.4) 3938–6856 Other 12 327 (5.4) 10 192–14 463 Subtotal 229 646 (100.0) 189 045–270 246Disposition from ED Treated and released 219 653 (95.4) 181 010–258 297 Admitted 10 408 (4.5) 7426–13 390 Left against medical advice 212 (0.1)b 2–422 Subtotal 230 273 (100.0) 189 615–270 931Mechanism of injury Fell down the stairs 169 809 (74.1) 134 715–204 903 Fell out of walker 33 776 (14.7) 27 387–40 165 Proximity mechanism 6455 (2.8) 4942–7969 Pulled on object 4378 (1.9) 3211–5546 Direct thermal contact 2077 (0.9) 1342–2812 Other 19 244 (8.4) 16 025–22 463 Struck on surface 8451 (3.7) 6629–10 273 Struck by object or person 2836 (1.2) 2019–3654 Entanglement 1689 (0.7) 1117–2260 Product malfunction 1149 (0.5)b 581–1717 Removed from walker by adult 907 (0.4)b 432–1383 Other 4211 (1.8) 3147–5275 Subtotal 229 284 (100.0) 188 769–269 799No. steps child fell down ≤10 steps 51 917 (66.3) 39 476–64 358 >10 steps 26 353 (33.7) 19 889–32 816 Subtotal 78 270 (100.0) 60 418–96 121
a Percentages may not sum to 100.0% because of rounding error.b Potentially unstable estimate because of sample size <20 cases, estimate <1200 cases, or coefficient of variation >33%.
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

and continued to decline by 59.7% from 2003 to 2014 (593* injuries), although this decrease was not statistically significant (slope: −47.4; P = .628). The number of injuries associated with other mechanisms also decreased significantly by 58.9% (slope: −265.2; P < .001) from 4200 injuries in 1990 to 1728 injuries in 2003 and then decreased nonsignificantly (slope: −20.0; P = .413) by 18.9% to 1402 injuries in 2014. The number of infant walker–related concussions or CHIs decreased by 82.4% (slope: −457.6; P < .001) from 4698 in 1990 to 828* in 2002 and remained constant (slope: −5.3; P = .881) from 2002 to 2014 (858* injuries; Fig 3).
There was a 22.7% (P = .019) decrease in the average annual number of infant walker–related injuries during the 4-year period (2165 injuries annually for 2011–2014) after the federal mandatory safety standard went into effect in 2010 compared with the 4-year period before the standard (2801 injuries annually for 2006–2009; Fig 4). Although the average annual number of injuries associated with falls down the stairs decreased by 40.7% (1479 annual injuries in 2006–2009 compared with 878* annual injuries in 2011–2014; P = .020), the average annual number of injuries associated with other mechanisms increased slightly by 2.3% (1225 annual injuries in 2006–2009 compared with 1253* annual injuries in 2011–2014; P = .857) after the implementation of the mandatory standard.
DISCUSSION
From 1990 to 2014, an estimated 230 676 children <15 months old
* Potentially unstable estimates.* Potentially unstable estimates.* Potentially unstable estimates.* Potentially unstable estimates.* Potentially unstable estimates.
were treated in US EDs for infant walker–related injuries. The characteristics of these injuries are in agreement with those found in studies from other countries.8, 14, 24 – 28 Similar to what was reported in previous studies, the majority of infant walker–related injuries resulted from falls down the stairs, were sustained to the head or neck, and were diagnosed as a soft-tissue injury or concussion or CHI.2, 10, 11, 24, 28
There was an 84.5% decline in infant walker–related injuries from 1990 to 2003, which was driven by a 91.0% decrease in falls down the stairs during this period. This reduction is most likely attributable to (1) a decrease in infant walker use after an increase in public awareness of infant walker–related injury risks when advocacy groups petitioned the CPSC in 1992 to ban infant walker sales in the United States, (2) the increasing use of stationary activity
PEDIATRICS Volume 142, number 4, October 2018 5
FIGURE 2Estimated number of infant walker–related injuries among children <15 months old treated in US EDs by year and mechanism of injury (NEISS 1990–2014).
FIGURE 3Estimated annual number of infant walker–related concussions or CHIs among children <15 months old treated in US EDs (NEISS 1990–2014).
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

centers as an alternative to infant walkers, and (3) improvements in the voluntary infant walker safety standard.7 Introduced in the United States in 1994, stationary activity centers resemble infant walkers but are without wheels and allow a child to rock, bounce, and swivel without the mobility to fall down the stairs or approach other hazards.1, 2, 20 As use of stationary activity centers increased, infant walker use and injuries began to decrease (Fig 2).20
The voluntary safety standard ASTM F977 for infant walkers was first established in 1986.29 It initially addressed tip overs and structural failures, but in 1996, it was revised to address falls down the stairs. Effective in 1997, ASTM F977-96 required that infant walkers be wider than a standard doorway or brake to a halt if ≥1 wheels drop over the edge of a step.1, 2, 4, 9, 20 There were subsequent minor revisions to the voluntary standard until June 2010, when the CPSC issued a mandatory standard (16 CFR 1216) for infant walkers under section 104(b) of the CPSIA, which modified ASTM F977-07 and included more stringent
requirements.7, 21 It standardized the evaluation method for falls down the stairs by creating specifications for testing equipment and a new formula for calculating launch distance that incorporated the weight of the infant walker. The mandatory rule also added a parking brake test for infant walkers that had a parking brake, which was adopted from European standards.21 These new requirements in the mandatory standard would be expected to primarily affect the likelihood of falls down the stairs. In addition, a mandatory standard makes it easier for the CPSC to stop noncompliant infant walkers at entry points to the United States before they enter the marketplace. This is important because all of the 10 infant walker recalls from 2001 to 2010 were imported products.7
The average annual number of infant walker–related injuries decreased by 22.7% during the 4-year period after the implementation of the federal mandatory safety standard compared with the previous 4-year period, whereas the average annual number of injuries associated with falls down the stairs decreased by
40.7% between these 2 periods. Although the federal standard may have contributed to this decline, its impact is uncertain because of a number of potentially confounding factors and the lack of a comparison group. The frequency of injuries had been decreasing before its implementation. Other factors, such as changes in infant walker sales and the number in use, the life span of old infant walkers in homes, and infant walker recalls, may have influenced the observed decline in injuries.
Although there was a decrease in the percentage of infant walker–related injuries associated with falling down the stairs from 80% during the beginning of the study period to 41% during the end of the period, falls down the stairs continue to be the leading injury mechanism associated with these products. Friction strips attached to the bottom of infant walkers are the most commonly employed braking feature and are designed to stop falls by gripping the floor if ≥1 wheels go over the edge of the top step. However, they may become ineffective over time because of overuse and accumulated debris, and strong children may be able to bypass the friction strips by lifting up on the walker.7, 17 In addition, the type of floor surface and the child’s weight can influence the effectiveness of braking systems.6 Although federal regulations also require infant walkers to meet forward and backward tip-resistance tests to ensure proper stability, 14.7% of infant walker–related injuries in the current study were caused by children falling out of the walker, including from tip overs.17
From 2001 to 2010, there were 10 infant walker recalls because of failure to meet the stair-fall prevention requirement, and given that only an estimated 10% of recalled children’s products are properly corrected, replaced, or returned by consumers, many noncompliant infant walkers
SIMS et al6
FIGURE 4Estimated annual number of infant walker–related injuries among children <15 months old treated in US EDs before and after the mandatory federal safety standard went into effect (NEISS 2006–2014).
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

remain in homes today.7, 30 In addition, although infant walkers that were purchased before 2010 will eventually be discarded, the mandatory standards will not be able to eliminate the dangers associated with these older products that may still remain in use.
Parental motivation to use infant walkers stems from the perceptions that they offer entertainment, promote walking, and provide an infant with an activity while parents are engaged in other activities.1, 5, 20, 31 Contrary to some parents’ belief that infant walkers accelerate walking skills or motor development, studies reveal that their use can transiently delay mental and motor development.1, 2, 12, 28, 31 – 34 Infant walkers can give parents a false sense of security. Because children in infant walkers can travel at speeds up to 1 m/second, adults have little time to react to dangerous situations.1, 2 The increased mobility that infant walkers provide to young children increases their risk of proximity injuries from access to items such as heaters, hot beverages, and poisons.9
Warning labels and educational campaigns have not been shown to be effective strategies for reducing infant walker–related injuries.1, 2 The authors of 1 study found that 59% of families whose child was treated in an ED for an infant walker–related injury reported knowing of the potential dangers associated with the product before the incident, and 32% indicated that they used
the device again after the injury.10 Because infant walkers provide no substantial benefit to children and pose a significant injury risk, Canada banned the manufacture, sale, and importation of infant walkers in 2004, and the AAP recommends that the United States also adopt such a policy.1, 2, 7, 21, 35 Combining a ban with a public education campaign and offering incentives for the return of infant walkers could improve the success of such an initiative.19, 25
This study has several limitations. In this study, we underestimate the true number of infant walker–related injuries because the NEISS only identifies injuries of patients who are treated in EDs and does not include those who are treated in urgent care centers and other health care settings or those for whom medical care is not sought. The NEISS also does not capture fatalities that are not transported to the ED or that occur after inpatient admission. The level of detail that is contained in NEISS narratives is based on information documented in ED medical records and extracted by NEISS coders and therefore can be inconsistent. Information was not available regarding the safety features that were incorporated into the individual infant walkers in this study. In addition, some estimates in this study are potentially unstable because of small numbers of injuries. We were also unable to quantify the effects of potential confounding factors, such as infant walker sales and use over time. Despite the limitations of this study, we provide a
comprehensive epidemiologic update on infant walker–related injuries over a 25-year period using a large, nationally-representative sample with an investigation of the effect of the mandatory federal infant walker safety standard on these injuries.
CONCLUSIONS
Infant walker–related injuries decreased after the implementation of the federal mandatory safety standard in 2010. This decrease may, in part, be attributable to the standard as well as other factors, such as decreased infant walker use and fewer older infant walkers in homes. Despite the decline in injuries, infant walkers remain an important and preventable source of injury among young children, which supports the position of the AAP to call for a ban on their manufacture and sale in the United States.
PEDIATRICS Volume 142, number 4, October 2018 7
FUNDING: Ms Sims received a research stipend from the National Student Injury Research Training Program at the Center for Injury Research and Policy at The Research Institute at Nationwide Children’s Hospital and was funded by the National Center for Injury Prevention and Control, the Centers for Disease Control and Prevention (grant R49CE002106), and the Child Injury Prevention Alliance while she worked on this study. The interpretations and conclusions in this article do not necessarily represent those of the funding organizations.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
ABBREVIATIONS
AAP: American Academy of Pediatrics
CHI: closed-head injuryCI: confidence intervalCPSC: Consumer Product Safety
CommissionCPSIA: Consumer Product Safety
Improvement ActED: emergency departmentNEISS: National Electronic Injury
Surveillance SystemRR: relative risk
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

REFERENCES
1. American Academy of Pediatrics. Committee on Injury and Poison Prevention. Injuries associated with infant walkers. Pediatrics. 2001;108(3):790–792
2. Shields BJ, Smith GA. Success in the prevention of infant walker-related injuries: an analysis of national data, 1990-2001. Pediatrics. 2006;117(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 117/ 3/ e452
3. Rodgers GB, Leland EW. An evaluation of the effectiveness of a baby walker safety standard to prevent stair-fall injuries. J Safety Res. 2005;36(4):327–332
4. Rodgers GB, Leland EW. A retrospective benefit-cost analysis of the 1997 stair-fall requirements for baby walkers. Accid Anal Prev. 2008;40(1):61–68
5. Fazen LE III, Felizberto PI. Baby walker injuries. Pediatrics. 1982;70(1):106–109
6. Ridenour MV. How effective are brakes on infant walkers? Percept Mot Skills. 1997;84(3, pt 1):1051–1057
7. US Consumer Product Safety Commission. Statement of the Honorable Thomas H. Moore on the final rule for infant walkers under section 104(b) of the Consumer Product Safety Improvement Act (CPSIA). 2010. Available at: https:// www. cpsc. gov/ ~/ link/ 136cf994237446f59 98d36f7b0c1f349. pdf. Accessed December 12, 2017
8. Shiva F, Ghotbi F, Yavari SF. The use of baby walkers in Iranian infants. Singapore Med J. 2010;51(8):645–649
9. Thompson PG. Injury caused by baby walkers: the predicted outcomes of mandatory regulations. Med J Aust. 2002;177(3):147–148
10. Smith GA, Bowman MJ, Luria JW, Shields BJ. Babywalker-related injuries continue despite warning labels and public education. Pediatrics. 1997;100(2). Available at: www. pediatrics. org/ cgi/ content/ full/ 100/ 2/ e1
11. Chiaviello CT, Christoph RA, Bond GR. Infant walker-related injuries: a prospective study of severity and incidence. Pediatrics. 1994;93(6, pt 1):974–976
12. Cassell OC, Hubble M, Milling MA, Dickson WA. Baby walkers–still a major cause of infant burns. Burns. 1997;23(5):451–453
13. Mroz LS, Krenzelok EP. Examining the contribution of infant walkers to childhood poisoning. Vet Hum Toxicol. 2000;42(1):39–40
14. Barss P, Grivna M, Al-Hanaee A, Al-Dhahab A, Al-Kaabi F, Al-Muhairi S. Baby walker injury, disability, and death in a high-income middle eastern country, as reported by siblings. Inj Epidemiol. 2016;3(1):17
15. Gaw CE, Chounthirath T, Smith GA. Nursery product-related injuries treated in United States emergency departments. Pediatrics. 2017;139(4):e20162503
16. Sabir H, Mayatepek E, Schaper J, Tibussek D. Baby-walkers: an avoidable source of hazard. Lancet. 2008;372(9654):2000
17. US Consumer Product Safety Commission. Notice of proposed rulemaking for infant walkers briefing package. 2009. Available at: https:// www. cpsc. gov/ PageFiles/ 88525/ infantwalkers. pdf. Accessed December 12, 2017
18. Chagas PS, Mancini MC, Tirado MG, Megale L, Sampaio RF. Beliefs about the use of baby walkers. Rev Bras Fisioter. 2011;15(4):303–309
19. Desapriya E, Scime G, Subzwari S, Pike I. Prevention of baby-walker-related injury. Lancet. 2009;373(9663):545
20. DiLillo D, Damashek A, Peterson L. Maternal use of baby walkers with young children: recent trends and possible alternatives. Inj Prev. 2001;7(3):223–227
21. US Consumer Product Safety Commission. CPSC issues final mandatory rule on infant baby walkers. 2010. Available at: https:// www. cpsc. gov/ content/ cpsc- issues- final- mandatory- rule- on- infant- baby- walkers. Accessed December 12, 2017
22. US Consumer Product Safety Commission. NEISS: the National Electronic Injury Surveillance System: a tool for researchers. 2000. Available at: https:// www. cpsc. gov// PageFiles/
106626/ 2000d015. pdf. Accessed December 12, 2017
23. Schroeder T, Ault K. The NEISS Sample (Design and Implementation) 1997 to Present. Washington, DC: US Consumer Product Safety Commission; 2001. Available at: https:// www. cpsc. gov// PageFiles/ 106617/ 2001d011- 6b6. pdf. Accessed December 12, 2017
24. Emanuelson I. How safe are childcare products, toys and playground equipment? A Swedish analysis of mild brain injuries at home and during leisure time 1998-1999. Inj Control Saf Promot. 2003;10(3):139–144
25. Morrison CD, Stanwick RS, Tenenbein M. Infant walker injuries persist in Canada after sales have ceased. Pediatr Emerg Care. 1996;12(3):180–182
26. Morrison L, Chalmers DJ, Parry ML, Wright CS. Infant-furniture-related injuries among preschool children in New Zealand, 1987-1996. J Paediatr Child Health. 2002;38(6):587–592
27. Petridou E, Simou E, Skondras C, Pistevos G, Lagos P, Papoutsakis G. Hazards of baby walkers in a European context. Inj Prev. 1996;2(2):118–120
28. Stoffman JM, Bass MJ, Fox AM. Head injuries related to the use of baby walkers. Can Med Assoc J. 1984;131(6):573–575
29. US Consumer Product Safety Commission. Safety standard for infant walkers: final rule. Fed Regist. 2010;75(118):35266–35279
30. Kids in Danger. A KID report card: children’s product recalls in 2016. 2017. Available at: www. kidsindanger. org/ docs/ research/ KID_ 2017_ Annual_ Report_ 040317. pdf. Accessed December 12, 2017
31. Bar-on ME, Boyle RM, Endriss EK. Parental decisions to use infant walkers. Inj Prev. 1998;4(4):299–301
32. Siegel AC, Burton RV. Effects of baby walkers on motor and mental development in human infants. J Dev Behav Pediatr. 1999;20(5):355–361
33. Taylor B. Babywalkers. BMJ. 2002;325(7365):612
34. Badihian S, Adihian N, Yaghini O. The effect of baby walker on child
SIMS et al8 by guest on July 13, 2020www.aappublications.org/newsDownloaded from

development: a systematic review. Iran J Child Neurol. 2017;11(4):1–6
35. Health Canada. Health Canada: Canada’s new government accepts
recommendation of baby walker
board of review upholding the
product ban. 2007. Available at: www.
marketwired. com/ press- release/
health- canada- canadas- new-
government- accepts- recommendation-
baby- walker- board- review- 740656. htm.
Accessed December 12, 2017
PEDIATRICS Volume 142, number 4, October 2018 9 by guest on July 13, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-4332 originally published online September 17, 2018; 2018;142;Pediatrics
SmithAriel Sims, Thitphalak Chounthirath, Jingzhen Yang, Nichole L. Hodges and Gary A.
Related Injuries in the United States−Infant Walker
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/142/4/e20174332including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/142/4/e20174332#BIBLThis article cites 28 articles, 11 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/home_safety_subHome Safetyson_prevention_subhttp://www.aappublications.org/cgi/collection/injury_violence_-_poiInjury, Violence & Poison Preventionfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 13, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-4332 originally published online September 17, 2018; 2018;142;Pediatrics
SmithAriel Sims, Thitphalak Chounthirath, Jingzhen Yang, Nichole L. Hodges and Gary A.
Related Injuries in the United States−Infant Walker
http://pediatrics.aappublications.org/content/142/4/e20174332located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2018has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 13, 2020www.aappublications.org/newsDownloaded from