Embed Size (px)
Citation preview
A c t a P a t h . J a p . 29(3) : 377-388, 1979
INFANTILE AND ADULT FIBROSARCOMAS O F THE SOFT TISSUES
Hiroshi IWASAKI* and Munetomo ENJOJI**
* First D e p r t w n t of Pathology. Fukmka Univeraity School of Medicine, Fukuoku. ** Second Department of Pathology, Faculty of Medicine,
Kyuahu University, Fukuoku
(Received on Sept. 22, 1978)
Histologic sections of 68 soft-tissue sarcomas initially diagnosed as Abrosarcoma were reviewed, and 36 were excluded because of revised diagnosis. The tumors from the remaining 32 patients were analyzed clinicopathologically, and were classifled into two types; the adult type (22 cases) and the infantile type (10 cases). The adult type Abrosarcoma occurred in adults aged 25 to 67 years and consisted of spindle-shaped Abroblastic cells which formed interlac- ing bundles accompanied by variable amounts of collagen or reticulin fibers. The infantile Abrosarcoma affected children below the age of seven years in this series and was characterized by proliferation of immature fibroblasts forming indistinct bundles, frequently exhibiting areas of an angiosarcoma- like pattern and cavernous blood vessels. The authors expressed the view that infantile Abrosarcoma should be separated from adult Abrosarcoma, because between these two types of Abrosarcoma there were marked differences in the histologic feature as well as in the age, sex and anatomical distributions. ACTA PATH. JAP. 29: 377-388, 1979.
Introduction
Fibrosarcoma has been considered one of the most frequent sarcomas of the soft tissues, STOUT (1948) analyzed 218 cases of fibrosarcoma and clarified the histopatho- logic feature of this sarcoma. MACKENZIE (1964), who reviewed the various classihations of fibrosarcoma in the literature, divided it into three types: well, moderately, and poorly differentiated fibrosarcomas, but in 1970 he considered the majority of tumors originally classified a8 Grade I (well differentiated fibrosarcoma) should really had been labeled as musculo-aponeurotic fibromatoses, i.e. desmoid type tumors, so that fibrosar- coma should be reclassified into two types: well and poorly differentiated types! PRITCHARD et a2. (1974) reported 199 cases of adult fibrosarcoma which they classified into four groups according to microscopic criteria, and demonstrated a striking relation- ship between survival and histologic grade. CHUNG and ENZINGER (1976) reveiwed 53
$5m P, B%3 %% This work was supported by a Grant-in-Aid for Cancer Research from the Ministry of
Health and Welfare, and a Grant from the Fukuoka-ken Anti-Cancer Association. Presented at the 36th Annual Meeting of the Japanese Cancer Aseociation on October 14, 1977 in Tokyo.
Reprint requests to Dr. H. Iwasaki, Department of Pathology, Fukuoka University School of Medicine, 34 Nanakuma, Nishi-ku, Fukuoka 814, Japan.
377
378 FIBROSARCOMA A c h Path. Jap.
cases of infantile fibrosarcoma and presented the clinicopathologic characteristics of this tumor, but on the other hand, SOULE and PRITCHARD (1977) could not find any differences in the histologic features of fibrosarcoma of adults and children.
It is important to recognize the distinctive pattern of fibrosarcoma, because they are often confused with a wide variety of other soft-tissue tumors. Actually in the present study, 36 lesions that were once classified as fibrosarcoma are now recognized as belonging to other categories : malignant Schwannoma, malignant fibrous histiocytoma, leiomyosarcoma, rhabdomyosarcoma, synovial sarcoma, pseudosarcomatous carcinoma, benign fibromatosis, etc.
The purpose of this study is to demonstrate the histopathologic details of fibrosar- coma, and to fhd whether there are any differences between adult and infantile fibrosar- comas in clinical and histopathologic aspects.
Materials and Methods Histologic sections of 68 patients with a diagnosis of fibrosarcoma were collected at our
laboratory from eight institutions in Japan including ours. The patients were examined histologi- cally in each institution in a period from 1970 to 1977.
The caae history and tissue sections of each were studied. Thirty-six cases were excluded because of a revised diagnosis. They were reclassified as follows: malignant Schwannoma 6, malignant fibrous histiocytoma 3, leiomyosarcoma 3, rhabdomyosarcoma 3, synovial sarcoma 1, malignant melanoma 2, unclassified sarcoma 2, squamous cell carcinoma or pseudosarcomatous carcinoma 6, fibromatosis (desmoid tumor) 4, dermatofibrosarcoma protuberans 2, nodular fasciitis 1, neurofibroma 1, leiomyoma 1, and orbital granuloma 1.
The remaining 32 cases were studied clinicopathologically. I n all cases, hematoxylin and eosin-stained sections were available. I n 30 cases, paraffin blocks were recut and stained with Mawon’s trichrome, silver impregnation for retioulin, PAS with and without prior diastase diges- tion, and alcian blue.
Results
In this series the tumors have been put in two groups according to the histologic features described later. The 22 adult type tumors were conventional fibrosarcomas in adults, and the other 10 tumors were of infantile fibrosarcoma occurring in children below age 7 years. Adult type tumors were further divided into three subtypes: eight well differentiated, ten moderately differentiated and four poorly differentiated fibrosarcomas.
Clinical Findings
The most common symptom in the present series was a lump which varied in size from 2 cm to 15 cm in the greatest diameter. The tumors usually originated as small, firm, painless nodules which grew slowly for a long time, and might attain a large size a t the time of operation. All patients with infantile sarcomas were below 7 years of age a t the time of first operation, seven of them were below two years, four of them were discovered during the first year of life, and eight of the ten patients in this type were males (Table 1). Adult type fibrosarcomas occurring in adults aged 25 to 67 years with a median of 40 years affected 12 men and 10 women (Table I) .
29(3): 1979 H. IWASAKI AND M. ENJOJI 379
Table 1. Distribution by Age and 9ex of 32 Patienb with Pibrosarcoma
Age, yrs. Male Female Total
0- 4 6- 9
10-19
30- 39 40-49 60-89 60-69
Total
ao-a9
ao
0
0
3
3 0
la
a
a
a
~~
7 3 0 S 7 4 6 3
3a
The length of history was variable. In the infantile type sarcomas the duration of symptoms before operation varied from 20 days to one year with a median of 3 months, and in the adult type it ranged from 6 months to 17 years with a median of two years. The principal sites of involvements were different between infantile and adult sarcomas (Table 2). Half of adult type sarcomas affected the trunk, whereas all of the infantile sarcomas involved the extremities (lower leg 4, foot 2, thigh 2, upper arm 1, elbow 1). Seventeen tumors involved the skeletal muscle and/or deep fascia, and the other one was present within the retroperitoneal soft tissue. In the remaining 14 tumors the affected tissue was not indicated.
Table 2. Anatomical Distribution of Infantile and Adult Fibrosarcmnae
Site Infantile Adult
Upper extremity a Lower extremity 8 Anterior torso 0 Posterior torso 0 Head and neck 0 Retroperitoneum 0
Total 10
a 4 6 6 4 1
aa
GTOSS Appearances
Most of them (92%) were more than 3 cm, and 66% of tumors were more than 4 cm. The borders of the tumors were definite in 12 cases and indistinct in four cases. In adult Gbrosarcomas the masses were generally firm and grayish white. On the contrary, infantile fibrosarcomas often developed soft and fragile masses which were frequently well-vascularized and hemorrhagic (Fig. 9).
MiCroscopiC Appearances
Fibrosarcoma is a malignant tumor composed solely of fiber-forming connective- tissue cells. However, a great variability in the histopathology of fibrosarcoma exists,
The excised masses were measured 2 om to 16 crn in the widest diameter.
380 EIBROSARCOMA Acta Path. Jap.
2913): 1979 H. IWASAKI AND M. ENJOJI 381
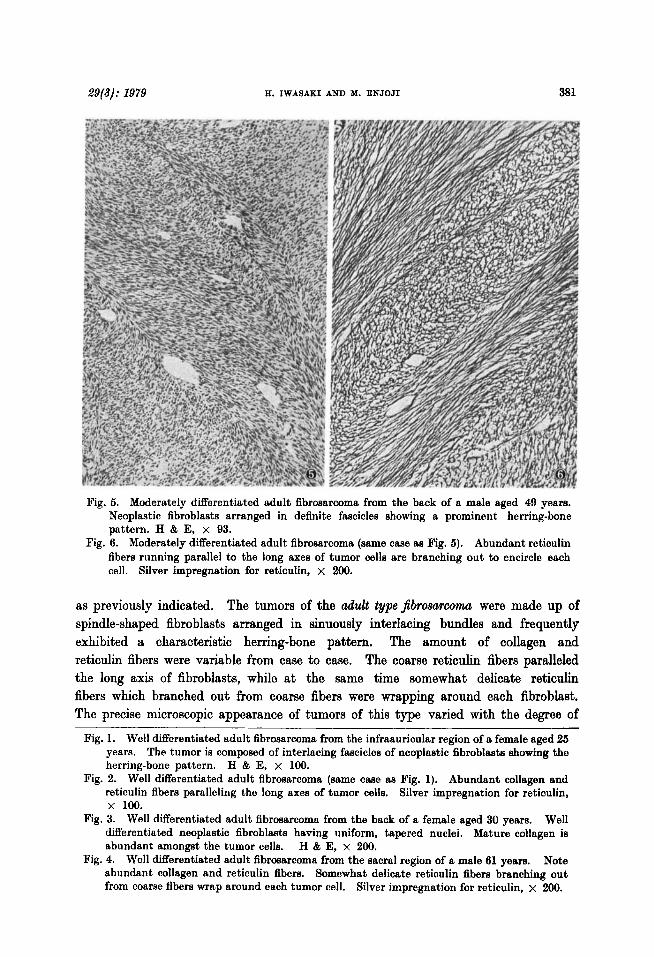
Fig. 6. Moderately differentiated adult fibrosarcoma from the back of a male aged 49 years. Neoplastic fibroblasts arranged in definite fascicles showing a prominent herringbone pattern. H & E, x 93.
Abundant reticulin fibers running parallel to the long axes of tumor cells are branching out to encircle each cell. Silver impregnation for reticulin, x 200.
Fig. 6. Moderately differentiated adult fibrosarcoma (same case as Fig. 5).
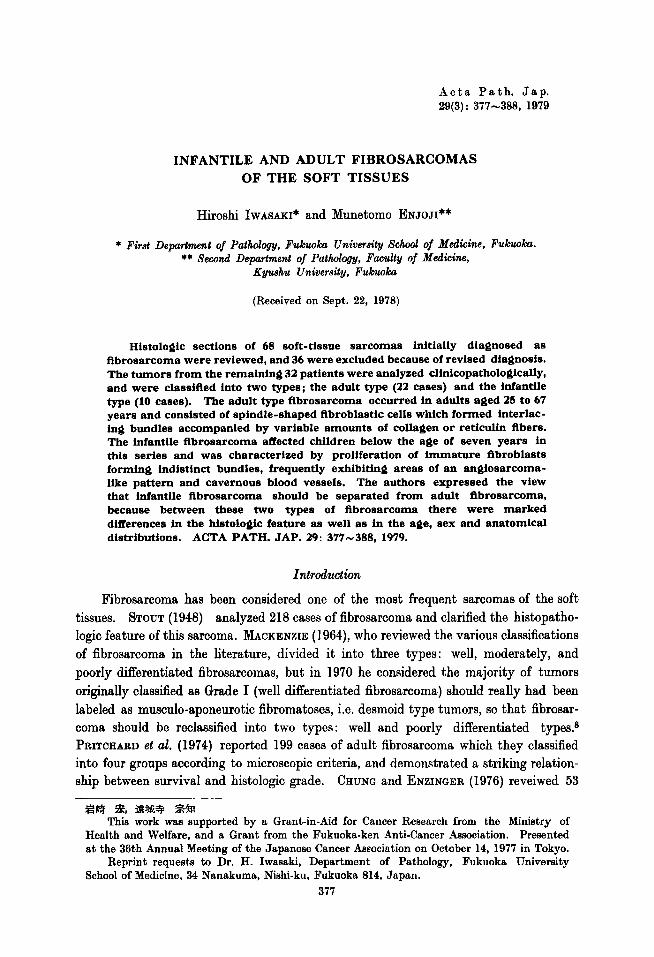
as previously indicated. The tumors of the ad& typeJibrosarcomu were made up of spindle-shaped fibroblasts arranged in sinuously interlacing bundles and frequently exhibited a characteristic herring-bone pattern. The amount of collagen and reticulin fibers were variable from case to case. The coarse reticulin fibers paralleled the long axis of fibroblasts, while a t the same time somewhat delicate reticulin fibers which branched out from coarse fibers were wrapping around each fibroblast. The precise microscopic appearance of tumors of this type varied with the degree of
Fig. 1. Well differentiated adult fibrosarcoma from the infraauricular region of a female aged 26 years. The tumor is composed of interlacing fascicles of neoplastic fibroblasts showing the herring-bone pattern. H & E, x 100.
Fig. 2. Well differentiated adult fibrosarcoma (same case as Fig. 1). Abundant collagen end reticulin fibers paralleling the long axes of tumor cells. Silver impregnation for reticulin, x loo.
Well differentiated neoplastic fibroblasts having uniform, tapered nuclei. Mature collagen is abundant amongst the tumor cells.
Note abundant collagen and reticulin fibers. Somewhat delicate reticulin fibers branching out from coarse fibers wrap around each tumor cell. Silver impregnation for reticulin, x 200.
Fig. 3. Well differentiated adult fibrosarcoma from the back of a female aged 30 years.
H & E, x 200. Fig. 4. Well differentiated adult fibrosarcoma from the sacral region of a male 61 years.
382 BIBROSARCOM A Acta Path. Jap.
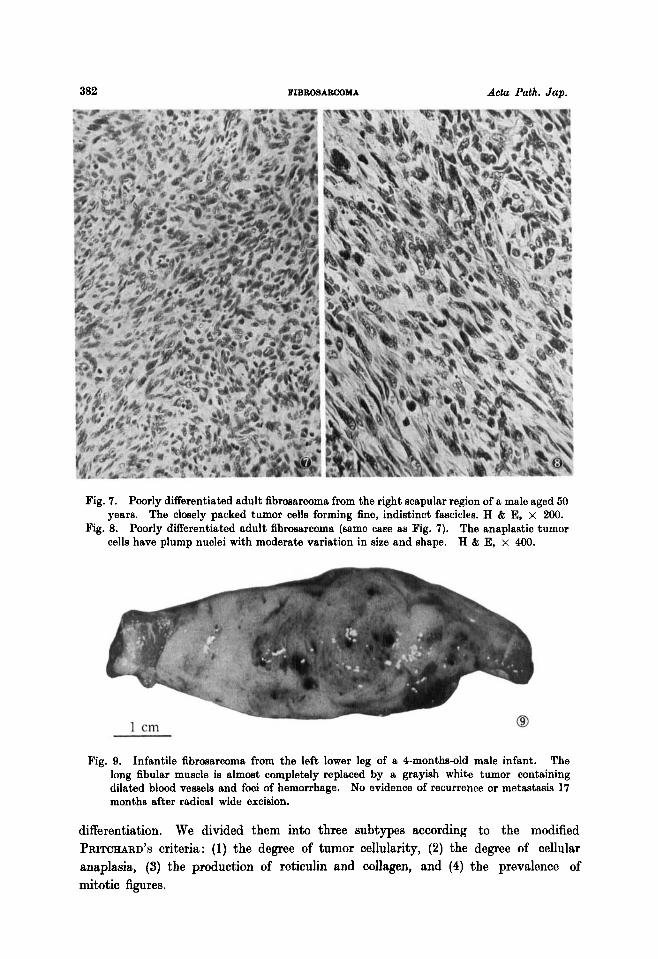
Fig. 7. Poorly differentiated adult fibrosarcoma from the right scapular region of a male aged 50 years.
Fig. 8. Poorly differentiated adult fibrosarcoma (same case as Fig. 7). The anaplastic tumor cells have plump nuclei with moderate variation in size and shape. K & E, x 400.
The closely packed tumor cells forming fine, indistinct fascicles. H & E, x 200.
Fig. 9. Infantile fibrosarcoma from the left lower leg of a 4-months-old male infant. The long fibular muscle is almost completely replaced by a grayish white tumor containing dilated blood vessels and foci of hemorrhage. No evidence of recurrence or metastasis 17 months after radical wide excision.
differentiation. We divided them into three subtypes according to the modified PRITCHARD’S criteria: (1) the degree of tumor cellularity, (2) the degree of cellular anaplasia, (3) the production of reticulin and collagen, and (4) the prevalence of mitotic figures.
29(3): 1979 H. IWASAKI AND M. ENJOJI 383
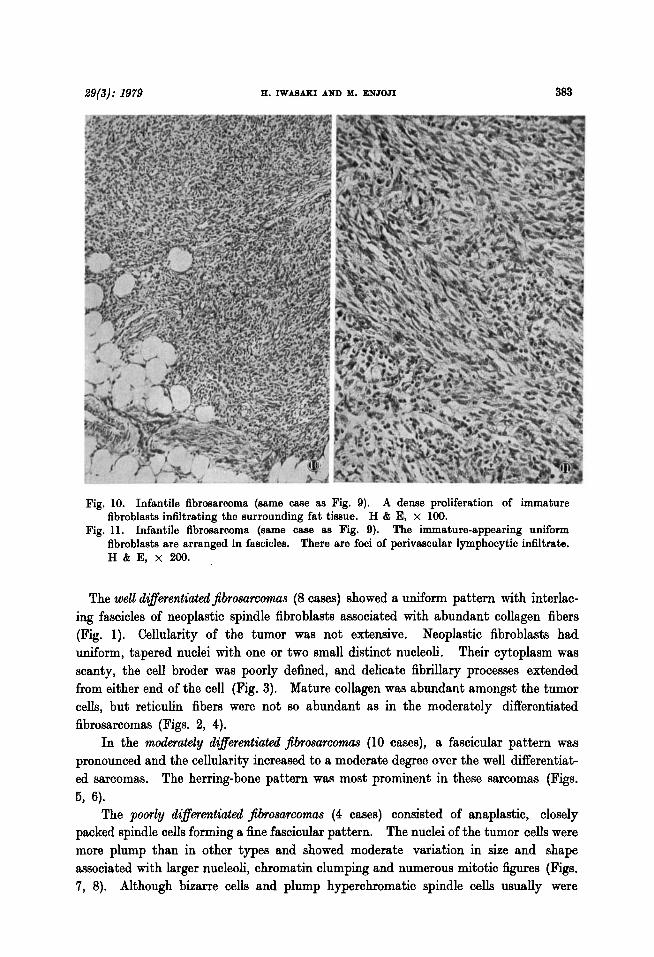
Fig. 10. Infantile fibrosarcoma (same case as Fig. 9). A dense proliferation of immature fibroblasts infiltrating the surrounding fat tisaue. H & E, x 100.
Fig. 11. Infantile fibrosarcoma (same case as Fig. 9). The immature-appearing uniform fibroblasts are arranged in fascicles. There are foci of perivascular lymphocytic infiltrate. H & E, x 200.
The well di$erentiated$brosarcomas (8 cases) showed a uniform pattern with interlac- ing fascicles of neoplastic spindle fibroblasts associated with abundant collagen fibers (Fig. 1). Cellularity of the tumor was not extensive. Neoplastic fibroblasts had uniform, tapered nuclei with one or two small distinct nucleoli. Their cytoplasm was scanty, the cell broder was poorly defined, and delicate fibrillary processes extended from either end of the cell (Fig. 3). Mature collagen was abundant amongst the tumor ceh, but reticulin fibers were not so abundant as in the moderately differentiated fibrosarcomas (Figs. 2, 4).
In the moderately differentiated Jibrosarcomas (10 cases), a fascicular pattern was pronounced and the cellularity increased to a moderate degree over the well differentiat- ed sarcomas. The herring-bone pattern was most prominent in these sarcomas (Figs.
The pomly differentiated Jibrosarcomas (4 cases) consisted of anaplastic, closely packed spindle cells forming a fine fascicular pattern. The nuclei of the tumor cells were more plump than in other types and showed moderate variation in size and shape associated with larger nucleoli, chromatin clumping and numerous mitotic figures (Figs. 7, 8). Although bizarre cells and plump hyperchromatic spindle cells usually were
5, 6).
384 FIBR081LBOOYA Acta Path. Jap.
29(3): 1979 H. IWASAKI AND 111. ENJOJI 386
present, multinucleated giant cells were never a conspicuous feature in these fibrosarcomas. Both collagen and reticulin fibers were more scant than in well and moderately differentiated sarcomas.
The infantile type Jibrosarcomas (10 cases) bore a close resemblance to the adult type fibrosarcomas, but the tumor cells appeared less mature. The neoplastic spindle fibroblasts were uniform and were arranged in indistinct bundles or fascicles (Figs. 10, 11, 14). Their cytoplasms were ill-defined and amphophilic in routine hematoxylin and eosin-stained sections, but they were faintly fuchsinophilic with the Masson's trichrome stain. Occasional tumor cells contained a small amount of glycogen in the cytoplasm which was PAS-positive and digested by diastase. Nuclear pleo- morphism and tumor giant cells were almost completely absent. Mitotic figures were present, but their number varied from tumor to tumor. Focal perivascular inflammatory infiltration consisting of lymphocytes and plasma cells was a prominent feature in some cases (Fig. 11). The herring-bone pattern was present in three cases, but less prominent than in the adult type sarcomas. The blood vessels were well developed and, in six cases, cavernous vascular spaces were prominent in some parts of the tumors accompanied by focal endothelial proliferation, thrombosis, and hemorrhage, the feature simulating an angiosarcoma (Fig. 13). In addition, a pericytomatous pattern was observed in portions of five tumors where the tumor cells were arranged around the vascular spaces of various sizes and shapes in the manner of hemangioperi- cytoma (Figs. 12, 15). The amount of collagen or reticulin fibers was variable, but generally it was smaller than in the adult type tumors. Extramedullary hematopoiesis was not observed in any case of this series.
Treutment and Survival
Information about treatment and follow-up was not always sufficient in our series. Sixteen of our patients were treated by means of local excision. Two patients were treated by amputation. Radiation was applied to two patients. One patient was initially treated by local excision and followed by amputation and perfusion of anti-tumor agents.
There were six deaths with the fibrosarcoma within five years after initial treatment, and eleven were alive 5 to 17 years after treatment. The 3-year survival rate was 71% in infantile fibrosarcomas and 75% in adult fibrosarcomas, and the 5-year rate was 67% in infantile fibrosarcomas and 64% in adult fibrosarcomas. Relation between the histologic types and survival could not be determined because of the insufficient number of patients.
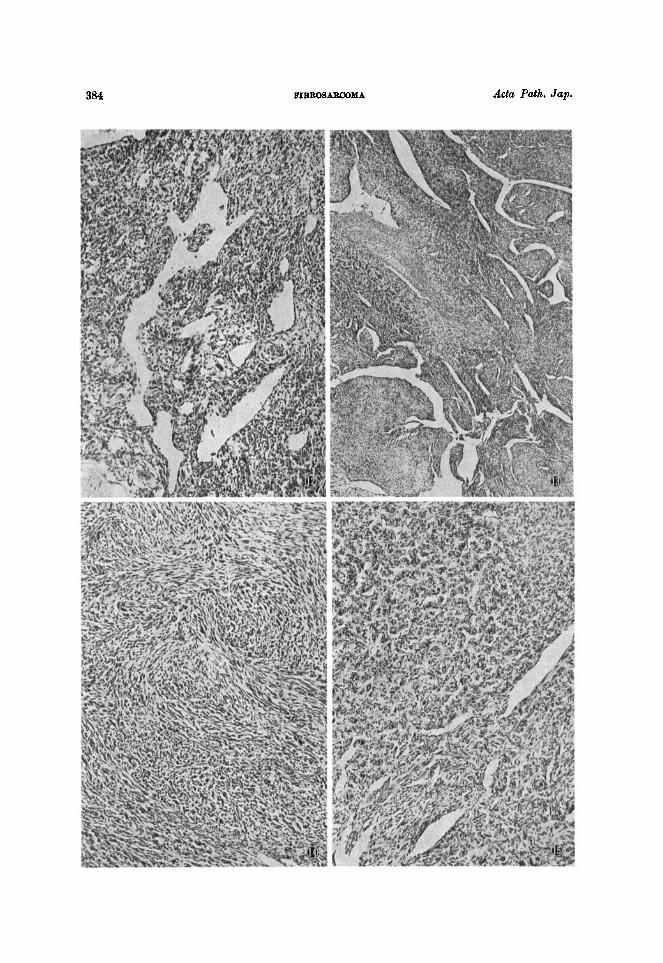
Fig. 12. Infantile fibrosarcoma (same case as Fig. 9). Hemangiopericytomatous area showing perivascular arrangement of tumor cells. H & E, x 100.
Fig. 13. Infantile fibrosarcoma from the right sole of a male aged 4 years. The tumor contains many dilated blood vessels. H & E, x 35.
Fig. 14. Infantile fibrosarcoma (same case as Fig. 13). The neoplastic fibroblasts arranged in interlacing fascicles form occasional storiform-like patterns. H & E, x 100.
Fig. 15. Infantile fibrosarcoma (same case as Fig. 13). Hemangiopericytomatous area showing tumor cells arranged around vascular spaces lined by non-neoplastic endothelial cells. H & E, x 93.
386 BIBBOSARCOYA Acta Path. Jap.
Discussion
Although for many years fibrosarcoma was considered the most commonly occurring sarcoma of the soft parts, it is now recognized that the true fibrosarcoma is a relatively rare neoplasm. Generally, the histopathologic appearance of fibrosarcoma lacks a striking peculiarity in comparison with other types of sarcomas. The herring-bone pattern, bundle formation, and abundant collagen or reticulin fibers are the characteristics of the fibrosarcoma, but sometimes these histologic features are pronounced in other forms of spindle-cell sarcomas of the soft parts.4 In 36 of the 68 cases collected for this study, the diagnosis of fibrosarcoma was revised to different diagnoses after careful re-examination. Such cases were omitted from the materials for the present analysis.
In this study we divided the fibrosarcoma into two main groups according to the clinical and histologic characteristics. The adult type fibrosarcoma which occurs only in adults and consists of interlacing bundles of fibroblasts accompanied by variable amounts of collagen and reticulin fibers is separated into three subgroups; well, moderately and poorly differentiated fibrosarcomas.
The infantile fibrosarcoma is a specific type sarcoma which seems to differ from adult fibrosarcoma. STOUT, in 1962, reported 23 cases of “juvenile fibrosarcoma” occurring in infants and children up to 16 years of age and he found 31 similar cases in the literature. Recently CHUNG and ENZINGER reported a series of fibrosarcoma occurr- ing in infants and children younger than five years, grouping under a new title of “infantile fibrosarcoma”. In their series of 63 cases, the tumor nearly always occurred during the first two years of life, was more common in boys (60%) and affected chiefly the distal portions of the lower and upper extremities (72%). Age, sex and anatomical distributions of our ten cases of infantile fibrosarcoma are similar to those of C H U N ~ and ENZINGER’S series. Microscopically, the tumors are composed of uniform immature-appearing fibroblastic spindle cells arranged in curved fascicles. The herring-bone pattern is inconspicuous in most cases of this type. As CHUNG and ENZINGER emphasized, the angiosarcoma-like vascular pattern is a striking histologic feature in some cases of infantile sarcomas. In six of our cases endothelial proliferation similar to that of angiosarcoma was prominent within the cleft-like or cavernous vascular structures associated with hemorrhage and a mild lymphocytic infiltrate. Besides, in five cases is noted a hemangiopericytoma-like arrangment of tumor cells around vascular spaces of various sizes and shapes. We think infantile fibrosarcoma should be separated from adult or common type fibrosarcoma, because between these two types of fibrosarcoma there were marked differences in the histologic features as well as in the age, sex and anatomical distributions.
Fibrosarcoma must be differentiated from various sarcomas and certain benign lesions. Malignant Schwannomas are composed of spindle tumor cells having slender nuclei admixed with a small number of round cells; the tumor cells are arranged in a complicated loose and dense pattern or in concentric spherical structures, and the reticulin fibers of malignant Schwannoma usually are delicate and wavy.4 The spindle
2913): 1979 E. IWASAKI AND M. ENJOJI 381
cells of leiomyosarcomas have cigarette-shaped nuclei and eosinophilic abundant cyto- plasm stained deep red with Masson’s trichrome, frequently exhibiting intra-cytoplasmic longitudinal fibrils and “Sonnenbild” or perinuclear halo ; the cells usually form inter- secting bundles which are separated from each other and encricled by collagen or thick reticulin fibers in cross section.
Fibrosarcoma-like spindle cell areas are also common in liposarcoma, synovial sarcoma, rhabdomyosarcoma, angiosarcoma, and malignant fibrous histiocytoma. Myxoid liposarcoma contains vacuolated cells and stellate cells within a myxomatous stroma associated with plexiform networks of capillaries. Pleomorphic liposarcoma and fibrosing liposarcoma are characterized by bizarre pleomorphic giant cells, and should never cause much confusion. Furthermore, stroma and cytoplasm of the tumor cells in liposarcomas are strongly positive for alcian-blue. Synovial sarcoma is suggested, if the tumor is located in the vicinity of a large joint, and affects a patient between 16 and 36 years of age.%’ The typical biphasic pattern, uniform spindle- cell component and deposition of calcium are diagnostic for synovial sarcoma.
The presence of acidophilic round cells and strap cells and the presence of cross-striations in some tumor cells are not the features of infantile fibrosarcoma. When characterized by many blood vessels and perivascular arrangement of tumor cells, infantile fibro- sarcoma may be confused with malignant hemangioendothelioma or malignant hemang- iopericytoma, but the proliferating endothelial cells appear non-neoplastic without cellular anaplasia, and the pericytoma-like pattern is restricted only to small portion of infantile fibrosarcoma.
If a storiform-like pattern is present, fibrosarcoma must be differentiated from malignant fibrous h i s t i o ~ y t o m a . ~ ~ ~ ~ ~ ~ ~ ~ ~ In contrast to the fibrosarcoma which is a pure spindle-cell tumor, polymorphic cellular infiltration is the hallmark of malignant fibrous histiocytoma. Clear-cell sarcoma can readily be separated from fibrosarcoma by the presence of “clear” tumor cells with large nucleoli bearing little resemblance to the fibroblasts of fibrosarcoma.
Pseudosarcomatous carcinoma of the skin consisting of fibroblast-like spindle cells may be confused with fibrosarcoma, especially when the tumor involves the skin. The pseudosarcomatous carcinoma, however, mainly involves the dermis and forms a superficial polypoid lesion and infiltration of the deeper structures such as muscles and tendons is not marked.
Among the benign lesions, desmoid tumor is most frequently confused with fibrosarcoma. The major distinguishing factors between these two conditions are cellularity, nuclear atypism and the number of mitotic figures which are never prominent in desmoid, but are prominent in fibrosarcoma. Moreover the herring-bone pattern is common in fibrosarcoma, but is inconspicuous in desmoid.
Acknowledgement: The authors are grateful to the following members of the study group for malignant soft-tissue tumors who submitted the caees and when possible furnished follow-up informa- tion: Dr. K. FURUYA, Tokyo Medical and Dental University; Dr. E. ISHIKAWA, Jikei University School of Medicine; the late Dr. R. SANO and Dr. E. HIRQTA, National Cancer Center, Tokyo; Dr.
Infantile fibrosarcoma may be confused with embyronal rhabdomyosarcoma.
388 FIEROSARCOMA Ada Path. Jap.
A. TATEISHI, University of Tokyo; Dr. H. USIZIMA, Nagoya University; Dr. K. HIZAWA, Tokushima University; and Drs. I. MAEYAMA and T. YUMOTO, Tottori University.
1. 2.
3.
4.
5.
6.
7. 8.
9.
10.
11.
12. 13. 14.
R e f e r e m
Infantile fibrosaroma. Cancer 38: 729-739, 1976. CHUNQ, E.B. and ENZINQER, F.M.: ENZINQER, F.M. : Recent developments in classification of soft tissue sarcomas, pp. 219-234. In: Menagment of Bone and Soft Tissue Tumors. Year Book Medical Publishers Inc., Chicago, 1977. ENZINQER, F.M. and Smith, B.H.: Hemsngiopericytoma. An analysis of 106 cases. Hum. Pathol. 7: 61-82, 1976. IWASAKI, H. : Spindle cell sarcomas of soft tissues. A histopathologic analysis and differential diagnosis. Fukuoka Acta Med. 68: 183-185, 1977 (in Japaneae). KEMPSON, R.L. and KYRIAKOS, M.: A type of malignant fibrous histiocytoma. Cancer 29 : 961-976, 1972. MACKENZIE, D.H.: Fibroma: a dangerous diagnosis. A review of 205 cases of fibrosarcoma of soft tissues. Br. J. Surg. 51 : 607-612, 1964. MACRENZIE, D.H.: Synovial sarcoms. A review of 58 cases. Cancer 19: 169-180, 1966. MACRENZIE, D.H. : The Differential Diagnosis of Fibroblastic Disorders. Blackwell, Oxford and Edinburgh, 1970. PRITCRARD. D.J., SOULE, E.H., TAYLOR, W.F., and IVINS, J.C.: Fibrosarcoma. A clinicopathologic and statistical study of 199 tumors of the soft tissues of the extremities and trunk. Cancer 33: 888-897, 1974. SOULE, E.H. and ENRIQUEZ, P. : Atypical fibrous histiocytoma, malignant fibrous histiocytoma, malignant histiocytoma, and epithelioid sarcoma. A comparative study of 65 tumors. Cancer 30: 128-143, 1972. SOULE, E.H. and PRITCHARD, D.J.: Fibrosarcoma in infants and children. A review of 110 cases. Cancer 40: 1711-1721, 1977. STOUT, A.P.: STOUT, A.P.: WEISS, S.W. and ENZINQER, F.M.: Malignant fibrous histiocytoma. An analysis of 200 caaes. Cancer 41: 2260-2266. 1978.
Fibroxanthosarcoma of the soft tissues.
Fibrosarcoma. Fibrosarcoma in infants and children.
The malignant tumor of fibroblasts. Cancer 1 : 30-63, 1948. Cancer 15: 1028-1040, 1962.





























