Embed Size (px)
Citation preview

Infantile Digital Fibromatosis
Identification of Actin Filaments in Cytoplasmic Inclusions by Heavy Meromyosin Binding
HlROSHl IWASAKI, MD,' MASAHIRO KIKUCHI, MD,' IWAO OHTSUKI, MD,t MUNETOMO ENJOJI, MD,* NORIKO SUENAGA, PHD,t AND RYOlCHl MORI, MDS
Cell cultures were carried out from four patients with infantile digital fibromatosis. The cultured cells, which contained cytoplasmic inclusions identical to those of the original tumor cells, possessed cortical bundles of microfilaments, rich network of granular endoplasmic reticulum, and well-developed Golgi complex. To demonstrate the distribution of actin filaments in the cultured cells, the heavy meromyosin- binding method was applied to saponin-treated cells from one of the four patients. The microfilaments constituting the inclusions as well as the cortical bundles were decorated with heavy meromyosin, presenting the "arrowhead complexes" specific for actin filaments. The inclusion may represent ab- normal contraction of actin filaments in the cytoplasm of myofibroblasts.
Cancer: 52: 1653- 166 I, 1983.
NFANTILE DIGITAL FIBROMATOSIS (recurring digital I fibrous tumors of childhood) is a rare fibrous tumor arising on the fingers or toes of infants and young chil- dren.'-20 The tumor may recur after excision, but it never metastasizes, and spontaneous regression also has been reported.'.' '*'6-20 A distinct morphologic feature is a round eosinophilic inclusion in the cytoplasm of tu- mor cells. However, there is much confusion concerning the exact origin of the inclusions and the true nature of the
pointed out that the tumor consisted of myofibroblasts that contained inclusions probably representing abnormal accumula- tion of cytoplasmic contractile proteins. The inclusions had been connected with viral etiology of the tumor by some in~estigators,~.~*'-'' but the results of our previous
Recently Bhawan et al." and
From the 'Department of Pathology, Fukuoka University School of Medicine, and the ?Department of Pharmacology, the $Department of Pathology, and the §Department of Virology, Faculty of Medicine, Kyushu University.
Supported by grants-in-aid for Scientific Research and Cancer Re- search from the Ministry of Education, Science and Culture, and from the Fukuoka Cancer Association, Japan.
Address for reprints: M. Kikuchi, Professor, Department of Pa- thology, Fukuoka University School of Medicine, 34 Nanakuma, Jonan-ku, Fukuoka 814-01, Japan.
The authors thank H. Ishikawa, MD, Associate Professor of Anat- omy, Faculty of Medicine, University ofTokyo, for his valuable advice in electron microscopic studies, and N. Shinohara, MD, Department of Orthopedics, National Fukuoka Central Hospital, and Dr. A. Mat- suzaki, Department of Orthopedics, Fukuoka University School of Medicine, for supplying the surgical materials.
Accepted for publication August I I , 1982.
virologic study indicated a nonviral origin of the inclu- s i o n ~ . ' ~ ' ' ~
In this report, electron microscopic cytochemistry was applied to the cultured cells to provide definitive evi- dence that the inclusions are composed chiefly of actin filaments aggregated in the cytoplasm of myofibroblasts.
Materials and Methods
The clinical data in three of the four cases studied were reported elsewhere." In the fourth case, a 2-month- old female infant was found to have a small reddish nodule on the dorsal surface of the middle phalanx of her left fifth finger. The lesion gradually enlarged to 1 .O cm in diameter and was removed at the age of 10 months. Two months later, a recurrent nodule devel- oped at the margin of the skin graft, and a similar nodule appeared on the left fourth finger. Both lesions were removed at the age of 14 months. After a follow-up of 20 months, there has been no further recurrence.
Surgical Specimens
The removed tumor tissues immediately divided into three parts were processed for cell cultures, and light and electron microscopy as described previously. ".I9
Cell Cultures
The primary cultures were carried out by trypsin digestion or explant technique. The former method was
0008-543X/83/1101/1653 $1.25 0 American Cancer Society
1653
1654 CANCER November I 1983 Vol. 5 2
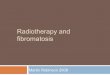
FIG. I , Typical histologic appearance of infantile digital fibroma- tosis. The tumor is composed of fibroblast-like cells having cytoplasmic inclusions (arrows) H & E, X830).
described elsewhere.”,” For the latter, minced frag- ments of tumor tissues were explanted in the plasma clots placed on the bottom of glass culture flasks. Culture medium employed consisted of Eagle’s MEM (GIBCO, Grand Island, NY) or DM-170 (Kyokuto Pharmaceu- tical Industries, Tokyo, Japan) supplemented with 10% fetal bovine serum (GIBCO). Cells were grown at 37°C in a humidified atmosphere containing 5% COz in air, and cultures were fed twice a week. Subconfluent cell layers were obtained within 3 weeks, then subcultured by treatment with the mixture of 0.1% trypsin and 0.02% EDTA. After that, serial subcultures were done every 4 to 5 days at 1.2 dilution.
Treutment of Cultured Cells for Heavy Meromyosin Binding
Myosin was purified from rabbit skeletal muscle by the method of Szent-Gyorgyi: Heavy meromyosin (HMM) was prepared by tryptic digestion of myosin.21 Cultured cells from one patient (the fourth case) were used for HMM binding.
The cells at the 2nd to 4th passage, grown in 25 cm2 plastic flasks (Corning Glass Works, Corning, NY), were made permeable with saponin by the method of Ohtsuki et ul.” The cell layers were treated with 2 ml of saponin (ICN Pharmaceuticals, Inc., Life Sciences Group, Cleve- land, OH) at a concentration of 0.1 mg/ml in Dulbecco’s phosphate buffered saline (PBS) containing 2 mM MgClz for 10 minutes at room temperature. After wash- ing with PBS, the cell layers were incubated with 2 ml of HMM (2 mg/ml) in PBS containing 1 mM diisopro- pyl fluorophosphate (Sigma, St. Lous, MO) for 8 hours at 2°C.
Electron Microscopy
The cells treated with HMM were fixed in 2% glu- taraldehyde in 0.1 M cacodylate buffer for 15 minutes and postfixed with 1% osmium tetroxide for 30 minutes. After a distilled water rinse, samples were stained c w bloc with 1% uranyl acetate for 30 minutes, dehydrated in a graded series of ethanol, and embedded in Epon 8 12. Thin sections were cut parallel to the growth substrate, stained with uranyl acetate and lead citrate, and ex- amined with a JEM IOOCX electron microscope (JEOL, Tokyo, Japan). Untreated cells and portions of fresh surgical specimens were processed in a similar way.
Results
Morphologic Findings of’ Surgical Specimens
The light and electron microscopic findings in the surgical specimens were similar to those described pre- viously. The tumor consisted of fibroblast-like cells embedded in an abundant collagenous matrix. In the cytoplasm of many tumor cells were round, eosinophilic inclusions measuring 1.5 to 10 pm in diameter (Fig. I ) . The ultrastructural study demonstrated that the tumors were made up of myofibroblasts characterized by well- developed granular endoplasmic reticulum, prominent Golgi complex, and bundles of microfilaments with in- terspersed dense patches (Fig. 2A). The intracytoplasmic inclusions were composed chiefly of closely packed mi- crofilaments which measured 5 to 7 nm in diameter (Fig. 2B).
Morphology of Cultured Cells
The cultured cells were arranged in monolayers with parallel orientation, resembling fibroblasts in appear- ance (Fig. 3A). Many cells had intracytoplasmic inclu- sions that were essentially identical to those in the sur- gical specimens (Figs. 3B, 4A and 4B). In the cortex of the cultured cells, the microfilaments were arranged in closely spaced parallel bundles, which were often fused with the inclusions (Fig. 4A). The inclusions were not uniform in size, ranging 1 .O to 10 pm in diameter. They were composed chiefly of randomly ravelled microfila- ments measuring 5 to 7 nm in diameter (Fig. 4B). The interstices among the microfilaments were occupied by a fine granular matrix of low density. Dense patches resembling those of the smooth muscle cells were often noted in the inclusions as well as in the bundles of mi- crofilaments. Small membrane-bound vesicles probably derived from entrapped cell organelles were found in the larger inclusions. The 10-nm filaments were absent in

No. 9 INFANTILE DIGITAL FIBROMATOSIS - Iwasaki rt al. 1655
FIGS. 2A AND 2B. (A) A cytoplasmic inclusion is noticed in a myofibroblast characterized by well-developed granular endoplasmic reticulum and bundles of microfilaments with interspersed dense patches. The inclusion is connected with the bundles of microfilaments (X6400). (B) Portion of an inclusion composed chiefly of closely packed microfilaments measuring 5-7 nm in diameter. Notice dense patches in the periphery of the inclusion (X52.400).
the smaller inclusions, while they were sometimes abun- dant in the periphery of the larger inclusions.
The cortical microfilament bundles were particularly plentiful in the region of cell-substrate contact. These bundles often extended into the cell processes and con- nected with cell membrane through the dense patches, where extracellular matrix fibrils attached also ( F i g . 5B). Many caveolae and coated vesicles in various stages of
development were found to be adjacent to the cell mem- brane of the free surface (Figs. 4A and SA). The deeper region of the cytoplasm contained well-developed gran- ular endoplasmic reticulum, numerous polysomes, prominent Golgi complex, and moderate number of mitochondria. The 10-nm filaments as well as scattered microtubules were also found in the deeper region of the cytoplasm.

I656 CANCER November 1 I983 Vol. 52
FIGS. 3A A N D 3B. Cells cultured from infantile digital fibromatosis. (A) Phase contrast photomicrograph showing cultured cells arranged in monolayer with parallel orientation ( X 160). (B) Cultured cells hav- ing cytoplasmic inclusions (arrows) resembling those in the surgical materials (H & E, X824).
IdentiJcation of’Acfin Filaments by HMM Binding
The inclusions and bundles of microfilaments ap- peared well preserved and unaffected by saponin treat- ment (Fig. 6). The microfilaments in the bundles, which were often connected with inclusions, were decorated with HMM, displaying the characteristic arrowhead complexes (“decorated filaments”). The decorated mi- crofilaments were recognized by the increased thickness (20-25 nm in diameter), electron density, and fuzzy appearance. They were easily distinguished from the 10- nm filaments that did not bind HMM (Figs. 6 and 7). The polarity of longitudinally sectioned filaments could be determined by the directions of arrowheads, except for in areas of very close packing. Within the bundles,
the microfilaments were arranged with dual direction- ality as shown in the stress fibers in some cultured
The microfilaments in the inclusions also bound HMM and proved to be actin filaments, although they were tangled each other, lying in haphazard arrangement without uniform polarity (Fig. 7). Arrowhead complexes were most clearly demonstrated in the periphery of the inclusions; some decorated filaments pointed toward the inclusions, while others pointed away from them (Figs. 7 and 8).
Discussion
Myofibroblasts (modified fibroblasts) currently have been found in a variety of neoplastic and non-neoplastic lesion^.".'^ In infantile digital fibromatosis, most tumor cells exhibit the feature of myofibroblasts: bundles of microfilaments, rich network of granular endoplasmic reticulum, and well-developed Golgi complex. ”,” The cultured cells in this study presented essentially the same morphologic features as those of the myofibroblasts in the surgical specimens. The cytoplasmic inclusions char- acteristic of infantile digital fibromatosis have been shown to be composed of the same material as the bun- dles of microfilaments, because they are often contin- uous and share the dense patches as well as the size of filaments.” Although the microfilaments constituting the inclusions and bundles have been thought to be actin filaments, no conclusive evidence has ever been ob- tai ned. I ’- l 9
The in sifu distribution of actin filaments in non- muscle cells was first demonstrated by the elegant ex- periments of lshikawa et ul.23,24 Their technique was based on Huxley’s demonstration that isolated F-actin forms arrowhead complexes (“decorated filaments”) when treated with HMM.” This reaction is considered to be specific for actin, since HMM do not decorate other filamentous structures in cell^.^"^^) Recently Oht- suki et al.22 developed a saponin-treatment technique useful for macromolecular tracers such as HMM pen- etrating into cells without severe destruction of intra- cellular structures. In the current study, saponin-treated cells were incubated with HMM, and the microfilaments constituting the inclusions were identified as actin fila- ments by characteristic arrowhead complexes. The mi- crofilaments arranged in bundles, identical to stress fi- bers, also formed arrowhead complexes and proved to be actin filaments.
The intracellular filamentous masses resembling the inclusions described herein were reported in the cultured cartilage cells and fibroblasts treated with ATP24.3’ or cytochalasin.32 These filamentous masses composed of

No. 9 INFANTILE DIGITAL FIBROMATOSIS - Iwasaki et af. I657
FIGS. 4A AND 4B. Electron micrographs of a thin section of flat-embedded cells cut parallel to the growth substrate. (A) Cultured cell at the top contains an inclusion connected with a bundle of microfilaments with interspersed dense patches. Well-developed granular endoplasmic reticulum is present in a cell in the lower portion (X8600). (B) Higher magnification of the inclusion in Fig. 4A. Its morphology is essentially identical with that of the surgical materials (see Fig. 2B). The continuity of the inclusion with the microfilament bundle is evident (X52.400).

1658 CANCER November I 1983 VOl. 52
FIGS. 5A A N D 5B. Distribution of microfilaments in flatt-embedded cells. (A) Thin-section at the level of free sides of a cultured cell. Microfilament bundle is located in the cell cortex. whereas 10 nm filaments are present in the deeper region of the cytoplasm. Notice many caveolae and some coated vesicles near t o t h e cell surface (X41,OOO). (B) Thin section made ad- jacent to the adhesive surface of cul- tured cells. showing particularly abun- dant microfilaments arranged in par- allel bundles with interspersed dense patches. These bundles are often con- nected with cell membrane through the dense patches, where extracellular matrix fibrils attach also ( X 10.000).
tightly packed microfilaments measuring 5 to 7 nm in and aggregation pattern corresponding exactly to the diameter were considered to represent a contracted form phases of the contraction-relaxation cycle. The micro- of the actin filament network in the cell cortex. filament bundles transform themselves into feltwork
Nagai el al.33 have noted that microfilaments (actin (“skein body”) in the shortening phase of maximal con- filaments) of the slime mould change their morphology traction, while the microfilaments regain their parallel
T
FIG. 6. Incubation of the saponin-treated cells with rabbit HMM. Arrowhead complexes are noted along the microfilaments within bundles and in the periphery of inclusion. The decorated actin filaments are recognized by the increased thickness. electron density. and fuzzy appearance. The 10 nm filaments remain unlabeled (X24.500).
FIG. 7. Microfilaments constituting the cytoplasmic inclusion are decorated with HMM. presenting the arrowhead complexes specific for actin filaments. The decorated actin filaments ranging in diameter between 20 and 25 nm are easily distinguished from the intermediate filaments measuring 10 nm in diameter. The polarity of actin filaments is not uniform (arrows indicate the polarity oftilaments adjacent to them) (X52.400).


1660 CANCER November 1 1983 Vol. 52
FIG. 8. Higher magnification of the HMM-actin filament complexes formed in the periphery of cytoplasmic inclusion. Some decorated filaments pointed toward the inclusion, while others pointed away from it (The polarity ofactin filaments is indicated by adjacent arrows.) (X8 I.000).
order and bundle structures in the relaxing phase. The “skein body” in the contracting slime mould also may be comparable to the cytoplasmic inclusions of infantile digital fibromatosis. Therefore, it is reasonable to assume that the inclusions result from abnormal contraction of actin filament bundles in the myofibroblasts. Although the current study provides definitive evidence that actin filaments are major constituents of the inclusions of in- fantile digital fibromatosis, we cannot rule out the pos- sibility that the inclusions contain some additional com- ponents (proteins?), since the interstices among the actin filaments are occupied by a fine granular matrix of low density.
The nonmuscle cells have been shown to contain sev- eral types of muscle proteins in addition to actin, in- cluding myosin, tropomyosin, a-actinin, and some ac- tin-binding proteins34 such as f i l a m i ~ ~ , ~ ~ gelsolin,’6 ac- tin~gelin,~’ and f r a g m i r ~ . ~ ~ These regulatory proteins, together with local concentration of free CA++, may reg- ulate the cellular contractile mechanisms and structural organization of cytoskeletons by means of controlling the cytoplasmic actin gel-sol t ran~formation.’~-~~ This leads to another speculation that some abnormality of the regulatory proteins may be present in the tumor cells of infantile digital fibromatosis.
REFERENCES
I . Sakurane K. A case of fibroma durum multiplex on the ends of fingers and toes by an infant. Jpn J Dermutol Urol 1924; 24:92-93.
2. Reye RDK. Recurring digital fibrous tumors of childhood. Arch Puthol 1965; 80:228-23 I .
3. Pohjanpelto P. Ahlqvist J, Hurme K, Hjelt L. Recurring digital fibrous tumour of childhood: 2. Isolation of a cell transforming agent, Actu Puthol Microhiol Scund 1967; 70:297-299.
4. Shapiro L. Infantile digital fibromatosis and aponeurotic fi- broma. Arch Dermutol 1969; 99:37-42.
5 . Burry AF, Kerr JFR, Pope JH. Recurring digital fibrous tumour ofchildhood: An electron microscopic and virological study. Puthology 1970; 2:287-29 I .
6. McKenzie AW, lnnes FLF, Rack JM, Breathnach AS, Gross M . Digital fibrous swellings in children. Br J Dermutol 1970; 83:446-458.
7. Battifora H, Hines JR. Recurrent digital fibromas of childhood: An electron microscope study. Cuncer 197 1; 27: 1530-1 536.
8. Allen PW. Recurring digital fibrous tumours of childhood. Pu- thology 1972; 4:215-223.
9. Mehregan AH, Nabai H, Matthews JE. Recurring digital fibrous tumor of childhood. Arch Dermutol 1972; 106:375-378.
10. Grunnet N, Genner J, Mogensen B, Myhre-Jensen 0. Recur- ring digital fibrous tumour of childhood: Case report and survey. Actu Puthol Microbiolscund [A] 1973; 81:167-173.
I I . lwasaki H, Tsuneyoshi M, Enjoji M. Infantile digital fibro- matosis: Histopathological and electron microscopic study with a re- view of the literature. Actu Puthol Jpn 1974; 24:7 17-732.
12. Stiller D, Katenkamp D. Morphogenesis of intracytoplasmic dense (inclusion) bodies in a recurring digital fibrous tumor of child- hood. Light- and electron-microscopic investigations. Virchows Arch [Puthol Anal] 1975; 367:13-8 I .
13. Gebhart W, Jaschke E, Reichel K. Rezidivierende digitalfi- brome in kindesalter. 11. Mitteilung: Ultrastruktur. Z Huutkr 1976;
14. Beckett JH, Jacobs AH. Recurring digitial fibrous tumors of childhood: A review. Pediulrics 1977; 59:401-406.
15. Santa Cruz DJ, Reiner CB. Recurrent digital fibroma of child- hood. J Cutun Puthol 1978; 5:339-346.
16. Kohda H, Hino Y. Spontaneous regression of infantile digital fibromatosis. Nishinihon J Dermutol 1978; 40:609-6 10.
17. Bhawan J, Bacchetta C, Joris I, Majno G. A myofibroblastic tumor: Infantile digital fibroma (recurrent digital fibrous tumor of childhood). Am J Puthol 1979; 94: 19-36.
18. lwasaki H, Kikuchi M, Mori R ei 01. Infantile digital fibro- matosis: Ultrastructural, histochemical, and tissue culture observa- tions. Cuncer 1980; 46:2238-2247.
19. Miyazono J, Mori R, Takade A, lwasaki H, Kikuchi M. Cell culture of infantile digital fibromatosis. In Vitro 1980; 16:281-287.
20. Faraggiana T, Churg J, Strauss L, Voglino A. Ultrastructural histochemistry of infantile digital fibromatosis. Ultrustricct Puthol 1981; 2:241-247.
2 I . Szent-Gyorgyi AG. Meromyosins, the subunits of myosin. Arch Biochem Biophys 1953; 42:305-320.
22. Ohtsuki I, Manzi RM, Palade GE, Jamieson JD. Entry of mac- romolecular tracers into cells fixed with low concentrations of alde- hydes. Biol Celluluirc. 1978; 3 I : 1 19- 126.
23. lshikawa H,, Bischoff R, Holtzer H. Formation of arrowhead complexes with heavy meromyosin in a variety of cell types. J Cell Biol 1969; 43:312-328.
24. lshikawa H. Identification and distribution of intracellular fil- aments. In: Hatano s, lshikawa H, Sat0 H, eds. Cell Motility: Mole- cules and Organization. Tokyo: University of Tokyo Press, 1979; 4 17- 444.
25. Huxley HE. Electron microscope studies on the structure of natural and synthetic protein filaments from striated muscle. J Mol
26. Chang CM, Goldman RD. The location of actin-like fibers in cultured neuroblastoma cells as revealed by heavy meromyosin bind- ing. J Cell B i d 1973; 57:867-874.
27. Goldman RD. The use of heavy meromyosin binding as an ultrastructural cytochemical method for localizing and determining the possible functions of actin-like microfilaments in nonmuscle cells. J Hislochem Cytochem 1975; 23:529-542.
51:109-116.
B i d 1963; 7:281-308.

No. 9 INFANTILE DIGITAL FIBROMATOSIS Iwusuki d al. 1661
28. Perdue JF. The distribution. ultrastructure. and chemistry of microfilaments in cultured chick embryo fibroblasts. J Cell B i d 1973:
29. Shimada Y. Obinata T. Polarity of actin filaments at the initial stage of myofibril assembly in myogenic cells in vitro. J Cell B i d 1977:
30. B e g DA. Rodewald R. Rebhun L1. The visualization of actin filament polarity in thin section: Evidence for the uniform polarity of membrane-associated filaments. J Ci# Bid 1978: 791846-852.
3 I . Schafer-Danneel S, Weissenfels N. Licht- und elektronenmi- kroskopische untersuchungen iiber die ATP-abhangige kontraktion kultivierter fibroblasten nach glycerin-extraktion. C.v/obio/ogie 1969:
32. Miranda AF, Godman GC, Tanenbaum SW. Action of cyto- chalasin D o n cells of established lines: 11. Cortex and microfilaments. J C d Bid 1974; 62:406-423.
33. Nagai R. Yoshimoto Y, Kamiya N. Cyclic production often-
581265-283.
721777-785.
1185-98.
sion force in the plasmodia1 strand of physarum polycephalum and its relation to microfilament morphology. J Cell Sci 1978: 33:205- 225.
34. Pollard TD. Cytoplasmic contractile proteins. J Cell Biol I98 I : 9 I : 156s-165s.
35. Stossel TP. Hartwig JH. Yin HL, Davies WA. Actin-binding protein. In: Hatano S. lshikawa H, Sato H, eds. Cell Motility: Mole- cules and Organization. Tokyo: University ofTokyo Press, 1979: 189- 209.
36. Yin HL, Stossel TP. Control of cytoplasmic actin gel-sol trans- formation by gelsolin, a calciumdependent regulatory protein. Nufurc. 1979: 28 1583-586.
37. Mimura N, Asano A. Ca*+-sensitive gelation of actin filaments by a new protein factor. Nufure 1979; 282:44-48.
38. Hasegawa T, Takahashi S, Hayashi H. Hatano S. Fragmin: A calcium ion sensitive regulatory factor on the formation of actin fil- aments. Biochmnisfry 1980: 19:2677-2683.