Embed Size (px)
Citation preview
Infantile hypertrophic pyloric stenosis
浙江大学医学院附属儿童医院
江米足
Gastric outlet obstruction Hallmark is non-bilious vomiting Other symptoms include abdominal pain a
nd nausea Other signs include abdominal distention a
nd bleeding from secondary inflammation Most common cause of non-bilious vomitin
g is infantile hypertrophic pyloric stenosis Similar symptoms including pyloric atresia,
antral webs, gastric duplications, and gastric volvulus
Pyloric Stenosis
First described by Hirschsprung in 1888
Ramstedt described an operative procedure to alleviate the condition in 1907 – the procedure used to this day to treat pyloric stenosis
Harald Hirschsprung (1830-1916)
Infantile hypertrophic pyloric stenosis
Description: thickening of the pyloric portion of the st
omach causing obstruction of gastric outflow(1, 2, 4)
Also called: infantile hypertrophic pyloric stenosis hypertrophic pyloric stenosis congenital pyloric stenosis
Epidemiology age distribution almost always between
age 3-8 weeks 4-5 times more common in boys than girls highest incidence in first-born infants less common in black and Asian patients
than white patients in United States more common in Western world reported incidence 1-5 per 1,000 births(1, 2
, 4)
Causes unknown(3, 4) hypotheses include(1, 3)
abnormal neurophysiology in muscular layer including decreased nerve terminal number reduced nitrous oxide reduced number of interstitial cells of Cajal
bacteria infection, such as Helicobacter pylori genetic factors
pyloroduodenal duplication cysts as cause of neonatal gastric outlet obstruction in case report
Pathogenesis circular muscle of pylorus becomes
hypertrophied(4) pyloric sphincter fails to open causing
obstruction of gastrointestinal tract(3) stomach cannot drain, becomes fuller
and stretches until emesis occurs(3) jaundice seen in 1%-2% of infants with
hypertrophic pyloric stenosis(1, 2)
Complications
dehydration(1, 4) starvation(1) hyperbilirubinemia(1) jaundice(2)
History Chief concern (CC):
projectile nonbilious vomiting(1, 2, 3, 4) voracious appetite despite inability to tolerate feeds(1) may also present with dehydration or weight loss(1, 3, 4)
History of present illness (HPI): non-vomiting at birth followed by gradual onset of nonb
ilious vomiting until emesis follows every feeding(1, 3, 4) median duration of symptoms 10 days median age at operation 40 days
Physical:General physical only 14% infants with pyloric stenosis prese
nt with all 3 signs of "classic triad" (nonbilious projectile vomiting, visible peristalsis, palpable "olive")
signs of dehydration may include(4) acute body weight change poor mucous membrane hydration decreased capillary refill time absence of tears
Abdomen palpable mass in epigastrium or right upper
quadrant(1, 2, 3, 4) olive-sized, 1.5-2 cm may require experience and persistence to find due
to presence of gastric distention and need for calm infant with relaxed abdominal muscles
less prevalent with earlier diagnosis distended stomach may be identifiable in hy
pochondrium with visible peristalsis (1, 3)
Making the diagnosis: diagnosis suspected in infant with(1, 4)
forceful (projectile) nonbilious vomiting good appetite visible peristalsis hypochloremic alkalosis
diagnosis often confirmed by palpation of olive-shaped pyloric muscle mass but may be difficult to appreciate by inexperienced examiners and requires calm infant with relaxed abdominal muscles(1, 4)
Making the diagnosis: ultrasound is preferred imaging test to
confirm diagnosis with commonly used diagnostic criteria of(1, 3, 4) pyloric muscle thickness > 3 mm (threshold
in various studies ranges from > 2.5 mm to > 4.5 mm)
pyloric length > 15-18 mm (threshold in various studies ranges from > 14 mm to > 20 mm)
upper gastrointestinal study used with atypical presentation or when ultrasound negative(4)
Testing overview: imaging studies
ultrasound upper gastrointestinal imaging
blood tests to assess for dehydration and metabolic alkalosis serum electrolytes arterial blood gas blood glucose
Ultrasound considered test of choice for pyloric stenosis due to
absence of ionizing radiation exposure and oral contrast use (4)
ultrasound using gray-scale and color Doppler techniques by experienced sonography appears highly sensitive and specific for diagnosis of IHPS
negative ultrasound required pylorus muscle wall thickness < 3 mm pylorus canal length < 14 mm pylorus diameter < 12 mm absent or minimal vascular flow
pyloric muscle thickness ≥ 2.5 mm on ultrasound may be most sensitive finding for diagnosis of IHPS
had 98.8% sensitivity and 85% specificity
Upper gastrointestinal (UGI) study
UGI used when(4) presentation atypical (bilious emesis,
emesis present since birth, patient age extreme)
ultrasound negative
UGI study UGI may show(1, 2, 4)
prepyloric antrum failure to relax, seen as "elongation" of pyloric canal
pyloric canal outlined by string of contrast material ("string sign")
contrast material as linear tracts separated by mucosa ("double-track sign")
thickened pylorus causing external impression on gastric antrum ("shoulder sign")
ancillary findings of gastric hyperperistalsis, large volume gastric residue, delayed gastric emptying
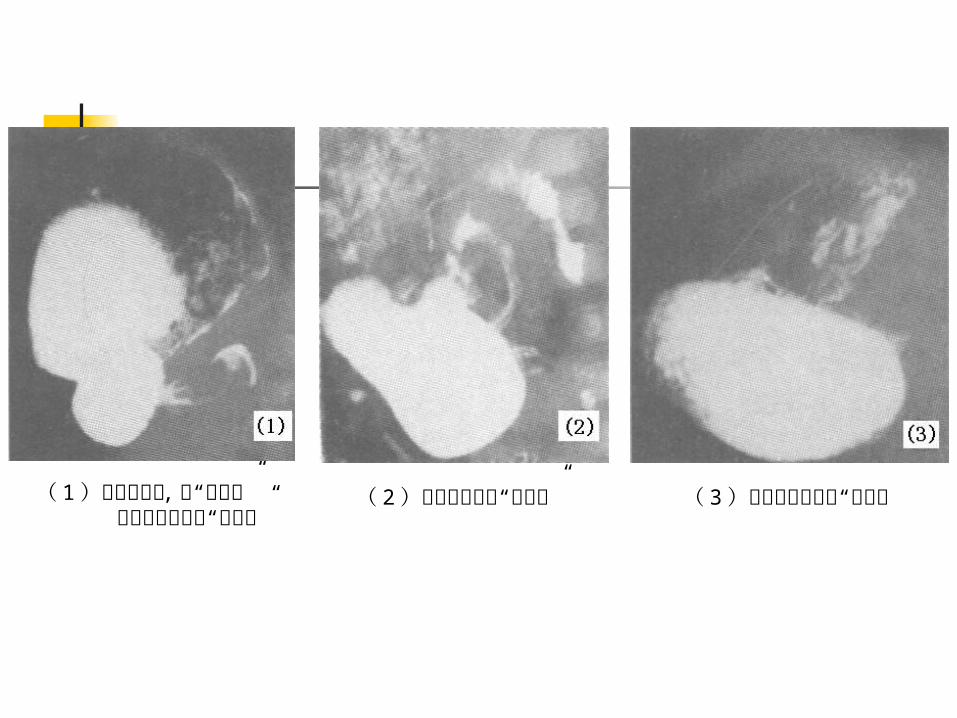
( 1 )幽门管细长 , 呈“线样征” 十二指肠球底见“蕈伞征”
( 2 )幽门管内可见“双轨征” ( 3 )胃窦部幽门前区“鸟嘴征
Treatment overview
preoperative management infant should have nothing by mouth(3) correction of dehydration and alkalosis preoperative antibiotics for prophylaxis (4)
surgery is treatment of choice pyloromyotomy (Ramstedt procedure) laparoscopic pyloromyotomy for pyloric ste
nosis associated with fewer complications,
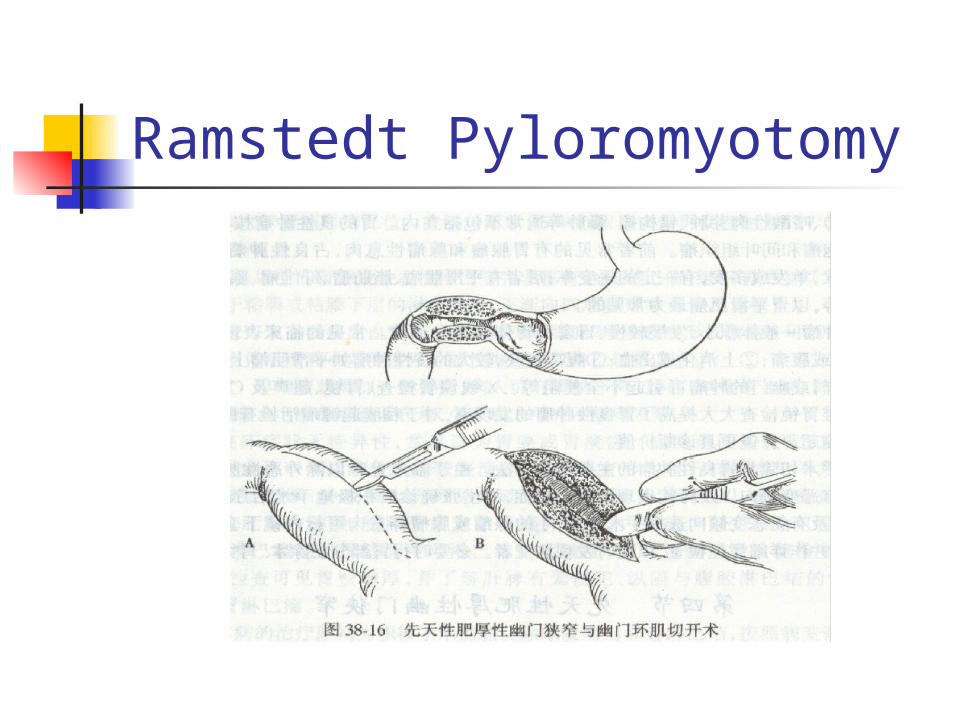
Ramstedt Pyloromyotomy
Follow-up postoperative analgesia(4) discharge following surgery(4) Underlying pyloric mass is split without cutting the
mucosa and the incision is closed Post-op vomiting occurs in ½ the patients and tho
ught to be due to edema of the pylorus Feedings can usually be initiated within 12-24 hour
s ad libitum feeding may be as safe and effective as s
tandardized feeding regimen after pyloromyotomy