Embed Size (px)
Citation preview

Infections in drug injectorsInfections in drug injectorsClostridium Clostridium species and species and
othersothers
Nick BeechingNick Beeching
Tropical & Infectious Disease UnitTropical & Infectious Disease Unit
Royal Liverpool University HospitalRoyal Liverpool University Hospital
Liverpool School of Tropical MedicineLiverpool School of Tropical Medicine
[email protected]@rlbuht.nhs.uk

Plan of talkPlan of talk
• Outline of non viral infections and sourcesOutline of non viral infections and sources• Clinical examples of technique related Clinical examples of technique related
infectionsinfections• Contaminated substance related anaerobic Contaminated substance related anaerobic
clostridial infections:clostridial infections:– TetanusTetanus– BotulismBotulism– Septic shock (Septic shock (Cl novyiCl novyi etc) etc)
• Lessons & preventionLessons & prevention

Tropical IVDU related infectionsTropical IVDU related infections
• MalariaMalaria• MelioidosisMelioidosis• American trypanosomiasis (Chagas disease)American trypanosomiasis (Chagas disease)• Leishmaniasis (Spanish IVDU)Leishmaniasis (Spanish IVDU)• SyphilisSyphilis• Hepatitis B & CHepatitis B & C• HIV HIV
All blood borne/technique relatedAll blood borne/technique related

© N Beeching
© N Beeching

Candida endophthalmitisCandida endophthalmitis
• CandidaCandida sp are sp are natural natural commensals in commensals in citrus fruitscitrus fruits
• Sudden Sudden blindnessblindness
Non viral infectionsNon viral infections
• Usually staphylococci (75%) and/or streptococci from Usually staphylococci (75%) and/or streptococci from skin skin
• NB MRSA emerging in IVDU in UKNB MRSA emerging in IVDU in UK• Anaerobes from mouthAnaerobes from mouth• Faecal organisms from groin areaFaecal organisms from groin area• Fungi from lemon juiceFungi from lemon juice• Contaminants from drugsContaminants from drugs• Anaerobes with muscle poppingAnaerobes with muscle popping
Murphy EL Murphy EL et al. J Inf Diset al. J Inf Dis 2001; 33: 35-40 2001; 33: 35-40Bassetti S, Battegay M. Bassetti S, Battegay M. InfectionInfection 2004; 32: 163-9 2004; 32: 163-9

Generalised infectionsGeneralised infections
• Bacteraemia (septicaemia)Bacteraemia (septicaemia)
• Pneumonia & lung abscessPneumonia & lung abscess
• Endocarditis (heart valves)Endocarditis (heart valves)
• Other deep abscessesOther deep abscesses
• Septic arthritisSeptic arthritis
• OsteomyelitisOsteomyelitis
• etcetc

DVT auditDVT audit
• 6 years 1996- 20016 years 1996- 2001• University Hospital AintreeUniversity Hospital Aintree• All DVTs in people aged 18-40 All DVTs in people aged 18-40
• IVDU in IVDU in 158/251 (62.9 %) of all admissions158/251 (62.9 %) of all admissions• Soft tissue infections in 60/96 (61.2%) IVDU Soft tissue infections in 60/96 (61.2%) IVDU • Bacteraemia was found in 33/80 (41.3%) of blood Bacteraemia was found in 33/80 (41.3%) of blood
cultures takencultures taken
Syed FF & Beeching NJ. Syed FF & Beeching NJ. QJ MedQJ Med 2005; 98: 139-45 2005; 98: 139-45Jenkins N et al (submitted for publication)Jenkins N et al (submitted for publication)

Anaerobic infections in Anaerobic infections in British IDU – early 2000s British IDU – early 2000s
• 2000 Necrotising fasciitis & sepsis 2000 Necrotising fasciitis & sepsis
Clostridium novyi Clostridium novyi 44/108 died44/108 died
• 2002 Botulism (2002 Botulism (Cl botulinumCl botulinum))– 2002 182002 18– 2003 82003 8– 2004 402004 40
Different Clostridial toxins have different local Different Clostridial toxins have different local and geralised efectsand geralised efects

Patient 1 40 M Window cleanerPatient 1 40 M Window cleaner
• 29 Oct 200329 Oct 2003
• 2 days L elbow 8 x 8 cm cellulitis after injecting heroin2 days L elbow 8 x 8 cm cellulitis after injecting heroin• Rx Methadone 50 ml, heroin £15 Rx Methadone 50 ml, heroin £15 (20 year career)(20 year career)• Oral penicillin, flucloxacillin, metronidazoleOral penicillin, flucloxacillin, metronidazole
• 30 Oct – Improving enough to have illicit 30 Oct – Improving enough to have illicit heroin injectionheroin injection
•

Not so good……Not so good……
• Day 7Day 7
• stiff L armstiff L arm
• cannot swallow methadonecannot swallow methadone
• agitatedagitated
• stiffness in neckstiffness in neck

Day 7Day 7
• ExaminationExamination
• arched back & neck (opisthotonus)arched back & neck (opisthotonus)• sweatingsweating• agitatedagitated• cannot open mouth or stick out tonguecannot open mouth or stick out tongue
• T36.8 P100 BP 140/76T36.8 P100 BP 140/76• No response diazepam, procyclidineNo response diazepam, procyclidine

Diagnosis: severe tetanusDiagnosis: severe tetanus
• Resuscitation – IV line, fluids, 0Resuscitation – IV line, fluids, 022
• Antibiotics – IV pen G, metronidazoleAntibiotics – IV pen G, metronidazole• Sedation – more IV diazepamSedation – more IV diazepam• Intubate & ventilateIntubate & ventilate• Antitetanus toxoid 5,750 units (IM)Antitetanus toxoid 5,750 units (IM)• as 23 x 250 u (1ml)as 23 x 250 u (1ml)• Routine debridement of woundsRoutine debridement of wounds• Transfer to intensive careTransfer to intensive care

ICU progressICU progress
• Initially settled on sedationInitially settled on sedation
• Severe arm/leg spasms within 24 hoursSevere arm/leg spasms within 24 hours
• Paralysed (atracuronium) days 2-24Paralysed (atracuronium) days 2-24– cardiac arrest on early withdrawal day 14cardiac arrest on early withdrawal day 14
• Labile BP & pulseLabile BP & pulse– Esmolol, metoprolol & clonidine triedEsmolol, metoprolol & clonidine tried

ICU continuedICU continued
• Continued spasmsContinued spasms• CSF, EEG, CT head normal• Phenytoin stopped• Magnesium infusions to keep Mg++ >4• Resulting hypocalcaemia
• Increased secretions week 3Increased secretions week 3
• Coagulase neg Staph bacteraemiaCoagulase neg Staph bacteraemia

Transfer ID Ward Day 45 Transfer ID Ward Day 45
• Still has trismus, flexed L arm, 45 degree Still has trismus, flexed L arm, 45 degree • contractures both feet, limb spasmscontractures both feet, limb spasms
– Rx DantroleneRx Dantrolene– Standing with physio day 63Standing with physio day 63
• Frozen L shoulderFrozen L shoulder• Tracheostomy removed day 70Tracheostomy removed day 70• Intermediate care days 88-100 (4 Feb)Intermediate care days 88-100 (4 Feb)• Follow-up - drug free, still a bit stiffFollow-up - drug free, still a bit stiff

Infection issuesInfection issues
• No memory of tetanus immunizationsNo memory of tetanus immunizations• Anti-tetanus IgG levels after TIG and first Anti-tetanus IgG levels after TIG and first
immunization <0.04 u/ml (Protection > 0.11u/ml) immunization <0.04 u/ml (Protection > 0.11u/ml) • Started on course of 3 immunizationsStarted on course of 3 immunizations• Remembers unusual “score” of heroin from Remembers unusual “score” of heroin from
outside dealer – drugs had been buriedoutside dealer – drugs had been buried• Tetanus not culturedTetanus not cultured• Hepatitis A & B immune, current HCV, HIV Hepatitis A & B immune, current HCV, HIV
negativenegative

Wound isolatesWound isolates
Cl novyiCl novyi
Cl histolyticumCl histolyticum
Cl baratiiCl baratii
Cl perfringensCl perfringens
All sensitive to metronidazole & penicillinAll sensitive to metronidazole & penicillin

Patient 2. 48M GardnerPatient 2. 48M Gardner
• IDU > 20 yearIDU > 20 year• Skin popper > 5 yearSkin popper > 5 year• Methadone 60 ml plus £15 heroinMethadone 60 ml plus £15 heroin• Polydrug use in pastPolydrug use in past• Shares heroin with female partner only (citric Shares heroin with female partner only (citric
acid solvent)acid solvent)• 3 suppliers of “brown” (heroin from Asia), no 3 suppliers of “brown” (heroin from Asia), no
new onesnew ones• Decrease in quality since Dec 2003Decrease in quality since Dec 2003

Jan 2004 Emergency roomJan 2004 Emergency room
• 2 days back pain2 days back pain
agitatedagitated
• 1 day lock jaw 1 day lock jaw
• Exam infected wound sitesExam infected wound sites
trismus, rigid necktrismus, rigid neck
blepharospasm & limb spasms blepharospasm & limb spasms
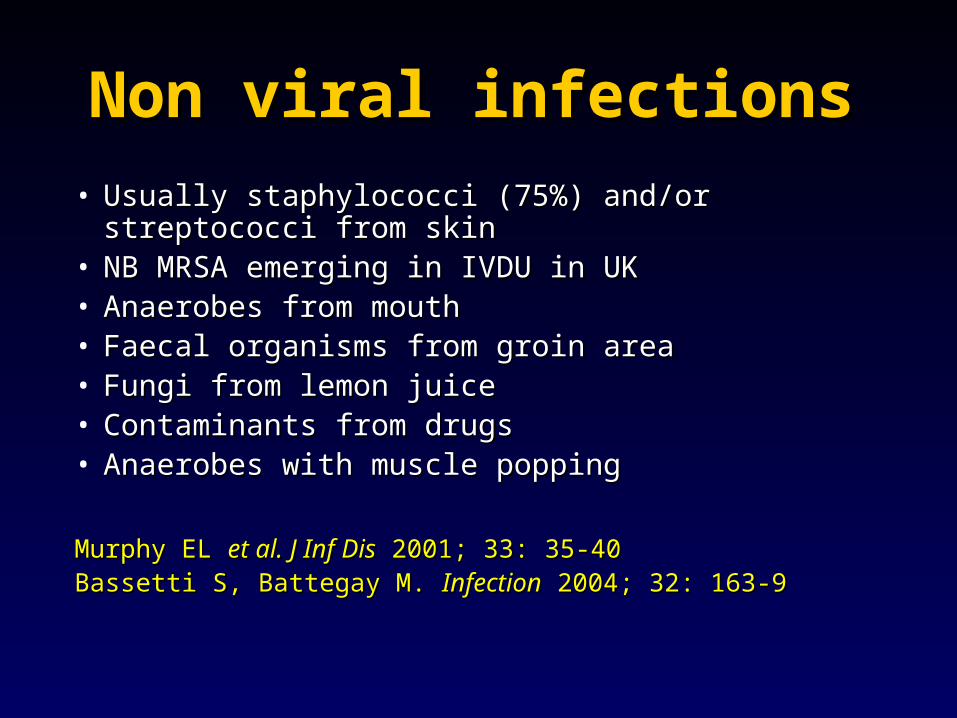
IsolatesIsolates
• Cl tetaniCl tetani• Staph aureusStaph aureus• Beta Haem Group A Beta Haem Group A
streptococcusstreptococcus• Mixed anaerobesMixed anaerobes
© N Beeching
Tetanus in IDUTetanus in IDU1876 Morphine addict Southsea (1876 Morphine addict Southsea (LancetLancet))1879 Death in Dublin (1879 Death in Dublin (BMJBMJ) ) 1950s 15% of Chicago tetanus is in IDU (100%1950s 15% of Chicago tetanus is in IDU (100% mortality) mortality) 1960s Higher incidence & mortality in New York 1960s Higher incidence & mortality in New York (muscle/skin popping)(muscle/skin popping)1990s IDU account for 55% cases in California 1990s IDU account for 55% cases in California (black tar heroin from Mexico) (black tar heroin from Mexico) 18% elsewhere in USA18% elsewhere in USA
1984-2000 2/175 cases in England1984-2000 2/175 cases in England
2002 1 in Scotland2002 1 in Scotland
MMWR 20 June 2003; 52 (SS3): 1- 7; Rushdy AA et al . Epidemiol Infect 2003;130:71-7 7 ; SCIEH Weekly 2002; 36: 19

20 cases in Feb CDR 20 cases in Feb CDR www.hpa.org.ukwww.hpa.org.uk

July 2003 – March 2004July 2003 – March 2004•22 cases notified22 cases notified•2 fatal2 fatal•13 (59%) female13 (59%) female•Median ages: Males 37, Females 32Median ages: Males 37, Females 32

Summary of tetanus outbreakSummary of tetanus outbreak
New phenomenon in the UKNew phenomenon in the UKSevere disease in most of 22 patientsSevere disease in most of 22 patientsMost patients no immunity and/or history of immunizationsMost patients no immunity and/or history of immunizationsMainly skin poppers, older and more femalesMainly skin poppers, older and more femalesNo specific drug dealer implicated, but North West No specific drug dealer implicated, but North West (Liverpool) key role(Liverpool) key roleSuggests contamination at source in UKSuggests contamination at source in UKVarious organisms isolatedVarious organisms isolatedAlmost all severe (10% death so far) and expensive to careAlmost all severe (10% death so far) and expensive to care forfor
Beeching NJ & Crowcroft NS. Beeching NJ & Crowcroft NS. BMJ BMJ 2005; 330: 208-92005; 330: 208-9

Tetanus summaryTetanus summary
• Prevention is essential in this group Prevention is essential in this group who do not always access health carewho do not always access health care
• Role of general practice, emergency Role of general practice, emergency rooms, drug dependency units in rooms, drug dependency units in immunizingimmunizing

PreventionPrevention
• Passive immunization – TIG for woundsPassive immunization – TIG for wounds
• Active immunization x 5Active immunization x 5– Maybe extend for IDU ?Maybe extend for IDU ?– Or for those >50?Or for those >50?
• Promotion of less, and safer, injecting Promotion of less, and safer, injecting

MMWRMMWR 20 June 2003; 52 (SS3): 1-7 20 June 2003; 52 (SS3): 1-7

Difficulty speaking…..Difficulty speaking…..
28 male IVDU28 male IVDU
– IVDU 7 years heroin & cocaineIVDU 7 years heroin & cocaine– insulin dependent diabeticinsulin dependent diabetic
Seen in emergency roomSeen in emergency room– IncoherentIncoherent– Assumed to be due to drug influenceAssumed to be due to drug influence

Over next 4 hoursOver next 4 hours
• Cannot open eyesCannot open eyes• DribblingDribbling• Speech worseSpeech worse• SlumpSlump
• Respiratory arrestRespiratory arrest• Ventilated in ICU for 4 weeksVentilated in ICU for 4 weeks• Non specific lesions on legs from skin Non specific lesions on legs from skin
poppingpopping

OutcomeOutcome
• Diagnosis of botulism confirmed by Diagnosis of botulism confirmed by nerve conduction & EMG studies of nerve conduction & EMG studies of upper limbupper limb
• Given antitoxin lateGiven antitoxin late
• Survived prolonged stay in ICUSurvived prolonged stay in ICU

Botulinum ToxinBotulinum ToxinProduct of anaerobicProduct of anaerobic Clostridium botulinum Clostridium botulinum
7 types, A to G7 types, A to G–Man A, B, EMan A, B, E–Ducks DDucks D–Horses CHorses C
•Commonest source is poorly preserved foodCommonest source is poorly preserved food•Lethal dose for man <1 µgLethal dose for man <1 µg•Incubation period <1->5 daysIncubation period <1->5 days•Blocks messages from nerve to muscleBlocks messages from nerve to muscle•Takes 2-4 months to recover functionTakes 2-4 months to recover function

Symptoms and signs of Symptoms and signs of botulismbotulism
•Descending paralysisDescending paralysis Affects muscles with highest innervation firstAffects muscles with highest innervation first
•Four D’sFour D’s– Diplopia: double visionDiplopia: double vision– Dysphagia: difficulty swallowingDysphagia: difficulty swallowing– Dysarthria: impaired speech enunciation (tongue, face)Dysarthria: impaired speech enunciation (tongue, face)– Dysphonia: impaired speech production (larynx)Dysphonia: impaired speech production (larynx)
•Paralysis and respiratory arrestParalysis and respiratory arrest•Dose dependentDose dependent

Practical antitoxin usePractical antitoxin use
• Test dose for hypersensitivityTest dose for hypersensitivity• Therapeutic doseTherapeutic dose• Repeat therapeutic dose if symptoms deteriorateRepeat therapeutic dose if symptoms deteriorate• Will not reverse existing pathology!Will not reverse existing pathology!• Cardiovascular and ventilatory support may be requiredCardiovascular and ventilatory support may be required
Brett MM Brett MM et al. J Med Microbiolet al. J Med Microbiol 2004; 53: 555-61 2004; 53: 555-61

ShockShock
31 female IVDU31 female IVDU
– 10 year history f injecting10 year history f injecting– Multiple injection abscessesMultiple injection abscesses
• Presents to ER with 1 day historyPresents to ER with 1 day history– UnwellUnwell– Pain in legPain in leg
• ExaminationExamination– Hypotensive shockHypotensive shock– Small boggy abscess in buttock Small boggy abscess in buttock

ProgressProgress
• Circulatory collapseCirculatory collapse• High white countHigh white count• Intubated & ventilatedIntubated & ventilated• Broad spectrum antibioticsBroad spectrum antibiotics• Dies 12 hours laterDies 12 hours later
• AutopsyAutopsy– Liquified abscess with Liquified abscess with Clostridium novyiClostridium novyi

Clostridial infectionsClostridial infections
• Gas gangreneGas gangrene• Offensive, black, rapidly progressiveOffensive, black, rapidly progressive• Complication of wound infectionsComplication of wound infections• High mortalityHigh mortality
– Cl novyiCl novyi– Cl perfringensCl perfringens– Cl histolyticumCl histolyticum

Associations in IVDUAssociations in IVDU
• Muscle poppingMuscle popping• Older patientsOlder patients• FemalesFemales• Higher purity heroinHigher purity heroin• Sharing filtersSharing filters
• Point source outbreaks and sporadicPoint source outbreaks and sporadic
McGuigan C McGuigan C et al. J Med Microbiolet al. J Med Microbiol 2002; 51: 971-7 2002; 51: 971-7Jones JA Jones JA et al.et al. J Med MicrobiolJ Med Microbiol 2002; 51: 978-84 2002; 51: 978-84

LessonsLessons
Bacterial infections are common and preventableBacterial infections are common and preventable
Safe storage of “clean” drugsSafe storage of “clean” drugsClean needles & syringesClean needles & syringesClean diluentsClean diluentsNo lemon juiceNo lemon juiceGeneral hygiene General hygiene Wash handsWash handsCleaning of skinCleaning of skinNo sharingNo sharingNo needle lickingNo needle lickingAvoid muscle poppingAvoid muscle poppingImmunisation (tetanus)Immunisation (tetanus)

Final messageFinal message
• Keep open mind in abnormal behaviour in Keep open mind in abnormal behaviour in IVDUIVDU
– BotulismBotulism (4 D’s diplopia, dysarthria, (4 D’s diplopia, dysarthria,
dysphonia, dsyphagia)dysphonia, dsyphagia)– TetanusTetanus stiff neck, arms, abdo, back, jaw stiff neck, arms, abdo, back, jaw– NovyiNovyi infection necrotising fasciitis/shock infection necrotising fasciitis/shock

AcknowledgementsAcknowledgements• Patients for permission to show their details Patients for permission to show their details • Celia Jukka Liverpool/Southport for MRSA dataCelia Jukka Liverpool/Southport for MRSA data• V Hope, F Ncube, L Desouza, M Brett, N V Hope, F Ncube, L Desouza, M Brett, N
Crowcroft, S Hahne, J McLaughlin (HPA)Crowcroft, S Hahne, J McLaughlin (HPA)• Anaerobic Reference Unit, Cardiff Anaerobic Reference Unit, Cardiff • D Goldberg, HPS for information on Scottish D Goldberg, HPS for information on Scottish
casescases• Health Protection Units in England, NHS boards in Health Protection Units in England, NHS boards in
Scotland and the National Public Health Service Scotland and the National Public Health Service for Walesfor Wales
• Clinicians and microbiologists who have notified Clinicians and microbiologists who have notified cases and provided further detailscases and provided further details