Embed Size (px)
Citation preview

Catheterization and Cardiovascular Diagnosis 21 :14&147 (1 990)
Inflation Pressure Requirements During Coronary Angioplasty
Joel K. Kahn, MD, Barry D. Rutherford, MD, David R. McConahay, MD, and Geoffrey 0. Hartzler, MD
To examine the balloon inflation pressures required for successful percutaneous trans- luminal coronary angioplasty (PTCA), the maximal inflation pressure required for 477 coronary lesions in 200 consecutive patients was determined retrospectively. When graded balloon infaltions just sufficient to achieve full expansion were used, the maximal inflation pressure used was 5 8 atm in 412 stenoses (86?'0) and was 510 atm in 463 stenoses (97%). Successful PTCA was achieved in 98% of lesions with a 3.5% major procedural complication rate. In a second group of 100 patients studied prospectively, the inflation pressure required to achieve full balloon expansion was 5 8 atm in 214 of 232 stenoses (92%) and 510 atm in 228 stenoses (98%). Thus, PTCA of coronary stenoses can be achieved with high success rates and low complication rates when graded infla- tions to pressures just sufficient to achieve full balloon expansion are performed. Most coronary stenoses will respond to pressures 58-10 atm.
Key words: coronary artery disease, myocardial ischemia, coronary artery bypass sur- gery, myocardial infarction
INTRODUCTION
The procedural goal of percutaneous transluminal cor- onary agnioplasty (PTCA) is to achieve the maximum improvement in arterial luminal diameter possible with a minimum of vessel disruption [ I ] . The optimal method- ology to achieve this goal, however, is unknown. For example, operator selection of balloon pressure and in- flation time remains enipiric. The few data available on this subject are often conflicting as to whether high pres- sure or low pressure, sudden or gradual, or short or long balloon inflations are desirable [2-51. The purpose of this study is to describe a method of balloon inflation used in more than 10,000 PTCAs over the past decade, analyze from a contemporary experience the balloon in- flation pressures commonly required during PTCA, and report the hospital outcome of this method.
METHODS
Observations on the inflation pressure requirements for successful PTCA were derived from 2 patient groups treated by 7 interventional cardiologists within our group. Data from the first patient group were obtained from a retrospective review of procedural records from 200 consecutive patients treated with PTCA in Novem- ber and December 1989. For each lesion dilated, the maximal inflation pressure used during the procedure was recorded along with success of the dilatation and any
procedural complications. A successful dilatation was considered a reduction in luminal diameter narrowing to 540% as assessed visually in 2 orthogonal views.
As the retrospective review only permitted an assess- ment of the maximal inflation pressures used during F'TCA, a group of 100 consecutive patients treated with PTCA between December 1989 and January 1990 was studied prospectively. For each lesion dilated, the pri- mary dilator recorded the balloon inflation pressure at which full balloon expansion was achieved, even if higher pressures were ultimately used. Full balloon ex- pansion was considered to be the total resolution of any waisting of the balloon from the underlying stenosis. Inability to achieve full balloon expansion was also re- corded. Procedural complications were assessed pro- spectively.
Although the inflation sequence used during the PTCA procedures was not mandated by protocol, a uni-
From the Cardiovascular Consultants, Inc., Mid America Heart Insti- tute, St. Luke's Hospital, Kansas City, Missouri.
Received April 23, 1990; revision accepted June 11, 1990
Address reprint requests to Geoffrey 0. Hartzler, MD. Cardiovascular Consultants, Inc., Medical Plaza 11-20. 4320 Wornall Road, Kansas City, MO 641 11.
Joel K. Kahn's current address is Ann Arbor Cardiology Consultants, P.C., Michigan Heart and Vascular Institute, Ann Arhor, MI.
0 1990 Wiley-Liss, Inc.

PTCA Balloon Inflation Pressures 145
form approach was used by the dilators. Each lesion was usually dilated 3 times for 45 to 90 sec per inflation. The first inflation was performed at only 2 to 3 atm. Frequent fluoroscopic monitoring of the balloon outline was per- formed to assess balloon expansion. If narrowing of the balloon profile persisted, during sequential inflations, balloon pressure was increased in 1-2 atm increments per inflation until full balloon expansion was achieved. Full balloon expansion was confirmed in orthogonal views. The maximal inflation pressure used was usually I to 2 atm higher than the pressure required to achieve full balloon expansion, although at pressures above 8-1 0 atm this additional increment was often omitted.
The 18 patients requiring >10 atm for full balloon inflation were reviewed for possible clinical or morpho- logic characteristics associated with lesion “hardness. ” Using the angiographic criteria of Ellis et al. [6], stenoses were graded as to whether they were: chronic total occlusions, at a bend point, associated with calci- fication, diffuse, of a length > 2 luminal diameters, or associated with thrombus or ulceration. Stenoses that demonstrated arterial calcification were further graded subjectively as to whether the calcification was mild, moderate, or severe. The clinical and angiographic char- acteristics of these 18 patients were compared to 36 con- trol patients undergoing PTCA of 79 stenoses without lesion ‘‘hardness. ” The control patients were selected because they represented the PTCAs preceding and fol- lowing each index case.
The 2-tailed Student t test was used for comparison of continuous variables and the chi-square test was used between categorical variables. A P value of <0.05 was considered significant.
RESULTS Retrospective Study
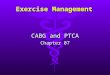
In the 200 patients undergoing PTCA, balloon dilata- tions were performed in 477 coronary lesions. Successful PTCA was achieved in 471 of 477 lesions (98%) in 195 patients (97%). Two of the 477 lesions (0.4%) failed to dilate due to an inability to achieve full balloon expan- sion despite high inflation pressures. The maximal infla- tion pressures used during PTCA in these 200 patients are shown in Figure 1. The range of maximal inflation pressure used was 2 to 21 atm. A maximal inflation pressure of 1 8 atm was used in 412 stenoses (86%) and an maximal pressure of 510 atm was used in 463 stenoses (97%).
Major procedural complications occurred in 7 patients (3.5%). There was 1 procedural death following urgent bypass surgery for a dissected left anterior descending artery (0.5%). Out of laboratory acute reclosure occurred in 3 patients (1.5%), and resulted in myocardial infarc-
130 ’ 2 0 +
: 8 0 -
g i i 0 - Q 100 - f Y0-
d 70-
50 t 4 0
117
1 2 3 4 5 6 7 6 9 10 11 12 13 14 15 16 17 18 19 20 21 Maximal Inflation Pressure (Atmospheres)
Fig. 1. Graph of the maximal inflation pressure (atmospheres) used for each of 477 coronary lesions during percutaneous transluminal coronary angioplasty in 200 consecutive patients studied retrospectively.
tion documented by serial cardiac enzymes in 2 of these patients. An additional 3 patients had an elevation of cardiac enzymes following PTCA, for a total myocardial infarction rate of 2.5%. Urgent coronary bypass surgery was performed in 4 patients (2%), including the one death.
Prospective Study In the 100 patients, 232 stenoses were dilated. The
inflation pressures required for full balloon expansion are shown in Figure 2. The range in inflation pressure was 2 to 18 atm. Full balloon expansion was observed at 5 8 atm in 214 of 232 stenoses (92%) and at 510 atm pressure in 228 of 232 stenoses (98%). During this period, there were no procedural deaths or urgent refer- rals for coronary artery bypass surgery. One out-of- laboratory acute reclosure occurred and resulted in a my- ocardial infarction. One additional patient had a procedural myocardial infarction documented by serial cardiac enzymes for an overall rate of 2%.
Angiographic Analysis
The results of the clinical and angiographic review of the 18 patients with stenoses requiring > 10 atm inflation pressure are presented in Table 1. The mean age was 64 yr (range 48 to 81) and 9 were 2 6 5 yr. Six patients had hypertension and 3 had diabetes mellitus. Chronic renal insufficiency (creatinine >1.5 mg/dl) was present in 3 patients, and 2 were on chronic hemodialysis. Calcifica- tion was present at the stenosis in 9 patients but was moderate to severe in only 3 lesions. Eleven of the stenoses were eccentric. None of the clinical or morpho- logic characteristics were significantly different than the results in the control group of patients.

146 Kahn et al.
70
62
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 Inflation Pres su re (Atmospheres)
Fig. 2. Graph of the inflation pressure (atmospheres) required to achieve full balloon expansion as determined by fluoro- scopic monitoring of the inflated catheter outline during percu- taneous transluminal coronary angioplasty. The results are shown for 232 coronary lesions in 100 consecutive patients studied prospectively.
TABLE 1. Clinical and Angiographic Features of 18 Patients With Stenoses Requiring >10 Atm During Coronary Angioplasty
Patients Control Simificance"
Clinical variables No. Mean age. years
(range) Maleifemale Hypertension Diabetes mellitus Chronic dialysis
No. of lesions Chronic total occlusion Bend point Calcification
Mild Moderate or severe
Angiographic variables
Diffuse disease Eccentric Length > 2 luminal diameters Thrombus Ulcer
18 36 64 2 I I 6 2 % 9
1315 2911 6 16 3 1 2 0
(48-81) (41-82)
18 19 0 0 1 7 9 29 6 25 3 4 7 24
I I 55 8 31 0 9 0 4
NS
NS NS NS NS
NS NS NS NS N S NS NS NS NS NS
'NS = not significant.
DISCUSSION
In the past decade PTCA has been used to treat hun- dreds of thousands of patients with widening indications, increasing success rates, and low complication rates [7]. An appreciation of the technical aspects of balloon an- gioplasty has not kept pace with these advances. While it is intuitive that the rate, duration, and maximal inflation pressure of balloon dilatation might effect primary suc-
cess, complications, or late recurrences, few studies have drawn attention to these variables.
The results of the present study provide additional in- formation regarding the methodology of successful PTCA. In this study, a protocol of gradual balloon in- flation pressures was used with the maximal inflation pressure selected to be only 1 or 2 atm higher than the pressure resulting in full balloon expansion. Graded bal- loon inflations were used empirically by Gruentzig from the time of his first procedures [2]. A preliminary report of 79 patients randomized to either gradual or rapid bal- loon inflations to maximal pressures indicated that graded inflations were associated with fewer arterial dis- sections and procedural complications [8]. The optimal maximal inflation pressure for successful PTCA is less certain. The introduction of high-pressure balloon cath- eters was correlated in one study with improved hemo- dynamic responses indicated by lower residual transle- sional gradients compared to low-pressure catheters [2]. However, inflation pressures were increased only to the point of full expansion. The procedural outcome of roil- tinely using high pressures on all lesions, regardless of their opening pressure, is unknown. A preliminary in- vestigation of the effects of incremental increases in in- flation pressures to 10 atm in 50 coronary lesions using relatively non-compliant balloon catheters suggests that additional gains in stenosis reduction occur with higher inflation pressures [9]. In contrast, our practice in over 10,000 procedures has been to limit inflation pressures to only those necessary for full balloon expansion, even if this occurs at low levels, in order to avoid applying un- necessary stress to the arterial wall. The results of this study indicate that successful dilatation can be achieved for most lesions at pressures below 8 to 10 atm, and often at 4 to 6 atm. Furthermore, this protocol is associated with low complication rates. Only a randomized study comparing a protocol such as ours to one routinely using high pressures will provide information regarding the role of high-pressure inflations.
Follow-up angiography was not performed in our study, and restenosis rates cannot be assessed. Observa- tions from other laboratories indicate that higher infla- tion pressures may have an adverse effect on intimal hyperplasia. Sarembock et al. studied the effect of bal- loon size and inflation pressure on the acute and long- term outcomes of balloon angioplasty in New Zealand White rabbits with bilateral femoral atherosclerosis [ 5 ] . Vessels exposed to high inflation pressure (10 atm) had significantly higher incidences of mural thrombus, dis- section, and medial necrosis vs low-pressure (5 atm) in- flations. Furthermore, morphometric analysis demon- strated that segments treated with high inflation pressures and large balloons demonstrated the most marked intimal hyperplasia at 28 d. In human studies,

PTCA Balloon Inflation Pressures 147
higher balloon inflation pressures have been associated with increased restenosis in some, but not all, series [10,11].
Another potential reason to avoid the routine use of high inflation pressures reflects the desire to avoid bal- loon rupture. Although balloon rupture can be unpredict- able, it most commonly occurs at inflation pressures at or above those recommended by the manufacturer. Balloon rupture is generally benign; however, on occasion seri- ous consequences can occur [ 121.
The results of this study may have implications for new balloon and non-balloon technologies under devel- opment. The primary success rates achieved with cur- rently available catheters are very high and approach 100%. Although specialty balloons permitting very high inflation pressures may be needed on rare occasions, most stenoses can be successfully dilated with pressures obtainable with current catheters. Only 0.4% of the le- sions studied retrospectively could not be dilated ade- quately despite high pressures. Several new non-balloon technologies currently under investigation, such as cor- onary excimer laser therapy and directional atherectomy, may prove to have a role for lesions not readily dilated with conventional balloon catheters, but the demand does not appear to be great.
In summary, graded balloon inflations during PTCA permit dilatation with very high success rates and low complication rates. Most coronary lesions can be dilated at inflation pressures below 10 atm. No clinical or angi- ographic variable appears to be useful in predicting stenoses not yielding to usual inflation pressures. Ran- domized studies may be warranted in the future to assess whether the routine use of high inflation pressures has any merit over pressures tailored to the response of the individual stenosis.
REFERENCES
1. Abele J: Balloon catheters and transluminal dilatation: technical considerations. AJR 135:90 1-906, 1980.
2. Meier B, Gruentzig AR, King SB, Douglas JS, Hollman J, Isch- inger T, Galan K: Higher balloon dilatation pressure in coronary angioplasty. Am Heart J 107:619-622, 1984.
3. Jain A , Demer LL, Raizner AE, Roberts R: Effect of inflation pressures on coronary angioplasty balloons. Am J Cardiol 57: 26-28. 1986.
4. Douglas JS, King SB, Roubin GS: Influence of the methodology of percutaneous transluminal coronary angioplasty on restenosis. Am J Cardiol 60:29B-33B, 1987.
5 . Sarembock IJ, LaVeau PJ, Sigal S , Timms 1, Sussman J . Hau- denschild C, Ezekowitz MD: Influence of inflation pressure and ballon size on the development of intimal hyperplasia after bal- loon angioplasty . A study in the atherosclerotic rabbit. Circula- tion 80: 1029-1040, 1989.
6. Ellis SG. Roubin GS, King SB, Douglas JS, Jr., Weintraub WS, Thomas RG. Cox WR: Angiographic and clinical predictors of acute closure after native vessel coronary angioplasty . Circulation
7. Tuzcu EM, Simpfendorfer C, Dorosti K, Franco I, Hollman J , Badwhar K, Whitlow P: Changing patterns in percutaneous trans- luminal coronary angioplasty. Am Heart J 117:1374-1377, 1989.
8. Remetz MS, Cabin HS, McConnell S , Cleman M: Gradual bal- loon inflation protocol reduces arterial damage following percu- taneous transluminal coronary angioplasty (abstr.). J Am Coll Cardiol l l : l 3 lA , 1988.
9. Lehmann KG, Le HM, Feuer JM, Atwood JE, Wenton JA: In- fluence of inflation pressure on stenosis reduction during coro- nary angioplasty (abstr.). Circulation 80:11-372, 1989.
10. Marantz T, Williams DO, Reinert S , Gewirtz H, Most AS: Pre- dictors of restenosis after successful coronary angioplasty (abstr.). Circulation 70:11-176, 1984.
11. Leimgruber PP, Roubin GS, Hollman J, Cotsonis GA, Meier B, Douglas JS, King SB, Gruentzig AR: Restenosis after successful coronary angioplasty in patients with single-vessel disease. Cir- culation 73:710-171, 1986.
12. Rothschild R, Voda J: Coronary artery dissection caused by an- gioplasty balloon rupture. Cathet Cardiovasc Diagn I9:26-29, 1990.
77:372-379, 1988.





![MICHIGAN DEPARTMENT OF COMMUNITY HEALTH (MDCH) … · coronary angioplasty [PTCA] or coronary atherectomy), 36.06, or 36.07 (Insertion of non-drug (or drug) eluting coronary artery](https://img.pdfslide.net/doc/110x75/5ecd8ab463258f0f735fc3eb/michigan-department-of-community-health-mdch-coronary-angioplasty-ptca-or.jpg)