Embed Size (px)
Citation preview

Iipoj 1
CASE REPORTS
BOJHOCAHMTETCKI1 OPErJlEJI CTPaua 81
UDC: 616.127-005.8-085-036.82
Primary percutaneous transluminal coronaryangioplasty in the acute infarction of the
right ventricle
Branko Gligic', Vjekoslav Orozovic', Siobodan Obradovic', Sinih Rusovic',Jelena Kostic" Branislav Baskotl, Dragan Dineic', Andelka Ristic·
-Andelkov'
Mililary Medical Academy, "'Clinic for Urgent Internal Medicine. 'Institute of Radiology,;'nstitule of Nuclear Medicine. Belgrade
BackgrouTld. Predilection sire for the acute myocardial ill/arclion of the right ventricle, (AMI-RV) is the upper third of the rig/II corollary artery and for this reasonsitch an infarction is followed by numerous complications, primarily by conductiondisorders and very often by suddell and rapid cardiogenic shock developme1lf.Methods. Primary percwafleolls trans/uminal coronary oll8ioplasry (PPTCA) wasperformed 011 three patiellts, ill whom the acllfe infarction of the right \'ell(ricular \Vasdiagnosed and who had been hospitalized six hours after the beginning 0/ chest pain./n all three patiellls ill(racoronary stell( was implanted. 0" the admission potiell(s hadbeen in the threatening cardiogenic shock, with the prominent chest pain and with theelevation oj ST-segmelll in V4R>2 m V. /n the course of i"ten1entioll patients wereadministered low-molecular intracoronary heparin, witli direct platelet glycoproteinlib/II/a illhibitors (abciximab), according to the established procedure applied ill suchcases. Results. The complete dilatation of the inJarcted artery lVas established with tilesigns 0/ reperfusion alld the further clinical course was completely nonnal. there wasno heart Jail//re and patients had 110 sI/bjectil'e difficulties. Conclusion. Invasiveapproach in the trealmem ofAMI-RV is justifiable. alld possibly the therapy oj choicea/these patients, providing well trained and equipped team is available.
Key words: myocardial infarction; ventricular disfunction, right;angioplasty, transluminal, percutaneous coronary;coronary vessels; stenls; platelet aggregationinhibitors; heparin, low.molecular.weight; plateletglycoprotein GpUb·lIIa complex.
Introduction
The goal of the current therapy of myocardial infarclionof the right ventricle (AMI·RV) is rapid, and if possible,complete patency achievement of the infarction artery in order to reduce the size of necro~is, establish the reperfusion ofthe affected area and at the same time prevent other possiblecomplications, and reduce mortality rdte (I, 2). The extensivenecrosis is affecting inferoposterior segment of the right ven·tricle associated with the infarction extension to the free wallof the right ventricle (RV), distal half of interventricular sepIUm. papillary muscles. valvular apparatus with cardiac con-
dUClioll system. Owing (0 these facts prognosis and earlyclinical course within the first 24 hours are quite uncertain.and the mortality rale is from 20 do 50% (3-5). Parallel wilhfibrinolytic therapy administration, there is a growing interestfor mechanical reperfusion by using primary or delayed (lifesaving or rescue) balloon dilatation (6-8).
Three patients with the diagnosed AMJ-RV associatedwilh inferoposterior infarction of the left ventricle in whomspecific treatmenl protocol and primary percutaneous transluminal coronary angioplasty (PPTCA) were applied are pressented in (his paper. On the admission. patients recived aspirin300 mg peroraly together with the combination of intracoro·
Gligic B, et aJ. Vojnosanit Preg12003; 60(1): 81-87.

CrpaHa 82 BOJHOCAHI1TETCKI1 nPErJlElI 6poj I
intracoronary low-molecular heparin (enoxaparin 20 mg) andintravenous unfracuoned heparin 5000 intravenous (Lv.) immediately before angioplasty. All patients received abciximab, glycoprotein UbJUla inhibitor 10 mg before and 10 mgafter the stent implantation into the right coronary anery. Thetherapy wall continued with enoxaparin I mglkg subcutanously (s.c.) every 12 hours and with 10 mg of abciximab inLv. infusion during the first 12 hours after the performedPPTCA.
Case reports
l. Female patient, 60 years of age. first infarction: onthe admission there was a slow atrial fibrilation with ventricular response 60/min, logetner with the signs of inferoposterior infarction of the right ventricle. Blood pressurewas 80/40 mmHg. Risk factors were smoking and the in-
creased cholesterol level. Ultrasound of the hean performedimmediately after admission showed dilated right ventricleassociated with tricuspid failure and RV pressure of 40mmHg. Three hours after the onset of AMI-RV. PPTCAand intracoronary stent implantation were performed. ECGtaken immediately after PPTCA showed the rapid resolutionof ST segment for more than 70% with the early formationof the negative T-wave (signs of the early mechanical reperfusion). Control echocardiography before discharging stillshowed dilated right ventricle and RV pressure was still 40mmHg. After the discharge clinical finding was normal andthere were no subjective difficulties during the four monthsfollow-up period.
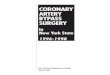
Fig. I) ECG on the admission. Fig. 2) ECG right-sidedleads. Fig. 3) Before and after the dilatation (PPTCA). Fig.4) ECG immediately after the dilatation. Fig. 5) ECG rightsided leads after the dilatation.
Fig. 1 - ECG on the admission.
,1 \1
" ,'--
Fig. 2 - ECG right-sided leads.
Fig. 3 - Before and after the dilatation (PPTCA).

...
6poj I BOJHOCAHHTETCKH nPErnEJI
~~--'ij-=-r~i---'~f--"i-~W;Jt'-W).
...,-,,,~~~ ....J:LJ.-Jl
rr~rl"~~MJA t:J· J I" L-I' (( v-., r~
"
,,_. ,,-··F-' ...- .~'F}.., .••
Fig. 4- ECG immediately afIer the dilatation.
erpaHa 83
.. ..,--r---~.- --,_...-.-....--- r...-... 1
Fig. 5 - ECG righi-sided leads afIer the dilatation.
2. Female, 69 years of age, first infarction: on the admission sinus bradycardia was 55/min, AV block grade UO
(MobilZ II), and there were signs of inferoposterior infarction of the right ventricle. Blood pressure was 80/40. Riskfactors were smoking and the increased cholesterol level.Ultrasound of the heart on the admission showed dilated
right ventricle, tricuspid regurgitation 2+ and RV pressurehigher than 30 mmHg. PPTCA was performed two hours after the infarction and due to the dissection of Lhe right coronary artery intima 3 imracoronary stems were implanted
suecessefuly. Echocardiography finding before the discharge estimated ejection fraction (EF):50%, with the inferior wall hypokinesis and normal RV. Clinical findingswere nonnal, and after being discharged from the hospitalthe paticm was without subjective difficulties within Lhethree months follow-up period.
Fig. 6) ECG on the admission. Fig. 7) ECG right-sidedleads. Fig. 8) High stenosis of the RCA. Fig. 9) Coronarography after PPTCA with 3 scents in a series.
.., "
••/J'
"
."-..J"",,' '
...
u ~•
.r~J ........---1,. r--1- ..I./\--.-.I1,.......'--.-,I I
J~ /"
Fig_ 6 - ECG on the admission.

CorpaHa 84 BOJIIOCAHHTETCKH IIPErJlEtl 6poj I
." _.,/
.'.....Jr""---' __ .._ \ r-.1 ! f r
.'
I
" , ..o
-~ ~.•I
.---H~~:. '·_""il"l.l~; ......'w.'" 1'0;,
Fig. 7 - ECG right-sided leads
Fig. 8 - High stenosis of the RCA
3. Male, 77 years of age, first infarction: on the admission, sinus rhythm, heart rale 70/min., AV block was 1°,with signs of inferopostcrior infarction of the right ventricle. Blood prcssure was 120nO. Risk faclOrs were peripheral arterial disease (intcrrniuem claudication of the lowerleg), diabetes type 2, and stable angina pectoris. Six hours
after the onset of chest pain PPTCA of the right coronaryartery was performed and intracoronary slcnt was im
planted. The patient also had the complete left anterior de-
Fig. 9 - Coronarography after PPTCA with 3 stems in a series
scendent (LAD) occlusion. Cardial ullrasound finding before the discharge showed EF 45%, akinesia of the medialand apical segment of inferior wall together with hypokinesis of inferior segment of the lateral wall and RV of normaldimensions. After being discharged, patient'S clinical findings were nonnal and without subjective diflicuhies duringthe three months follow-up period.
Fig. 10) ECG on the admission. Fig. II) Dilatation ofRCA with the stcnt implanta[ion.
"""",--y
.~~";'-Y--'Gl~·rl(~t~~rJ.l'
-J~~-i:--G--Lh ;~'/'-I,A-L-L--L-.·lJl1ft 'I . IIII ,~ .j n
~l~~J'-~,",--I't-"~(-'rLL.-L-lfl"
I'..,). "_,•• 1.~ •. ~ •...••.•1",,, ,,,,,'Fig. 10 - ECG on the admission.

6poj I BOJIIOCAIIHTETCKI1 nPErJIEJ:l
Fig. 11 - Dilatation of RCA with the sten! implamalion.
CTpana 85
Discussion
Paticllls with combined myocardial infarction of thelert and right ventricle generally require complex therapy:volume replacing. in order La increase the reduced minutevolume, fibrinolytic or PPTCA therapy in combination withanliaggrcgatory and anlieoagulam Iherapy, or delayed?TeA and imracoronary SlenL FirSl communications onsueeessrul application or PPTCA in pallellls with AMI-RVand rapid hacrnodynamic recovery of lhe patient previouslybeing in cardiogcnic shock indicated a new era of illlcrvcnlional cardiology in the treatment of these patiems (9). Agreal number of following studies dealing with the problemor PPTCA or the delayed PTCA in the treatmelll or theacute myocardial infarction cited that In about 90% of pa~
ticnts the maximum blood now (TlMI-J) through the infarcled anery was achieved after the balloon dilatation, giv~
ing much better results in comparison wiLh the common intravenous fibrinolytic therapy (10-12).
The results of an extensive randomized study GUSTOIlb by comparing erreclS or the accelerated protocol with Lissue~typc plasminogen activalor and PPTCA showed that mechanical reperfusion had reduced mortalily rale for 33% inAMJ and in serious cerebrovascular accidents during the first30 days or the hospital treatmenl. However, during the rollowing 4 monLhs the pereemage or the engaged .neryrestenosis was even 45%, which significamly diminished theefficiency or this metllOd or treatment (13).
For this reason modified PPTCA was introduced anddirect glycoprotein inhibitors (abciximab) in combinationwilh antiaggrcgation agents and low-molecular heparinwere included into the Iherapeutic protocol. A great numberof foHowing studies, as well as several randomized ones,showed thai thcrapy modified in this way and administeredwithin the first 12 hours from the onsel of AMI reduced themortality rate, myocardial reinfarction, urgent revascularization and postinfarction angina for 48% in comparisonwith the patients underwent PTeA, but without glycoprotein inhibitors (J 4, 15).
This is the first rcpon in our medical hterature or thesuccessrul lrC3lJnem or AMI-RV by PPTCA in combinationwith abciximab and low~molccular weight heparin togetherwith intracoronary Slent implanlation in all 3 patients and is inaccordance with ACClAI-IA recommendations (16). Patientswho displayed the threatening cardiogenie shock confirmedby ECG, with eonduclion disorders in the rorm or AV blockgrade IO_mo and who Came within the first 6 hours rrom theonset of AMI~RV were urgClllly selll to catheterizalion roomdue to lheir serious condition. where pacemaker wa.~ im~
plamed and urgent coronarography with PPTCA was per~
romled in the same act. Rapid clinical recovery, ST clevationregression ror more than 50% within the first 6 hours arler theintervention and the maximum increase of cardiospecific enzymes within lhe first 12 hours from the onset of AMI con~
vincingly confirmed ravourable clinical course. TIle SPECfperformed within two weeks after the intervention confirmedsueeessrul rcperrusion in the area or the inrareted artery. Onlyin one case cchocardiographic finding showed slower courseof the right ventricle recovery with persisting tricuspid failureand right ventricle pressure of 40 mmHg, bUI all other clinicalindicators were nonnal.
Our experience in lhe treallnel1l of patients with PPTCAwas also confirmed by other studies which undoubtedly upholded our altitude that invasive approach wilh urgentcoronarography was the only hope ror survival or thesc patients and Lhat it should be performed whenever possible, ifpersonnel and technical equipment are provided (17-20).
Conclusion
Patients with AMI~RV represent a subgroup with thevery high risk within the scope of inferoposlerior engagingor the left ventricle with numerous and hardly predictablecomplications resulting in high mortality ralC. Our initialexperience in the treatment of these patients by PPTCAcomplelely confirmed that this thernpcutic approach wasabsolutely justifiable in patients with cardiogenic shock, ifthere were comraindications for fibrinolytic therapy. or if

CrpaHa 86 BOJIIOCAIII1TETCKH nPErJ1Eil 6poj I
the optimal period of 6 hours after the onset of infarctionhad passed. Complete recovery of our paticnrs and theirnormal clinical course within the first three months after being discharged from Ihe hospilal showed Ihal Ihe invasive
approach in Ihe Irealmem of AMI-RV was juslifiable andthe possible therapy of choice of these paticnls. providingboth trained personnel, including a (cam of inrcrvenlionalcardiologists. and technical equipment.
REFERENCES
I. Kinch JW. Ryall rJ. Righi ventricular infarclion. NEngl J Med 1994; 330(17): 1211-7.
2. Isner 1M. Roberts We. Right ventricular infarctioncomplicating lefl venlricular infarction secondary [0
coronary heart disease. Frequency, location, associatedfindings and significance from analysis of 236necropsy p.i1licnts with acute or healed myocardialinfarclion. Am J Cardiol1978: 42(6): 885-94.
3. Del/'llalia U. The righl venlricle: analomy. physiologyand clinical imporlance. Curr Probl Cardiol 1991;16(10): 653-720.
4. COIIII IN. Gllilw Nfl. Broder MI. Limas CJ. Righiventricular infarclion. Clinical and hemodynamicfealures. Am J Cardiol1974; 33(2): 209-14.
5. Eliene Y, Boschat I, Poinson P, Cu;serix J. Beller M.Blanc Jl, el 31. Right ventricular function during theconvalescence phase of posterior primary infarclion.Arch Mal Cocur Vaiss 1985; 78(3): 396-403. (inFrench)
6. Zehellder M. Kasper IV. Km",der E, ScllOllfhaler M.Geibel A, Olchewski M. cl al. Right venLIicular
infarctions as an independent predictor of prognosisafter acute inferior myocardial infarction. N Engl JMed 1993; 328(14): 981-8.
7. Serratlo Junior CV. Ramires JA, Cesar LA, Zweier JL,Rafi M. De Luz P, et al. Prognostic signi ficanec of rightYCnLricuJar dysfunction in patients with acule inferiormyocardial infarction and right ventricularinvolvement. Clin Cadiol 1995: 18(4): 199-205.
8. Erhardt LR. Clinical and palhologieal observalions indifferent types of acute myocardial infarction. A studyof 84 patients deceased after treatment in a coronarycare unil. Ac'a Med Seand 1974; 560 Suppl: 1-78.
9. Moreyra AE. Such C. Por"ay MN. Ko,.lis JB. Rapidhemodynamic improvement in right vcnLricularinfarelion afler coronary angioplasty. Chesl 1988;94( I): : 197-9.
10. MOllahed A. Treatment of right ventricular infarction.Am Fam Physician 1999; 60(6): 1640-9.
II. Orozol'ic V. Krgovic M. Rajajlovski S. Thromboly,ietherapy and percutaneous Lransluminal coronaryangioplasty in patients with right ventricular infarctionKardiologija 2001; 22(1-2): 33-41. (in Serbian)
J2. Jorgensen B. Simonsen S. Forfa1Jg K. Endersen K,Thall/OW E. Effect of percutaneous transluminalcoronary angioplasty on exercise in paticllls with andwithout previous myocardial infarction. Am J Cardial1998: 82(9): 1030-3.
13. THE GUSTO II INVESTIGA TORS. A clinical lrialcomparing primary coronary 3ngioplasty with tissueplasminogen 3ctivator for acute myocardial infarction[edilorial]. The Global Use of Stralegies to OpenOccluded Coronary Arteries in Acute CoronarySyndromes (GUSTO lib) Angioplasly SubsludyInvesliga'ors. N Eng J Med 1997; 336(23): 1621-8.
14. Schomig A, Kasfrati A. Dirschil1ger J. Mehilli J,Schricke U. Pache J, et al. Coronary stenting plusplalelel glyeoprolein Ilbffila blockade compared withtissue plasminogen activator in acute myocardialinfarction. Stent versus Thrombolysis for OccludedCoronary Arteries in Patients with Acute MyocardialInfarcrion. Siudy Invesligators. N Engl J Med 2000;343(6): 385-9 I.
15. MOIl/alescot G. Barragall P, lVillellberg O. Ecollall P,Elhadlld S. Villa ill P. el al. Plalelel glycoproleinIIb1llIa inhibition with coronary stenting for acutemyocardial infarelion. N Engl J Med 2001; 344(25):: 1895-903.
16. Ryall rJ, AllderSOIl JL, Ammall EM, Braniff BA.Brooks Nfl, Califf RM, el al. ACCIAHA guidclines forthe management of patienlS with acute myocardial infarction: executive summary. A report of the AmericanCollege of Cardiology/American Heart AssociationTask Force on Praclice Guidelines. J Am Coli Cardiol1996; 28(5): 1328-428.
17. Comparison of invasive and conservative sLrategiesaner treatment Wilh intravenous tissue plasminogenactiwtor in acute myocardial infarction [editorial].Results of the thrombolysis in myocardial infarction(TlMl) phase 11 trial (Comillee on Management ofAcUle Myocardial Inrarclinn). TIm TlM1 Siudy Group.N Engl J Med 1989: 320(10): 618-27.
18. O'Rourke RA. Treatment of right ventricular infarction:thrombolytic therapy, coronary angioplasty or neither?J Am Coli Cardiol 1998; 32(4): 882-4.
19. Goldsteill JA. Righi hearl ischemia: palhophySiology,nalural history, and clinical management. ProgCardiovase Dis 1998; 40(4): 325-41.
20. Berger PB, Rllocco NA Jr, Ryall TJ, Jacobs AK, 211mBL, lVackers FJ. el al. Frequency and significance ofrigln vcnLricular dysfunction during inferior wall leftventricular myocardial infarction treated withIhrombolYlie lherapy (resulls from the Ihrombolysis inMyocardial Infarclion [TIMI] 1I trial). The TlMlResearch Group. Am J Cardiol 1993: 71 (13): 1148-52.
TIle paper was received on April 4, 2002.

6poj I BOJlIOCAHI1TETCKI1 nPErJlEil
Apslrakl
Gligie B, Orozovie V, Obradovie S, Rusovie S, Kostic J, Ba~kot B, Dincie D, Ristie-Andelkov A. Vojnosanit Pregl 2003; 60(1): 81-87.
PRIMARNA PERKUTANA TRANSLUMINALNA KORONARNA ANGIOPLASTIKA UAKUTNOM INFARKTU DESNE KOMORE
Uvod. Predilekeijsko mesto za nastanak akutnog interkta miokarda desne komore(AIM-DK) je gornja treeina desne koronarne arterije, zbog cega je ovakav in/arktpraeen mnogobrojnim komplikaeijama, u prvom redu poremeeajima sprovodenja icesto naglim i brzim razvojem kardiogenog ~oka. Melode. Primarna perkutanaIransluminalna koronarna angioplastika (PPTKA) uradena je kod Iri bolesnika kodkojih je dokazan akutni intarkt desne komore (AIM-DK), a koji su primljeni nabolnicko lecenje u prvih ~est sati od pocetka anginoznih bolova i sva Iri bolesnikasu dobila inlrakoronarni stent. Pri prijemu, bolesniei su ispoljavali simptomepreleeeg kardiogenog soka, sa izrazenim anginoznim bolovima i elevaeijom STsegmenta u V,R veeom od 2 mV. U loku interveneije svi su dobili niskomolekulskiheparin intrakoronarno uz direktni inhibitor glikoproteina tromboerta lib/lila(abeiksimab), prema ustaljenom protokolu koji primenjujemo u takvimslucajevima. Rezullali. Postignula je potpuna dilataeija zahvaeene arterije uzznake reperfuzije i dalji klinicki tok je prosao potpuno normalno, a u daljempracenju u sledeea tri meseea po izlasku iz balnice, bolesnici su kardijalnokompenzovani i bez ikakvih subjektivnih legoba. lakliucak: Invazivni pristuplecenju AIM-DK je opravdana i moguca terapija izbora za ove bolesnike, poduslovom da je sprovodi dobro obucen i opremljen tim.
CTp'H.87
K Ij u c n ere c i : infarkt miokarda; sree, disfunkcija desne komare;angioplastika, translumenska, perkutana, koronarna;A.A.coronariae; stentovi; antiagregaciona sredslva;heparin, niskomolekulski; glikoproteini trombocita,GPllb-lIla kompleks.
Correspondence 10: Gligic Branko; Mladen. Mitric. 4a/21, 11040 Beograd, Srbij. i Crna Gora. Tel: +381 I 1546598, Tel(work): +381 I J 663379