Embed Size (px)
Citation preview
Influence of p53 Status on Prognosis inPreoperatively Irradiated Rectal Carcinoma
Oliver Nehls, M.D.1
Bodo Klump, M.D.1
Karlheinz Holzmann, Ph.D.1
Guido Lammering, M.D.2
Franz Borchard, M.D.3
Hans-Helmut Gruenagel, M.D.4
Vera Gaco1
Michael Gregor, M.D.1
Rainer Porschen, M.D.1
1 Department of Internal Medicine I, UniversityHospital of Tubingen, Tubingen, Germany.
2 Department of Radiotherapy and Radiooncology,University Hospital of Dusseldorf, Dusseldorf, Ger-many.
3 Department of Pathology, Hospital of Aschaffen-burg, Aschaffenburg, Germany.
4 Department of Surgery, Evangelic Hospital ofDusseldorf, Dusseldorf, Germany.
Address for reprints: Prof. Dr. Rainer Porschen,Medizinische Universitatsklinik und Poliklinik, Ot-fried-Muller-Strasse 10, D-72076 Tubingen, Ger-many.
Received September 8, 1998; revision receivedMarch 4, 1999; accepted March 4, 1999.
BACKGROUND. Even when they are analogous in microscopic and macroscopic
appearance, tumors vary in their response rates to radiotherapy. Cell culture and
xenograft experiments with colorectal cell lines have demonstrated that wild-type
p53 increases radiosensitivity. Hence, the authors investigated, in a well-defined
population of patients treated at the same institution, whether p53 status was a
prognostic factor in preoperatively irradiated rectal carcinoma patients.
METHODS. The p53 status of rectal adenocarcinomas was examined immunohis-
tochemically (with monoclonal antibody DO-1) in preirradiated biopsy samples
(n 5 100) and corresponding postirradiated resected specimens (n 5 97). The
mean follow-up was 73.2 months (median, 71.3 months; range, 4.3–157 months).
Statistical analysis was performed using the SPSS program (SPSS, Chicago, IL).
RESULTS. p53 protein expression was detected in 55 of 100 biopsy samples ($5%
nuclear staining). There was essentially no difference in p53 expression between
biopsy samples and corresponding resected specimens (54 of 97 vs. 55 of 97). In
univariate analysis, p53 immunoreactivity of biopsy samples did not correlate with
age, gender, tumor location, TNM stage, pT category, pN category, or histologic
grade. Unlike clinicopathologic variables, p53 expression did not have a statisti-
cally significant association with local recurrence free, disease free, or overall
survival in either univariate (P 5 0.91, 0.18, and 0.17, respectively) or multivariate
analysis.
CONCLUSIONS. In contrast to cell line studies, this immunohistochemical study
demonstrates that p53 status is not useful as a prognostic marker in preoperatively
irradiated rectal carcinoma. Cancer 1999;85:2541– 8.
© 1999 American Cancer Society.
KEYWORDS: p53, preoperative radiotherapy, prognosis, rectal carcinoma.
Approximately 36,000 new cases of rectal carcinoma are estimatedto have presented in the United States in 1998.1 Local recurrence
rates in rectal carcinoma after curative surgical resection vary be-tween 2.6%2 and 32%,3 and a median of .15% was reported.4 There-fore, preoperative and postoperative radiotherapy with and withoutchemotherapy have been evaluated in randomized trials to improvelocal control rates and overall survival in rectal carcinoma pa-tients.5–10 Most of these trials, delivering preoperative radiotherapywith cumulative doses between 25 gray (Gy) and 40 Gy, found asignificant reduction in local recurrence,5–7 and one study also dem-onstrated a significant improvement of overall survival over surgeryalone.8 Postoperative radiotherapy as a sole adjuvant treatment mo-dality was observed to be less dose effective than preoperative radio-therapy11; however, in combination with chemotherapy, it was shownto improve significantly either both overall survival and local recur-rence9 or only time to local recurrence.10 Although radiotherapy
2541
© 1999 American Cancer Society

might result in a reduction of local recurrence rates oreven in a benefit of overall survival in rectal carci-noma, some tumors obviously do not respond to ra-diation. Otherwise, it is still unknown why cancers ofsimilar histologic type respond differently to radio-therapy.
It recently has been suggested that p53 gene mu-tations might result in increasing radioresistance ofcells.12,13 The p53 gene is the most common mutatedgene in human carcinomas,14 with mutations occur-ring in .75% of colorectal carcinomas.15 Wild-typep53 is required for mediating G1 arrest in the cell cycleafter g irradiation.13 Thus, it is believed that the DNA-repair system is given extra time to repair geneticdamage or, if the repair is not possible, to induceapoptosis.16 In contrast, p53 deficiency is suggested tocause abrogation of G1 arrest after g irradiation, whichmight result in replication of mutant DNA.16
Preclinical studies using mouse thymocytes haveshown previously that g irradiation of cells bearingwild-type p53 caused apoptosis, whereas p53 deficientcells were radioresistant.17 In colorectal cell models, italso has been observed that wild-type p53 increasesradiosensitivity in vitro18 and/or in vivo,18,19 which hasbeen contradicted by others, however.20,21 Further-more, a clinical study has recently observed that neg-ative p53 immunostaining was associated with an en-hancement of apoptotic cell death after g irradiationin rectal carcinoma.22
Wild-type p53 protein has a very short half-lifeTherefore, it is almost undetectable with immunohis-tochemistry,23 whereas the half-life of mutant p53 isincreased by conformational changes,24 permittingimmunohistochemical detection of the stabilized p53protein in the nucleus of the cell.25 The aim of thecurrent study was to determine whether p53 immu-noreactivity of pretreatment biopsy samples is a prog-nostic factor in preoperatively irradiated patients withrectal carcinoma.
MATERIALS AND METHODSPatients and Tissue SamplesThis study included 100 patients with preoperativelyirradiated adenocarcinomas of the rectum undergoingcurative surgical resection at the Department of Sur-gery, Evangelic Hospital of Dusseldorf, Germany, be-tween January, 1981 and December, 1988. Of the 151consecutive rectal tumors originally identified, 51 pa-tients (21 males and 30 females) were excluded, 47patients on the basis of missing biopsy samples (tu-mors were diagnosed in other hospitals) and 4 pa-tients because of perioperative death. PostoperativeTNM stage distribution of excluded tumors for StagesI, II, and III was 57%, 10%, and 33%, respectively.
Of the 100 study patients, 74 patients underwentanterior resection, and 26 patients underwent abdom-inoperineal excision of the rectum. At this institution,all patients with clinical resectable rectal carcinomareceived routinely preoperative radiotherapy, regard-less of clinical tumor stage. The radiation doses (Co-balt-60 units) given were 30 Gy (2-Gy fractions) over15 days followed by surgery with a median interval of14 days (range, 3– 85 days). Prior to radiation, one ortwo biopsies were taken from every tumor. In addi-tion, in 97 of the 100 patients, corresponding resectedspecimens were available, whereas postirradiated tis-sue blocks were missing in 3 patients. The biopsy andresected specimens from the patients were fixed informalin and embedded in paraffin. Before immuno-histochemical examination, one section from each tu-mor block was stained with hematoxylin and eosin toidentify the tumor tissue.
The mean age of the study patients was 63.7 years(range, 38 – 84 years). There were 46 males and 54females. Follow-up data were obtained from thecharts of the patients and the local tumor register.Up-to-date information on survival or death wasgained from the local tumor register, the proper reg-istration offices, the family doctors of the patients, orthe patients themselves. The mean follow-up was 73.2months (median, 71.3 months; range, 4.3–157months). Apart from 2 patients who were lost duringfollow-up after 30.2 months and 37.1 months, livingpatients were followed for at least 5 years. Patientswho died of causes unrelated to rectal carcinoma andthose who were lost during follow-up were treated ascensored events.
Sections were reevaluated by an experienced gas-trointestinal pathologist (F.B.). Pathologic diagnosisand classification of variables were performed accord-ing to the TNM staging system26 and the World HealthOrganization grading system.27 Postoperative TNMstage distribution of resected tumors for Stage I(T1–T2 N0 M0), Stage II (T3–T4 N0 M0), and Stage III(T1–T4 N1–N3 M0) was 57%, 6%, and 37%, respec-tively. The numbers of lesions classified as pT1, pT2,pT3, and pT4 were 12, 72, 14, and 2, respectively.Sixty-three tumors were classified as category pN0; 35were classified as category pN1, and 2 were classifiedas category pN2. One tumor was graded Grade 1, welldifferentiated; 81 tumors were graded Grade 2, mod-erately differentiated; and 19 tumors were gradedGrade 3, poorly differentiated. For statistical analyses,patients were divided into groups with sufficient sizesas follows: TNM Stage I versus Stages II–III; categorypT1/2 versus pT3/4; category pN0 versus pN1/2; his-tologic Grade 1–2 versus Grade 3.
2542 CANCER June 15, 1999 / Volume 85 / Number 12

ImmunohistochemistryParaffin sections (5 mm) of preirradiated biopsy sam-ples (n 5 100) and postirradiated resection specimens(n 5 97) were stained using the avidin-biotin peroxi-dase complex method. In brief, sections were dewaxedin xylene twice for 10 minutes each, rehydrated ingraded alcohols, and immersed in 3% hydrogen per-oxide for 10 minutes to block endogenous peroxidaseactivity. For antigen retrieval, microwave pretreat-ment in citrate buffer, pH 6.0, was performed threetimes for 5 minutes each at 780 Watts. The sectionswere then incubated in a 1:20 dilution of normal horseserum (Vector Laboratories, Burlingame, CA) for 15minutes to block nonspecific background staining.The slides were incubated consecutively with the pri-mary antibody DO-1 (Oncogene Science, Cambridge,MA), a monoclonal antibody that recognizes wild-typeas well as mutant forms of p53.28 The DO-1 antibodywas used at a dilution of 1:50 for 1 hour, followed byincubation at a 1:200 dilution with biotinylated anti-mouse immunoglobulin G-horse serum (Vector Labo-ratories) for 30 minutes and an avidin-biotinylatedperoxidase complex (Vector Laboratories) for 1 hour.Peroxidase staining was performed for 10 minutes us-ing a solution of 3-39-diaminobenzidine tetrahydro-chloride (DAB) in Tris-HCl, pH 7.6, containing 0.03%hydrogen peroxide. The sections were counterstainedwith hematoxylin and mounted. Incubations wereperformed at room temperature, and slides werewashed twice between incubations with Tris-bufferedsaline, pH 7.4. Sections of colon tumors with high p53expression were used as positive controls. Negativecontrols were performed by substituting phosphate-buffered saline for primary antibody.
All slides were evaluated semiquantitatively andindependently by two authors (O.N. and B.K.). Sec-tions that were categorized discrepantly were reas-sessed together with a third author (R.P.) to reach aconsensus. Immunoreactivity was classified from 2 to111, in accordance with the percentage of tumorcells stained. Slides were categorized as follows: 2,,5% nuclear staining; 1, 5–25%; 11; 25–50%; 111,.50%. Staining intensity was graded qualitatively as2, not detectable; 1, weak; 11, moderate, and 111,strong. The intensity was referred relative to corre-sponding positive controls.
Statistical AnalysisStatistical analysis was performed using SPSS for Win-dows 7.5 (SPSS, Inc., Chicago, IL). Possible associa-tions between p53 status and clinicopathologic vari-ables were analyzed by using the chi-square test.Survival was measured from the date of operation to
the date of last follow-up or death. Survival rates werecalculated by using the Kaplan–Meier method30 andwere tested for significance by using the log-rank test.To determine independent prognostic factors for sur-vival, multivariate analysis was calculated with theCox regression model. Statistical significance was con-sidered as P , 0.05.
RESULTSIn pretreatment biopsy samples, nuclear p53 expres-sion of tumor cells was detected in 55 of 100 speci-mens. Distribution for p53 immunoreactivity was 2,45%; 1, 3%; 11, 12%; and 111, 40%. Comparisons ofpreirradiated biopsy samples with corresponding post-irradiated resected specimens revealed nearly no dif-ference in the classification of sections (positive, 54 of97 vs. 55 of 97). When comparing p53 expression inequivalent biopsy and resected specimens of the samepatients, both were classified positive in 49 of 97 pa-tients and negative in 37 of 97 patients, whereas bi-opsy samples in 5 of 97 patients were evaluated aspositive, and fitting resected specimens were evalu-ated as negative. Conversely, biopsy samples in 6 of 97patients were classified as negative, and fitting re-sected specimens were classified as positive.
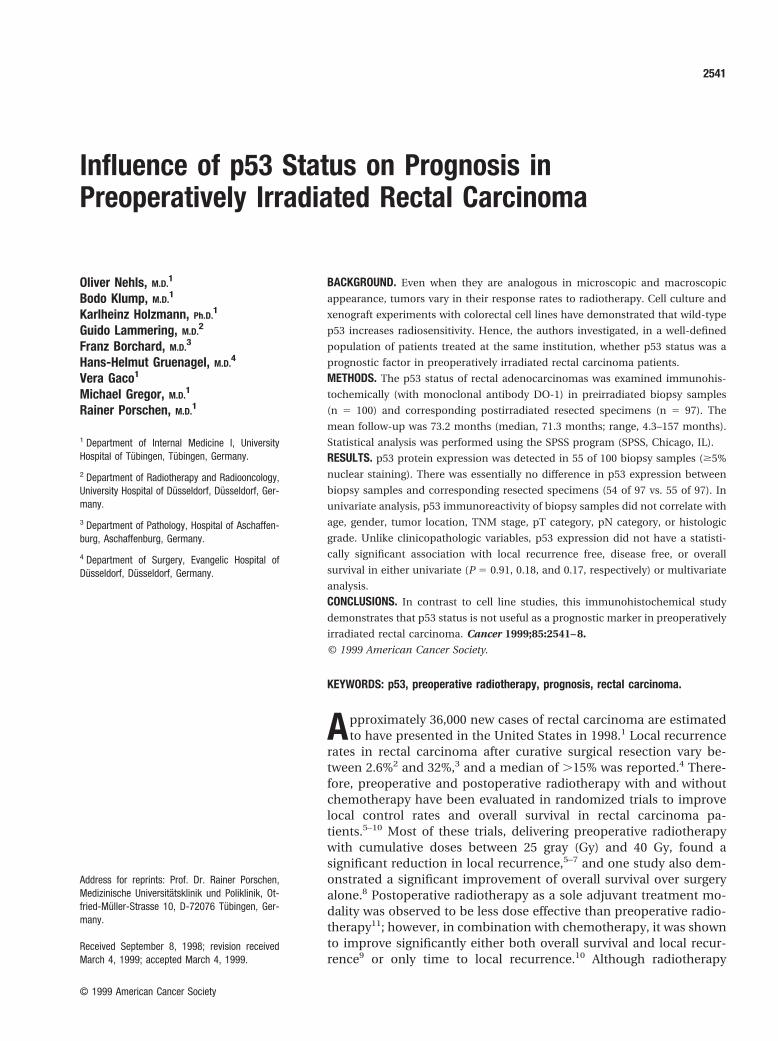
Histologically, normal rectal mucosa and stromalcells, which were used as intratumor controls, showedno immunoreactivity for the p53 antigen. In nearly allbiopsy sections, only nuclear staining was detected,whereas, in three biopsies, cytoplasmic staining alsowas observed. The staining pattern was quite variable,with some tumors showing generalized p53-positivenuclei throughout the tumor, whereas others pre-sented only with focal staining. Differences in stainingpatterns between biopsy specimens and correspond-ing resected specimens were observed, with someposttreatment specimens showing fibrosis and withonly small numbers of tumor cells stained, which werenever noted in biopsy samples. In staining intensity,pretreatment specimens and corresponding posttreat-ment specimens were classified identically in 70 of 97sections (72%; example shown in Fig. 1), whereas 16 of97 sections (17%) showed a difference of only onegrade, and 11 of 97 sections (11%) showed a differenceof two or more grades. Thus, posttreatment stainingintensity was evaluated in 9 specimens with a differ-ence of one grade greater and in 7 samples with adifference of two or three grades greater comparedwith corresponding pretreatment slides. In contrast, 7posttreatment slides were classified qualitatively witha difference of one grade less and 4 resected speci-mens were classified qualitatively with a difference oftwo grades less compared with corresponding biopsysamples.
p53 Status and Radiotherapy/Nehls et al. 2543
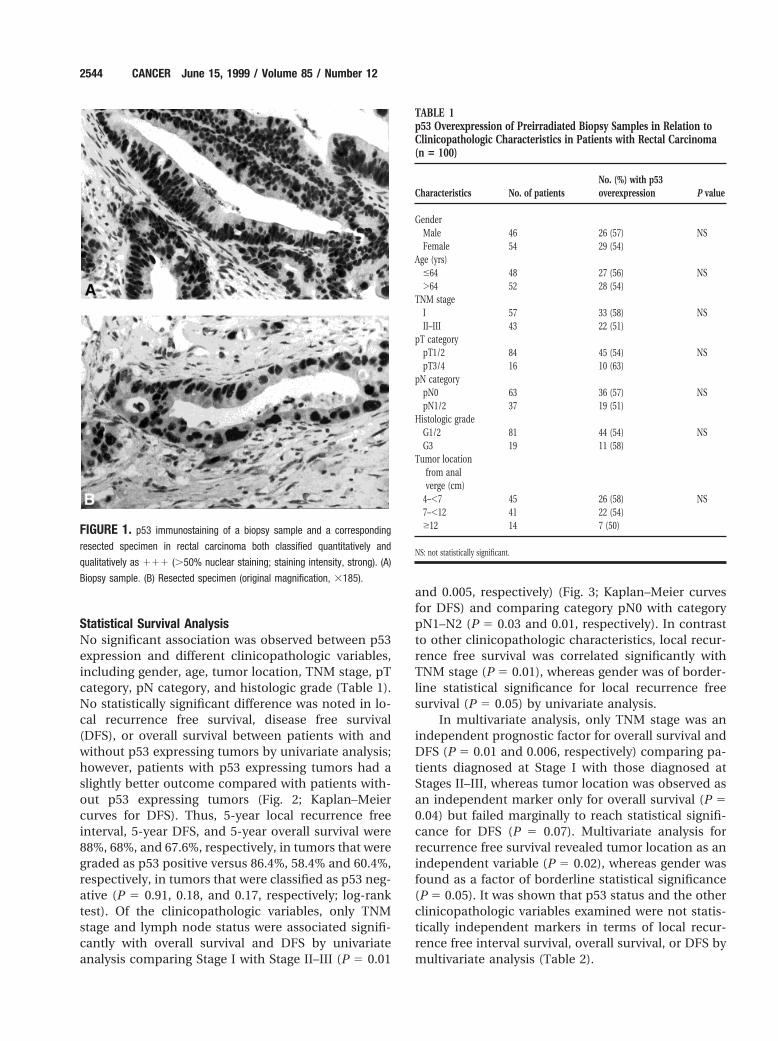
Statistical Survival AnalysisNo significant association was observed between p53expression and different clinicopathologic variables,including gender, age, tumor location, TNM stage, pTcategory, pN category, and histologic grade (Table 1).No statistically significant difference was noted in lo-cal recurrence free survival, disease free survival(DFS), or overall survival between patients with andwithout p53 expressing tumors by univariate analysis;however, patients with p53 expressing tumors had aslightly better outcome compared with patients with-out p53 expressing tumors (Fig. 2; Kaplan–Meiercurves for DFS). Thus, 5-year local recurrence freeinterval, 5-year DFS, and 5-year overall survival were88%, 68%, and 67.6%, respectively, in tumors that weregraded as p53 positive versus 86.4%, 58.4% and 60.4%,respectively, in tumors that were classified as p53 neg-ative (P 5 0.91, 0.18, and 0.17, respectively; log-ranktest). Of the clinicopathologic variables, only TNMstage and lymph node status were associated signifi-cantly with overall survival and DFS by univariateanalysis comparing Stage I with Stage II–III (P 5 0.01
and 0.005, respectively) (Fig. 3; Kaplan–Meier curvesfor DFS) and comparing category pN0 with categorypN1–N2 (P 5 0.03 and 0.01, respectively). In contrastto other clinicopathologic characteristics, local recur-rence free survival was correlated significantly withTNM stage (P 5 0.01), whereas gender was of border-line statistical significance for local recurrence freesurvival (P 5 0.05) by univariate analysis.
In multivariate analysis, only TNM stage was anindependent prognostic factor for overall survival andDFS (P 5 0.01 and 0.006, respectively) comparing pa-tients diagnosed at Stage I with those diagnosed atStages II–III, whereas tumor location was observed asan independent marker only for overall survival (P 50.04) but failed marginally to reach statistical signifi-cance for DFS (P 5 0.07). Multivariate analysis forrecurrence free survival revealed tumor location as anindependent variable (P 5 0.02), whereas gender wasfound as a factor of borderline statistical significance(P 5 0.05). It was shown that p53 status and the otherclinicopathologic variables examined were not statis-tically independent markers in terms of local recur-rence free interval survival, overall survival, or DFS bymultivariate analysis (Table 2).
FIGURE 1. p53 immunostaining of a biopsy sample and a corresponding
resected specimen in rectal carcinoma both classified quantitatively and
qualitatively as 111 (.50% nuclear staining; staining intensity, strong). (A)
Biopsy sample. (B) Resected specimen (original magnification, 3185).
TABLE 1p53 Overexpression of Preirradiated Biopsy Samples in Relation toClinicopathologic Characteristics in Patients with Rectal Carcinoma(n 5 100)
Characteristics No. of patientsNo. (%) with p53overexpression P value
GenderMale 46 26 (57) NSFemale 54 29 (54)
Age (yrs)#64 48 27 (56) NS.64 52 28 (54)
TNM stageI 57 33 (58) NSII–III 43 22 (51)
pT categorypT1/2 84 45 (54) NSpT3/4 16 10 (63)
pN categorypN0 63 36 (57) NSpN1/2 37 19 (51)
Histologic gradeG1/2 81 44 (54) NSG3 19 11 (58)
Tumor locationfrom analverge (cm)
4–,7 45 26 (58) NS7–,12 41 22 (54)$12 14 7 (50)
NS: not statistically significant.
2544 CANCER June 15, 1999 / Volume 85 / Number 12
Univariate subgroup analysis revealed that gain orloss of immunoreactivity in equivalent biopsy and re-sected specimens (n 5 11) was not associated signif-icantly with prognosis. Therefore, 5-year DFS and the5-year overall survival were 50% and 44%, respectively,in tumors with gain of immunoreactivity (n 5 6) ver-sus 60% and 60% in tumors that showed a loss ofimmunoreactivity (n 5 5) (P 5 0.69 and 0.65, respec-tively). Moreover, 5-year DFS and 5-year overall sur-
vival were 55% and 53%, respectively, in tumors withgain or loss of immunoreactivity (n 5 11) versus 65.1%and 65.7% in tumors with constant absence or pres-ence of immunoreactivity in corresponding biopsyand resected specimens (n 5 89) (P 5 0.53 and 0.49).
DISCUSSIONIn the present study, p53 overexpression was observedin 55 of 100 pretreatment biopsy samples from pa-tients with rectal adenocarcinoma using the monoclo-nal antibody DO-1. This percentage is in agreementwith the results from several other studies of gastro-intestinal carcinomas that also used the monoclonalantibody DO-1, including esophageal,30 gastric,31
colorectal,32 and rectal33 carcinoma, in which p53 ex-pression varied between 54.8% and 67%.
In this study, sections were classified as p53 pos-itive only when $5% of the nuclei of tumor cells werestained, as described previously.34 This threshold waschosen because positive staining of only a few nucleiwas regarded as correlating not with p53 alterationsbut with wild-type p53l.35 Although the DO-1 antibodywas shown to recognize wild-type p53 as well as mu-tant p53,28 wild-type p53 is considered to be almostundetectable by immunohistochemistry (IHC) be-cause of its short half-life.23 Nevertheless, the value ofIHC in examining p53 gene status as a prognosticmarker still is controversial. In previous studies onidentical tumor sets of colorectal carcinoma samples,concordant results between IHC and single strandconformation polymorphism (SSCP) ranged between53% and 71%.36,37 Furthermore, Greenblatt et al.38
FIGURE 2. Kaplan–Meier curves for cumulative disease free survival in 100
patients with rectal carcinoma according to p53 status: immunopositive, $5%
nuclei stained (n 5 55); immunonegative, ,5% nuclei stained (n 5 45) (P 5
0.18, log rank test).
FIGURE 3. Kaplan–Meier curves for cumulative disease free survival in 100
patients with rectal carcinoma according to TNM Stage I (n 5 57) and Stages
II–III (n 5 43) (P 5 0.005, log rank test).
TABLE 2Multivariate Cox Regression Analyses of ClinicopathologicCharacteristics for Overall, Disease Free, and Local Recurrence FreeSurvival in Patients with Preoperatively Irradiated Rectal Carcinoma(n 5 100)
Characteristics Categories
P values
Overallsurvival DFS
LR freesurvival
Gender Male vs. female NS NS 0.05Age (yrs) #64 vs. .64 NS NS NSTNM stage I vs. II–III 0.01 0.006 NSHistologic grade 1/2 vs. 3 NS NS NSTumor location from
anal verge (cm)4–,7 vs. 7–,12 vs.
$12 NS NS 0.02Time from completion
of RT to surgery(weeks) #2 vs. .2 NS NS NS
p53 status Negative vs. positive NS NS NS
DFS: disease free survival; LR free: local recurrence free; NS: not statistically significant; RT: radiother-
apy.
p53 Status and Radiotherapy/Nehls et al. 2545

noted that the results of IHC and DNA sequencingshould not be regarded as equal in terms of wild-typep53 and the mutant genotype. Moreover, when IHCwas used for detection of p53 mutations, false negativeand false positive results were observed due to a vari-ety of reasons, such as technical conditions, nonsensemutations, and stabilization of wild-type p53 by inter-actions with a considerable number of substances.35,39
In contrast, our prior studies demonstrated a nearperfect concordance of p53 overexpression and mu-tant p53 detected by polymerase chain reaction (PCR)-SSCP in premalignant conditions of the gastrointesti-nal tract (unpublished data). In addition, IHC wasconsidered to be more suitable than DNA sequencingfor the evaluation of the functional p53 status because,regardless of whether stabilization of p53 occurreddue to mutations or to other mechanisms like viralproteins, the stabilized and therefore immunohisto-chemically detectable protein might result in loss oftumor suppression.39 Thus, although DNA-sequenc-ing might be the most precise technique with which toidentify p53 mutations, immunohistochemistry wasused to detect stabilized p53 due to mutational as wellas nonmutational mechanisms that possibly caused aloss of tumor suppression.
In the current study, no statistically significantcorrelation was observed between p53 expression andclinical outcome in irradiated rectal carcinoma. Pa-tients with p53 expressing tumors were demonstratedto have a slightly better (although not statistically sig-nificant) clinical outcome. In contrast, recent studiesusing colorectal model systems have suggested thatthe presence of wild-type p53 is associated with in-creased radiosensitivity in cancer cell lines or xeno-graft tumors18 and in mice.19 This has been strength-ened by in vitro and in vivo studies in cell systemsother than the colorectal system, including mousethymocytes,17 mouse fibroblasts,12 and hematopoieticcell lines.40
However, other preclinical studies have shownthat, consistent with the current results, p53 statuswas not correlated with radiosensitivity in colorectal,20
human lymphoblastoid,41 or head and neck cancercell lines.42 Furthermore, the current results are sup-ported by a previous clinical investigation, which ex-amined advanced stage rectal carcinomas (n 5 23)with a median follow-up of 3 years, that also found nosignificant difference in DFS between the p53 negativeand the p53 positive groups by IHC.43 Clinical studiesof irradiated carcinomas other than colorectal carci-noma showed that p53 overexpression correlated withshortened survival in cervical44 and prostate carcino-ma,45 whereas no such correlation was observed inhead and neck46 or glottic carcinoma.47
The conflicting results regarding the correlationbetween p53 status and radiosensitivity might be ex-plained by the recent detection of p53-independentpathways in colorectal carcinoma cell lines after g-ir-radiation.48 Thus, cells might undergo apoptotic celldeath after DNA damage regardless of their p53 status.This is consistent with the observation that inductionof apoptosis did not require wild-type p53 when suf-ficient doses of DNA-damaging agents were applied.12
In contrast, a recent in vivo study on rectal cells frommice has demonstrated that the presence of wild-typep53 was correlated significantly with radioresistancecompared with p53 deficient cells.21 This has beenconfirmed by a clinical study on glioblastomas, inwhich it has been hypothesized that p53-mediated G1
arrest might allow repair of genetic damage and there-fore prevent p53-independent apoptosis.49 Further-more, another mechanism of p53-independent apo-ptosis has recently been suggested by Waldman et al.50
That study revealed an uncoupling of S- and M-phasesof the cell cycle in p21- and p53-deficient colorectalcell lines after DNA damage, resulting in polyploidcells undergoing apoptosis, whereas cells bearingfunctional p21 and p53 were radioresistant.
In summary, p53-dependent as well as p53-inde-pendent pathways have been suggested to induce ap-optotic cell death after g-irradiation. Thus, response toradiation might depend on more complex mecha-nisms than only one specific pathway, which has alsobeen concluded recently by Levine.51
In this study, no difference in p53 expression wasobserved between pretreatment samples and corre-sponding posttreatment samples that were gainedwithin a median of 14 days after completion of irradi-ation. This observation is in contrast to that of Fritscheet al.,52 who demonstrated that nuclear p53 proteinaccumulation after DNA damage persisted in differentcell cultures for at least 20 days. Therefore, in contrastto in vitro models, induction of p53 expression afterg-irradiation seems to be of only short duration invivo. In the current study, a cumulative dose of 30 Gywas applied. The underlying regimen was modifiedslightly according to the regimen of a randomized trialconducted by the European Organization for Researchand Treatment for Cancer,5 in which the cumulativedose was 34.5 Gy. That trial demonstrated a significantreduction in local recurrence in patients who under-went preoperative irradiation compared with patientswho underwent surgery alone.
In the current study, Stage I tumors were diag-nosed in 57% of patients. However, tumors were clas-sified postoperatively after a median period of 14 daysafter completion of radiotherapy. Thus, it is highlyprobable that considerable numbers of tumors were
2546 CANCER June 15, 1999 / Volume 85 / Number 12

downstaged by radiation, which has been demon-strated in a previous randomized trial that adminis-tered a regimen for patients with rectal carcinomasimilar to that used in this study.53 That trial used apreoperative radiotherapy dose of 31.5 Gy (18 frac-tions of 1.75 Gy) followed by surgery after 2–3 weeksand demonstrated a significantly lower rate of positivelymph nodes in resected specimens compared withsurgery alone (18.4% vs. 27.5%; P , 0.05).
In conclusion, p53 immunoreactivity in pretreat-ment biopsy samples is not useful as a prognosticmarker in preoperatively irradiated rectal carcinoma.In the current study, TNM stage was the only statisti-cally significant prognostic factor for overall and dis-ease free survival by multivariate analysis. Furtherstudies will be required to evaluate additional molec-ular factors or combinations of markers that will helpto distinguish between radiosensitive tumors and ra-dioresistant tumors.
REFERENCES1. Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics,
1998. CA Cancer J Clin 1998;48:6 –29.2. Karanjia ND, Schache DJ, North WR, Heald RJ. ‘Close shave’
in anterior resection. Br J Surg 1990;277:510 –2.3. Hurst PA, Prout WG, Kelly JM, Bannister JJ, Walker RT. Local
recurrence after low anterior resection using the staple gun.Br J Surg 1982;69:275– 6.
4. Abulafi AM, Williams SN. Local recurrence of colorectalcancer: the problem, mechanisms, management and adju-vant therapy. Br J Surg 1994;81:7–9.
5. Gerard A, Buyse M, Nordlinger B, Loygue B, Pene F, KempfP, et al. Preoperative radiotherapy as adjuvant therapy inrectal cancer. Ann Surg 1988;208:606 –14.
6. Cedermark B, Johansson H, Rutqvist LE, Wilking N. Stock-holm Colorectal Cancer Study Group. The Stockholm I trialof preoperative short term radiotherapy in operable rectalcarcinoma. A prospective randomized trial. Cancer 1995;75:2269 –75.
7. Medical Research Council Rectal Cancer Working Party.Randomised trial of surgery alone versus radiotherapy fol-lowed by surgery for potentially operable locally advancedrectal cancer. Lancet 1996;348:1605–10.
8. Swedish Rectal Cancer Trial. Improved survival with preop-erative radiotherapy in resectable rectal cancer. N EnglJ Med 1997;336:980 –97.
9. Krook JE, Moertel CG, Gunderson LL, Wieand HS, CollinsRT, Beart RW, et al. Effective surgical adjuvant therapy forhigh risk rectal carcinoma. N Engl J Med 1991;324:709 –15.
10. Gastrointestinal Tumor Study Group. Prolongation of dis-ease-free interval in surgically treated rectal carcinoma.N Engl J Med 1985;312:1465–72.
11. Glimelius B, Isacsson U, Jung B, Påhlman L. Radiotherapy inaddition to radical surgery in rectal cancer: evidence for adose-response effect favoring preoperative treatment. Int JRadiat Oncol Biol Phys 1997;2:281–7.
12. Lowe SW, Ruley E, Jacks T, Housman DE. P53 dependentapoptosis modulates the cytotoxicity of anticancer agents.Cell 1993;74:957– 67.
13. Kastan MB, Zhan Q, El-Deiry WS, Carrier F, Jacks T, Walsh
WV, et al. A mammalian cell cycle checkpoint pathwayutilizing p53 and GADD45 is defective in ataxia teleangiec-tasia. Cell 1992;71:587–97.
14. Levine AJ, Momand J, Finlay CA. The tumor suppressorgene. Nature 1991;351:453– 6.
15. Baker SJ, Fearon ER, Nigro JM, Hamilton SR, Preisinger AC,Jessup JM, et al. Chromosome 17 deletions and p53 muta-tions in colorectal carcinomas. Science 1989;244:217–21.
16. Lane DP. P53, guardian of the genome. Nature 1992;358:15– 6.
17. Lowe SW, Schmitt EM, Smith SW, Osborne BA, Jacks T. P53is required for radiation induced apoptosis in mouse thy-mocytes. Nature 1993;362:847–9.
18. Spitz FR, Nguyen D, Skibber JM, Meyn RE, Cristiano RJ, RothJA. Adenoviral-mediated wild-type p53 gene expression sen-sitizes colorectal cancer cells to ionizing radiation. Clin Can-cer Res 1996;2:1665–71.
19. Merritt AJ, Potten CS, Kemp CJ, Hickman JA, Balmain A,Lane DP, et al. The role of p53 in spontaneous and radiationinduced apoptosis in the gastrointestinal tract of normaland p53-deficient mice. Cancer Res 1994;54:614 –7.
20. Slichenmyer WJ, Nelson WG, Slebos RJ, Kastan MB. Loss ofa p53-associated G1 checkpoint does not decrease cell sur-vival following DNA damage. Cancer Res 1993;53:4164 – 8.
21. Hendry JH, Cai WB, Roberts SA, Potten CS. P53 deficiencysensitizes cells to irradiation in the large but not the smallintestine. Radiat Res 1997;148:254 –9.
22. Hamada M, Fujiwara T, Hizuta A, Gochi A, Naomoto Y,Takakura N, et al. The p53 gene is a potent determinant ofchemosensitivity and radiosensitivity in gastric and colorec-tal cancers. J Cancer Res Clin Oncol 1996;122:360 –5.
23. Lane DP, Benchimol S. P53: oncogene or antioncogene?Genes Dev 1990;4:1– 8.
24. Finlay CA, Hinds PW, Tan TH, Eliyahu D, Oren M, Levine AJ.Activating mutations for transformation by p53 produce agene product that forms an hsc70-p53 complex with analtered half-life. Mol Cell Biol 1988;8:531–9.
25. Baas IO, Van den Berg FM, Mulder JWR, Clement MJ, SlebosRJC, Hamilton SR, et al. Potential false-positive results withantigen enhancement for immunohistochemistry of the p53gene product in colorectal neoplasms. J Pathol 1996;178:264 –7.
26. Sobin LH, Wittekind C. TNM classification of malignanttumours. UICC, International Union Against Cancer, 5th ed.New York: Wiley-Liss, Inc., 1997.
27. Jass JR, Sobin LH. Histological typing of intestinal tumours.International histological classification of tumours. Geneva:World Health Organization, 2nd ed. Berlin: Springer-Verlag,1989.
28. Vojtesek B, Bartek J, Midgley CA, Lane DP. An immuno-chemical analysis of the human nuclear phosphoproteinp53. New monoclonal antibodies and epitope mapping us-ing recombinant p53. J Immunol Methods 1992;151:237– 44.
29. Kaplan E, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc 1959;53:457– 81.
30. Sarbia M, Porschen R, Borchard F, Horstmann O, Willers R,Gabbert HE. P53 protein expression and prognosis in squa-mous cell carcinoma of the esophagus. Cancer1994;74:2218 –23.
31. Gabbert HE, Muller W, Schneiders A, Meier S, Hommel G.The relationship of p53 expression to the prognosis of 418patients with gastric carcinoma. Cancer 1995;76:720 – 6.
p53 Status and Radiotherapy/Nehls et al. 2547

32. Poller DN, Baxter KJ, Shepherd NA. P53 and Rb1 proteinexpression: are they prognostically useful in colorectal can-cer? Br J Cancer 1997;75:87–93.
33. Spitz FR, Giacco GG, Hess K, Larry L, Rich TA, Janjan N, etal. P53 immunohistochemical staining predicts residual dis-ease after chemoradiation in patients with high-risk rectalcancer. Clin Cancer Res 1997;3:1685–90.
34. Ahnen DJ, Feigl P, Quan G, Fenoglio-Preiser C, Lovato LC,Bunn PA, et al. Ki-ras mutation and p53 overexpressionpredict the clinical behaviour of colorectal cancer: a South-west Oncology Group study. Cancer Res 1998;58:1149 –58.
35. Hall PA, Lane DP. P53 in tumour pathology: can we trustimmunohistochemistry?—revisited! J Pathol 1994;172:1– 4.
36. Dix B, Robbins P, Carrello S, House A, Iacopetta B. Compar-ison of p53 gene mutation and protein overexpression incolorectal carcinomas. Br J Cancer 1994;70:585–90.
37. Smith DR, Ji CY, Goh HS. Prognostic significance of p53overexpression and mutation in colorectal carcinomas. Br JCancer 1996;74:216 –23.
38. Greenblatt MS, Bennett WP, Hollstein, Harrris CC. Muta-tions in the p53 tumor suppressor gene: clues to canceretiology and molecular pathogenesis. Cancer Res 1994;54:4855–78.
39. Wynford-Thomas D. P53 in tumour pathology: can we trustimmunocytochemistry? J Pathol 1992;166:329 –30.
40. Lee JM, Bernstein A. P53 mutations increase resistance toionizing radiation. Proc Natl Acad Sci USA 1993;90:5742– 6.
41. Xia F, Wang X, Wang YH, Tsang NM, Yandell DW, Kelsey KT,et al. Altered p53 status correlates with differences in sen-sitivity to radiation-induced mutation and apoptosis in twoclosely related human lymphoblast lines. Cancer Res 1995;55:12–5.
42. Brachman DG, Beckett M, Graves D, Haraf D, Vokes E,Weichselbaum RR. P53 mutation does not correlate withradiosensitivity in 24 head and neck cancer cell lines. CancerRes 1993;53:3667–9.
43. Desai GR, Myerson RJ, Higashikubo R, Birnbaum E, Flesh-
man J, Fry R, et al. Carcinoma of the rectum. Possiblecellular predictors of metastatic potential and response toradiotherapy. Dis Colon Rectum 1996;39:1090 – 6.
44. Nakano T, Oka K, Taniguchi N. Manganese superoxide dis-mutase expression correlates with p53 status and local re-currence of cervical carcinoma treated with radiation ther-apy. Cancer Res 1996;56:2771–5.
45. Grignon DJ, Caplan R, Sarkar FH, Lawton CA, HammondEH, Pilepich MV, et al. P53 status and prognosis of locallyadvanced prostatic adenocarcinoma: a study based onRTOG 8610. J Natl Cancer Inst 1997;89:158 – 65.
46. Awwad S, Jaros E, Somes J, Lunec J. P53 overexpression inhead and neck carcinoma and radiotherapy results. Int JRadiat Oncol Biol Phys 1996;34:323–32.
47. Kokoska MS, Piccirillo JF, El-Mofty SK, Emami B, HaugheyBH, Scholnick SB. Prognostic significance of clinical factorsand p53 expression in patients with glottic carcinomatreated with radiation therapy. Cancer 1996;78:1693–700.
48. Bracey TS, Miller JC, Preece A, Paraskeva C. g-Radiation-induced apoptosis in human colorectal adenoma and car-cinoma cell lines can occur in absence of wild-type p53.Oncogene 1995;10:2391– 6.
49. Tada M, Matsumoto R, Iggo RD, Onimaru R, Shirato H,Sawamura Y. Selective sensitivity to radiation of cerebralglioblastomas harboring p53 mutations. Cancer Res 1998;58:1793–7.
50. Waldman T, Lengauer C, Kinzler KW, Vogelstein B. Uncou-pling of S phase and mitosis induced by anticancer agents incells lacking p21. Nature 1996;381:713– 6.
51. Levine AJ. P53, the cellular gatekeeper for growth and divi-sion. Cell 1997;88:323–31.
52. Fritsche M, Haessler C, Brandner G. Induction of nuclearaccumulation of the tumor-suppressor protein p53 by DNA-damaging agents. Oncogene 1993;8:307–18.
53. Horn A, Morild I, Dahl O. Tumour shrinkage and downstag-ing after preoperative radiation of rectal adenocarcinomas.Radiother Oncol 1990;18:19 –28.
2548 CANCER June 15, 1999 / Volume 85 / Number 12