Embed Size (px)
Citation preview

Turkish Neurosurgery 3: 128· 133. 1993 Erongun: 1n1Iatemporal Approac1i
Infratemporal Approach For Jugular Foramen Meningioma
UGUR ERONGUN. YAVUZ UYAR. BiLGE ÇAKIR. ALI UYGUN. YALÇIN KOCAOGULLAR.
Selçuk University Medical School Departments of Neurosurgery (UE. AU. YK).Otorhinolaryngology (YU)and Radiology (BÇ)Konya. TÜRKIYE
Abstract : The properties of tumours of the jugular foramen arepresented and the details of the infratemporal A approach. a newtechnique for neurosurgeons. are discussed.
INTRODUCTION
The jugular foramen is a canal in the skull basebetween the lateral aspect of the occipital bone andthe inferiomedial part of the petrous pyramid andis divided anatomically into two parts by a bone orfibrous septum. anteriody the pars nervosa andposteriorly the pars venosa. While the inferiorpetrousal sinus and the N. glassopharingeus are pass·ing through the pars nervosa. the V. jugularis interna. N. vagus. N. accessorius. ascendant pharingealartery and meningeal branches of the occipital arterypass though the pars venosa. The foramen jugularewhich has such a complicated structure. is affectedby congenitaL. vascular and. most frequently.tumoural lesions and these lesions reveal various
clinical syndromes. Most often encountered tummours in the foramen jugulare region are glomusjugulare tumour. neuroma. meningioma. metastaticcarcinoma. chondroma.· nasopharynx carcinoma andcarcinoma of the tympanic cavity. Symptomatologyof these tumours may be primarily otological orneurological or a combination ofboth (3.7). The mostencountered initial symptoms are loss ofhearing. tinnitus. otorrhoea. facial paralysis. pain and 9th. lOth.IIth aanial nerve paralysis. Paralysis of these nervesis called Syndrome of the jugular fossa or Vernet'ssyndrome and is characterized by loss of taste sensation in the posterior third of the tongue. paralysis
128
Key Words Jugular foramen. Meningioma. InfratemporalA approach.
of the vocal cords and soft palate and weakness ofthe trapezius and sternocleidomastoid muscles. Iftumours of the foramen jugulare region extendmedial1y to the hypoglossal canal and causehypoglossal nerve paralysis. the clinical presentationis known as Collet-Sicard syndrome.
CASE REPORT
This 42-year-old female was admitted to the ENTclinic on 2l January 1992 with a complaint ofhoarseness. After questioning the patient it wasrevealed that the prasent complaint started 9 monthspreviously and had inaeased since then and duringthe pa st two months headache and difficulty inswallowing were added. General physical examination reve ale d no significant finding. Afterotoneurolaryngological examination. it was foundthat the right vocal cord was fixed in the paramedianline. the uvula was retracted to the left and the gagreflex was lost.
Routine laboratory studies and plain X-rays showed no significant abnormality. Although clinical1ythere was no neurological deficit related to the IIthcranial nerve. EMG revealed partial denervation ofthe sternocleidomastoid muscle. Electrophysiologicalevaluation of the facial muscles. audiogram and electronystagmogram were within normal limits.

Turkish Neurosurgery 3: 128 - 133. 1993
After an axial and coronal CT investigation of thebasis cranU an 18x22x20 mm mass origiriating in thejugular canal was found. The mass had enlarged thecanal by filling the lumen and showed extracanaliculary extension at the caudal part. Themass, which had a dumb-bell configuration extended along the posterior contour of the petrous boneto the cerebello-pontine angle obliterating thecerebello-pontine dstern. There were amorphouscaldfications inside and around the mass. CT after
administration of contrast material show ed slightenhancement. There was no perifocal oedema. Thewidth of the internal acoustic canal was normaL. The
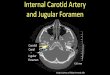
right lateral recess of the 4th ventric1e was compressed. (Fig1.2)Although the morphological appearance
Fig. 1a.b: Axia] and coranal CT showing a mass Eillingenlargingthe jugu1ar foramen with extracanaliculary extension.
Erongun: Infratempora] Approach
Fig.2a.b : On postoperative axia]and corana] CT, complete removelof the tumuor.
of the mass on CT was meningioma, it was thoughtthat it could be a neurogenic tumour due to its configuration so from that standpoint. the infratemporalA approach developed by Fisch. was chosen for complete removal of the mass.
Endotracheal general anestheisa was performed.A skin indsion in the shape of an inverse "S" wasmade beginning in the right temporal region andpassing through the postauricular area and extendingdownward to the hyoid bone at the neck. The indsion was carried down to the mastoid periosteum.A periosteal flap in connection with the externalauditory canal was prepared from mastoidperiosteum. The external auditory canal was
129

Turkish Neurosurgery 3: ll8 - 133. 1993
incised. the skin was turned back and stitched. The
entran ce of the external auditory canal was occluded using a periosteal flap. The branches of the facialnerve in the parotid gland was exposed. Then attention was directed to the neck and the vessel-nerve
sheath was exposed. The internal jugular vein. common carotid artery. external and internal carotidarteries were found and tracks of the N. vagus. N.glossopharingeus and N. accessorius were identified.Mastoidectomy was performed. The sigmoid sinus.digastric ridge. facial nerve and bony labyrinthinewere exposed by removing retrosigmoid. retrofadal.retrolabyrinthine. supralabyrinthine. infralabyrinthine. pericarotid and supratubal cells. At the sametime the posterior bone wall of the external auditorycanal was removed so that a bridge was made. Thetympanic membrane and ossicle chain were removed. A new fallopian canal beginning around thegeniculate ganglion and passing along the anteriorwall of the external auditory canal was made andthe facial nerve was elevated from its normal position and transported to this new canaL.(Fig 3) Themastoid apex and bony laminas on the sigmoid sinus
Erongun: Infratempora1 Approach
were removed. Small dural indsions were made in
front and behind the sigmoid sinus and then thesigmoid sinus was ligated with a pair of sutures.The vertical portion of the ICA was exposed on themedial wall of the middle ear. The tube efEustachian
was obliterated with bone-wax. The styloid processwas excised and using a high speed drill the inferiorpart of the tympanic bone was removed so that thejugular bulb. sigmoid sinus. V. jugularis interna andcervical segment of the ICA and its vertical segmentin the temporal bone were completely exposed. Thejugular bulb was partially filled by a tumoural mass.The V. jugularis interna was ligated in the neck andthe tumour was exposed by opening the bulbus ofthe jugular vein. During this period massive bleedingfrom the petrousal sinuses was contrelled. Thetumour had enlarged the jugular foramen and compressed the 9th. lOth and iIth aanial nerves. Bonystructure around the jugular foramen was remove dby drilling and 2x2 cm of the dura was exposed. Afteropening the dura mater the cerebello-pontine anglewas exposed. When the abnormally thickenedarachn9id walls of the dsterns were opened it was
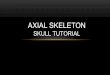
Fig. 3 : View of the operation Field after fadal nerve transposition (anterior reroruting)
1- Fadal nerve (at the tip of miaodissector)L· Bony labyrinthine3- The segment of the ICA in temporal bone.4- 1nternal jugular vein.5- Sigmoid sinus6- Middle cranial fossa
130

Turkish Neurosurgery 3: 128 - 133. 1993 Erongun: Infratemporal Approach
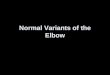
Fig. 4 : Tumoral tissue at the tip of the aspiration tube and cerebellum immediately above are seen.
Fig. 5 : The seventh and eight aanial nerves. brain stem. PICA and cerebellum at the tip of the bipolaryforcep after total exdsion of the tumour.
131

Turkish Neurosurgery 3: 128 . 133. 1993
seen that the operative field was completely occupiedby the tumour which had an epiarachnoidal deavagewith the cerebellum. (Fig 4) It was recognized thatthe tumour was macroscopically a meningiomarather than aneuroma. It was impossible to identifyany vital vascular and neural structure in theoperative field. so to achieve mobilization of the massinternal decompression was dissected from the 7thand Sth cranial nerves on the superior pole. Afterdissection was completed. both the cranial nerveswere visible. Preserving the epiarachnoidal deavagebetween the tumour and the brain stern. thetumoural mass was reduced in size and mobilizedfrom the nest it had made on the brain stern. At last
the PICA was dissected from the inferio-posteriorportion of the tumour and total tumour excision wasachieved. (Fig 5) The dural opening was covered bya musculo-facial graft from temparalis musde. Thecavity was packed using fat harvested from theanterior abdominal wall and a temporalis flap wasdesigned to cover the cavity completely.
The patient had no additional neurologic deficitsduring the postoperative period. Pathology revealedangioblastic meningioma.
DlSCUSSION
Radical surgical management of jugular faramentumours has made great progress in parallel with advances in neuroradiological investigations. Particularly the introduction of CT. NMR and DSA hasprovided considerable aid. The complexity of theanatomical structure in the jugular faramen region.the close proximity of the jugular foramen to veryimportant neurovascular structures like the ICA,jugular bulb. the seventh and eighth cranial nervesand the brain stern. and the possibility of an intracranial mass extending to the extracranial spaceor an extracranial one to the intracranium have in
creased the importance of surgical treatment ofjugular foramen tumours.
First of all. it should be determined whether
tumours of the jugular fararnen are purely intraaanialor solely extraaanial or have both extraaanial andintracranial components (5). After location thetranslabyrinthine. infratemporal A, transsigmoid.transmandibular. retrosigmoid or suboccipital surgicalapproaches can be used. depending upon the symptomatology. size and extension of the tumour.
132
Erongun: Infratemporal Approach
With the translabyrinthine approach. due tolabyrinthectomy. permanent total sensorineural hearing loss occurs postoperatively. For this reason. it canbe performed in cases with hearing loss. AlthoughHorn and House (4) postulated that this approach provided direct access to the jugular bulb and posteriorfossa. existence of the facial nerve superficially overthe jugular faramen limits surgical manipulations inthis region. Because the area exposed is limited.radical excision of intracranially located tumours isimpossible.
The transsigmoid appoach for jugular faramentumours was desaibed by Mann and et aL.(S).Withthis technique. the jugular foramen is exposedwithout performing facial nerve transposition andlabyrinthectomy thus cochleavestibular function isprotected. After mastoidectomy. the sigmoid sinusis found and the jugular bulb exposed. The disadvantage of this approach is limited exposure of thejugular fararnen so removal oflarge tumours and particularly their intracranial components. is dillicult.
With the transmandibulary approach anasteotomy is performed on the mandible at themidline (6). The parapharyngeal area is enteredthrough the floor of the mouth and the jugularforamen is exposed by retracting half the mandiblelaterally. But this type of approach is not practicalbecause as the area is deeply situated it is very dilficult to reach the intradural portion and haemostasismay be a surgical problem due to inability to control the sigmoid sinus.
The infratemporal A approach as performed byFisch provides direct access to the jugular foramen(i). The details of this technique were discussed inthe case report. The most important advantage of thisapproach is that it provides wide exposure of thefaramen jugulare region because transposition of thefacial nerve is possible and the intraaanial component can be exposed easily. The most importantdisadvantage is permanent conductive deafness sincethe bony chain of the middl,e ear and externalauditory way are excised and obliteration occurs, buthearing aids are effective. Despite the risk of paresisor paralysis after facial nerve transposition, this complication is rare and transient with meticuloussurgical manipulation. This technique of Fisch isalso prefered in tumours which have excessive extracranial extension since the neck has been exposed to the level of the hyoid bone.

Thrkish NeutOsurgery 3: 118 - 133. 1993
The subocdpital approach is preferred fortumours purely intraaanial in location which don'tcause hearing loss. This methot is advised for exdsion of tumours greater than 2 cm in diameter. it requires long-standing retraction of the cerebellum andto expose the extraaanial part of the tumour is difficult. On this appro;;ichcontrol of bleeding has somedifficulties related to surgical technique. However.with the infratemporal approach, the sigmoid sinusand internal jugular vein are ligated and profusebleeding from petrousal sinuses can easily be controlled (9).
Following examination of the techniques discussed above. the infratemporal A appoach was chosenfor our patient for three reasons:
1. The most direct and widest possible exposureof the jugular foramen is afforded due to transposition of the fadal nerve.
2. Bleeding can be controlled by haemostasis ofthe important sinuses and veins in the region.
3. It is also possible to expose the intracranialcomponent of the tumour.
Fisch. who developed the infratemporal A approach. described the removal of tumours greaterthan 2 cm in diameter in two stages (1.2). A1.thoughthe tumour was greater than 2 cm in diameter. in ourpatient complete removal was accomplished usinga one-staged surgical approach.
Erongun: Infratemporal Approach
Correspondence: Asso. Prof. Dr. Ugur ErongunSelçuk University, Medical schoolNeurosurgery DepartmentKonya - TÜRKIYE
RBFBRBNCBS
i. Fisch U,Mattox D: Infraternpora! fossa approach type A. In Fisch
U (ED): Miaosurger of the skull basi. Stuttgart-New York:
Thierne Medical Publishers. 198S: 136-281
2. Franklin DJ, Moore GF. Fisch U: Jugular forarnen peripheral
nerve sheath turnors. Laryngoscope 99: 1081-1087. 1989
3. Friedman CD, Costantino PD. Teitelbaum BS : Primary ex
raaania! meningiomas of the head and neek. Laryngoscope 100:
41-48. 1990
4. Hom KL. House WF. Hitselberger WE: Schwannomas of the
jugular foramen. Laryngoscope 95: 761-768. 1985
5. Janeeka lP-Sekhar LN: Meningiomas. Head and neek perspec
tives. In Fisch U. Va!avanis A, Yasargil MG (ED):Neurological
surgery of the ear and skull base. Amsterdan-Milano: Kuglerand Ghediki Publications, 1989: 139-152
6. Krespi YP.Sisson GA: Transmandibuler exposure of skull base.
Am J. Surg. 146: 102-106. 1984.
7. Kumen A. Mafee M, Vassalli L: lntraaanial and infratemporal
meningiomas with primary otologic symptoms. Otolaryngol
Head Neek Surg 99: 444-454. 1988.
8. Mann WJ, Amedee RG, Gilsbach J: Transsigmoid approach for
tumors of the jugu1ar forarnen. Skull base surg 1: 137-14i. 199 i.9. Raquet F, Mann WJ, Amedee RG: Funetiona! defidts of aanial
nerves in patients with jugular forarnen lesions. skull Base Surg1: 117-119. 1991.
133