Embed Size (px)
Citation preview

lnr J Rodiorion Oncology Biol Phys Vol. 8. pp 999-1003 036~3016/82/060000~103.0010
Printed in the U S A All rights reserved Copyght 63 ,9X2 Pergamon Press I td
??Original Contribution
INFRATENTORIAL GLIOBLASTOMA: THE ROLE OF NEURAXIS IRRADIATION
GENE KOPELSON, M.D. AND RITA LINGGOOD, M.D. Department of Radiation Medicine, Massachusetts General Hospital. Boston, MA 02 I I4
The patterns of clinical-and autopsy-documented tumor spread were evaluated for 15 patients with biopsy-proven infratentorial(8 cerebellar, 2 brainstem, 5 intramedullary spinal cord) glioblastoma. No patient developed clinical nor autopsy evidence of subarachnoid dissemination, even though no patient had received craniospinal axis irradiation. Fully 14 of the 21 previously reported patients with suharachnoid dissemination from infratentorial glioblastoma had this diagnosis made only at autopsy. The overall poor prognosis at present (8 % 3-year survival from the present series and recent literature) along with the demonstrated pattern of local-regional aggressiveness as the major form of initial spread and post-irradiation recurrence, suggests that routine craniospinal axis irradiation may not be indicated for most patients with infratentorial glioblastoma.
Cerebellar neoplasms, Brainstem neoplasms, Spinal cord neoplasms. Radiotherapy.
INTRODUCTION
Patients with infratentorial glioblastoma are uncommon. and in many series of patients with glioblastoma, only patients with supratentorial primary tumors have been included. Recent attention has focused on subarachnoid dissemination from intracranial glioblastoma, but most of the previously reported patients have had supratentorial primaries.” However, because subsequent clinical sub- arachnoid dissemination occurred in 4 of 6 patients with infratentorial glioblastomas seen at one institution34.3’ initial craniospinal irradiation was advocated for these patients. The present report examines the natural history of these tumors based upon 15 patients with biopsy- proven infratentorial (8 cerebellum, 2 brainstem, 5 intra- medullary spinal cord) glioblastoma along with the rele- vant literature in order to assess the need for routine neuraxis irradiation in such patients.
METHODS AND MATERIAL
From 1962 to 1980, 745 patients with central nervous system astrocytoma (grade I ,2) or glioblastoma (astrocy- toma grade 3,4) were registered at the Tumor Registry of the Massachusetts General Hospital. Fifteen patients with infratentorial glioblastoma form the basis of this report (Table 1). Excluded were patients with infratento- rial lesions which were of low grade (grade 1,2), without biopsy (i.e. premortem) proof of glioblastoma, of mixed cell type, or of indeterminate grade. Although there is
controversy as to whether grade I I I astrocytomas should be included as part of glioblastoma.” it was elected to include patients with grade III or IV in the present definition of glioblastoma.
Initial presentation and management including irradia- tion doses and fields appear in Table I. Described else- where are the specific irradiation techniques used for the patients with cerebellar’” and intramedullary spinal cord glioblastomas.“.” All irradiated patients were treated with supervoltage with “Co or with 2- or IO-MV X-rays.
Actuarial survival’ was calculated from the date of diag- nosis (i.e., initial surgery).
Survival
RESULTS
An overall actuarial survival rate of 14% at 5 years was achieved (Fig. I) with prognosis being relatively better
for lower-grade lesions (Fig. 2) and for tumors in the cerebellum (Fig. 3). These differences are due to one long-term survivor who had a grade III cerebellar lesion and is presently alive and well more than 8 years after partial resection plus 5000 rad delivered to the posterior fossa and upper cervical spinal cord.
Patterns ofspread
Of the 8 cerebellar patients, brainstem invasion was present at initial presentation in 3 and at autopsy in (Table 2). Upper cervical spinal cord involvement by
Presented at the 67th Annual Meeting of the Radiological Society of North America, Chicago, November 17, I98 I,
Reprint requests to: Dr. G. Kopelson, Dept. of Radiation Oncology, Salem Hospital, 81 Highland Ave., Salem, MA 01970.
Acknowledgements-The authors would like to thank Mind) and Barry Kopelson for their help in the preparation of this manuscript.
Accepted for publication I8 January 1982.
999
1000 Radiation Oncology ??Biology 0 Physics
Table I. Clinical presentation and management in 15 patients with infratentorial glioblastoma
Age (years) Range Median
Males:Females Histologic grade
III IV
Surgical procedure Complete resection Subtotal resection Biopsy
Cerebrospinal fluid cyto-
logy Positive Negative (preopera-
tively) Not performed
Myelogram Positive Negative Not performed
Radiation therapy tech- niques
Primary site irradia- tion
Primary and whole brain
Primary and whole spinal cord
Primary and whole neuraxis
No irradiation
Cerebellum Brainstem Intramedullary
spinal cord
IO-67 8-15 17-70 54 I2 34 612 2:o 2:3 4 0 2
4 2
2 0 3 I 3 I
0 0 4 0
5 I
0 0 0 0 8 2
3* l§
It 0
0 0
0 0
44 I$
3
0 0 5
5 0 0
5**
0
0
0
0
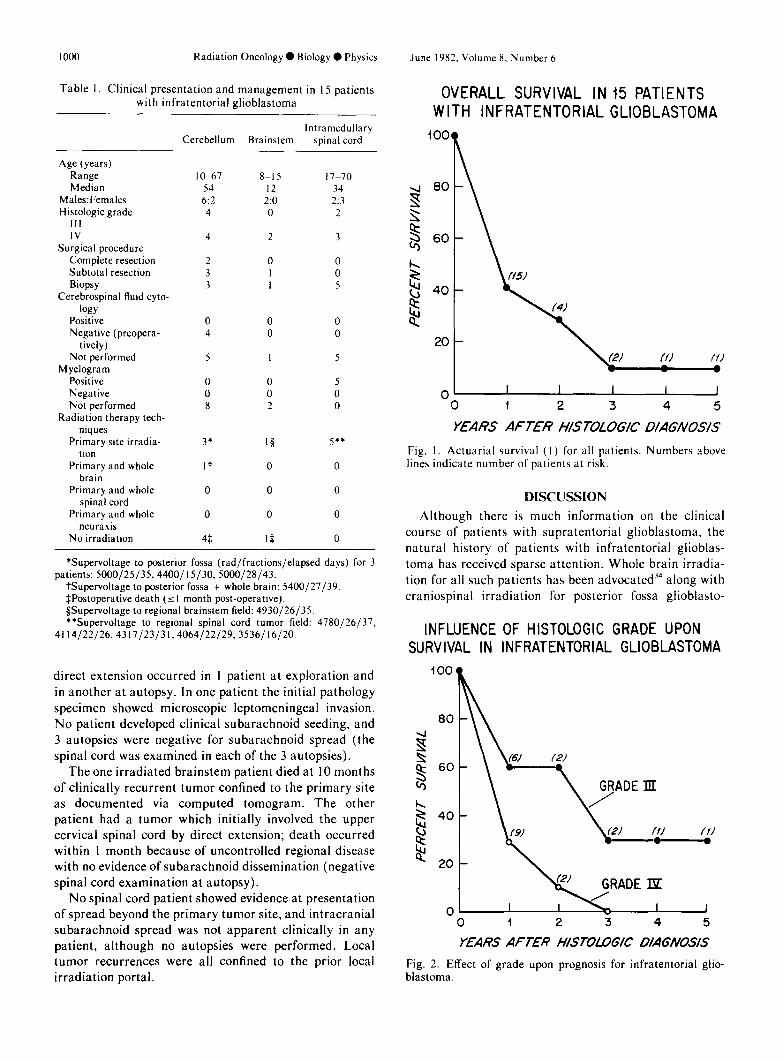
*Supervoltage to posterior fossa (rad/fractions/elapsed days) for 3 patients: 5000/25/35.4400/ 15130, 5000/28/43.
tsupervoltage to posterior fossa + whole brain: 5400/27/39. SPostoperative death (5 I month post-operative). SSupervoltage to regional brainstem field: 4930/26/35. **Supervoltage to regional spinal cord tumor field: 4780/26/37.
4114/22/26.4317/23/31,4064/22/29.3536/16/20.
direct extension occurred in 1 patient at exploration and in another at autopsy. In one patient the initial pathology specimen showed microscopic leptomeningeal invasion. No patient developed clinical subarachnoid seeding, and 3 autopsies were negative for subarachnoid spread (the spinal cord was examined in each of the 3 autopsies).
The one irradiated brainstem patient died at 10 months of clinically recurrent tumor confined to the primary site as documented via computed tomogram. The other patient had a tumor which initially involved the upper cervical spinal cord by direct extension; death occurred within I month because of uncontrolled regional disease with no evidence of subarachnoid dissemination (negative spinal cord examination at autopsy).
No spinal cord patient showed evidence at presentation of spread beyond the primary tumor site, and intracranial subarachnoid spread was not apparent clinically in any patient, although no autopsies were performed. Local tumor recurrences were all confined to the prior local irradiation portal.
June 1982. Volume 8. Number 6
OVERALL SURVIVAL IN 15 PATIENTS WITH INFRATENTORIALGLIOBLASTOMA
.J 80 3 2 $ 60
2 8 40
$
20
01 I I I I I 0 1 2 3 4 5
YEARS AFTER MSTOLOGK’ OIAG/VOS/S
Fig. I. Actuarial survival (I) for all patients. Numbers above lines indicate number of patients at risk.
DISCUSSION
Although there is much information on the clinical course of patients with supratentorial glioblastoma, the natural history of patients with infratentorial glioblas- toma has received sparse attention. Whole brain irradia- tion for all such patients has been advocated34 along with craniospinal irradiation for posterior fossa glioblasto-
INFLUENCE OF HISTOLOGIC GRADE UPON SURVIVAL IN INFRATENTORIAL GLIOBLASTOMA
O- I 1 0 I 2 3 4 5
YEARS AFTER H/SlOLOG/C D/AG#OS/S
Fig. 2. Effect of grade upon prognosis for infratentorial glio- blastoma.
lnfratentorial glioblastoma 0 G. KOPELSON AND R. LINGGOOD 1001
INFLUENCE OF TUMOR SITE UPON SURVIVAL IN INFRATENTORIAL GLIOBLASTOMA
0 \f2) I I 1
0 1 2 3 4 5
YEARS AFTEff H/STOLOG/C D/AG/VOS/S
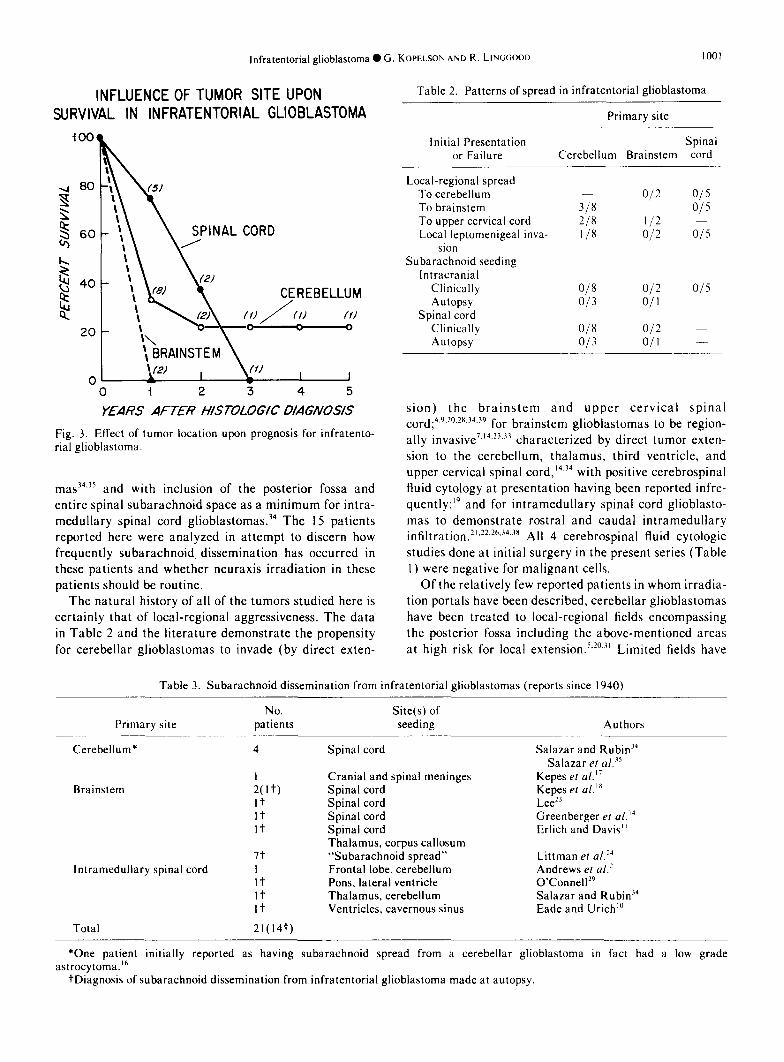
Fig. 3. ERect of tumor location upon prognosis for infratento- rial glioblastoma.
mas34.35 and with inclusion of the posterior fossa and entire spinal subarachnoid space as a minimum for intra- medullary spinal cord glioblastomas.34 The 15 patients reported here were analyzed in attempt to discern how frequently subarachnoid, dissemination has occurred in these patients and whether neuraxis irradiation in these patients should be routine.
The natural history of all of the tumors studied here is certainly that of local-regional aggressiveness. The data
in Table 2 and the literature demonstrate the propensity for cerebellar glioblastomas to invade (by direct exten-
Table 2. Patterns of spread in infratentorial glioblastoma
Primary site
Initial Presentation or Failure
Spinal Cerebellum Brainstem cord
Local-regional spread To cerebellum To brainstem To upper cervical cord Local leptomenigeal inva-
sion Subarachnoid seeding
Intracranial Clinically Autopsy
Spinal cord Clinically Autopsy
o/2 015 318 015 218 112 l/8 O/2 O/5
018 012 015 013 O/l
O/8 O/2 O/3 O/l
sion) the brainstem and upper cervical spinal cord;4.y.2”.‘X.34.39 for brainstem glioblastomas to be region- ally invasive7~14~23~33 characterized by direct tumor exten- sion to the cerebellum, thalamus, third ventricle, and upper cervical spinal cord,‘4.34 with positive cerebrospinal fluid cytology at presentation having been reported infre- quently;” and for intramedullary spinal cord glioblasto- mas to demonstrate rostra1 and caudal intramedullary in~~tr~tion.2’.22.2h.34.3X All 4 cerebrospinal fluid cytologic studies done at initial surgery in the present series (Table I) were negative for malignant cells.
Of the relatively few reported patients in whom irradia- tion portals have been described, cerebellar glioblastomas have been treated to local-regional fields encompassing the posterior fossa including the above-mentioned areas at high risk for local extension.s.2”.3’ Limited fields have
Table 3. Subarachnoid dissemination from infratentorial glioblastomas (reports since 1940)
Primary site No.
patients Site(s) of seeding Authors
Cerebellum* 4
Brainstem I
2(1-Q It It It
lntramedullary spinal cord 7t I It It It
Total 21(14t)
Spinal cord
Cranial and spinal meninges Spinal cord Spinal cord Spinal cord Spinal cord Thalamus, corpus callosum “Subarachnoid spread” Frontal lobe, cerebellum Pons, lateral ventricle Thalamus, cerebellum Ventricles. cavernous sinus
Salazar and Rubit? Salazar ef al.”
Kepes er al.” Kepes et al. I8
Lee*’ Greenberger et ~1.‘~ Erlich and Davis”
Littman et a1.14 Andrew et al.’ 0’Connellz9 Salazar and Rubi# Eade and Urich”
*One patient initially reported as having subarachnoid spread from a cerebellar glioblastoma in fact had a low grade astrocytoma.‘”
tDiagnosis of subarachnoid dissemination from infratentorial glioblastoma made at autopsy.

1002 Radiation Oncology 0 Biology 0 Physics June 1982. Volume 8, Number 6
also been described for patients with brainstem6,‘4.24.33 and intramedullary spinal cord glioblastomas.2’.22 Indeed, there have been few reports and/or recommendations for whole brain irradiation23,34 or neuraxis treatment.32.34.‘s
Table 4. Survival in patients with infratentorial glioblastoma reported since 1970
A literature review of the 21 specific patients reported in the past 40 years who had subarachnoid dissemination from infratentorial glioblastoma (Table 3) reveals that in fully 14 patients (67%), the diagnosis of subarachnoid seeding was made only at autopsy. Even in two large series which emphasized the occurrence of subarachnoid dissemination from intracranial glioblastomas, the spe- cific location of the primary tumors was not mentioned.3.4’ In a general literature review of this phenomena, by far the overwhelming majority of patients had glioblastomas that were not of infratentorial origin.” Because the survival of even recently reported patients is so poor (Table 4, Fig. 1) coupled with the few patients reported thus far with subarachnoid dissemination (Table 3), elective neuraxis irradiation may not be needed in these patients. All 4 of the autopsied patients in this series had no evidence of subarachnoid dissemination; however only 4 survived 2 years and it is possible that if there were more long-term survivors, perhaps some would have manifested late subarachnoid spread. However, even if future larger autopsy series demonstrate a high rate of subarachnoid spread, because local-regional recurrence post-irradiation is the major cause of therapeutic failure at present, elective neuraxis irradiation would probably not be of clinical benefit. And given the added treatment time, complex nature of craniospinal irradiation, and added morbidity such as effects on blood countsI on this group
Tumor site
Cerebellum Brainstem lntramedullary
spinal cord
No. patients with No. 3-year positive biopsy* survivorst
264 3 (5, 17. present report)
28§ 0 18** 3 (8)
Total 72 6 (8%)
*Includes only those patients in whom the report specifically stated that the diagnosis of glioblastoma was made premortem.
tlncludes only those patients in whom the report specifically stated that 3-year survival was achieved for a patient with biopsy-proven infratentorial glioblastoma.
SRef. No,s.9.‘~.‘7.*‘.*8.‘5 , present report. §Ref. No.‘~~~~~‘~~‘*~‘~~~~~‘~~~, present report. **Ref. No.*~‘~~~~~~‘~‘*, present report.
of patients with limited lifespan, probably the only patient in whom elective neuraxis irradiation might be considered would be a patient with a grade III lesion in whom cerebrospinal fluid cytology were positive. A possible longer lifespan (because of a grade III rather than grade IV lesion) might be made more comfortable with elective neuraxis irradiation if this added treatment prevented the clinical onset of spinal seeding.
In conclusion, although subarachnoid dissemination has occurred in patients with infratentorial glioblastomas, the present poor overall survival of these patients because of uncontrolled local-regional disease, indicates that elec- tive neuraxis irradiation of the majority of these patients should probably not be routine.
REFERENCES I.
2.
3.
4.
5.
6.
7.
8.
9.
10.
American Joint Committee for Cancer Staging and End Results Reporting (AJCCS): Manual for Staging of Can- cer 1977, Chicago, American Joint Committee. 1977, pp. 18-21. Andrews, A.A., Enriques, L., Renaudin, J., Tomiyasu, U.: Spinal intramedullary glioblastoma with intracranial seed- ing. Arch. Neurol. 35: 244-245, 1978. Bryan, P.: CSF Seeding of Intra-cranial tumors: A study of 96 cases. Clin. Radiol. 25: 355-360, 1974. Budka, H., Wober, G.: Primary glioblastoma of the cerebel- lum. Acta. Neurochirig. 13: I 15-121, 1974. Caldwell, W.L., Aristizabal, S.A.: Treatment of glioblas- toma multiforme. Acta. Radiol. 14: 505-5 12, 1975. Cassady, J.R., Greenberger, J.S.: Results in the treatment of brainstem, thalamic, and midbrain tumors. In Tumors of the Central Nervous System: Modern Radiotherapy in Multidisciplinary Movement. Chong, C.Y., Harisiadis, L., Chang, C.H.: Radiotherapy of brainstem tumors, presented at the 56th Annual Meeting of the American Radium Society, Maui, Hawaii, April 24, 1974. Clifton, M.D., Amromin, C.D., Perry, M.C., Abadir, R., Watts, C., Levy, N.: Spinal cord glioma following irradia- tion for Hodgkin’s disease. Cancer 45: 205 I-2055, 1980. Dohrmann, G.J., Dunsmore, R.H.: Glioblastoma multi- forme of the cerebellum. Surg. NeuroI. 3: 219-223, 1975. Eade, D.E., Urich, H.: Metastasizing gliomas in young subjects. J. Neurosurg. 45: 705-707, 1976.
I I.
12.
13.
14.
15.
16.
17.
18.
19
20. 21.
Erlich, S.S., Davis, R.L.: Spinal subarachnoid metastases from primary intracranial glioblastoma multiforme. Cancer 42: 2854-2864, 1978. Fresh, C.B., Takei, Y., O’Brien, M.S.: Cerebellar glioblas- tomas in childhood. J. Neurosurg. 45: 705-707, 1976.
Giudetti, B., Mercuri, S., Vagnozzi, R.: Long-term results of the surgical treatment of 129 intramedullary spinal gliomas. J. Neurosurg. 54: 323-330, I98 1. Greenberger, J.S., Cassady, J.R., Levene, M.B.: Radiation
therapy of thalamic midbrain, and brainstem gliomas. Radiology 122: 463-468, 1977. Harisiadis, L., Kopelson, G., Chang, C.H.: Lymphopenia caused by cranial irradiation in children receiving cranio- spinal radiotherapy. Cancer 40: 1102-I 108, 1977. Hochberg, F.H., Pruitt, A.: Assumptions in the radiother- apy of glioblastoma. Neurology 30: 907-9 1 1, 1980. Kepes, J.J., Lewis, R.C., Vergave, G.G.: Cerebellar astro- cytoma invading the musculature and soft tissues of the neck. J. Neurosurg. 52: 4 14-4 18, 1980. Kepes, J.J., Striebinger, CM., Brackett, C.E., Kishore, P.: Gliomas (astrocytoma) of the brainstem with spinal intra- and extradural metastases-a report of 3 cases. J. Neurol. Neurosurg. Psych. 39: 66-76, 1976. Kim, T.H., Chin, H.W., Pollan, S., Hazel, J.H., Webster, J.H.: Radiotherapy of primary brainstem tumors. In?. J. Radial. Oncol. Biol. Phys. 6: 51-57, 1980. Kopelson, G.: Cerebellar glioblastoma, Cancer (In press). Kopelson, G., Linggood, R.M.: Intramedullary spinal cord

lnfratentorial glioblastoma ??G. KOPELSON AND R. LIVGGOOD 1003
22
23
24
25
26
21
28
29
30
31
astrocytoma versus glioblastoma: The importance of histo- logic grade. Cancer (In press). Kopelson, G., Linggood. R.M., Kleinman, G.M., Doucette. J., Wang, C.C.: Management of intramedullary spinal cord tumors. Radiology 135: 473-479. 1980. Lee, F.: Radiation of infratentorial and supratentorial brainstem tumor. J. Neurosurg. 43: 65-68. 1975. Littman, P., Jarrett. P., Bilaniuk, L.T.. Rorke, L.B., Zim- merman. R.A. Bruce, D.A.. Carabell, SC., Schot. L.: Pediatric brainstem gliomas. Cancer 45: 2787-2792, 1980. Luccarelli, G.: Glioblastoma multiforme of the cerebellum: Description of three cases. .4cfa. Neurochirung. 53: lO7- 116. 1980.
Malis, l..l.: lntramedullary spinal cord tumors. C’lin. h’eu- rosurg. 25: 5 12~. 539. 1978.
Marsa. G.W., Geffinet, D.R., Rubinstein, L.J., Bagshaw, M.A.: Megavoltage irradiation of the treatment of gliomas of the brain and spinal cord. Cuncer 36: 1681-1689. 1975.
Miller. M.M., Mani. R.L.. Townsend, J.J.: Cerebellar glioblastoma in an adult. Surg. Neural. 5: 341-343, 1976.
O’Connell. .I.: The subarachnoid dissemination of spinal tumors. J. Neural. Neurosurg. Psych. 9: 55-62. 1946.
Onoyama, Y., Abe. M., Takahashi, M.. Yabumota. E.. Sakamoto. T.: Radiation therapy of brain tumors in chil- dren. Rudiology I IS: 6X7 693. 1975.
Ramsey. R.G., Brand, W.H.: Radiotherapy of glioblastoma multiformc. J. Ncurosurg. 39: 197-202, 1973.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
Riegel, D.H.. Scarff, T.B.. Woodford, G.: Biopsy of pediat- ric brainstem tumors. Child’s Brain 5: 329-340. 1979. Ryoo, M.C.. King, G.A.. Chung. C.T., Yu. W.S., Sager- man, R.H.: Irradiation of primary brainstem tumors. Radi- ology 131: 503-597, 1979. Salazar. O.M., Rubin. P.: The spread of glioblastoma multiforme as a determining factor in the radiation treated volume. Int J. Radiat. Oncol. Biol. Phj7.v. 1: 627~~631, 1976. Salazar, O.M., Rubin. P., McDonald, J.V., Feldstein. M.L.: Patterns of failure in intracranial astrocytoma after irradia- tion: Analysis of dose and field factors. ,4m. J. Radio/. 126: 279 292. 1976. Sheline. G.E.: Radiation therapy of primary tumors. Semin. Oncol. 2: 29-42. 1975. Sheline, C.E.: The importance of distinguishing tumor grade in malignant gliomas: Treatment and prognosis. /nt.- J. Radial. Oncol. Biol. Ph_vs. 1: 781 786, 1976. Stein. B.: Surgery of intramedullary spinal cord tumors. Clin ,Yeurosurg. 26: 529-542. 1979. Tibbs, P.A., Mortara. R.H.: Primary glioblastoma of the cerebellum. Acta. Neurochiruig 52: 13 18. 1980. Villani. R., Gaini, S.M., Tomei, G.: Follow-up study of brainstem tumors in children. Chilrl’.~ Brain I: 126-l 35. 1975. Yung. W.A.. Horten. B.C‘.. Shapiro. W.R.: Meningcal gliomatosis: A review of I2 casch. Anrr. .‘L’euro/. 8: 60 608. 1980.
ADDENDUM
experience, Salazar (Int. J. Rudiat. Oncol. Biol. Phi-s. 7:
166 I, I98 I ) continues to advocate elective craniospinal
In a recent update of the University of Rochester
axis irradiation for patients with cerebellar glioblastoma. However, perusal of the data presented reveals that the patients who received the elective craniospinal irradiation (with improved survival and no spinal cord failures claimed as a result of the neuraxis treatment), in fact had nlore aggressive treatment to the primary site (more generous regional fields and higher doses). In addition,
fields alone (usually to low doses) and who had failure in the spinal cord also failed at the primar~~ .ritcl: thus.
each of the patients who had been irradiated to small
re-seeding cannot be ruled out as the cause of spinal cord failures. Hence, the conclusions of the present paper are still advocated; i.e. generous regional fields (cncompass- ing known areas at risk for direct contiguous spread)
treated to appropriate doses n’ithout elective ncurrixis irradiation.