Embed Size (px)
Citation preview
Infrequently Performed Investigations in Nuclear Medicine
• A multitude of Radionuclide-basedinvestigations are being rarely performed inthe recent times
• This is owing either to the rarity of theindication or due to availability of tests whichare easier and/or more reliable
• Dacryoscintigraphy• Salivary gland scintigraphy• RBC survival studies• Blood volume estimation• Perchlorate discharge test• T3 suppression tests• Denatured RBC study• 99mTc – (V) – DMSA scintigraphy• LeVeen shunt scintigraphy• CSF shunt scintigraphy• Brain death scintigraphy
Dacryoscintigraphy
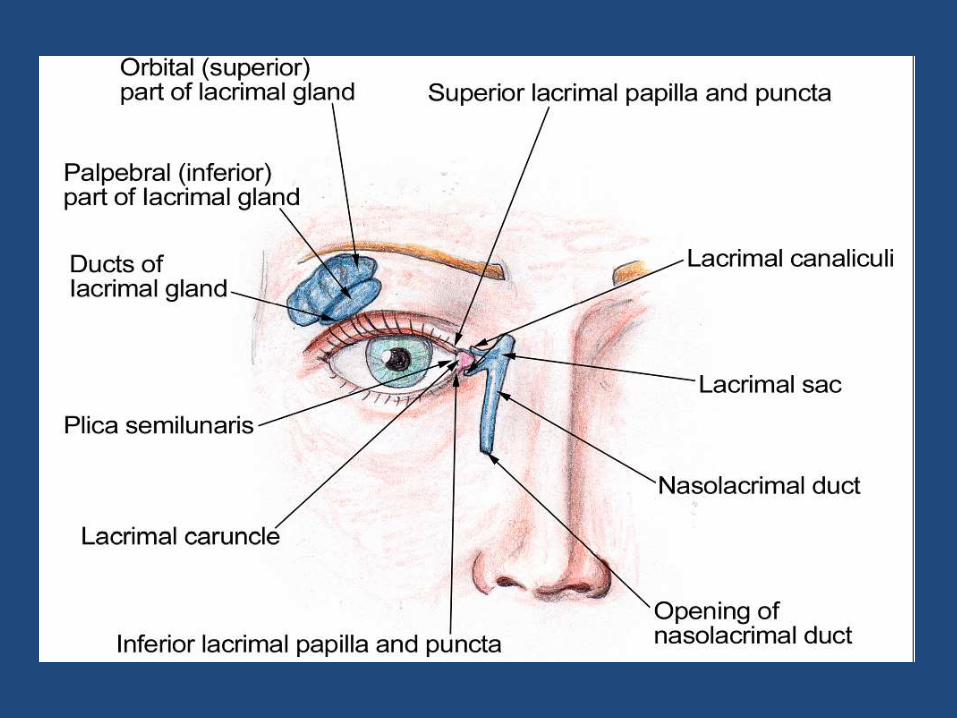
• Noninvasive, low-radiation-dose method ofevaluating the nasolacrimal drainage system
• Used to demonstrate patency of the system
• To preoperatively localize the area of obstruction
• Also can be used postoperatively to evaluatewhether the surgery was successful
• Patient must remove eyewear, including contact lenses, before starting the study
• 3.7 MBq(0.1 mCi) of 99mTcO4- administered per eye to the supine patient with an eyedropper or a needleless 1-mL tuberculin syringe
• Ensure that eyedrop administration is performed with care to prevent contaminationof the patient’s face
• Teary eyes: smear blot the tears
• Allow the tears to drain down the lateral aspectof the face
• Patient is placed in a sitting position for imaging
• Pinhole collimator (insert, 1–2 mm) or LEGP collimator with zoom may be used for acquisition
• dynamic imaging: use 10 s/frame for 1–2 minfollowed by 1 min/frame for 15–20 min
• Static imaging: 1-min image obtained immediately after the administration, followed by 1-min static images obtained at 5, 10, 15, and 20 min

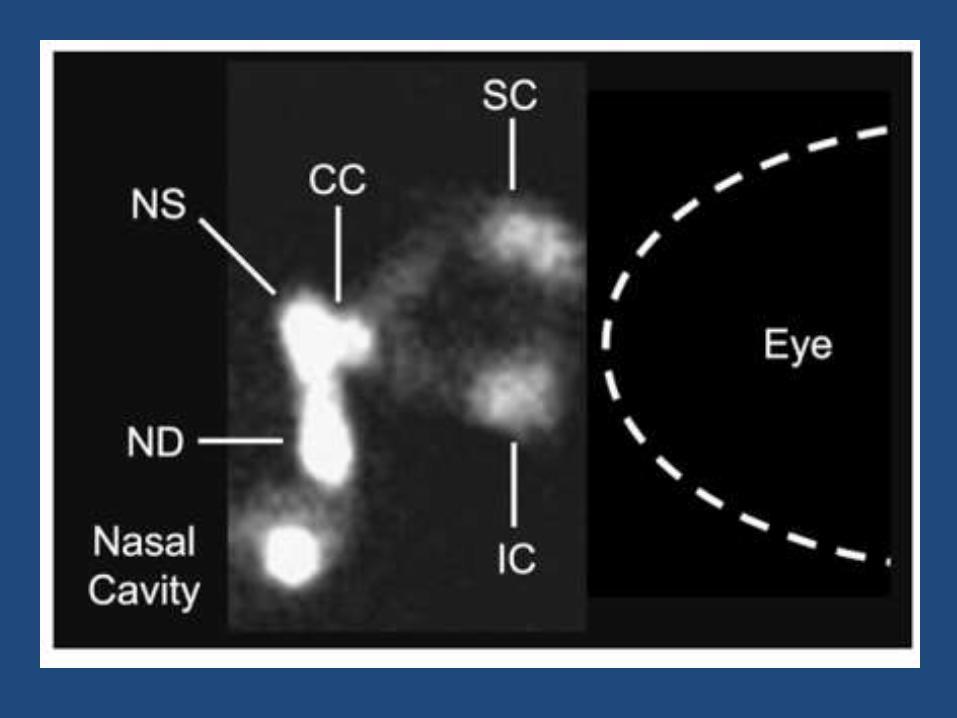
• Visualization of the nasolacrimal sac within 1 min
• drainage of activity from the nasolacrimal duct into the nasal cavity within 5 min/10-15 min
• one side should be compared with the other, rather than simply relying on quoted transit time values
• Evaluating both eyes simultaneously will bebetter for recognizing subtle differencesbetween the drainage of each eye
• When comparing one eye with the other, onemust assume that one eye is functioningnormally; however, bilateral obstruction ofvarying levels may exist

Dacryoscintigraphy: alternatives• Dye test
easy to perform, bedside
• Saccharin test
• Dacryocystography
Salivary gland scintigraphy
Indications:• Salivary gland function• Anatomic size and position of salivary glands• Salivary duct patency• Salivary gland tumors
Radiopharmaceutical: 99mTcO4-
Principle: ability of the glands to transport thepertechnetate from the surrounding blood supply intothe salivary glands through NIS
Procedure
• Preparation: stop NIS-inhibiting agents, such as iodide or perchlorate, for at least 48 h before the scan
• Position: supine, Water’s (chin and nose touching the collimator face)
• Dosage: 10 - 15 mCi administered IV
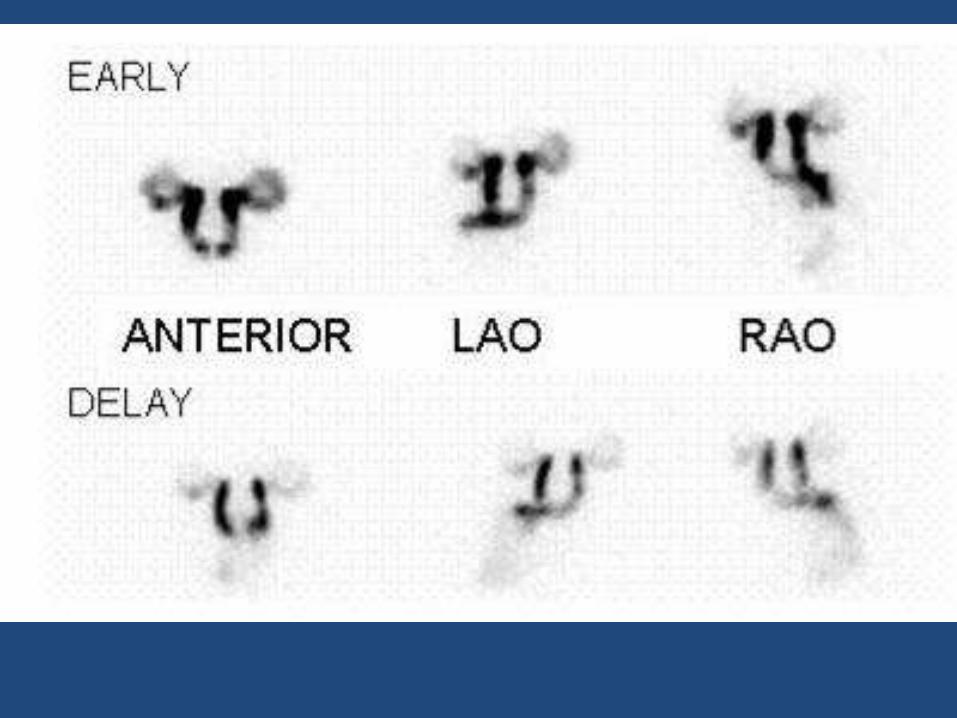
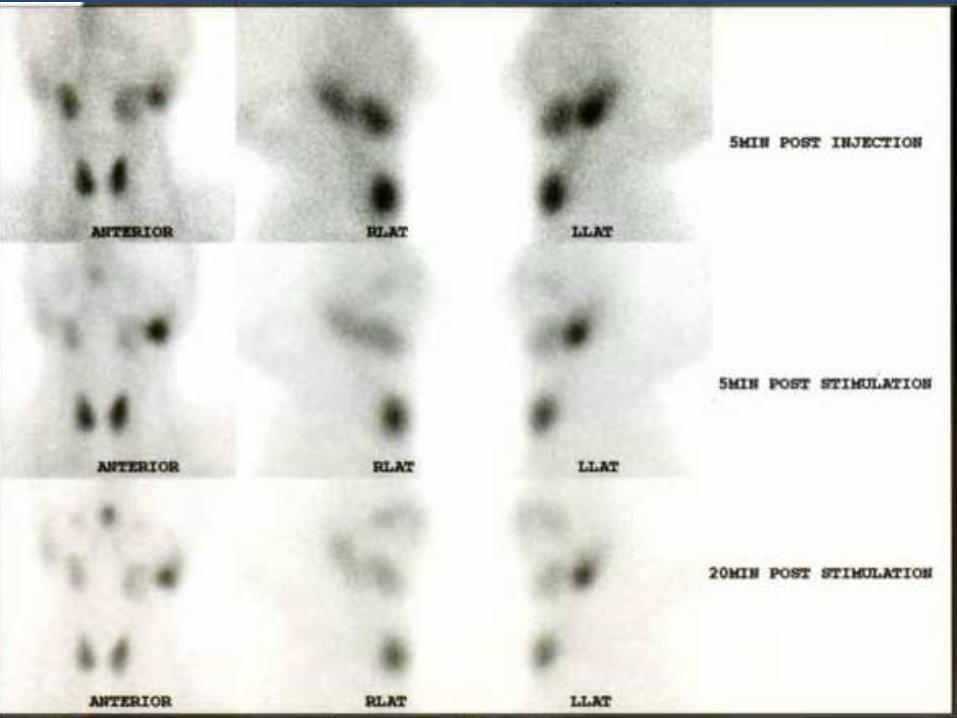
Pre-stimulus:
• Phase I (perfusion): performed immediatelyafter intravenous injection for 3–5 s/frame for1–2 min;
• Phase II (function/concentration): 20 min ofdynamic imaging for 2–3 min/frame
• Right and left lateral head images may then betaken for 500K

Stimulus (Phase III/washout):
• patient is asked to drink a mouthful of lemon juice via astraw and hold this in the oral cavity for a few secondsbefore swallowing
• Patient to be kept unaware about lemon juice to avoidpsychogenic stimulus
• Dynamic acquisition for 2–3 min/frame for 20 min
• Static images in lateral positions are acquired asneeded

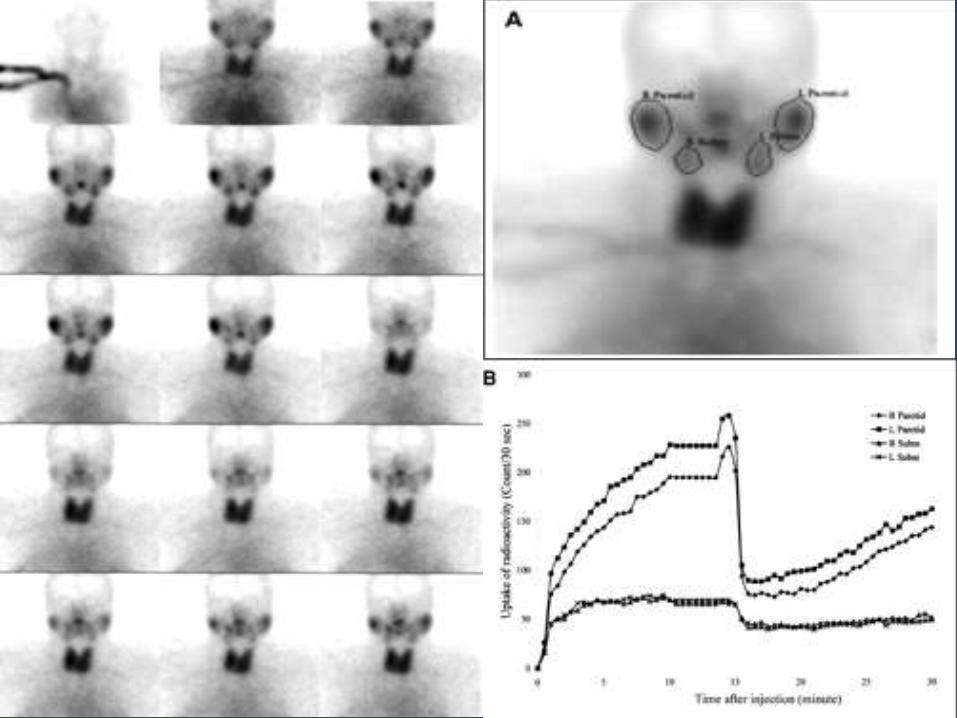
Interpretation
• Trapping of the 99mTcO4- should occur within 1 min of IVinjection in normal glands
• Peak activity occurs in the glands within 10 to 21 min
• During the prestimulus phase, an increase in uptake may bedue to local inflammation or infection (e.g. acutesialadenitis)
• Any gland activity remaining in the salivary gland afterstimulation is suggestive of obstruction, certain tumors,and inflammation
Uptake can be variable in chronic sialadenitis
Depends on the stage of chronic sialadenitis at the time of scintigraphy
• Focal adenitis
• Lymphocytic adenitis
• Sclerosing sialadenitis with sclerosis
• Progressive sclerosing sialadenitis with cirrhosis

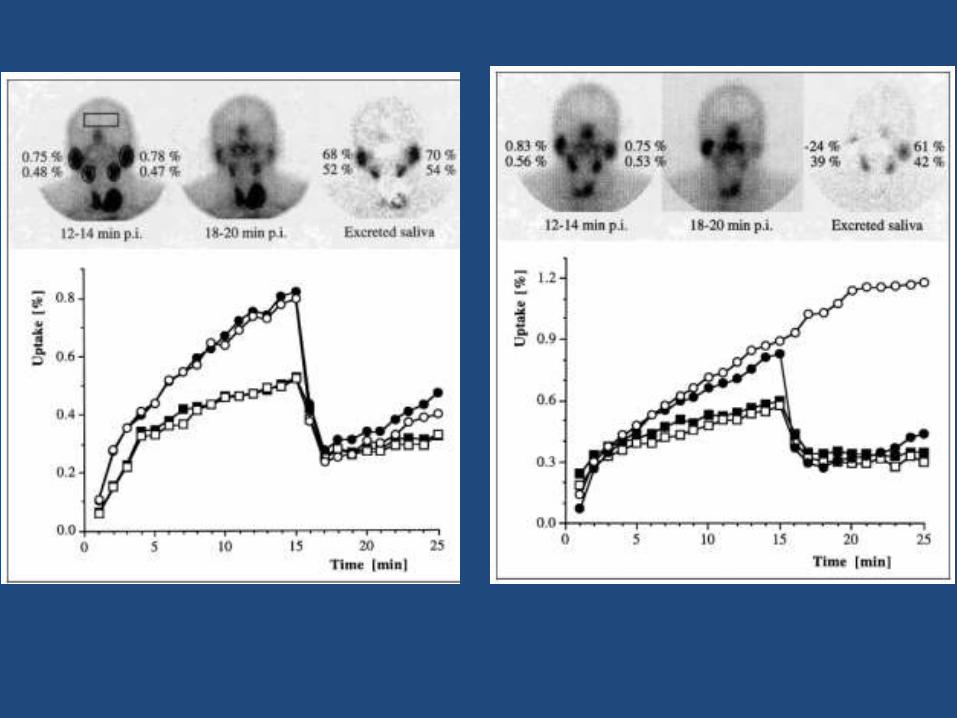
• Sjogren’s/sicca syndrome: Decreased uptakeand decreased excretion of the pertechnetatefrom the salivary glands
Other causes for reduced tracer uptake:
• Head and neck radiation therapy
• 131I therapy in thyroid cancer

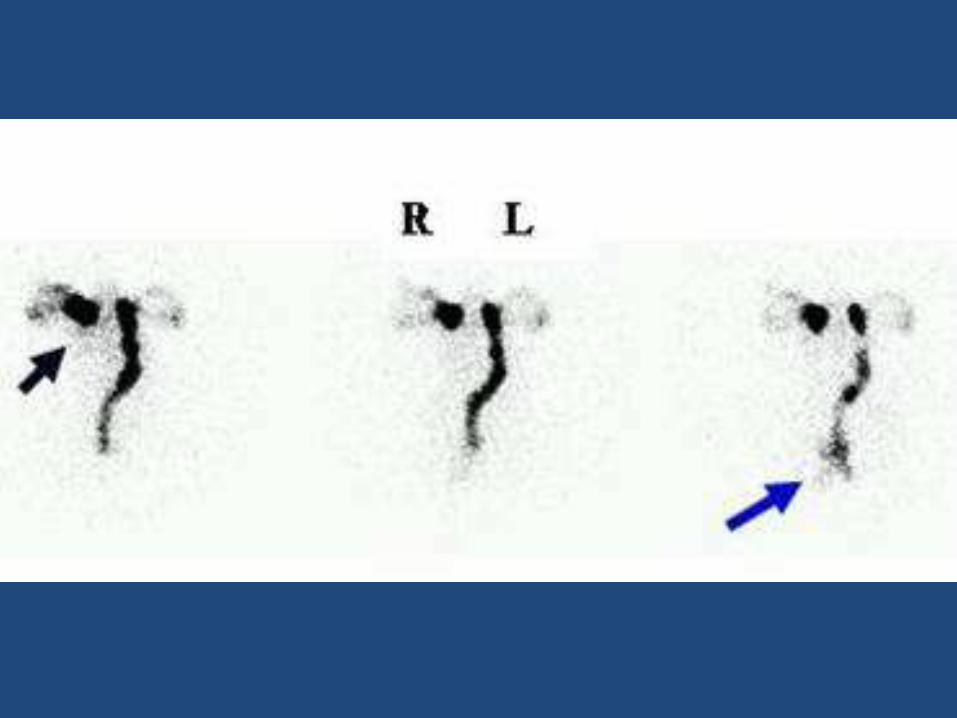
STIMULUS STIMULUS
NORMAL SJOGREN’S SYNDROME
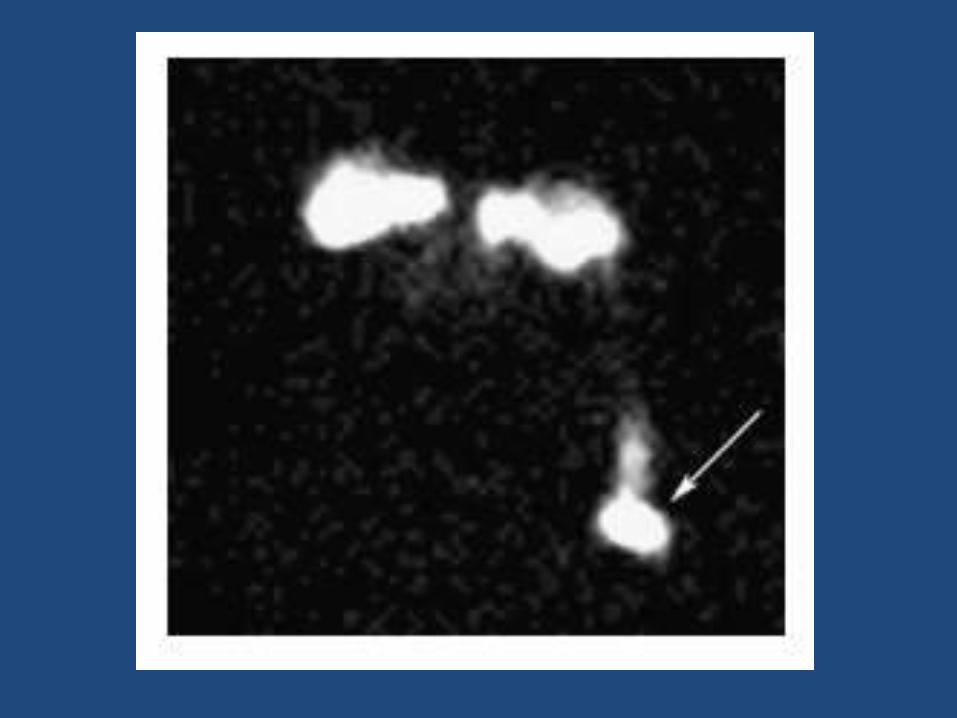
Salivary scintigraphy in tumors
• All salivary gland tumors produce a ‘cold defect’ on salivary gland scintigraphy
• An exception is adenolymphoma (Warthin’stumor) which produced a ‘hot spot’ when subjected to salivary scintigraphy
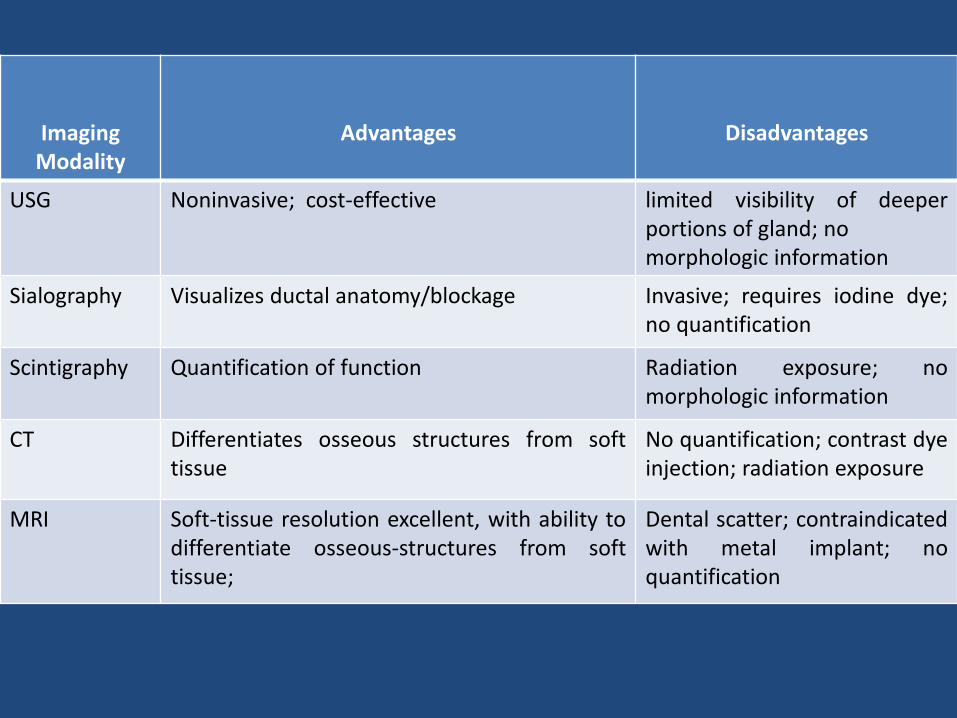
Imaging Modality
Advantages Disadvantages
USG Noninvasive; cost-effective limited visibility of deeperportions of gland; nomorphologic information
Sialography Visualizes ductal anatomy/blockage Invasive; requires iodine dye;no quantification
Scintigraphy Quantification of function Radiation exposure; nomorphologic information
CT Differentiates osseous structures from softtissue
No quantification; contrast dyeinjection; radiation exposure
MRI Soft-tissue resolution excellent, with ability todifferentiate osseous-structures from softtissue;
Dental scatter; contraindicatedwith metal implant; noquantification
Red cell survival study
• The use of 51Cr-labeled red blood cells can be used to determine erythrocyte survival in circulation
• can provide important data in cases of anemia in which increased haemolysis is suspected but not clearly demonstrated by other tests
• An accurate study can positively identify hemolytic anemia, a disorder characterized by premature destruction of erythrocytes
• Radioactive chromium (51Cr) is a γ-ray emitter (280keV,9% abundance) with a half-life of 27.8 days
• As a red cell label, hexavalent sodium chromate is used
• To facilitate passing into the RBC, it is reduced to thetrivalent form, preferentially to the β-chains of Hb
• In this form, it is not reutilised nor transferred to othercells in the circulation
Radio-labeling RBC with Cr-51
• Approximately 10 ml of blood to 1.5 ml of sterile acid–citrate–dextrose (ACD) solution in a sterile bottle with ascrew cap
• Centrifuge at 1200-1500 g for 5 min, discard thesupernatant plasma and buffy layer
• With continuous mixing, add to the cells 8 kBq/kg of Na251CrO4.
• Incubate for 15 mins at 37 degC
• Add 100 mg ascorbic acid and incubate for another 5 mins
• 0.02 MBq per kg body weight (an average total dose of2 MBq) is recommended
• If the study is to be combined with a spleen scan, ahigher dose (4 MBq) should be used
• After injection, allow the labeled cells to circulate inthe recipient for 10 min
• Can be extended to 60 min in pts with CCF orsplenomegaly, in whom in vivo tagging may be delayed
• Then collect a sample of blood from a vein otherthan that used for the injection, and mix withEDTA as anticoagulant
• The radioactivity in this sample provides abaseline for subsequent observations
• Retain part of the labelled cell suspension thatwas not injected into the patient to serve as astandard (enables the blood volume to becalculation)
• Take further 4-5 ml blood samples from the patient 24 hours later and subsequently at intervals (thrice a week for first 2 weeks, twice a week thereafter)
• Measurements should be continued until at least half the radioactivity has disappeared from the circulation
• Measurements to be carried out in a scintillation counter
• Estimate the percentage survival (of 51Cr) on any day using the formula:
• RBC survival on day t =cpm/ml on day t x 100
cpm/ml on day 0
Pitfalls
Two processes inherent to the technique hinder accurate red cell survival estimation:
• 51Cr-labelled cells are lost from the circulation by lysis, phagocytosis, or haemorrhage
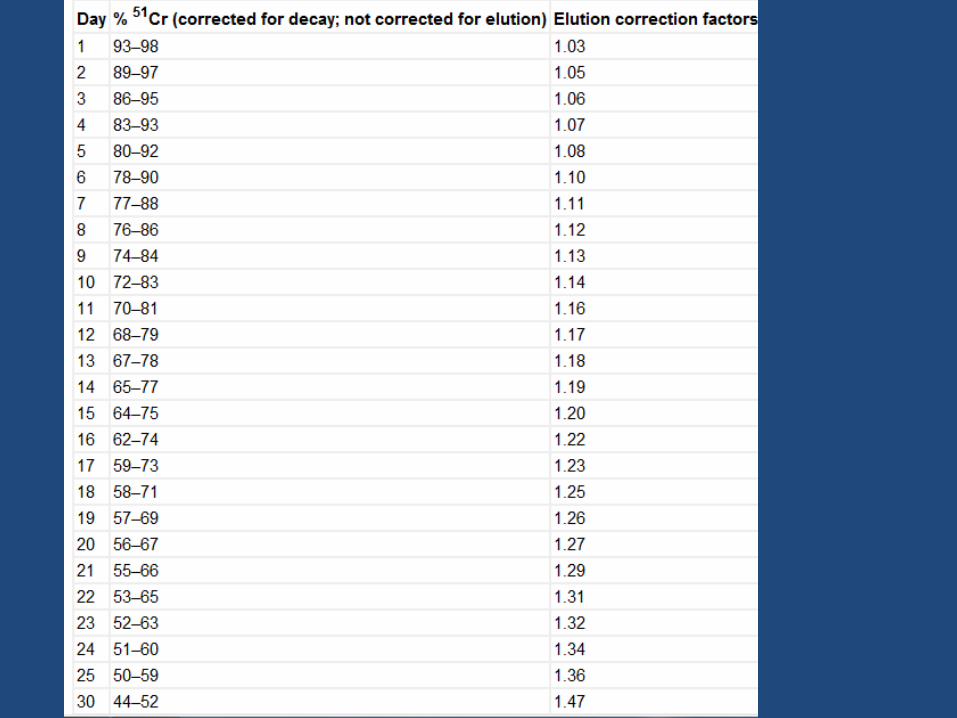
• 51Cr is eluted from intact red cells that still circulate
Correction for lysis
• Up to 10% of the 51Cr may be lost within the first 24 hours
• If this major loss does not continue beyond the first 2 days, it is often looked on as an artefact
• It is common practice to calculate the T50Cr (i.e., the time taken for the concentration of 51Cr in the blood to fall to 50% of its initial value) after correcting the data for physical decay
• The mean value of T50 in normal subjects is 30 days, with a range of 25-33 days
Advantages
• Other methods for evaluating hemolyticanemia (direct antiglobulin test and the G6PDenzyme screen) are not definitive forhemolysis
• 51Cr red cell survival study, in addition toassessing mean life-span of RBC, can also giveinformation about the site of hemolysis ifcombined with imaging the patient under agamma camera

Disadvantages
• Laborious and time-consuming
• Repeated measurements in the same pt are not possible owing to:
(1) long residence time
(2) multiple venipunctures for a single test
(3) compromised reproducibility in case a repeat study is opted for (owing to background counts)

51Cr – RBC blood volume estimation
• Chromium-51 labelled RBC can also be used to estimate the blood volume of an individual
• The long t1/2 of 51Cr isotope (27.8 days) is made use of to estimate this parameter
• The estimation is based on dilution principle
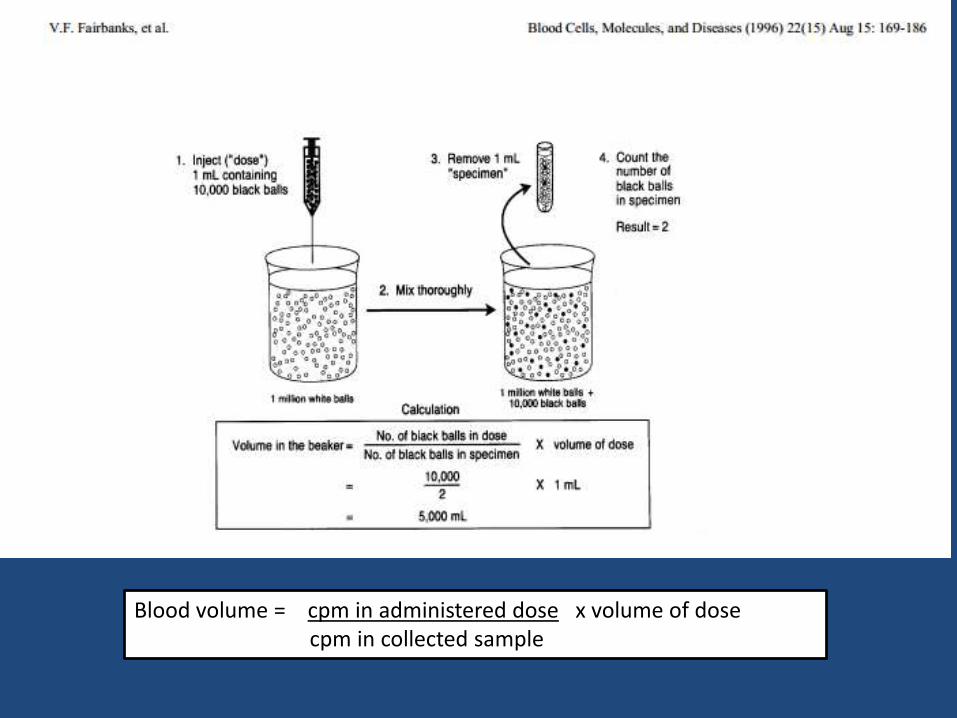
Blood volume = cpm in administered dose x volume of dose cpm in collected sample
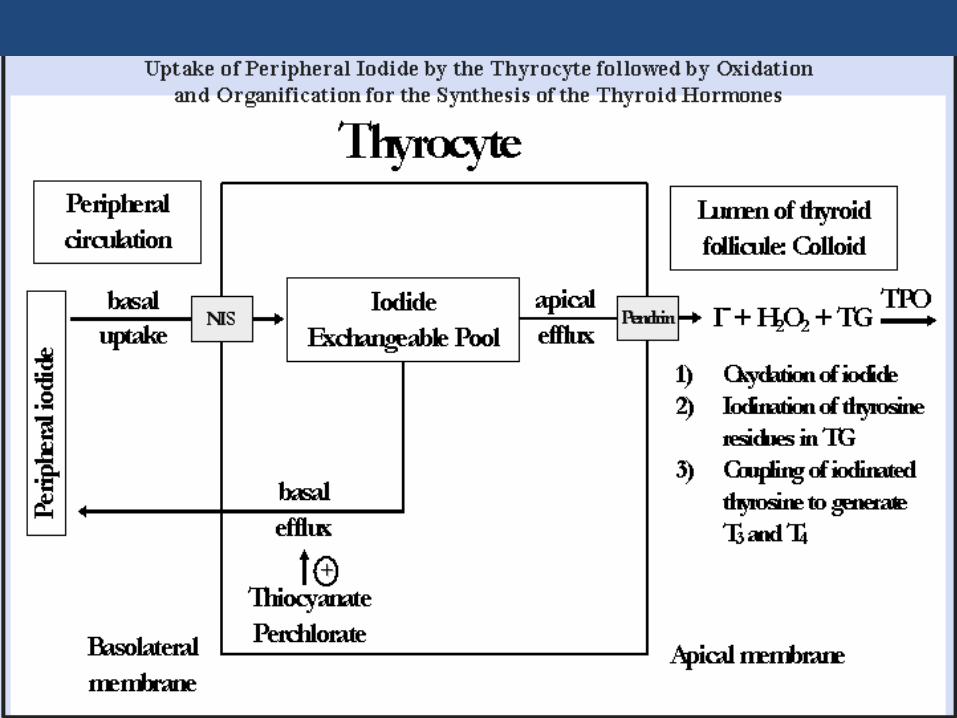
Perchlorate discharge test
• In normal subjects, the administration ofperchlorate blocks the continuedaccumulation of radioiodide by the thyroidbut causes virtually no release of previouslyaccumulated radioiodide from the gland
• In patients with an I- organification defect,administration of the ClO4- results in therelease of I- from the thyroid
Conditions with trapping-organificationdissociation:
• Congenital: Pendred syndrome
enzyme defect in TPO
• Acquired: chronic thyroiditis
therapy with ATD
Protocol
• The patient receives 10 µCi 131I for RAIU measurement
• %RAIU measured at 1 – 2 hours (Ui)
• 300 mg potassium perchlorate administered per orally
• %RAIU measured after one hour (Uf)
• %washout is estimated using the formula:
• Ui – Uf x 100
Ui
• If %washout > 10%, the test is considered positive, and is suggestive of organificationdefect
T3 suppression test
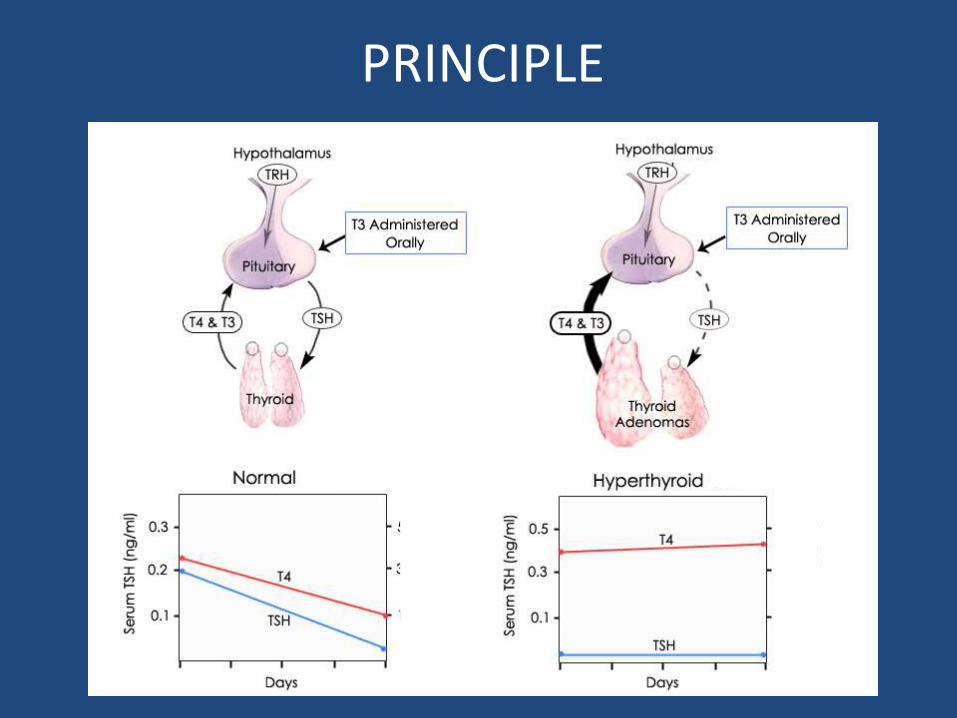
Principle
• Inhibition of pituitary TSH secretion by highcirculating concentrations of thyroid hormone(T3/T4) is a characteristic feature of normalhypothalamic-pituitary-thyroid regulation
• In contrast to the situation in normal patients,when thyroid function is autonomous,administration of large doses of exogenous T3/T4has little or no effect on T4 secretion
Indications:
• To confirm the presence of autonomousthyroid function in patients with borderlineclinical and laboratory findings ofhyperthyroidism
• To rule out central hyperthyroidism due toTSH-oma
PRINCIPLE
Protocol
• A baseline 24-hour uptake is obtained
• The patient then receives 25 mcg of T3 (liothyronine) four times a day for 8 days
• The 24-hour uptake is repeated beginning on day 7
• Normal: <50% suppression compared to baseline RAIU
<10% suppression overall
• Abnormal test result: confirms autonomy of thyroid gland in causing hyperthyroidism
rules out TSH-omas
Disadvantages
• Long duration of study hinders timely approachof diagnosis
• Thyrotoxicosis caused by exogenous hormoneadministration can lead to symptoms that maycause discomfort to the patients
• Strictly contraindicated in elderly patients orthose with coronary heart disease

Denatured RBC study
Principle:• Normal RBCs are deformable and pass readily through the spleen
• However, when heated, RBCs undergo fragmentation andspherocytosis -> increased stiffness -> entrapment by the spleen
• Heat-damaged, or heat-denatured, RBC labelled with 99mTcO4- areused
• Used to assess for the presence and location of splenic tissue
Indications:
• Identify accessory splenic tissue (splenunculi) postsplenectomy/thrombocytopenia/splenic trauma
• Assess whether a mass found on anatomic imaging,such as CT, is a splenunculus
• Assess congenital abnormalities of number (asplenia orpolysplenia) or location of spleen(wandering spleen)
• In vitro labeling of the patient’s RBCs with 1–3 mCi of 99mTcO4-
• Labeled RBCs then heated in a water bath at 49.5°C ± 0.5°C for 20 min
• Overheating -> excessive damage of the RBCs -> increased uptake by the liver and decreased uptake by splenic tissue
• Underheating -> insufficient damage of the RBCs -> decreased splenic uptake -> increased activity in the circulating blood pool
• Because of the rapid splenic sequestration of the damaged RBCs, imaging can begin 30 min after injection
• Planar and SPECT scans should be performed
• When the study is a search for accessory splenic tissue, the entire abdomen must be imaged
• h/o prior trauma: if there is h/o violation of diaphragm, imaging of thorax should also be done for splenic implants
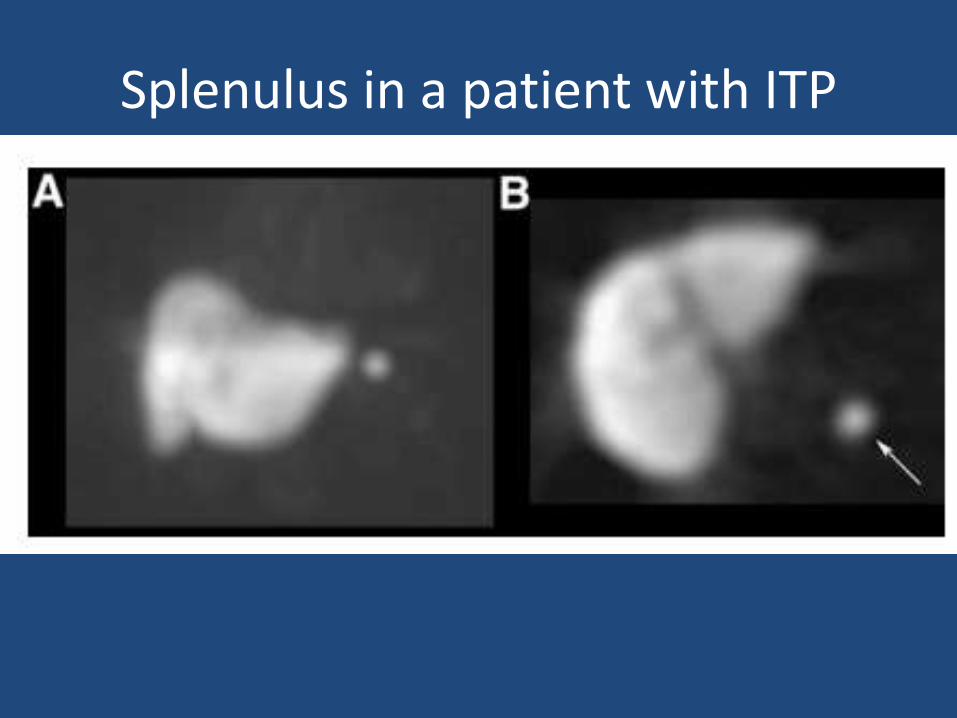
Splenulus in a patient with ITP
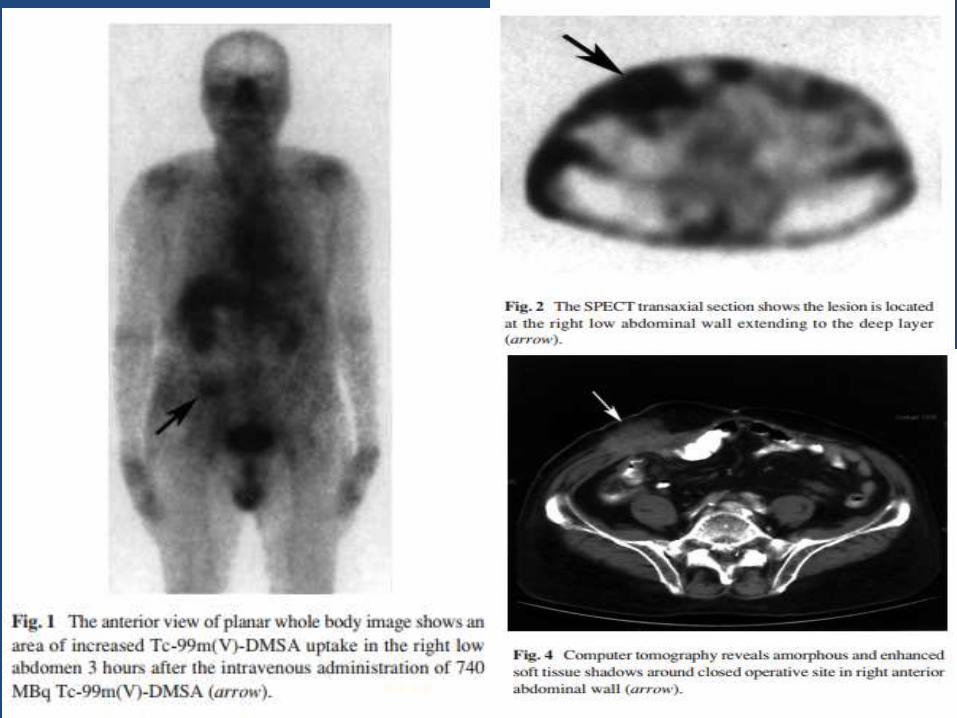
99mTc –(V) –DMSA scintigraphy
• Two different forms of 99mTc – DMSA find application in nuclear medicine
99mTc – (III) – DMSA : • acidic pH (2.5)• binds to renal tubuli99mTc – (V) – DMSA : • alkaline pH (7.5 - 8)• binds to bone and tissues with calcification• tumor-imaging agent (MTC, HNSCC, HCC, OS, GBM)• Inflammation imaging: IBD, surgical wound site
infections
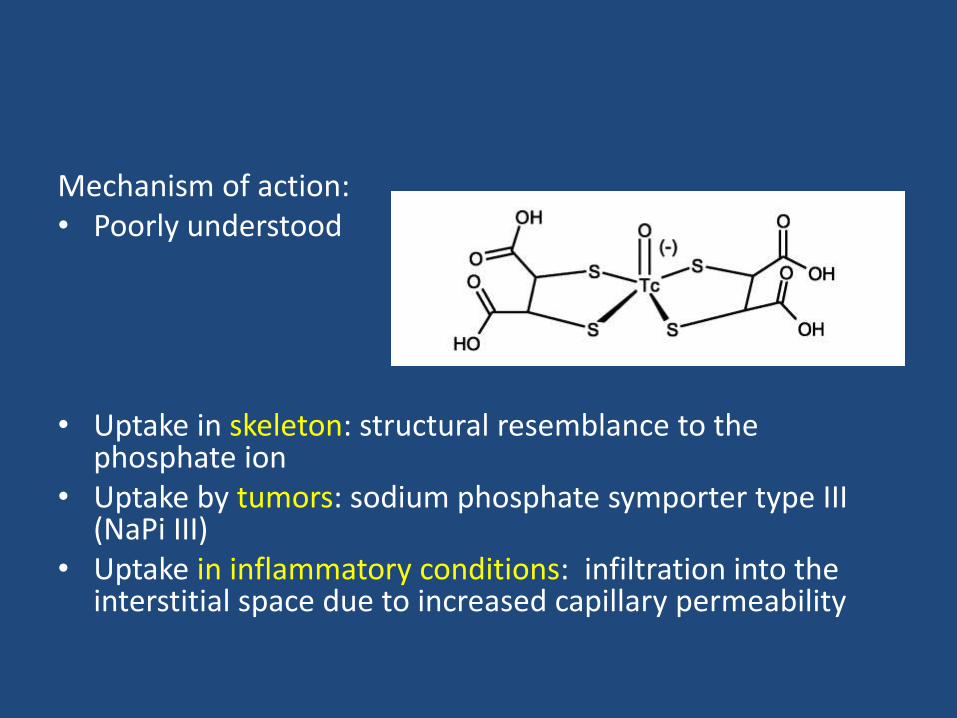
Mechanism of action:• Poorly understood
• Uptake in skeleton: structural resemblance to the phosphate ion
• Uptake by tumors: sodium phosphate symporter type III (NaPi III)
• Uptake in inflammatory conditions: infiltration into the interstitial space due to increased capillary permeability
Protocol
Dosage: 15 – 20 mCi (IV)
Static images to be acquired 2 – 4 hrs following injection
Images to be acquired on a gamma camera with LEHR collimators
Lateral views and SPECT/CT help in better anatomical localization

Bandopadhyay et al, ISRN Oncol. 2012

Bandopadhyay et al, ISRN Oncol. 2012
Disadvanatages
• The mechanism of action is speculative and is still poorly understood
• Imaging with radiotracers such as 131I – MIBG and radiolabeled SSTR analogs, which carry better sensitivity and specificity, have rendered 99mTc – (V) – DMSA scan obsolete
LeVeen shunt scintigraphy
• The LeVeen shunt, introduced in the 1970s, was designed to help manage patients with chronic ascites
• a peritoneovenous shunt, intended to drain the ascites into the venous system
• surgically placed in the peritoneal cavity and has a 1-way valve that connects into the patient’s jugular vein, which then empties into the superior vena cava
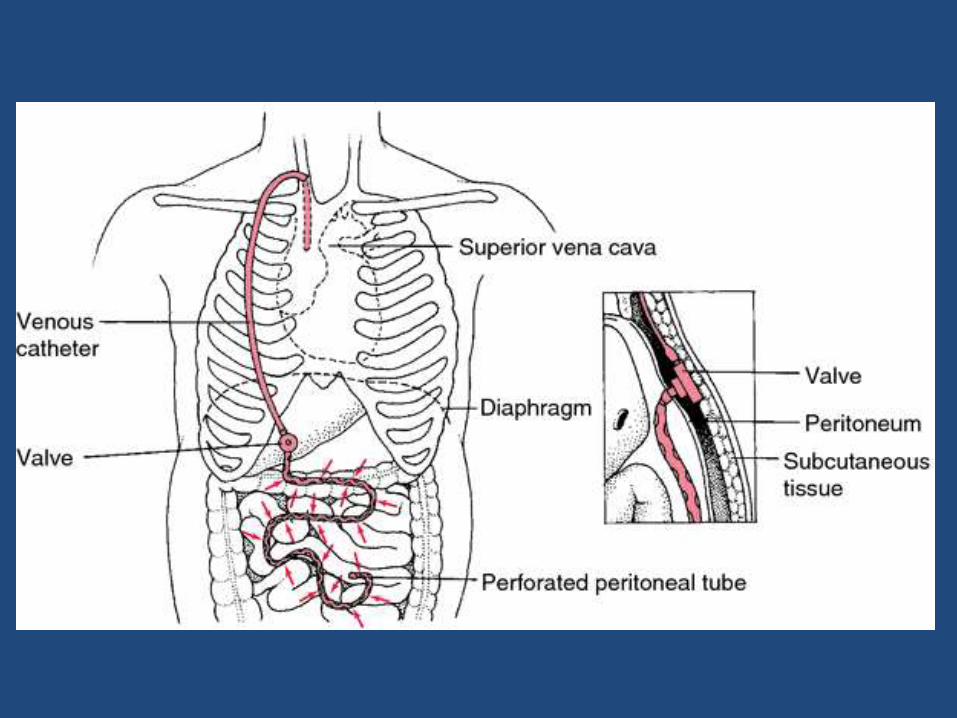
• A mechanical obstruction (by a valve malfunction or a thrombosis of the shunt tubing) can cause ascites accumulation despite a shunt in-situ
• LeVeen shunt study helps to identify whether the shunt is patent and rule out a mechanical obstruction
• A sensitivity of 100% and a specificity of 92.2%for detecting shunt patency

LeVeen shunt study: procedure
• No preparation is necessary
• Following local anaesthesia, an intraperitoneal injection of 185MBq (5 mCi) of 99mTc-MAA
• 99mTc sulfur colloid may also be used; however, not the preferred radiopharmaceutical because of the difficulty in discerning liver in the presence of radioactive ascitis
• After injection, the patient should be instructed to roll from one side to the other, which will facilitate mixing of the radioactive injection with the ascitic fluid

• Static images of the abdomen and chest are obtained at 15, 30, 45, and 60 min (upto 4 hours if required) after injection
• An appropriate injection is suggested by widespread accumulation of the radioactivity in the abdomen initially

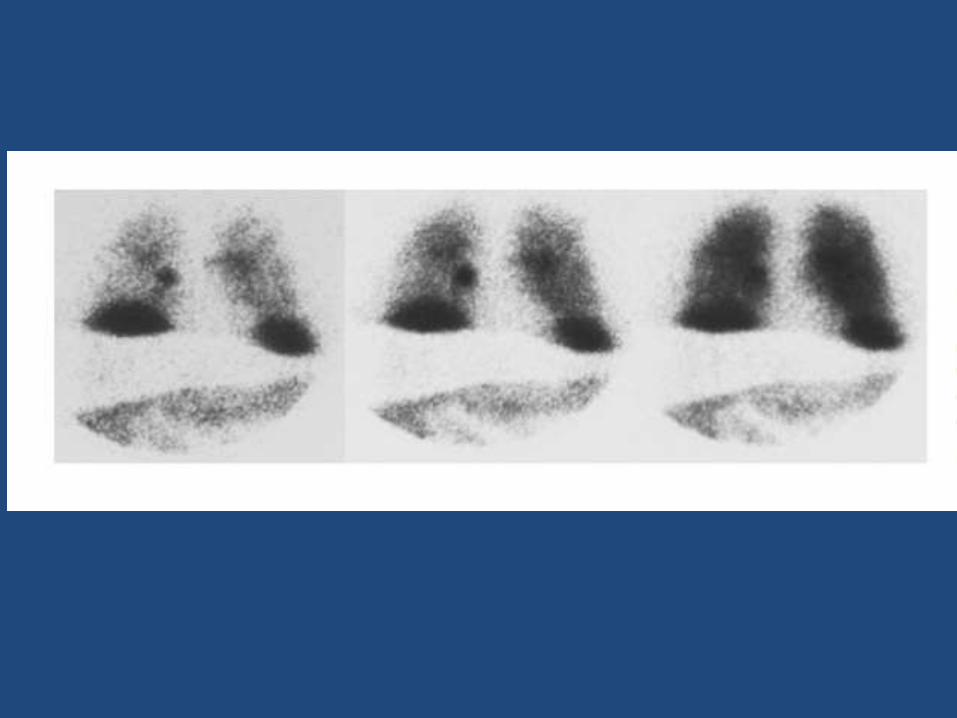
• When the LeVeen shunt is functional, the injected 99mTc MAA travels to the lungs and lodges in the capillaries
• The lungs should become visualized within 1 hour following injection (may occur as early as 10 min)
• Shunt tubing may or may not be visualized; depends on the radiotracer (greater with 99mTc MAA) and flow rate (better seen at intermediate flow: 60 mL/hr )
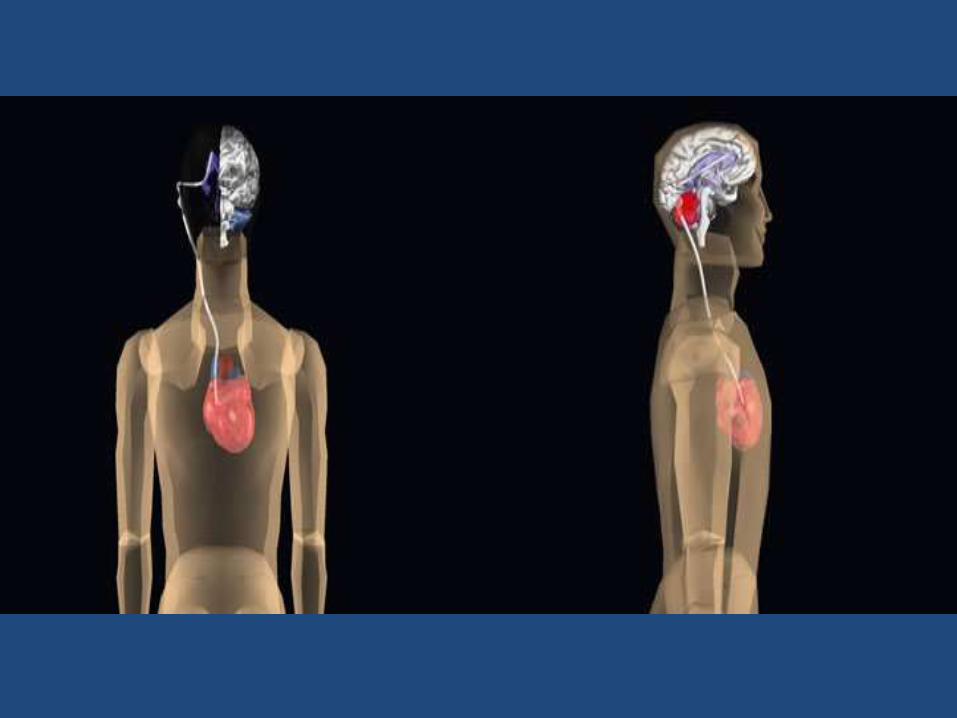
CSF shunt scintigraphy
• CSF shunts are inserted to treat the symptoms of hydrocephalus
• ventriculoperitoneal shunt (ventricle to peritoneal cavity)
• ventriculoatrial shunt (ventricle to right atrium)
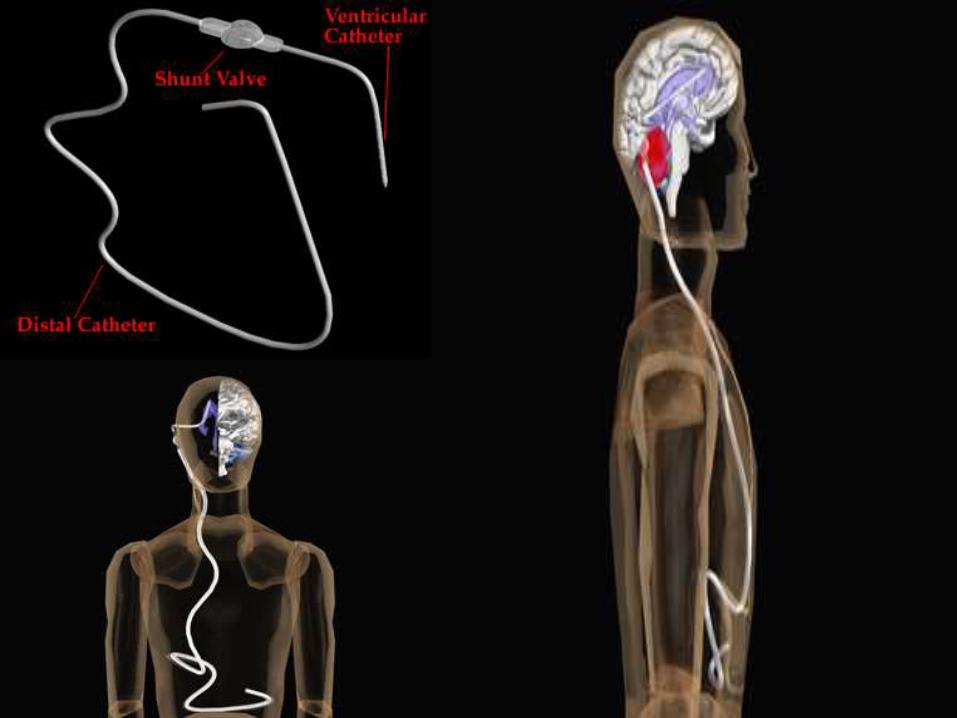

• A malfunctioning shunt may be caused by a mechanical issue such as disconnection or kinking of the shunt tubing
• Also, shunt obstructions may be caused by occlusion of the tip of the tubing by the omentum in the peritoneal cavity or emboli in the shunt tubing
• CSF shunt scan is used to determine whether the shunt is patent and to exclude shunt obstruction

Procedure
• Radiopharmaceuticals: 99mTc DTPA99mTc TcO4-111In DTPA
• 99mTc tracers prefered
• Recommended dose: 18.5 MBq (0.5 mCi)
• Volume: 0.3 – 0.5 mL (to ensure minimal disruption of the normal CSF flow physiology)
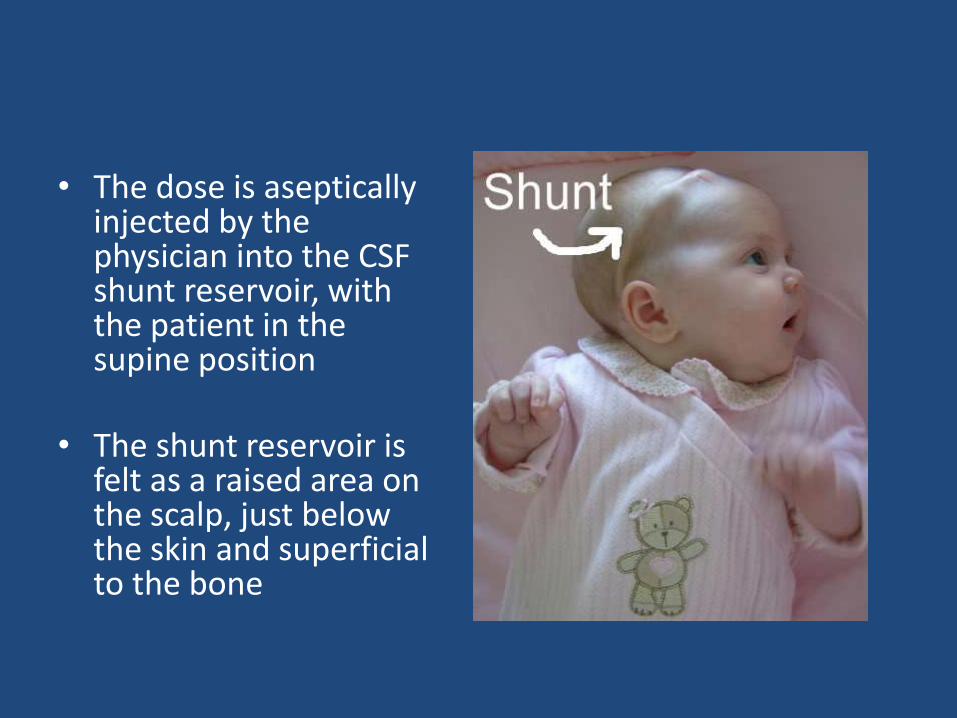
• The dose is aseptically injected by the physician into the CSF shunt reservoir, with the patient in the supine position
• The shunt reservoir is felt as a raised area on the scalp, just below the skin and superficial to the bone
• First measure the CSF opening pressure using a manometer on accessing the reservoir
• Once the opening pressure has been measured, the radiopharmaceutical is injected
• Immediately after injection, the patient is imaged in the supine position
• Include the injection site at the shunt reservoir to the location of the end tip of the distal tubing of the shunt
• Dynamic imaging at a rate of 1 min/frame


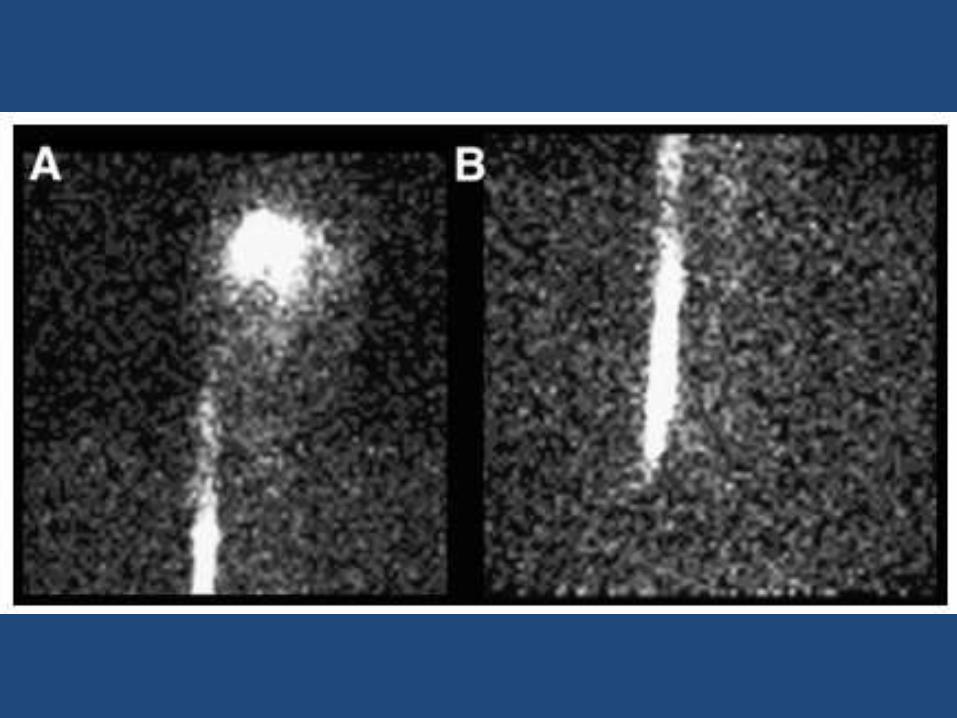
• Manually occluding the distal limb of the tubing where it leaves the reservoir: assessing patency of the proximal limb of the tubing
• Reflux of a portion of the radiotracer into the ventricles confirms patency of the proximal limb of the shunt
• Absence of reflux: doesn’t always imply occlusion in the proximal limb (presence of flap valve, )
Brain Death Scintigraphy
• Brain death is defined slightly differently by various organizations, but the overlying concept is of complete and irreversible loss of function of the brain.
• The term is usually applied in the context of continued function of other organ systems, such as the cardiovascular system
• An accurate and timely determination of braindeath is necessary to best address the griefand anxiety of family members and to allowtimely assessment for possible organ donation
• A nuclear medicine brain death study is asimple and minimally invasive test that mayassist in the diagnosis of brain death byassessing brain blood flow

2 approaches
• 99mTc-DTPA: non-brain-specific perfusion agent; does not cross BBB
• 99mTc-HMPAO or 99mTc-ECD: lipophilic agents
Procedure
Preparation:
• Ensure adequate ventilation (hyperventilation can lead to reduced CBF)
• Tourniquet around head: at the level of eyebrows, to diminish interference from scalp blood flow
Position:
• under a LEHR collimator
• Field of view to include carotids to skull vertex
• Camera anterior and parallel to the patient’s face
DTPA SCINTIGRAPHY
• Dynamic phase: study should be performed after intravenous injection, with 1–3 s/frame for at least 60 s (can be extended upto 5 min)
• Static phase: for a minimum of 5 min/view in the anterior, left, and right lateral positions
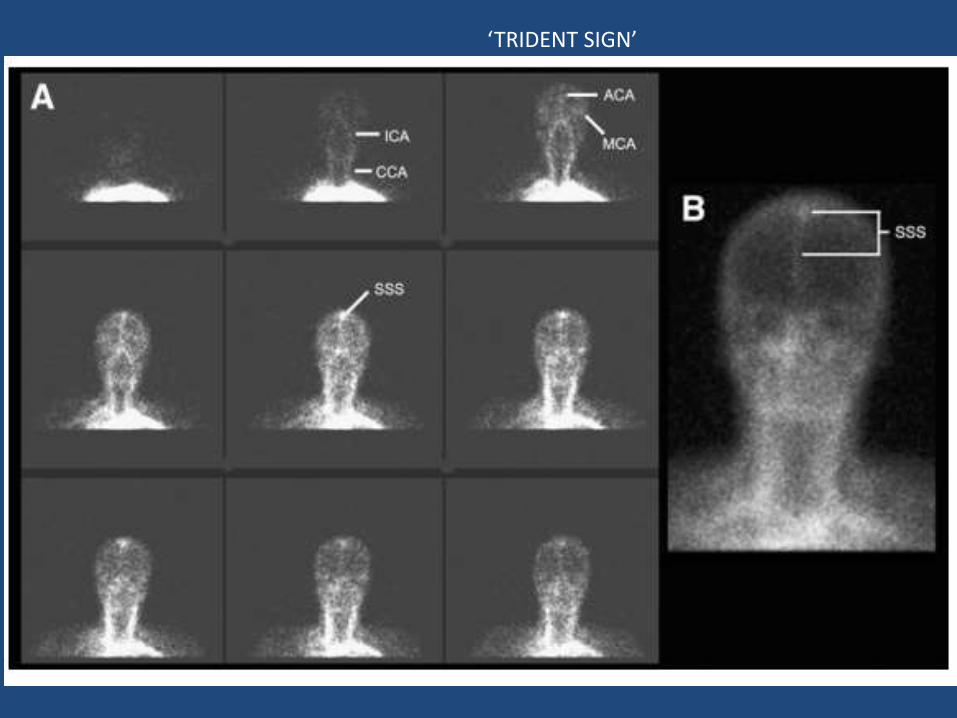
‘TRIDENT SIGN’

• In a positive brain-death study, theradiopharmaceutical bolus goes through thecommon carotid arteries but stops at the base ofthe skull
• Brain death results in raised intracranial pressurethat exceeds the cerebral perfusion pressuresupplied by the ICA
• However, flow to the ECA, which supplies the faceand scalp, persists and may even be elevated,often leading to the ‘‘hot-nose sign’’
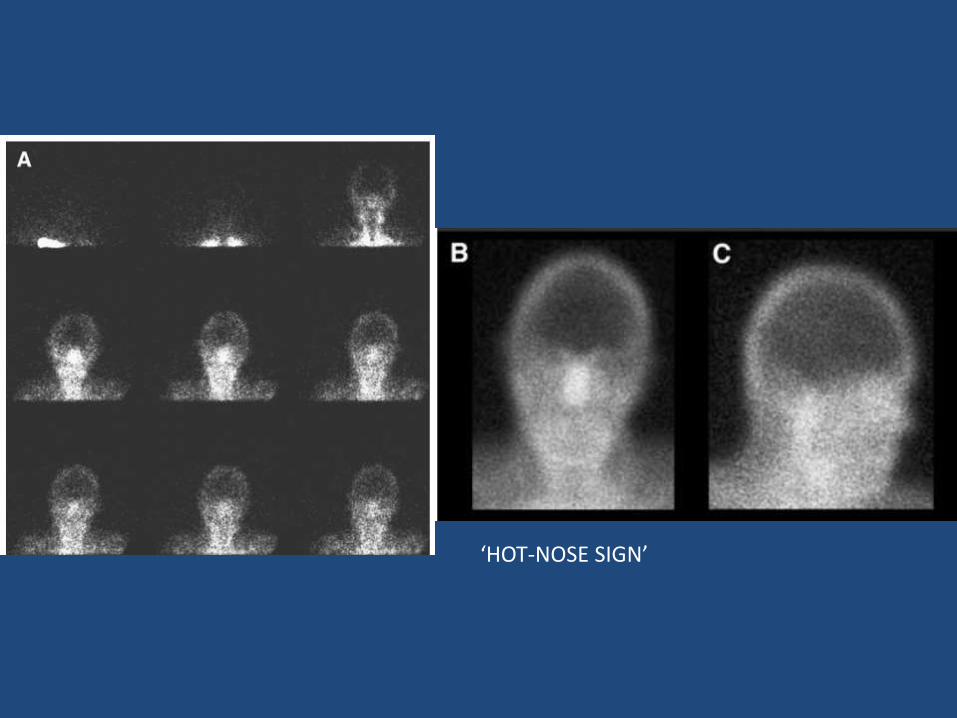
‘HOT-NOSE SIGN’
HMPAO/ECD SCINTIGRAPHY
99mTc – HMPAO or ECD, being brain-specific agents, are usually preferred for the following reasons:
• Delayed imaging is sufficient to assess cerebral blood flow
• Not dependent on a good bolus IV injection
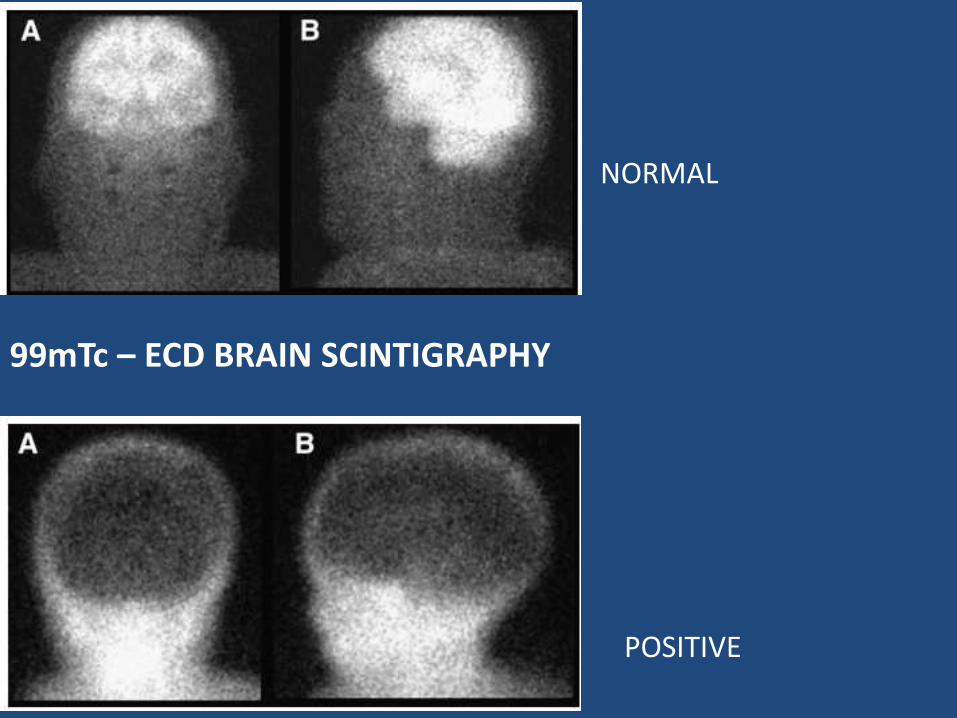
99mTc – ECD BRAIN SCINTIGRAPHY
NORMAL
POSITIVE
Drawbacks
• Does not adequately image the vasculature the posterior fossa
• Any temporary causes for cerebral edema (hepatic encephalopathy, acute intracranial hypertension) can lead to a false positive result
Alternatives
Angiography:
• Invasive
• Idiosyncratic reaction to IV contrast can lead to renal failure
Transcranial US doppler
MR angiography
Yet to be sufficiently validated

THANK YOU









![Determination of optimal location for installation of symmetry … · established GOST 32144 – 2013 values [3]. Following performed investigations, there is sufficiently high level](https://img.pdfslide.net/doc/110x75/5f89ce1ff104fd3c1c2b9c6a/determination-of-optimal-location-for-installation-of-symmetry-established-gost.jpg)








![Numerical Investigations on Fluid Flow through Metal Screens · NUMERICAL INVESTIGATIONS ON FLUID FLOW THROUGH METAL SCREENS 5 et al. [1] performed calculations on screens used in](https://img.pdfslide.net/doc/110x75/5e288afacf173c3dbe461046/numerical-investigations-on-fluid-flow-through-metal-screens-numerical-investigations.jpg)