-
8/15/2019 inhalan kortikosteroid
1/7
MiniReview
Use of Inhaled and Oral Corticosteroids in Pregnancy andthe Risk
of Malformations or Miscarriage
Anne-Mette Bay Bjørn1, Vera Ehrenstein2, Ellen Aagaard Nohr3 and
Mette Nørgaard2
1Department of Gynecology and Obstetrics, Aarhus University
Hospital Skejby, Aarhus N, Denmark, 2Department of Clinical
Epidemiology,
Aarhus University Hospital, Aarhus, Denmark and 3Research
Unit for Gynecology and Obstetrics, Institute for Clinical
Research, University of
Southern Denmark, Odense, Denmark
(Received 23 January 2014; Accepted 8 December 2014)
Abstract: Corticosteroids are potent
anti-inflammatory and immunosuppressive drugs, which sometimes must
be given to preg-nant women. Corticosteroids have been suspected to
be teratogenic for many years; however, there is conflicting
evidenceregarding the association. Based on a literature review of
three databases, this MiniReview provides an overview of inhaled
andoral corticosteroid use in pregnancy with specific emphasis on
the association between use of corticosteroids during pregnancy
and risk of miscarriage and congenital malformations in
offspring. The use of corticosteroids among pregnant women
rangedfrom 0.2% to 10% and increased nearly two times in recent
years. Taken together, the evidence suggests that the use of
corticos-teroids in early pregnancy is not associated with an
increased risk of congenital malformations overall or oral clefts
in offspring;at the same time, published estimates are
inconsistent. The use of inhaled corticosteroids was associated
with a slightly increasedrisk of miscarriage, whereas the use of
oral corticosteroids was not; however, confounding by indication
could not be ruled out.
Because of their anti-inflammatory and immunosuppressive
properties, corticosteroids are widely used to treat many
medi-
cal conditions, including asthma, rheumatoid arthritis,
eczema
and inflammatory bowel disease [1]. Cortisol, the naturally
occurring corticosteroid, exerts a range of
physiologicaleffects, including regulation of pathways in fat,
protein and
carbohydrate metabolism, cardiovascular function, growth and
immunity [2]. Synthetic corticosteroids act similarly to
corti-
sol: they bind to the same intracellular receptor proteins,
although most of the synthetic corticosteroids have
stronger
affinity (e.g. prednisolone’s potency is 5:1 as compared to
cor-
tisol; for dexamethasone, the potency is 30:1) [2].
Speculations about teratogenicity of corticosteroids arose
in
1951 because of the finding that treatment of pregnant mice
with corticosteroids caused cleft palate in the offspring
[3].
Concerns arose that corticosteroids could lead to more
severe
adverse pregnancy outcome, mainly because corticosteroids
affect almost every cell in the body [4] and because of the
higher potency of the synthetic corticosteroids [5].
Miscarriage
is the most common adverse event of early pregnancy, affect-
ing approximately 20% of pregnancies [6,7]. Studies of con-
genital malformations often focus on the prevalence of
malformations at birth, whereby pregnancies ending in a mis-
carriage are excluded [8,9].
In this MiniReview, we provide an overview of the use
of
inhaled and oral corticosteroids in pregnancy, with specific
emphasis on the association between use of corticosteroids
during pregnancy and risk of miscarriage and congenital mal-
formations in offspring.
Methods
To identify relevant studies, we searched the PubMed, EMBASE
and
CINAHL databases with the following limitations: studies in
human
beings, English language and published from January 1995 to
December
2013. In addition, we identified studies through communication
with
other researchers and by reviewing the reference lists of
relevant
articles. For the identification of studies of corticosteroid
use during
pregnancy, we used the following search terms: ‘drug
utilization’,
‘glucocorticoids’ or ‘anti-asthmatics’
and ‘pregnancy’. To identify
studies on congenital malformations in the offspring and use
of
corticosteroids, we used the following search terms:
‘congenital
abnormalities’ or ‘cleft palate’,
‘glucocorticoids’ or ‘anti-asthmatics’and
‘pregnancy’. Finally, we used the following search terms
‘sponta-
neous abortion’ and ‘glucocorticoids’
or ‘anti-asthmatics’ to identify
studies that addressed the association between miscarriage and
use of
corticosteroids.
We used the following criteria to restrict the literature: (1)
for the
drug utilization studies, we required that they include
corticosteroid
use in pregnancy; (2) for studies that addressed congenital
malforma-
tions and miscarriage, we selected only studies that
specifically
addressed inhaled or oral corticosteroid use in early pregnancy
defined
as the first trimester (until gestational week 12); and (3) if
more than
one study was conducted based on the same data sources and
with
overlapping study periods, we only included the most
comprehensive
study. We included seven drug utilization studies
[10 – 16], eleven
Author for correspondence: Anne-Mette Bay Bjørn, Department
of Gynecology and Obstetrics, Aarhus University Hospital,
Skejby, Breds-trupgaardsvej, 8200 Aarhus N, Denmark (e-mail
[email protected]).
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
Basic & Clinical Pharmacology & Toxicology, 2015,
116, 308–314 Doi: 10.1111/bcpt.12367
-
8/15/2019 inhalan kortikosteroid
2/7
prevalence studies [17 – 25] and six
case – control studies [26 – 31] that
met our criteria.
Results
Use of corticosteroids in pregnancy.
Prevalence of corticosteroid use in early pregnancy varied
from 0.5% [13] to 10% [14]. The studies classified the use
of
corticosteroids differently; most studies reported the
corticoste-
roid use classified as systemic [10,11,13 – 16] and
one study
reported the use of inhaled and oral corticosteroids
separately
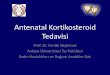
[12]. Differences over time of corticosteroid use during
preg-
nancy were described in one study [12], showing increases in
first-trimester use from 1.1% to 1.8% and in
second-trimester
use from 1.0% to 1.9% over the period of 1999 – 2000
to
2008 –
2009 (fig. 1).
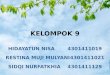
Corticosteroid use and risk of congenital malformations in
offspring.
Published estimates of the association between
corticosteroid
use and risk of congenital malformations in offspring were
inconsistent. Prevalence odds ratios (POR) ranged from 0.8
(95% confidence interval (CI), 0.4 – 1.7) [17] to 2.1
(95% CI,
0.5 – 9.6) [22] (table 1). The largest study, which
included
892,362 pregnant women, of whom 12,478 used corticoster-
oids during pregnancy, reported a POR for congenital malfor-
mations overall of 1.1 (95% CI, 1.0 – 1.2) comparing
users and
non-users of inhaled corticosteroids during pregnancy [21].The
association of corticosteroid use in early pregnancy and
oral clefts in offspring was evaluated in four prevalence
stud-
ies [18,20,21,32] and five case – control studies
[27 – 31], with
reported POR ranging from 0.5 (95% CI, 0.1 – 3.3) [18]
to 1.4
(1.0 – 1.9) [21], whereas the odds ratios (OR) ranged
from 0.6
(95% CI, 0.2 – 1.7) [30] to 5.2 (95% CI,
1.5 – 17.1) [31]
(table 1).
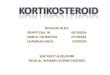
Studies on corticosteroid use and risk of miscarriage.
Most published studies found an association between the use
of corticosteroids and the risk of miscarriage
[19,24 – 26], with
relative risk estimates ranging from 1.2 [25,26] to 1.7
[19],
while one small study showed no association but had wide
confidence intervals (OR, 1.0; 95% CI, 0.5 –
2.1) [22] (table 2).
The largest prevalence study included almost 300,000 preg-
nancies from the Health Improvement Network in England
and Wales of whom 8849 used inhaled corticosteroids; they
reported an OR for miscarriage of 1.2 (95% CI,
1.2 – 1.3) [25].
In a Danish registry-based case – control study
(10,974 cases
and 109,740 controls), the adjusted OR for miscarriage
associ-
ated with the current use of inhaled corticosteroids within
60 days before the miscarriage was also 1.2 (95% CI,
1.0 – 1.4)
[26].
Discussion
The use of inhaled and oral corticosteroids in pregnancy is
common, and the use seems to have increased nearly two
times in recent years. Taken together, the evidence suggests
that the use of corticosteroids in early pregnancy is not
associ-
ated with an increased risk of congenital malformations
overall
or oral clefts in offspring. It seems that inhaled
corticosteroid
use increases slightly the risk of miscarriage, whereas the
use
of oral corticosteroids does not.
To interpret the results from drug utilization studies, it
is
important to consider the possibility of low compliance,
which
could lead to over-estimation of drug use. Among non-preg-
nant women in Denmark, there was a strong agreement
between self-reported drug intake and dispensation record[33];
however, this result may not be generalizable to pregnant
women, who may be more likely to be non-compliant for
fear
of teratogenicity [8]. At the same time, a series of
Hungarian
validation studies on drug use in pregnancy showed that only
a small group of pregnant women (2.4%) abstained from using
prescribed drugs due to fear of teratogenic effects [34]. A
recent Danish study of adherence to medical treatment among
women with ulcerative colitis (n = 115) before
and/or during
pregnancy estimated a positive predictive value of self-
reported drug use of 86.2% (95% CI 74.6 – 93.9) [35],
suggest-
ing high compliance with therapy among pregnant women
0
5
10
15
20
25
C S
t o t a l
C S
i n h a l e d
C S
o r a l
C S
t o t a l
C S
i n h a l e d
C S
o r a l
C S
t o t a l
C S
i n h a l e d
C S
o r a l
C S
t o t a l
C S
i n h a l e d
C S
o r a l
≤30 days before
pregnancy
first trimester second trimester third
trimester P r e v a l e n c e o f p r e s c r i
b e d d r u g u s e / 1 , 0
0 0
w o m e
n
1999+2000
2008+2009
Fig. 1. Prevalence (per 1000 women) of corticosteroid (CS) drug
use across pregnancy among primiparous women in
1999 – 2000 and 2008 – 2009
[12].
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
MiniReview USE OF CORTICOSTEROIDS IN PREGNANCY
309
-
8/15/2019 inhalan kortikosteroid
3/7
-
8/15/2019 inhalan kortikosteroid
4/7
T a b l e 1 .
( c o n t i n u e d )
A u t h o r , c o u n t r y ,
s t u d y p e r i o d
D a t a s o u r c e s , s t u d y p o p u l a t i o n
S t u d y d e s i g n
T y p e o f
c o r t i c o s t e r o i d
e x p o s u r e
O u t c o m e o f i n t e r e s t
C o n g e n i t a l m a l f o r m a t i o n s o v e r a l l
O
r a l c l e f t s
N o f
e x p o s e d
i n f a n t s w
i t h
a m a l f o r m a t i o n
R e l a t i v e r i s k
e s t i m a t e s * ( 9 5 %
c o n f i d e n c e
i n t e r v a l )
N o f
e x p o s e d
i n f a n t s w i t h
o r a l c l e f t s
R e l a t i v e r i s k e s t i m a t e s *
( 9 5 % c o n f i d e n c e i n t e r v a l )
P r a d a t [ 3 0 ]
A u s t r a l i a
, F r a n c e ,
I t a l y , I s r a e l ,
J a p a n , t h e N e t h e r l a n d s
,
S o u t h A m e r i c a
1 9 9 0 –
2 0 0 2
M a l f o r m a t i o n D r u g E x p o s u r e
S u r v e i l l a n c e P r o j e c t –
M A D R E
1 1 , 1
5 0
m a l f o r m e d i n f a n t s . 2 3
, 5 1 7 c o n t r o l i n f a n t s
C a s e – c o n t r o l
I n h a l e d
S y s t e m i c d
4 3 1
1 5 1 3
1
A l l : 0 . 6 ( 0
. 2 –
1 . 7 )
C L P : 0 . 7 ( 0
. 2 –
2 . 2 )
C P : 0
. 6 ( 0
. 1 –
5 . 1 )
A l l : 1 . 3 ( 0
. 7 –
2 . 2 )
C L P : 1 . 8 ( 1
. 0 –
3 . 1 )
C P : 0 . 3 ( 0
. 0 4 – 1 . 5 )
C a r m i c h a e l [ 2 7 ]
U S A
1 9 8 7 –
1 9 8 8
T h e C a l i f o r n i a B i r t h D e f e c t s M o n i t o r i n g P r o g r a m
1 2 9 9 m
a l f o r m e d i n f a n t s . 7 3 4 c o n t r o l i n f a n t s
C a s e – c o n t r o l
O r a l
6 3
C L P : 4 . 3 ( 1
. 1 –
1 7 . 2
)
C P : 5 . 3 ( 1
. 1 ; 2 6
. 5 )
R o d r i g u e z –
P i n i l l a [ 3 1 ]
S p a i n
A p r .
1 9 7 6 –
D e c .
1 9 9 5
S p a n i s h C o l l a b o r a t i v e S t u d y o f C o n g e n i t a l
M a l f o r m a t i o n s –
E C E M C
2 4 , 0
3 8
m a l f o r m e d i n f a n t s . 2 3
, 5 1 7 c o n t r o l i n f a n t s
C a s e – c o n t r o l
O r a l
5
A l l : 5 . 2 ( 1
. 5 –
1 7 . 1
)
C z e i z e l [ 2 8 ]
H u n g a r y
1 9 8 0 –
1 9 9 4
T h e H u n
g a r i a n C o n g e n i t a l A b n o r m a l i t y
R e g i s t r y –
H C C S C A
2 0 , 8
3 0
m a l f o r m e d i n f a n t s . 3 5
, 7 2 7 c o n t r o l i n f a n t s
C a s e – c o n t r o l
O r a l
1
A l l : 1 . 3 ( 0
. 8 –
2 . 0 )
A b b r e v i a t i o n s : A l l
, a l l c l e f t s ; C L P
, c l e f t l i p w i t h o r w i t h o u t c l e f t p a l a t e ; C P
, c l e f t p a l a t e
.
S t u d y p o p u l a t i o n d e f i n i t i o n : a t h e s t u d y p o
p u l a t i o n d e f i n e d i n K € a l l e n e t a l . [ 5 7 ]
.
E x p o s u r e d e f i n i t i o n s r e g a r d i n g s y s t e m i c u
s e :
b o r a l , i n t r a m u s c u l a r a n d i n t r a v e n o u s p r e p a r a t i o n s ; c o r a l a n d i n t r a v e n o u s p r e p a r a t i o n s ;
d o r a l a n d i n j e c t i o n a c c o r d i n g t o t h e A T C - c
l a s s i f i c a t i o n H 0 2 A
.
O u t c o m e d e f i n i t i o n r e g a r d i n g c o n g e n i t a l m
a l f o r m a t i o n s o v e r a l l : e n o t c a t e g o r i z e d ;
f d i
a g n
o s e s o f d i s l o c a t i o n o f t h e h i p ,
u n d e s c e n d e d t e s t e s a n d c h r o m o s o m a l d i s o r d e r s e x c l u d e d ; g s o n - g e n e t i c m a j o r c o n g e n i -
t a l m a l f o r m a t i o n s ;
h m a j o r a n d m i n o r m a l f o r m a t i o n s a c c o r d i n g t o H e i n o n e n e t a l . [ 5 8 ] ; i
m a j o r m a l f o r m a t i o n s .
* t h e r i s k e s t i m a t e s a r e g i v e n a s p r e v a l e n c e o d d s r a t i o s f o r t h e p r e v a l e n c e s t u d i e s a n d o d
d s r a t i o f o r t h e c a s e –
c o n t r o l s t u d i e s .
F o r r e f e r e n c e s 1 8 a n d 2 2
, t h e r i s k e s t i m a t e s a r e c a l c u l a t e d u s i n g t h e E p i s h e e t s o f t w a r e ( v e r s i o n 2 0 1 1 , b y K e n n e t h J . R o t h m a n ) .
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
MiniReview USE OF CORTICOSTEROIDS IN PREGNANCY
311
-
8/15/2019 inhalan kortikosteroid
5/7
with chronic diseases. Geographical differences in drug
utili-
zation patterns may stem from differences in reporting poli-
cies for over-the-counter or reimbursed drugs. Furthermore,
differences in socio-economic or health characteristics of
the
underlying populations may influence the use of prescribed
drugs during pregnancy [36]. Regarding the studies of
congenital malformations, factors such as the route of
admin-
istration of corticosteroids and the classification of
malforma-
tions differed among the existing studies, which
complicatedcomparisons. Furthermore, to detect even a common
congeni-
tal malformation, a population of at least half a million
preg-
nant women is needed and as many as 5 million are required
to detect rare events [37]. Even with large databases avail-
able, only very few women who used corticosteroids in early
pregnancy and who gave birth to an infant with oral
cleft
were identified [20,26]. Multinational studies could enable
sample sizes large enough to provide a better precision
of
the estimates [38].
Large population-based studies performed with medical da-
tabases from Sweden and Denmark found no association
between the use of corticosteroids in early pregnancy and
mal-
formations in offspring [18,20,21]. The Nordic medical
data-bases are considered a valid tool for epidemiological
research
of congenital malformations [38], with positive predictive
value of 88.2% (range 85.9 – 90.5%) for diagnoses
recorded in
the Danish National Registry of Patients compared
against
medical records [39].
In the case – control studies that reported an
increased risk of
oral clefts with the use of oral corticosteroids, early
pregnancy
exposure information was based on retrospective data col-
lected by means of interviews or questionnaires
[27,28,30,31],
with the risk of differential recall of drug use [40]. The
Hungarian Case-Control Surveillance System of Congenital
Abnormalities (HCCSSCA), which was established in 1980,
contains information on 22,843 cases of congenital malforma-
tions captured in 1980 – 1996 [41]. Data on exposure
during
pregnancy were collected by women’s self-report after having
given birth, potentially inducing spurious associations due
to
differential recall, which could result in observed odds
ratios
biased nearly two times [42]. Furthermore, two studies
reviewed here were based on teratogenic information system
reporting [19,22], in which self-referral bias cannot be
ruledout. Self-referral bias could create an apparent
association
where none exists [40], because reasons for contacting a
tera-
togenic information system may themselves be associated with
the outcome under study [43].
Taking the evidence all together, the use of corticosteroids
in early pregnancy does not seem to be associated with con-
genital malformations in offspring.
Asthma is a common indication for inhaled corticosteroids,
and it may be difficult to separate the effect of
corticosteroids
from the effect of the underlying asthma. A recent meta-
analysis indicated that infants of pregnant women with
asthma
were 11% more likely to have congenital malformations diag-
nosed compared with infants of women with asthma [RR 1.1(95% CI
1.0 – 1.2)], although discussion has been raised
that
this risk could be driven by minor malformations [44]. A
Canadian prevalence study using data from the RAMQ (the
Regie de l’assurance-maladie du Quebec) database included a
total of 41,637 pregnancies, divided into 13,280 pregnancies
in women with asthma and 28,357 pregnancies in women
without asthma, showed that maternal asthma was associated
with a 30% increased risk of any congenital malformation
(OR: 1.3; 95%CI, 1.2 – 1.4) [45]. However, this study
could
not distinctly separate asthma effects from drug effects
[45],
and although discussed thoroughly in several studies
[45 – 50],
Table 2.
Studies of corticosteroid use and risk of miscarriage.
Author, country, study period Data sources, s tudy population
Study design Exposure
Relative risk estimates*
(95% confidence interval);
N of exposed cases
Tata [25]
England and Wales
Jan. 1988 –
Nov. 2004
The Health Improvement Network
281,019 pregnancies
Prevalence studyc Inhaled 1.2 (1.2 – 1.3)
Gur [19]
Israel
1988 – 2001
The Israeli Teratogen Information Service
1101 pregnancies
Prevalence studyc Systemica 1.7 (1.1 – 2.5);
36
Silverman [24]
Trial including 32 countries
Oct. 1996 – Jan. 1998
START (inhaled Steroid Treatment
As Regular Therapy) trial
313 pregnancies
Prevalence studyc Inhaled 1.3 (0.6 – 2.5); 23
Park – Wyllie [22]
Canada
1985 – 1995
Canadian Motherisk cohort
372 pregnancies
Prevalence studyd Systemicb 1.0 (0.5 – 2.1); 13
Bjørn [26]
Denmark
1997 – 2009
The Danish National Registry of Patients
10,974 cases of miscarriage, 109,740 controls
Case – control studye Inhaled
Oral
1.2 (1.0 – 1.4); 140
0.8 (0.5 – 1.2); 28
Exposure definitions regarding systemic use: a
oral, intramuscular and intravenous preparations; b
oral and intravenous preparations.Outcome definition regarding
miscarriage: cnot defined; dmiscarriage before 26
gestational weeks; emiscarriage before 22 gestational
weeks.
*the risk estimates are given as prevalence odds ratios for the
prevalence studies and odds ratio for the case – control
studies.
For references 19, 22 and 24, the risk estimates are calculated
using the Episheet software (version 2011, by Kenneth J.
Rothman).
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
312 ANNE-METTE BAY BJØRN ET AL.
MiniReview
-
8/15/2019 inhalan kortikosteroid
6/7
the isolated effect of the underlying asthma is difficult to
estimate.
A large Swedish prevalence study of 2,205 infants with
cleft palate found a RR of 2.0 (95%CI, 1.1 – 3.8)
among preg-
nant users of corticosteroids [51] which also was the
associa-
tion found in the mouse experiments [3]. Some studies did
not
describe the oral clefts separately [18,21,29,31] or reported
the
effects on cleft lip in retrospective studies with risk of
recallbias [27,28,30].
Agreement that inhaled corticosteroids was associated with
a slightly increased risk of miscarriage was reported in two
large population-based studies [25,26], while no association
was identified for oral use [19,22,26]. Presence of an
associa-
tion with miscarriage for inhaled but not oral corticosteroids
is
counter-intuitive. Oral corticosteroids reach higher
concentra-
tions in the maternal circulation [2] and therefore could be
expected to lead to higher levels of foetal exposure. One
explanation for the association observed for inhaled
corticos-
teroids could be confounding by asthma [52]. Asthma may
also be a risk factor for miscarriage [23,25]. Biologically
explained, hypoxia is induced during asthma exacerbations
causing abnormal smooth muscle activity in the uterus,
similar
to airway smooth muscle contractions in the lungs [53,54].
An
increased risk of miscarriage of 1.57 (95% CI
1.02 – 2.41)
among 1,044 pregnant women with asthma compared with
860 pregnant women without asthma is reported [23]. Also a
higher risk of miscarriage (OR, 1.28; 95% CI,
1.15 – 1.43)
among women with asthma who experienced one or more
exacerbations in the year before pregnancy compared with
women with asthma has been reported [25].
Lack of an apparent association with miscarriage for oral
corticosteroids could also be a reflection of their
protective
effect. Miscarriage may occur as a result of an abnormalimmune
response [54], which anti-inflammatory properties of
corticosteroids might inhibit in high doses. In fact, high
doses
of corticosteroids are used to prevent recurrent
miscarriages
[53], although the effectiveness of this treatment is still
contro-
versial [53,55,56].
Only one study included information about gestational age
at miscarriage [26]. Data on gestational age allow
differentia-
tion between early and late miscarriage, which may have dif-
ferent aetiologies. Bjørn et al. found that
current use of
inhaled corticosteroids within 60 days before miscarriage
was
associated with a slightly increased risk of early
miscarriage
but not with late miscarriage [26]. This could reflect
that
exposure in early pregnancy influences the foetus’
environ-ment and therefore increases the risk of early pregnancy
loss.
Conclusion
Around 2% of all pregnant women use corticosteroids in early
pregnancy, and the prevalence of corticosteroid use has
increased in recent years. The use of corticosteroids did
not
seem to increase the risk of congenital malformations, but
the
use of inhaled corticosteroids was associated with a
slightly
increased risk of miscarriage. However, confounding by indi-
cation cannot be ruled out.
References
1 McGee DC. Steroid use during pregnancy. J Perinat Neonatal
Nurs
2002;16:26 – 39.
2 Chrousos G. Adrenocorticosteroids & adrenocortical
antagonists. In
Katzung B (ed.) Basic and Clinical Pharmacology. Tenth
edition.
McGraw-Hill Companies, Inc, UK; 2007: 635 – 52.
3 Fraser FC, Fainstat TD. Production of congenital defects in
the off-
spring of pregnant mice treated with cortisone: progress
report.Pediatrics 1951;8:527 – 33.
4 Rowland JM, Hendrickx AG. Corticosteroid teratogenicity.
Adv
Vet Sci Comp Med 1983;27:99 – 128.
5 Fraser F, Sajoo A. teratogenic potential of corticosteroids
in
humans. Teratology 1995;51:45 – 6.
6 Buss L, Tolstrup J, Munk C, Bergholt T, Ottesen B, Grønbaek
M
et al. Spontaneous abortion: a prospective cohort study of
younger
women from the general population in Denmark. Validation,
occur-
rence and risk determinants. Acta Obstet Gynecol Scand
2006;85:91 – 101.
7 Savitz DA, Hertz-Picciotto I, Poole C, Olshan AF.
Epidemiologic
measures of the course and outcome of pregnancy. Epidemiol
Rev
2002;24:91 – 101.
8 Mitchell A. Studies of drug-induced birth defects. In: Storm
B,
(ed). Pharmacoepidemiology, 4th edn. John Wiley and Sons
Ltd,West Sussex, 2011; 501 – 14.
9 Weinberg CR, Wilcox AJ. Methodologic issues in
reproductive
epidemiology. In: Rothman KJ, Greenland S, Lash TL, (eds).
Mod-
ern Epidemiology, 3rd edn. Lippincott Williams & Wilkins,
Phili-
delphia, 2008; 620 – 40.
10 Andrade SE, Gurwitz JH, Davis RL, Chan KA, Finkelstein
JA,
Fortman K et al. Prescription drug use in pregnancy.
Am J Obstet
Gynecol 2004;191:398 – 407.
11 Bakker M, Jentink J, Vroom F, Van Den Berg P, De Walle H,
De
Jong-Van Den Berg L. Drug prescription patterns before,
during
and after pregnancy for chronic, occasional and
pregnancy-related
drugs in the Netherlands. BJOG 2006;113:559 – 68.
12 Bjørn AMB. Use of corticosteroids in pregnancy
– with special
focus on the relation to congenital malformations in offspring
and
miscarriage. PhD thesis, 2012.13 Irvine L, Flynn RWV, Libby G,
Crombie IK, Evans JMM. Drugs
dispensed in primary care during pregnancy: a record-linkage
analysis in Tayside, Scotland. Drug Saf
2010;33:593 – 604.
14 Lacroix I, Mase-Michel C, Lapeyre-Mestre M, Montastruc JL.
Pre-
scription of drugs during pregnancy in France. Lancet
2000;356:1735 – 6.
15 Olesen C, Steffensen FH, Nielsen GL, de Jong-Van der Berg
L,
Olsen J, Sørensen HT. Drug use in first pregnancy and lactation:
a
population-based survey among Danish women. Eur J Clin Phar-
macol 1999;55:139 – 44.
16 Stephansson O, Granath F, Svensson T, Haglund B, Ekbom A,
Ki-
eler H. Drug use during pregnancy in Sweden - assessed by
the
Prescribed Drug Register and the Medical Birth Register. Clin
Epi-
demiol 2011;3:43 – 50.
17 Alexander S, Dodds L, Armson BA. Perinatal outcomes inwomen
with asthma during pregnancy. Obstet Gynecol 1998;92:
435 – 40.
18 Bjørn AMB, Ehrenstein V, Hundborg H, Nohr EA, Sørensen
HT,
Nørgaard M. Use of corticosteroids in early pregnancy is not
asso-
ciated with risk of oral clefts and other congenital
malformations
in offspring. Am J Ther 2012;21:73 – 80.
19 Gur C, Diav-Citrin O, Shechtman S, Arnon J, Ornoy A.
Pregnancy outcome after first trimester exposure to
corticoster-
oids: a prospective controlled study. Reproduc Toxicol
2004;18:
93 – 101.
20 Hviid A, Mølgaard-Nielsen D. Corticosteroid use during
pregnancy
and risk of orofacial clefts. CMAJ
2011;183:796 – 804.
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
MiniReview USE OF CORTICOSTEROIDS IN PREGNANCY
313
-
8/15/2019 inhalan kortikosteroid
7/7
21 K€allen B, Olausson PO. Use of anti-asthmatic drugs during
preg-
nancy. 3. Congenital malformations in the infants. Eur J Clin
Phar-
macol 2007;63:383 – 8.
22 Park-Wyllie L, Mazzotta P, Pastuszak A, Moretti ME, Beique
L,
Hunnisett L et al. Birth defects after maternal
exposure to corticos-
teroids: prospective cohort study and meta-analysis of
epidemiolog-
ical studies. Teratology 2000;62:385 – 92.
23 Schatz M, Zeiger RS, Harden K, Huffman CC, Chilingar L,
Petitti
D. The safety of asthma and allergy medications during
pregnancy.J Allergy Clin Immunol 1997;100:301 – 6.
24 Silverman M, Sheffer A, Diaz PV, Lindmark B, Radner F,
Brodd-
ene M et al. Outcome of pregnancy in a randomized
controlled
study of patients with asthma exposed to budesonide. Ann
Allergy
Asthma Immunol 2005;95:566 – 70.
25 Tata LJ, Lewis SA, McKeever TM, Smith CJP, Doyle P,
Smeeth
L et al. A comprehensive analysis of adverse
obstetric and pediat-
ric complications in women with asthma. Am J Respir Crit
Care
Med 2007;175:991 – 7.
26 Bjørn AMB, Nielsen RB, Nørgaard M, Nohr EA, Sørensen HT,
Ehrenstein V. Risk of miscarriage among users of
corticosteroid
hormones: a population-based nested case-control study. Clin
Epi-
demiol 2013;5:287 – 94.
27 Carmichael SL, Shaw GM. Maternal corticosteroid use and
risk
of selected congenital anomalies. Am J Med Genet
1999;86:242 – 4.
28 Carmichael SL, Shaw GM, Ma C, Werler MM, Rasmussen SA,
Lammer EJ. Maternal corticosteroid use and orofacial clefts. Am
J
Obstet Gynecol 2007;197:585.e1 – 7.
29 Czeizel AE, Rockenbauer M. Population-based case-control
study
of teratogenic potential of corticosteroids. Teratology
1997;56:335 –
40.
30 Pradat P, Robert-Gnansia E, Di Tanna GL, Rosano A, Lisi
A,
Mastroiacovo P et al. First trimester exposure to
corticosteroids
and oral clefts. Birth Defects Res A Clin Mol Teratol
2003;67:968 – 70.
31 Rodr ıguez-Pinilla E, Mart ınez-Fr ıas M.
Corticosteroids during
pregnancy and oral clefts: a case-control study. Teratology
1998;58:2 – 5.
32 Vasilakis-Scaramozza C, Aschengrau A, Cabral HJ, Jick
SS.Asthma drugs and the risk of congenital anomalies.
Pharmacother-
apy 2013;33:363 – 8.
33 Løkkegaard EL, Johnsen SP, Heitmann BL, Stahlberg C,
Pedersen
AT, Obel EB et al. The validity of self-reported
use of hormone
replacement therapy among Danish nurses. Acta Obstet Gynecol
Scand 2004;83:476 – 81.
34 Czeizel AF, Petik D, Vargha P. Validation studies of drug
expo-
sures in pregnant women. Pharmacoepidemiol Drug Saf
2003;12:409 – 16.
35 Julsgaard M, Nørgaard M, Hvas CL, Buck D, Christensen LA.
Self-reported adherence to medical treatment prior to and
during
pregnancy among women with ulcerative colitis. Inflamm Bowel
Dis 2011;17:1573 – 80.
36 Lee D, Bergman U. Studies of drug utilization. In: Storm B,
(ed).
Pharmacoepidemiology, 4th edn. John Whiley & Sons Ltd,
West Sussex, 2005; 401 – 8.
37 Skegg DCG, Doll R. Record linkage for drug monitoring. J
Epi-
demiol Community Health 1981;35:25 – 31.
38 Furu K, Wettermark B, Andersen M, Martikainen J,
Almarsdottir
AB, Sørensen HT. The Nordic countries as a cohort for
pharma-
coepidemiological research. Basic Clin Pharmacol Toxicol
2010;
106:86 – 94.
39 Larsen H, Nielsen GL, Bendsen J, Flint C, Olsen J, Sørensen
HT.
Predictive value and completeness of the registration of
congenital
abnormalities in three Danish population-based registries. Scand
J
Public Health 2003;31:12 – 6.
40 Ehrenstein V, Sørensen HT, Bakketeig LS, Pedersen L.
Medical
databases in studies of drug teratogenicity: methodological
issues.
Clin Epidemiol 2010;2:37 – 43.
41 Czeizel AE, Rockenbauer M, Siffel C, Varga E. Description
and
mission evaluation of the Hungarian case-control surveillance
of congenital abnormalities, 1980-1996. Teratology
2001;63:176 – 85.
42 Rockenbauer M, Olsen J, Czeizel AE, Pedersen L, Sørensen
HT.
Recall bias in a case-control surveillance system on the use
of
medicine during pregnancy. Epidemiology
2001;12:461 – 6.
43 Rothman KJ, Greenland S, Lash T. Validity in epidemiologic
stud-
ies. In: Rothman KJ, Greenland S, Lash T, (eds). Modern
epidemi-
ology, 3rd edn. Lippincott Williams & Wilkins,
Philadelphia,
2008; 128 – 47.
44 Murphy VE, Wang G, Namazy JA, Powel H, Gibson PG,
Chambers
C et al. The risk of congenital malformations,
perinatal mortality
and neonatal hospitalization among pregnant women with asthma:
A
systematic review and meta-analysis. BJOG
2013;120:812 – 22.
45 Blais L, Kettani FZ, Elftouh N, Forget A. Effect of
maternal
asthma on the risk of specific congenital malformations: A
popula-
tion-based cohort study. Birth Defects Res A Clin Mol
Teratol2012;88:216 – 22.
46 Dombrowski MP. Asthma and pregnancy. Obstet Gynecol
2006;108:667 – 81.
47 Namazy JA, Schatz M. Treatment of asthma during pregnancy
and
perinatal outcomes. Curr Opin Allergy Clin Immunol
2005;5:229 –
33.
48 Rey E, Boulet LP. Pregnancy plus: asthma in pregnancy.
BMJ
2007;334:582 – 5.
49 Schatz M. Asthma and pregnancy. Lancet
1999;353:1202 – 4.
50 Schatz M, Dombrowski MP, Wise R, Momirova V, Landon M,
Mabie W et al. The relationship of asthma medication
use to peri-
natal outcomes. J Allergy Clin Immunol
2004;113:1040 – 5.
51 K€allen B. Oral Clefts. In: K€allen B, (ed). Epidemiology of
Human
Congenital Malformations, 1st edn. Springer Verlag,
Springer
International Publishing Switzerland, 2014; 73 –
7.52 Csizmadi I, Collet JP, Boivin JF. Bias and confounding in
pharma-
coepidemiology. In: Storm B, (ed). Pharmacoepidemiology, 4th
edn. John Wiley&Sons Ltd, West Sussex, 2011;
791 – 809.
53 Laskin CA, Bombardier C, Hannah ME, Mandel FP, Ritchie
JW,
Farwell V et al. Prednisone and aspirin in women
with autoanti-
bodies and unexplained recurrent fetal loss. N Engl J Med
1997;337:148 – 54.
54 Mellor A, Munn D. Immunology at the maternal-fetal
interface:
lessons for T cell tolerance and suppression. Annu Rev
Immunol
2000;18:367 – 91.
55 Porter TF, LaCoursiere Y, Scott JR. Immunotherapy for
recurrent
miscarriage. Cochrane Database Syst Rev 2006;19:CD000112.
56 Salmon JE. A noninflammatory pathway for pregnancy loss:
Innate
immune activation? J Clin Invest 2004;114:15 – 7.
57 K€allen B, Otterblad Olausson P. Use of anti-asthmatic drugs
duringpregnancy. 1. Maternal characteristics, pregnancy and
delivery
complications. Eur J Clin Pharmacol
2007;63:363 – 73.
58 Heinonen OP, Slone D, Shapiro S. Birth Defects and Drugs
in
Pregnancy, 1st edn. Publishing Sciences Group, Inc.,
Littleton,
1977.
© 2014 Nordic Association for the Publication of BCPT
(former Nordic Pharmacological Society)
314 ANNE-METTE BAY BJØRN ET AL.
MiniReview