-
As Principal Scientist of Preclinical Development at Aradigm,
what are your key roles and responsibilities?
JB: It is my responsibility to provide broad evidence of the
efficacy and safety of our products from preclinical models. This
is a very interesting job that involves a variety of studies
typically conducted at universities, contract research
organisations or government labs. I’m responsible for all facets,
from study design to final reports. I’m the ‘hub’ between Aradigm
and all these institutions. I’m also responsible for applying for
government grants to fund research.
Can you outline the breadth of the R&D being carried out at
Aradigm? What is the common factor uniting the various research
strands?
Aradigm’s focus is on prevention and treatment of severe
respiratory diseases. Our pipeline includes inhaled antibiotics
(liposomal ciprofloxacin Pulmaquin® and Lipoquin®) for the
treatment of non-cystic fibrosis bronchiectasis, cystic fibrosis
and non-tuberculous mycobacteria, and for biodefence, as well as
inhaled nicotine for smoking cessation.
Aradigm has also developed the AERx® pulmonary delivery
platform, which has been tested in thousands of patients with drugs
and biologics including insulin, fentanyl, erythropoietin and
nicotine. The largest AERx® programme has been inhaled insulin for
diabetes management that progressed into phase III clinical trials.
This programme is available for out-licensing to a company with
expertise in diabetes.
How do Lipoquin® and Pulmaquin®, the two different formulations
of ciprofloxacin developed at Aradigm, differ?
Lipoquin® and Pulmaquin® differ in the proportion of rapidly
available and slow-release ciprofloxacin. Lipoquin® consists
entirely of
slow-release liposomal ciprofloxacin, whereas Pulmaquin®
consists of Lipoquin® mixed with a small amount of ciprofloxacin
dissolved in an aqueous medium. This provides an initial peak of
free ciprofloxacin in the lung followed by a sustained release of
ciprofloxacin from the liposomal component.
What benefits do inhaled liposome-encapsulated antibiotics
confer compared to traditional treatment approaches?
The main advantages of inhaled formulations are that they
deliver the required antibiotic ciprofloxacin rapidly and directly
in high concentrations to the lung ie. the site of the serious
infections. These concentrations are much higher than those that
could be achieved with oral or injected antibiotics at safe doses.
In contrast, the concentration of the antibiotic in the rest of the
body following its inhalation will be so low that the probability
of side effects is greatly minimised.
When inhaling un-encapsulated antibiotics, the drug residence
time in the lung is typically short. Therefore, frequent
administration of high concentrations of free antibiotic (to
compensate for the rapid loss from the respiratory lumen) would be
required to have adequate antibacterial activity, and this is
inconvenient and may cause airway irritation (cough or
bronchoconstriction). Liposomal encapsulation of antibiotics
overcomes these problems.
How does your research contribute to the development of
therapies against biowarfare agents in the fight against
bioterrorism?
Aradigm started developing inhaled liposomal ciprofloxacin for
biodefence purposes in 2004 through a Technology Demonstration
Program from Defence Research and Development Canada. There,
scientists led by Dr Jonathan Wong had already demonstrated the
efficacy of prototype liposomal ciprofloxacin formulations
in mouse models of Francisella tularensis lung infection – the
causative agent for inhalational tularaemia. More recently, the
development of Lipoquin® and Pulmaquin® for biodefence continued
via collaboration with the Defence Science and Technology
Laboratory (Dstl), UK, and Public Health England.
What are the next steps for Aradigm and ciprofloxacin?
For our non-cystic fibrosis bronchiectasis programme with
Pulmaquin®, we will complete our phase III clinical trials and
submit applications for approval, while for our non-tuberculous
mycobacteria studies, which are currently funded by a phase I Small
Business Innovation Research grant from the National Institute of
Allergy and Infectious Diseases, our next step is to apply for
further funding to expand into combination therapy.
For our biodefence programme, we are seeking funding, with the
help of our collaborators at Dstl, to complete the animal testing
to satisfy the requirements of the Animal Rule for approval by the
US Food and Drug Administration (the Animal Rule facilitates the
approval of certain products for human use, such as biodefence
medicines, without the need for efficacy testing in humans). This
funding will enable us to complete the development and approval of
Lipoquin® and/or Pulmaquin® for prophylaxis and treatment of
multiple potential inhaled bioterrorism infections including
pneumonic plague, inhalational tularaemia and Q fever.
Dr Jim Blanchard and colleagues Drs David Cipolla, Jürgen
Froehlich and Igor Gonda provide an insight into their
organisation’s work using liposomal encapsulation for inhaled
antibiotic development
Inhaled nanomedicines stop nasty infections
www.internationalinnovation.com 47
PHARMACOLOGY
-
ALTHOUGH INHALATION AS a means of drug delivery has a long
history in medicine, it was only in the last century that it became
a mainstay of modern healthcare. Inhalation holds several
advantages over other drug delivery methods such as oral or
intravenous administration – most notably, it can deliver high
levels of a drug rapidly and directly to the patient’s lungs – the
site of infection – while keeping drug concentrations in the rest
of the body comparatively low, thus minimising
side effects.
Aradigm is a California-based pharmaceutical company dedicated
to developing and commercialising products for the prevention and
treatment of severe respiratory diseases, including cystic
fibrosis, non-cystic fibrosis bronchiectasis and non-tuberculous
mycobacteria, as well as for biodefence. Aradigm believes that its
approach has the potential to provide solutions for unmet medical
needs or, where treatments are already available but suboptimal,
significantly improve patients’ quality of life through better
therapeutic outcomes, yet providing simple and convenient
self-administration.
LIPOSOMAL ENCAPSULATIONIn order to achieve this goal, the
Aradigm researchers have had to overcome several challenges: for
example, because of the short residence time in the lung of
conventional antibiotics delivered inhalationally, frequent
administrations of high drug concentrations were required, making
it inconvenient for the patients and more likely to lead to airway
irritation. The solution first identified by Dr
Jonathan Wong at Defence Research and Development Canada was to
liposomally encapsulate a well-tested broad spectrum antibiotic,
ciprofloxacin. The new treatments based on this idea are currently
being evaluated across various studies. The resulting formulations
yield slower drug release, improved antibacterial efficacy against
certain types of microorganisms, and lower systemic exposure,
thereby reducing risk of side effects. Furthermore, patient
experience may be improved as potential airway irritation due to
high concentrations of un-encapsulated ciprofloxacin is removed.
The slow release facilitates once-daily dosing for the patients’
convenience. Other, more subtle advantages of the liposomal
encapsulation are better penetration of the biofilms formed by some
particularly difficult microorganisms such as mycobacteria, and
enhanced uptake of the liposomally encapsulated drug into cells
infected with infections such as in inhalational tularaemia and
plague, as well as in pulmonary infections with non-tuberculous
mycobacteria.
Aradigm’s R&D work on liposomal encapsulation has resulted
in the development of two novel ciprofloxacin formulations:
Lipoquin® and Pulmaquin®. The former facilitates ciprofloxacin’s
continuous slow release, while the latter leads to an initial spike
of ciprofloxacin followed by a steadier, slow release.
CLINICAL TRIALSBoth Lipoquin® and Pulmaquin® have been tested in
clinical trials for use in treating non-cystic fibrosis
bronchiectasis. “Initially,
US pharmaceutical company Aradigm is developing cutting-edge
antibiotic products that can be delivered by inhalation, with
applications in the prevention and treatment of severe respiratory
infections as well as biodefence
Breathe it in
As part of Aradigm’s biodefence programme, the following
findings, using mouse models of lung infection, demonstrated the
significant benefits offered by Lipoquin® over conventionally
administered ciprofloxacin
AGAINST TULARAEMIA
When administered 24 hours postexposure, a single aerosolised
dose (1 mg/kg) of Lipoquin® provided 100% protection against lethal
doses of inhalational tularemia (Francisella tularensis Schu
S4)
In contrast, oral ciprofloxacin (50 mg/kg) given twice daily for
five days had >80% mortality
AGAINST PNEUMONIC PLAGUE
A single dose (50 mg/kg) of intranasally instilled Lipoquin®
provided 100% protection against pneumonic plague (Yersinia
pestis CO92)
In contrast, seven days of twice daily doses of oral
ciprofloxacin (50 mg/kg) were needed to provide 100% protection
AGAINST Q FEVER
When mice infected with Q-fever (caused by Coxiella burnetii)
were treated after 24 hours with Lipoquin® (50 mg/kg) once daily
for seven days, they were protected against clinical signs
In contrast, mice treated twice daily with oral ciprofloxacin
(50 mg/kg) or PBS had 15-20% body weight loss and exhibited
symptoms of the disease such as ruffled fur, arched backs and
dehydration
LIPOQUIN® FOR BIODEFENCE
48 INTERNATIONAL INNOVATION
-
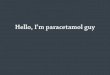
Spleen & liver
Free ciprofl oxacin kills bacteria in the plankton, liposomally
encapsulated ciprofl oxacin penetrates the biofi lm and kills
bacteria within it. Free ciprofl oxacin also blocks release of infl
ammatory cytokines. Liposomal ciprofl oxacin is phagocytosed by
macrophages infected with bacteria and kills the infection. These
ciprofl oxacin-loaded liposomes may also be able to be transported
via the lymphatic ducts to clear infections in the distal organs
such as the spleen and liver.
MECHANISM OF ACTION OF CIPROFLOXACIN ENCAPSULATED IN
LIPOSOMES
Biofi lm
Bacteria
Macrophage
Ciprofl oxacinLymphatic vessel
Lung cell Ciprofl oxacin encapsulated in liposome
ARADIGM CORPORATION
OBJECTIVETo complete the development and approval of a
broad-spectrum antibacterial prophylaxis and treatment product
against multiple, potential inhaled bioterrorism infections,
including pneumonic plague, inhalational tularaemia and Q
fever.
KEY COLLABORATORSDr Jonathan P Wong, Defence Research and
Development Canada, Canada
Dr Karleigh A Hamblin; Dr Sarah V Harding; Dr Isobel H Norville;
Dr Helen S Atkins, Microbiology Group, Defence Science and
Technology Laboratory, UK
Dr Julia Vipond; Graham J Hatch, Public Health England, UK
FUNDINGDefence Research and Development Canada
Aradigm Corporation
National Institutes of Health (NIH)
UK Ministry of Defence
CONTACTDr Jim BlanchardPrincipal Scientist
Aradigm Corporation3929 Point Eden WayHayward, California 94545
USA
T +1 510 265 8871E [email protected]
www.aradigm.com
DR JIM BLANCHARD is Principal Scientist of Preclinical
Development at Aradigm Corporation. He has over 20 years of
pharmaceutical industry experience and over 38 years of
research experience with inhaled aerosols, particularly in the
delivery of aerosolised drugs. At Aradigm, he is responsible for
all preclinical development activities, including the inhaled
antibiotic programme.
we tested the clinical effi cacy and safety of Lipoquin® for
treatment of chronic lung infections due to Pseudomonas aeruginosa
in patients with cystic fi brosis, and both Lipoquin® and
Pulmaquin® for non-cystic fi brosis bronchiectasis in a series of
phase I and II studies,” reveals Dr Jim Blanchard, Principal
Scientist of Preclinical Development at Aradigm.
Although results indicated that the formulations were both safe
and effective for reducing bacterial load, it was Pulmaquin® that
the Aradigm researchers ultimately decided to take on into phase
III trials. “Pulmaquin® signifi cantly improved the median time to
fi rst pulmonary exacerbation compared to placebo in patients with
non-cystic fi brosis bronchiectasis in a six-month phase IIb
study,” elaborates Blanchard. “Additionally, in preclinical models
we observed anti-infl ammatory properties associated with
Pulmaquin®.” As such, two worldwide phase III clinical trials
(ORBIT-3 and -4) are now underway examining the use of Pulmaquin®
to treat non-cystic fi brosis bronchiectasis patients who have
chronic lung infections with P. aeruginosa. Both trials are
scheduled for completion next year.
Additionally, Aradigm is investigating the usefulness of
Lipoquin® and Pulmaquin® for the treatment of lung infections
involving non-tuberculous mycobacteria, the incidence of which is
on the rise in the US. In collaboration with Dr Luiz Bermudez of
Oregon State University, Aradigm scientists have embarked on a
National Institutes of Health (NIH)-funded research programme aimed
at exploring the drugs’ effi cacy in preclinical models of
non-tuberculous mycobacteria infections. Already, in vitro assays
involving Mycobacterium avium and M. abscessus infections have
produced encouraging data demonstrating superior antibacterial
activity compared to ciprofl oxacin in both biofi lm and
intracellular infection models. As such, further effi cacy tests
involving animal models are now underway.
BUILDING BIODEFENCESAnother area in which the Aradigm
researchers have been testing the potential usefulness
of Lipoquin® and Pulmaquin® is biodefence – the investigational
drugs’ effi cacy against biowarfare agents including Francisella
tularensis, Yersinia pestis and Coxiella burnetii (which cause
inhalational tularaemia, plague and Q fever, respectively). Aradigm
is currently working in collaboration with the Defence Science and
Technology Laboratory and Public Health England in the UK to
develop these formulations for biodefence purposes. Already, they
have produced some promising results (see infographic on p 48).
Furthermore, Aradigm had an earlier R&D programme to develop
liposomal ciprofl oxacin for the localised treatment and prevention
of inhalational anthrax with funding from Defence Research and
Development Canada. Oral and intravenous ciprofl oxacin have been
approved by the US Food and Drug Administration as an anthrax
treatment since 2000, and the Aradigm researchers hope an
inhalational formulation will prove more effective, faster acting
and lead to fewer side effects.
Also under the research spotlight is Burkholderia pseudomallei –
the agent behind melioidosis. Importantly, although melioidosis
primarily represents a biowarfare risk to Western nations, its
incidence is widespread in Southeast Asia, where it is associated
with a high mortality rate. Aradigm researchers are therefore keen
for their work in this area to have applications both in biodefence
and public health.
WORKING TOGETHERRegarding the future, Aradigm will continue its
ciprofl oxacin R&D programmes – those involved are keen to see
their work translate into other clinical applications beyond the
current phase III programme in non-cystic fi brosis bronchiectasis
conducted in collaboration with the global pharmaceutical company
Grifols headquartered in Barcelona, Spain. To achieve this, Aradigm
will continue to forge productive, multidisciplinary partnerships
with diverse groups across the drug development spectrum, from
patient advocacy groups, non-government institutes and industry to
government bodies and regulatory authorities. “We want to provide
treatment for patients as soon as possible,” Blanchard
enthuses.
DR DAVID CIPOLLA
DR JÜRGEN FROEHLICH
DR IGOR GONDA
www.internationalinnovation.com 49