Embed Size (px)
Citation preview

Inhibition of bacterial growth
Osteostimulation*
Bioactive bone bonding
*non-osteoinduction
Clinical Cases Orthopaedics & Trauma
2
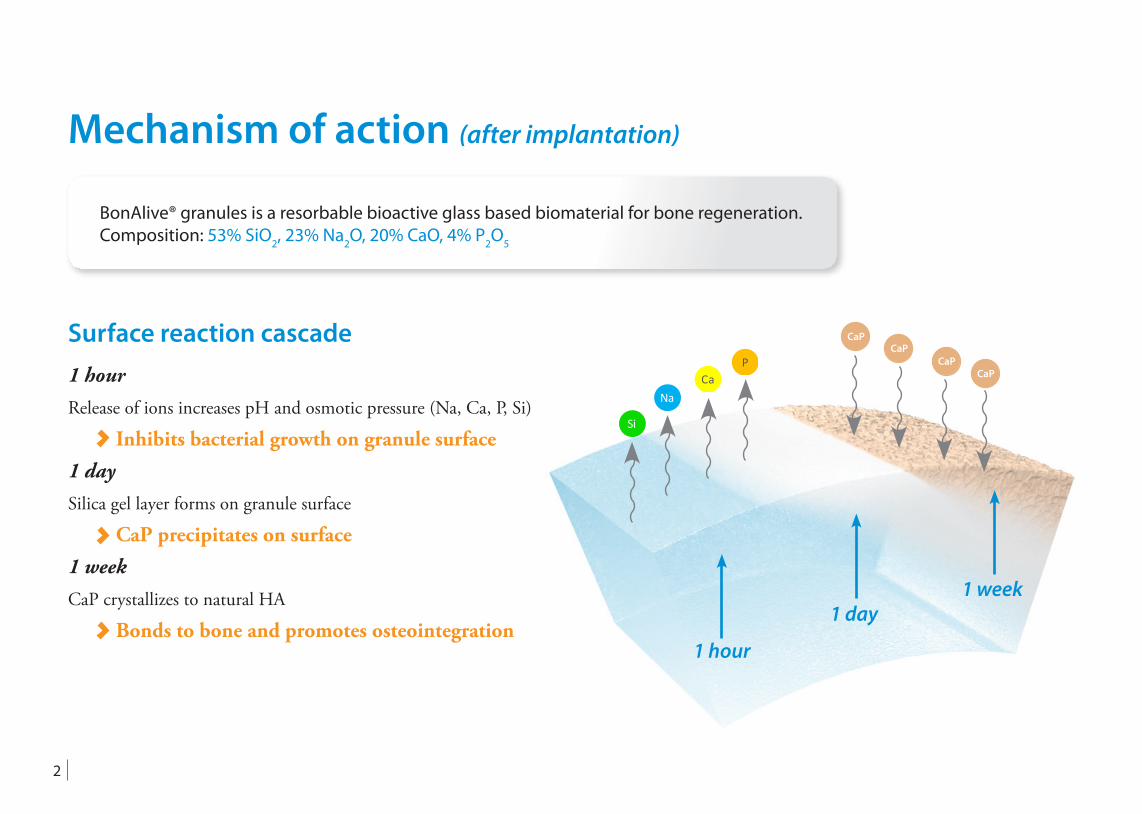
BonAlive® granules is a resorbable bioactive glass based biomaterial for bone regeneration. Composition: 53% SiO2, 23% Na2O, 20% CaO, 4% P2O5
Mechanism of action (after implantation)
1 hour
1 day1 week
Si
NaCa
P
CaPCaP
CaPCaP
Surface reaction cascade1 hour
Release of ions increases pH and osmotic pressure (Na, Ca, P, Si)
Inhibits bacterial growth on granule surface1 day
Silica gel layer forms on granule surface
CaP precipitates on surface1 week
CaP crystallizes to natural HA
Bonds to bone and promotes osteointegration
3
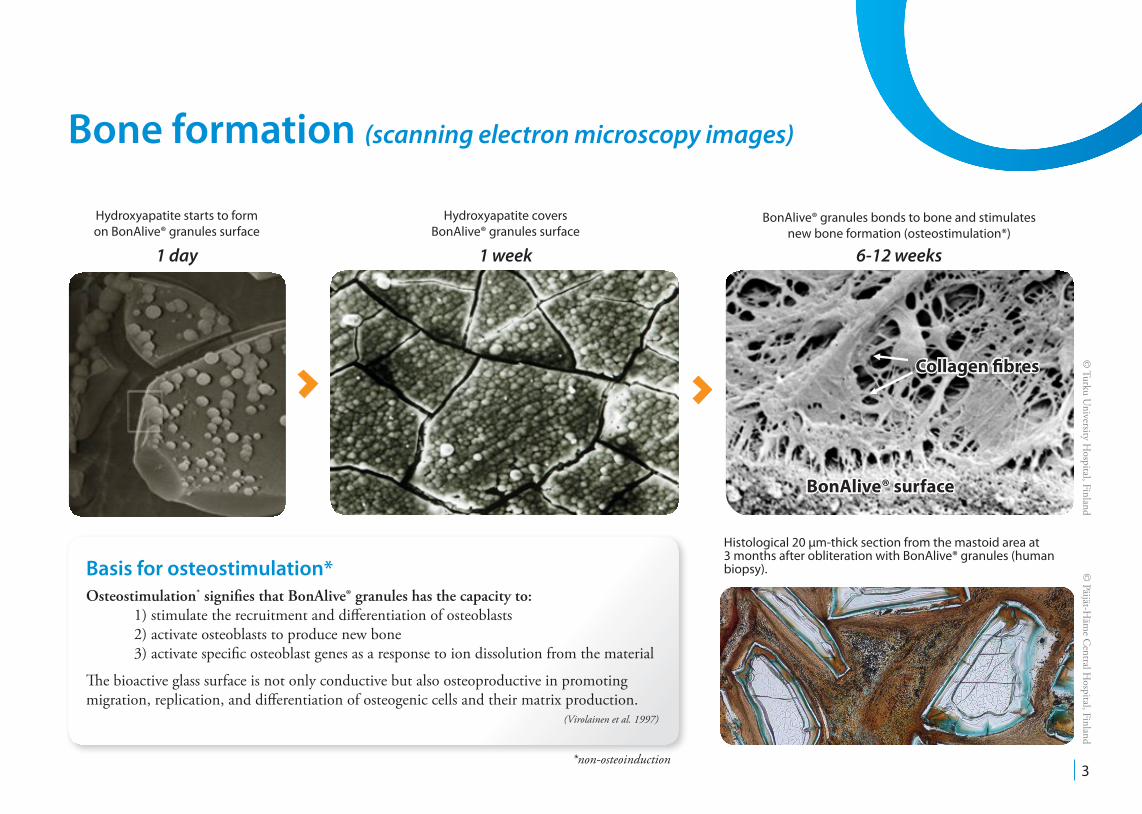
Hydroxyapatite starts to form on BonAlive® granules surface
Hydroxyapatite covers BonAlive® granules surface
BonAlive® granules bonds to bone and stimulatesnew bone formation (osteostimulation*)
Histological 20 µm-thick section from the mastoid area at 3 months after obliteration with BonAlive® granules (human biopsy). ©
Päijät-Häm
e Central H
ospital, Finland
Basis for osteostimulation*Osteostimulation* signifies that BonAlive® granules has the capacity to: 1) stimulate the recruitment and differentiation of osteoblasts 2) activate osteoblasts to produce new bone 3) activate specific osteoblast genes as a response to ion dissolution from the material
The bioactive glass surface is not only conductive but also osteoproductive in promoting migration, replication, and differentiation of osteogenic cells and their matrix production.
(Virolainen et al. 1997)
Bone formation (scanning electron microscopy images)
*non-osteoinduction
© Turku U
niversity Hospital, Finland
BonAlive® surface
Collagen fibres
1 day 1 week 6-12 weeks
4
Bactericidal effects of bioactive glasses on clinically important aerobic bacteria. Munukka E. et al. J Mater Sci: Mater Med. 2008;19:27-32.Antibacterial effect of bioactive glasses on clinically important anaerobic bacteria in vitro. Leppäranta O. et al. J Mater Sci: Mater Med. 2008;19:547-551.Comparison of antibacterial effect on three bioactive glasses. Zhang D. et al. Key Engineering Materials. 2006;309-311:345-348.Interactions between bioactive glass and periodontal pathogens. Stoor P. et al. Microbial Ecology in Health and Disease,1996;9:109-114.Interactions between the frontal sinusitis-associated pathogen Heamophilus Influenzae and the bioactive glass S53P4. Stoor P. et al. Bioceramics. 1995;8:253-258.
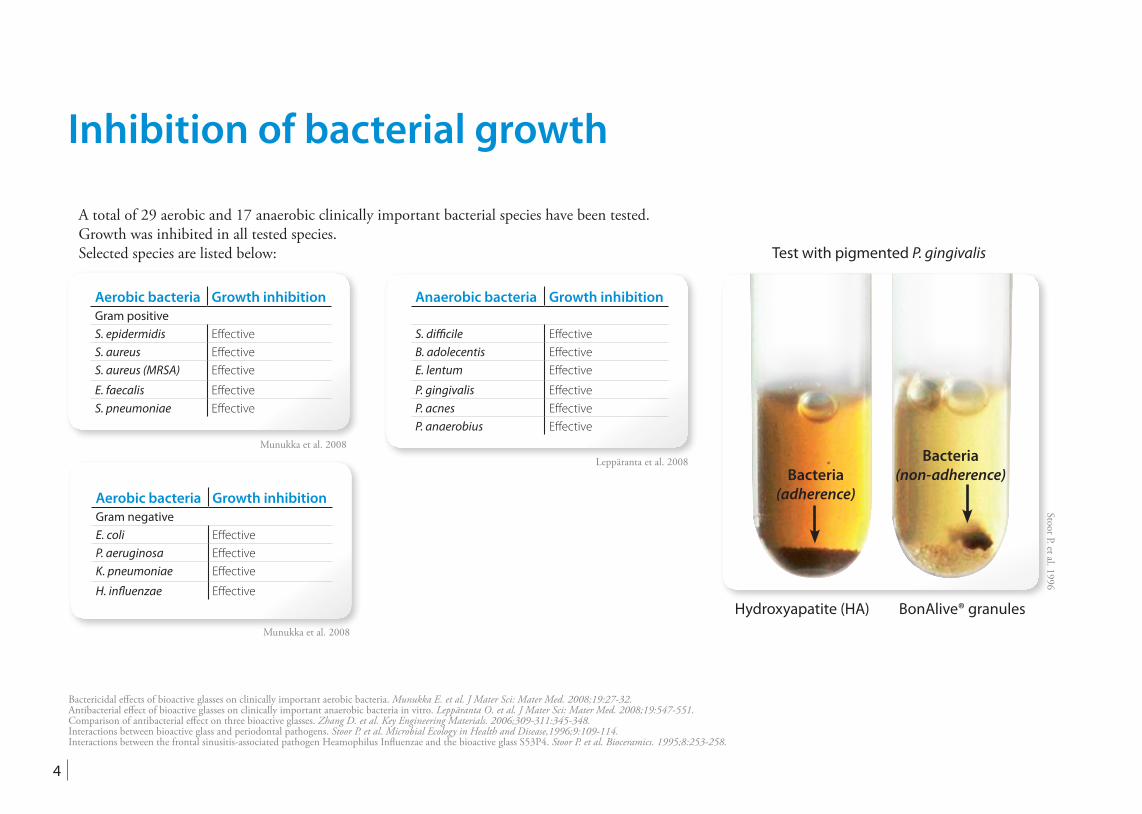
Test with pigmented P. gingivalis
Hydroxyapatite (HA) BonAlive® granules
Stoor P. et al. 1996
Inhibition of bacterial growth
Bacteria(non-adherence)Bacteria
(adherence)
Munukka et al. 2008
Aerobic bacteria Growth inhibitionGram positiveS. epidermidis EffectiveS. aureus EffectiveS. aureus (MRSA) Effective
E. faecalis EffectiveS. pneumoniae Effective
Leppäranta et al. 2008
Anaerobic bacteria Growth inhibition
S. difficile EffectiveB. adolecentis EffectiveE. lentum Effective
P. gingivalis EffectiveP. acnes EffectiveP. anaerobius Effective
Munukka et al. 2008
Aerobic bacteria Growth inhibitionGram negativeE. coli EffectiveP. aeruginosa EffectiveK. pneumoniae Effective
H. influenzae Effective
A total of 29 aerobic and 17 anaerobic clinically important bacterial species have been tested. Growth was inhibited in all tested species.Selected species are listed below:
5
© H
elsinki University C
entral Hospital, Finland
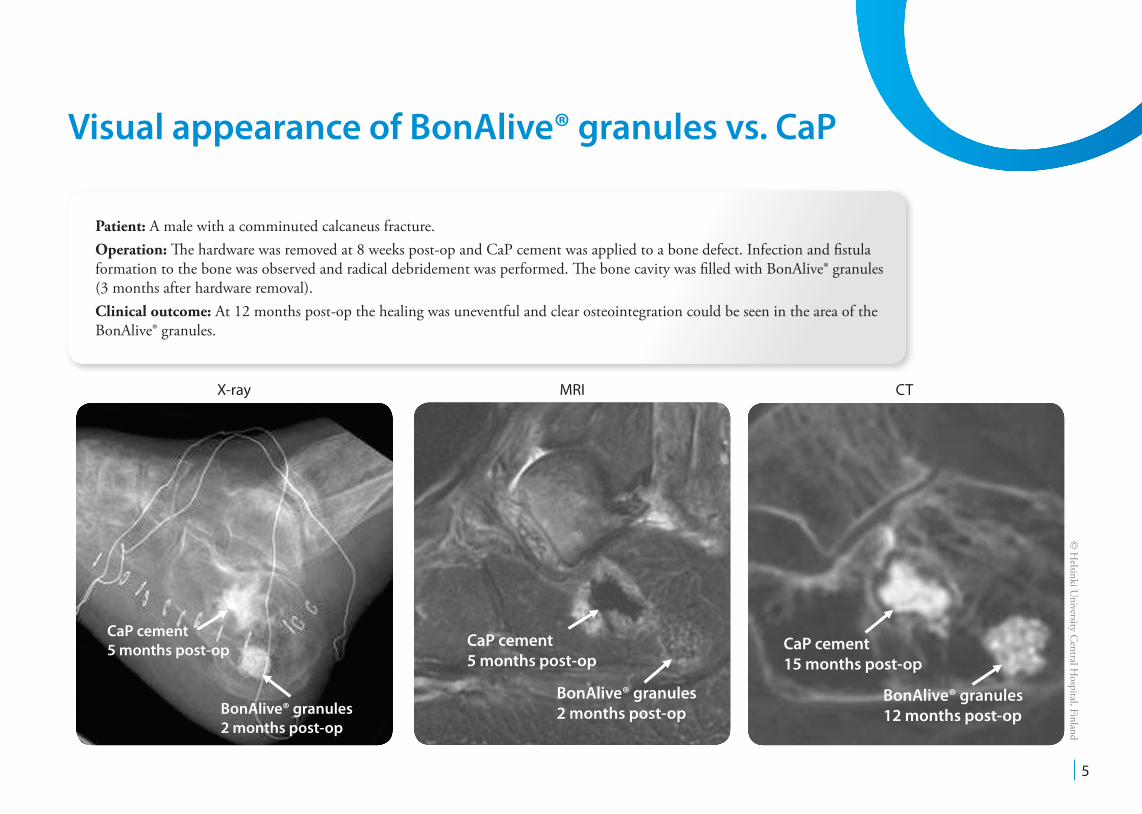
X-ray MRI CT
CaP cement 5 months post-op
BonAlive® granules 2 months post-op
CaP cement 15 months post-op
BonAlive® granules 12 months post-op
CaP cement 5 months post-op
BonAlive® granules 2 months post-op
Patient: A male with a comminuted calcaneus fracture.Operation: The hardware was removed at 8 weeks post-op and CaP cement was applied to a bone defect. Infection and fistula formation to the bone was observed and radical debridement was performed. The bone cavity was filled with BonAlive® granules (3 months after hardware removal). Clinical outcome: At 12 months post-op the healing was uneventful and clear osteointegration could be seen in the area of the BonAlive® granules.
Visual appearance of BonAlive® granules vs. CaP
6Treatment of a recurrent aneurysmal bone cyst with bioactive glass in a child allows for good bone remodelling and growth. Lindfors N. Bone, 2009;45(2):398-400.
Preop 1 month 12 months 24 months3 monthsPostop
Pre-op X-ray
1 month post-op X-ray
3 monthspost-op X-ray
12 monthspost-op X-ray
24 months post-op X-ray
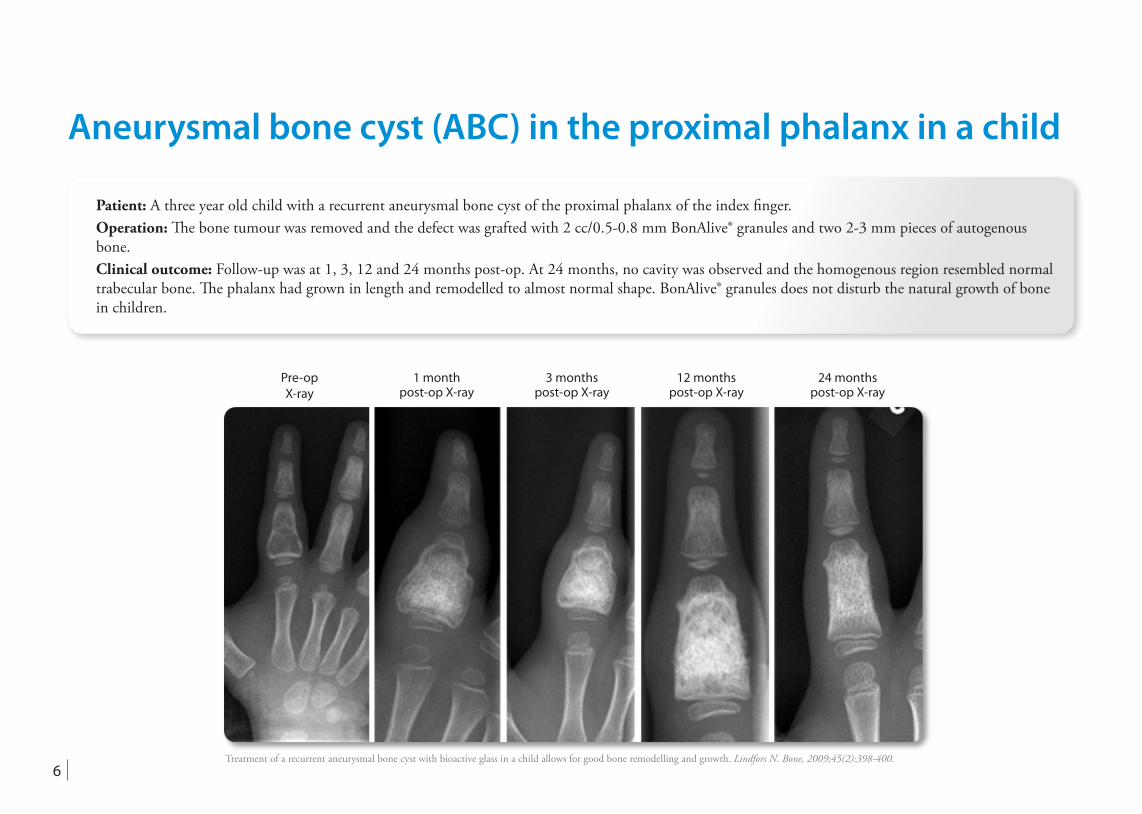
Aneurysmal bone cyst (ABC) in the proximal phalanx in a child
Patient: A three year old child with a recurrent aneurysmal bone cyst of the proximal phalanx of the index finger.Operation: The bone tumour was removed and the defect was grafted with 2 cc/0.5-0.8 mm BonAlive® granules and two 2-3 mm pieces of autogenous bone.Clinical outcome: Follow-up was at 1, 3, 12 and 24 months post-op. At 24 months, no cavity was observed and the homogenous region resembled normal trabecular bone. The phalanx had grown in length and remodelled to almost normal shape. BonAlive® granules does not disturb the natural growth of bone in children.
7
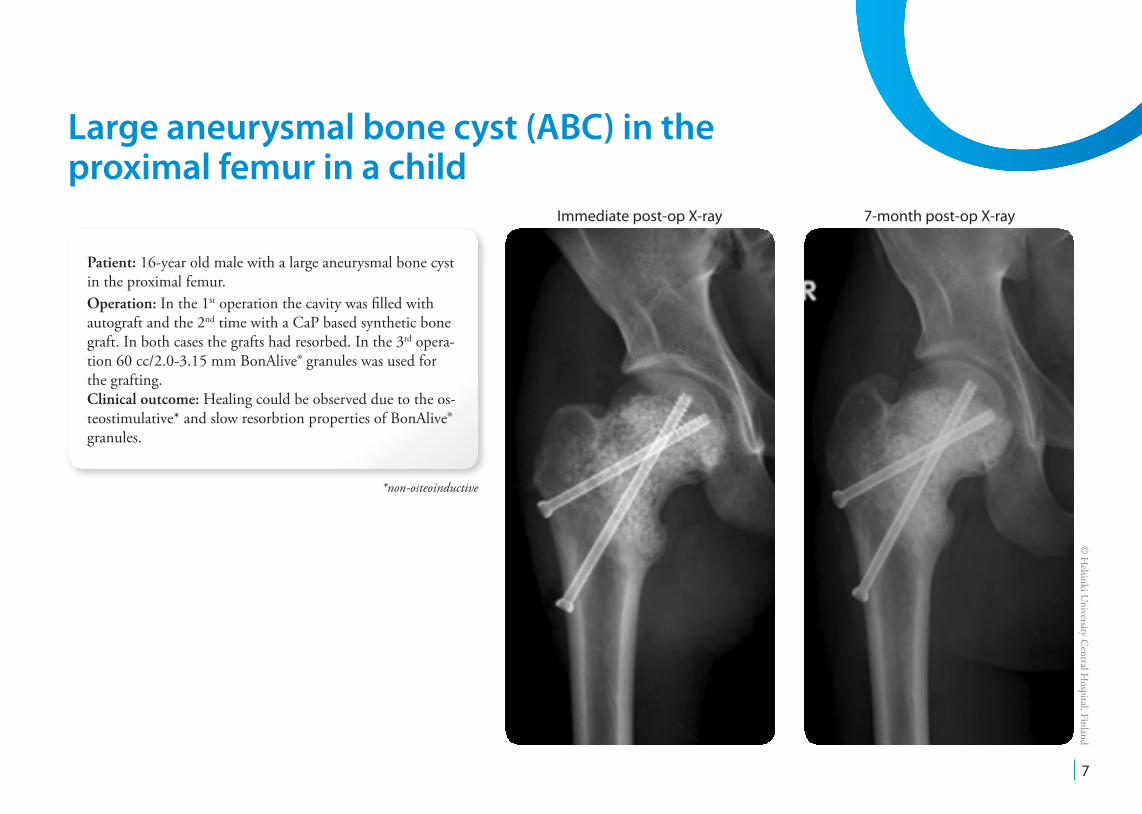
Immediate post-op X-ray 7-month post-op X-ray
© H
elsinki University C
entral Hospital, Finland
Large aneurysmal bone cyst (ABC) in the proximal femur in a child
Patient: 16-year old male with a large aneurysmal bone cyst in the proximal femur.Operation: In the 1st operation the cavity was filled with autograft and the 2nd time with a CaP based synthetic bone graft. In both cases the grafts had resorbed. In the 3rd opera-tion 60 cc/2.0-3.15 mm BonAlive® granules was used for the grafting.Clinical outcome: Healing could be observed due to the os-teostimulative* and slow resorbtion properties of BonAlive® granules.
*non-osteoinductive
8
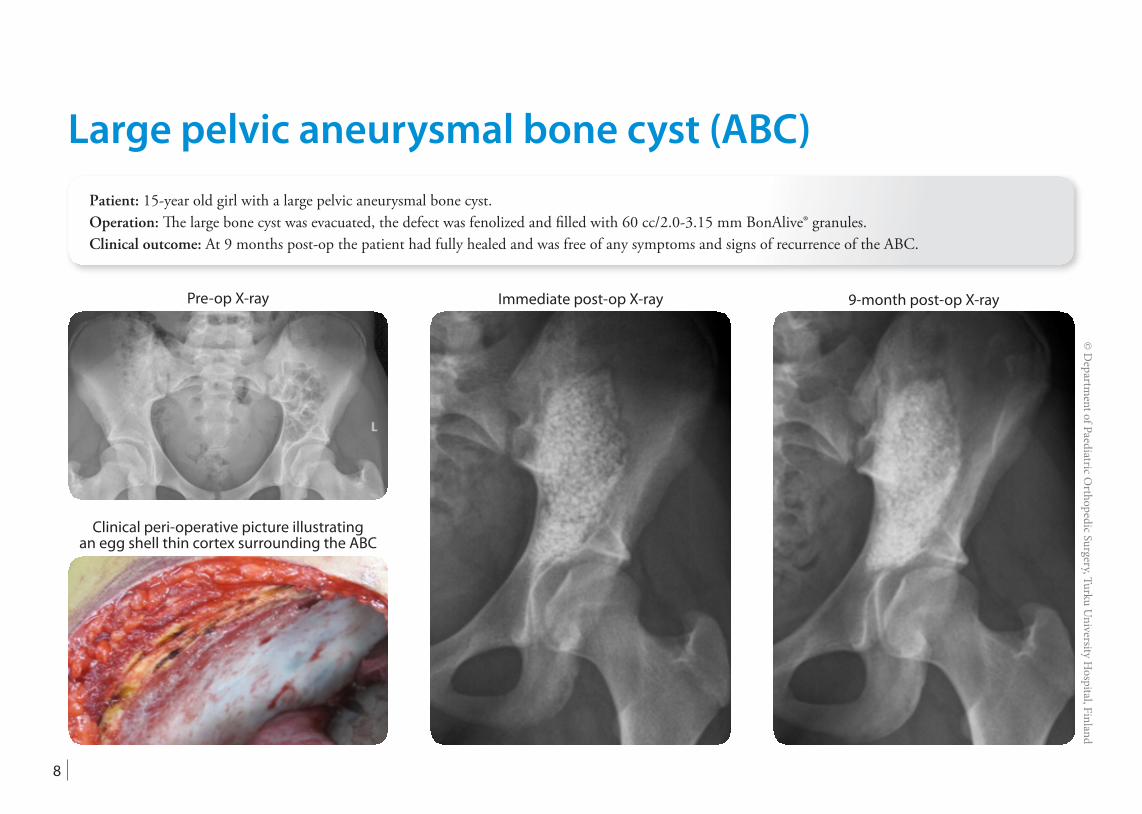
Patient: 15-year old girl with a large pelvic aneurysmal bone cyst.Operation: The large bone cyst was evacuated, the defect was fenolized and filled with 60 cc/2.0-3.15 mm BonAlive® granules.Clinical outcome: At 9 months post-op the patient had fully healed and was free of any symptoms and signs of recurrence of the ABC.
Pre-op X-ray
Clinical peri-operative picture illustrating an egg shell thin cortex surrounding the ABC
Immediate post-op X-ray 9-month post-op X-ray
Large pelvic aneurysmal bone cyst (ABC)
© D
epartment of Paediatric O
rthopedic Surgery, Turku University H
ospital, Finland
9
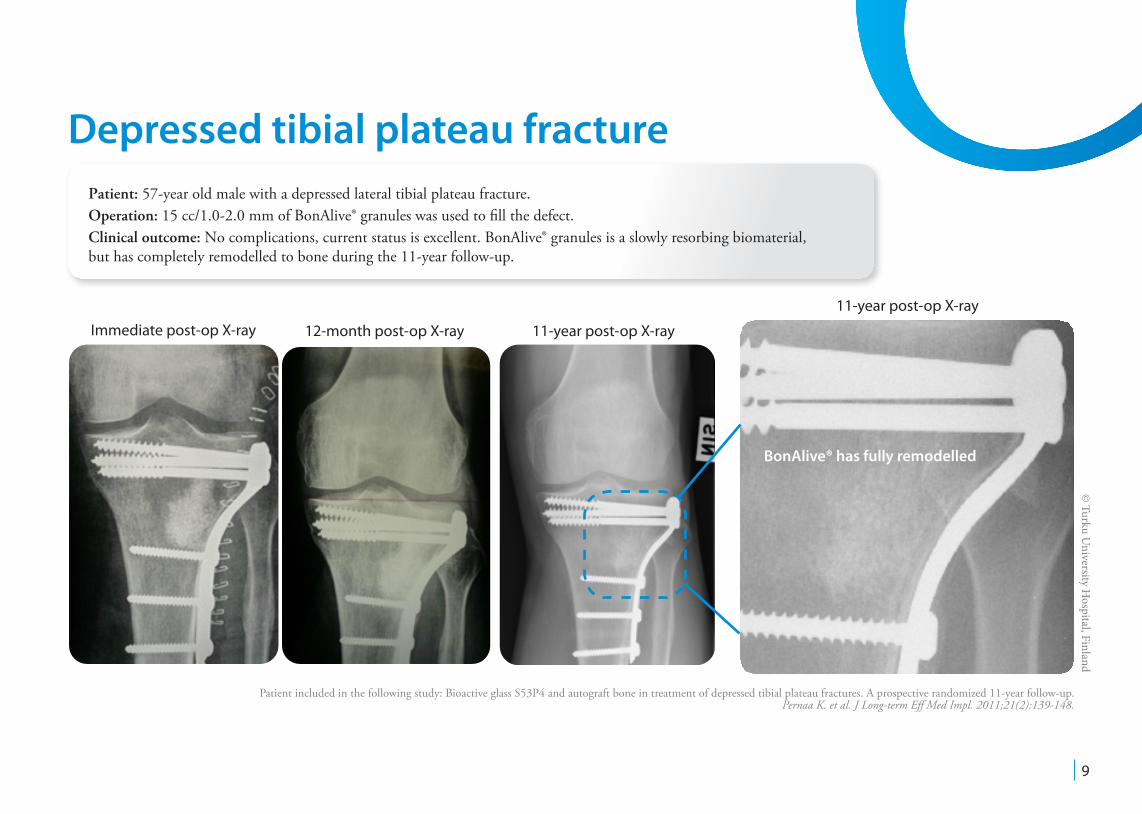
Immediate post-op X-ray 12-month post-op X-ray 11-year post-op X-ray
© Turku U
niversity Hospital, Finland
BonAlive® has fully remodelled
Patient included in the following study: Bioactive glass S53P4 and autograft bone in treatment of depressed tibial plateau fractures. A prospective randomized 11-year follow-up. Pernaa K. et al. J Long-term Eff Med Impl. 2011;21(2):139-148.
11-year post-op X-ray
Depressed tibial plateau fracturePatient: 57-year old male with a depressed lateral tibial plateau fracture.Operation: 15 cc/1.0-2.0 mm of BonAlive® granules was used to fill the defect.Clinical outcome: No complications, current status is excellent. BonAlive® granules is a slowly resorbing biomaterial, but has completely remodelled to bone during the 11-year follow-up.
10
Pre-op X-ray
© H
elsinki University C
entral Hospital, Finland
CaP 2 months post-op
BonAlive® granules7 months post-op
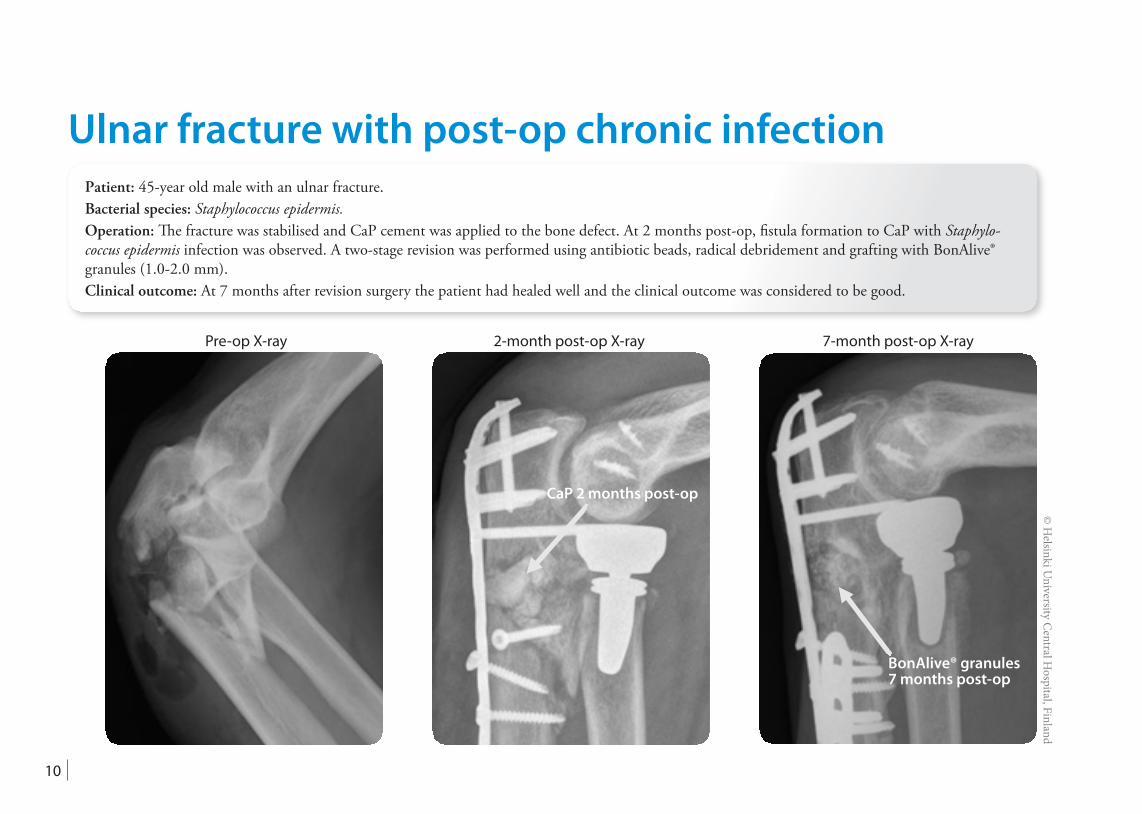
Patient: 45-year old male with an ulnar fracture.Bacterial species: Staphylococcus epidermis.Operation: The fracture was stabilised and CaP cement was applied to the bone defect. At 2 months post-op, fistula formation to CaP with Staphylo-coccus epidermis infection was observed. A two-stage revision was performed using antibiotic beads, radical debridement and grafting with BonAlive® granules (1.0-2.0 mm).Clinical outcome: At 7 months after revision surgery the patient had healed well and the clinical outcome was considered to be good.
2-month post-op X-ray 7-month post-op X-ray
Ulnar fracture with post-op chronic infection
11
© Turku U
niversity Hospital, Finland
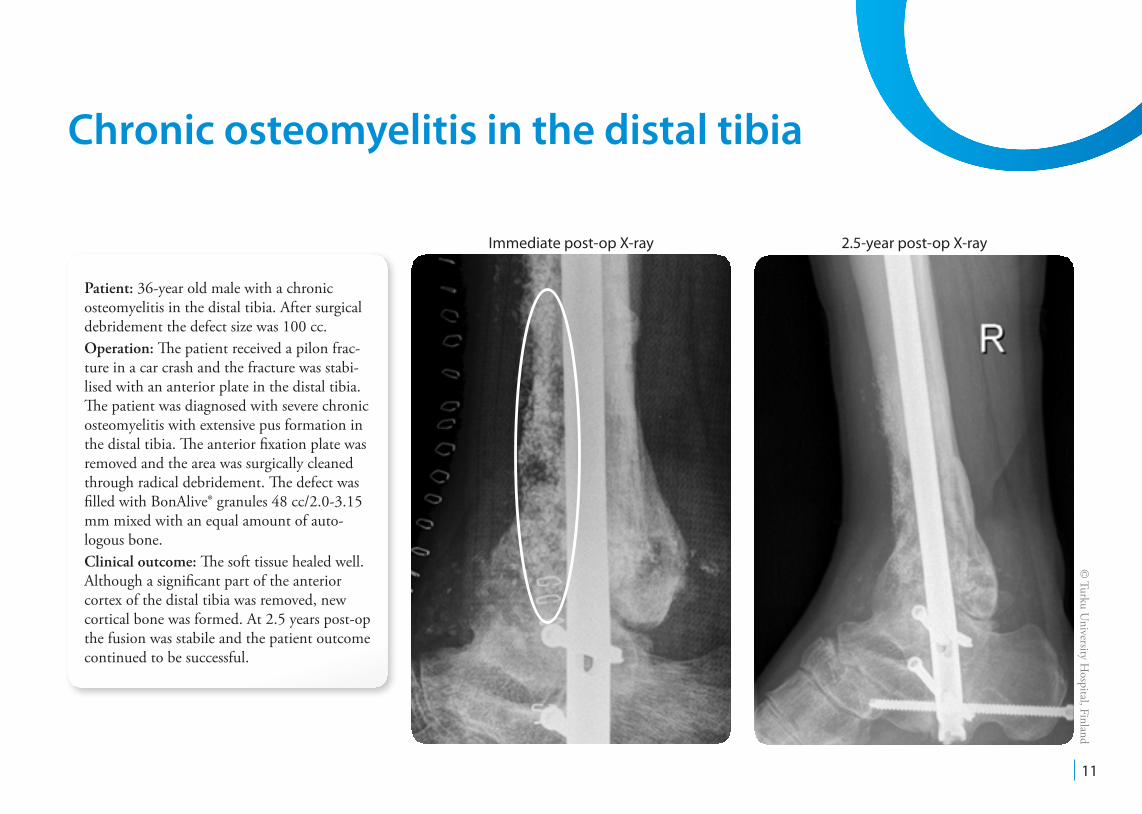
Immediate post-op X-ray 2.5-year post-op X-ray
Patient: 36-year old male with a chronic osteomyelitis in the distal tibia. After surgical debridement the defect size was 100 cc.Operation: The patient received a pilon frac-ture in a car crash and the fracture was stabi-lised with an anterior plate in the distal tibia. The patient was diagnosed with severe chronic osteomyelitis with extensive pus formation in the distal tibia. The anterior fixation plate wasremoved and the area was surgically cleaned through radical debridement. The defect was filled with BonAlive® granules 48 cc/2.0-3.15 mm mixed with an equal amount of auto-logous bone.Clinical outcome: The soft tissue healed well. Although a significant part of the anterior cortex of the distal tibia was removed, new cortical bone was formed. At 2.5 years post-op the fusion was stabile and the patient outcome continued to be successful.
Chronic osteomyelitis in the distal tibia

12
Pre-op Pre-op X-ray
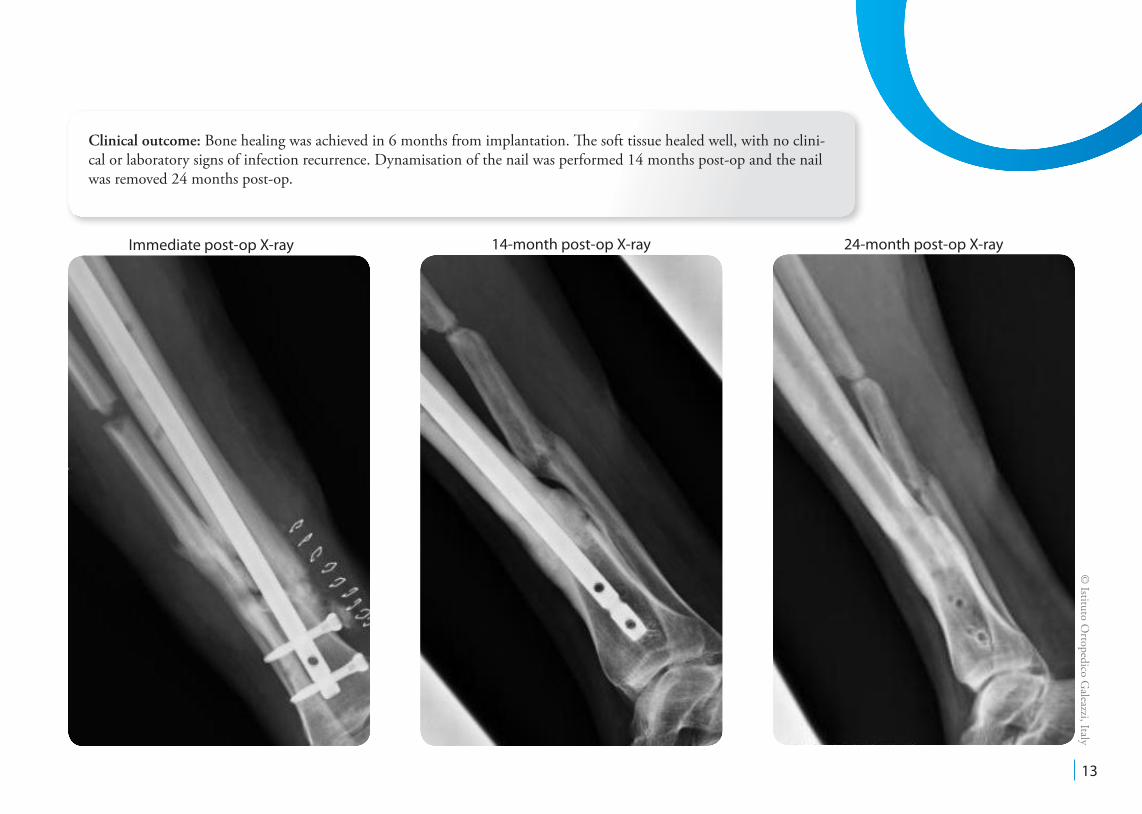
Patient: 32-year old female, type A host, was in a car crash and received an exposed pilon fracture that was stabilized with an external fixator.Bacterial species: Staphylococcus aureus.Surgeon: Prof. Carlo Romanó, Istituto Ortopedico Galeazzi, Milan, Italy.Operation: The patient was diagnosed with septic non-union 9 months after trauma. The patient refused new external fixation. The external fixator was re-moved and, after 15 days, an osteotomy of the fibula, debridement of the non-union septic focus, local application of BonAlive® granules (20 cc/1.0-2.0 mm granules) and intramedullary nailing were performed.
© Istituto O
rtopedico Galeazzi, Italy
Chronically infected non-union of the distal tibia
13
© Istituto O
rtopedico Galeazzi, Italy
Immediate post-op X-ray 14-month post-op X-ray 24-month post-op X-ray
Clinical outcome: Bone healing was achieved in 6 months from implantation. The soft tissue healed well, with no clini-cal or laboratory signs of infection recurrence. Dynamisation of the nail was performed 14 months post-op and the nail was removed 24 months post-op.
14
© H
elsinki University C
entral Hospital, Finland
Bioactive glass S53P4 as bone graft substitute in treatment of osteomyelitis. Lindfors NC, J. Bone. 2010;47:212-218.
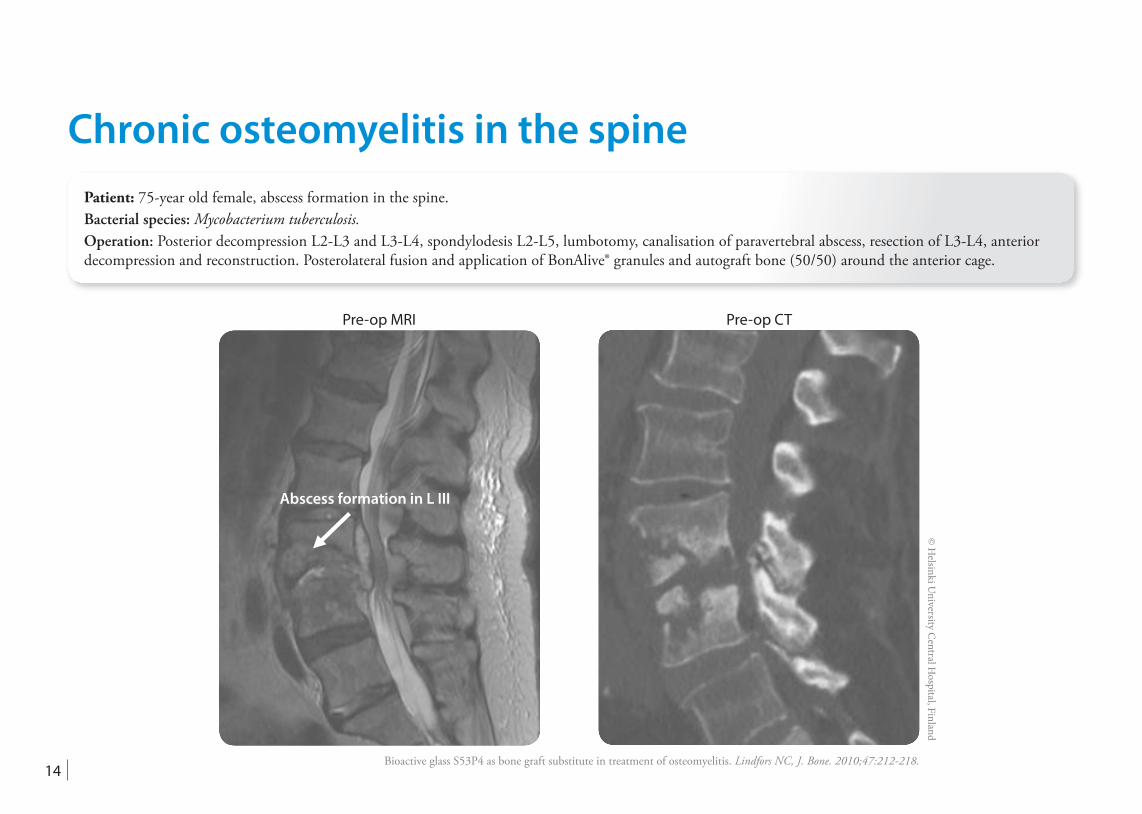
Abscess formation in L III
Pre-op MRI Pre-op CT
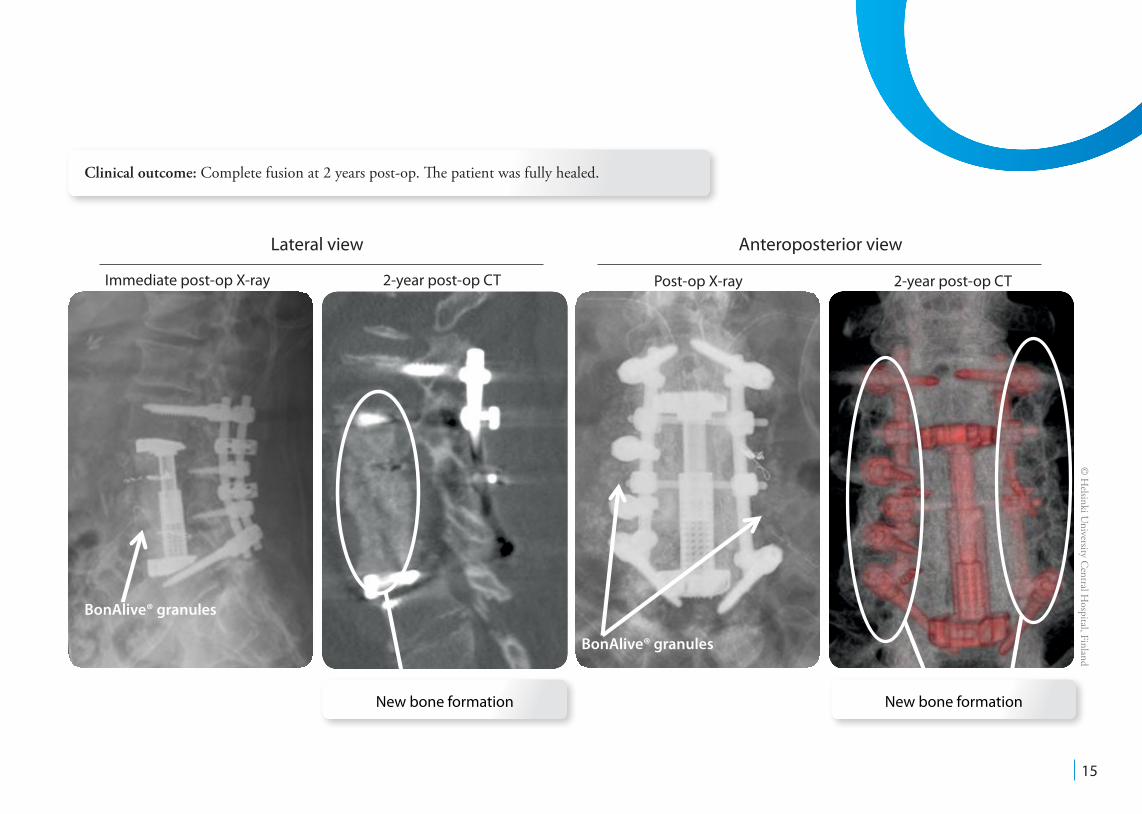
Patient: 75-year old female, abscess formation in the spine. Bacterial species: Mycobacterium tuberculosis.Operation: Posterior decompression L2-L3 and L3-L4, spondylodesis L2-L5, lumbotomy, canalisation of paravertebral abscess, resection of L3-L4, anterior decompression and reconstruction. Posterolateral fusion and application of BonAlive® granules and autograft bone (50/50) around the anterior cage.
Chronic osteomyelitis in the spine
15
Clinical outcome: Complete fusion at 2 years post-op. The patient was fully healed.
© H
elsinki University C
entral Hospital, Finland
Immediate post-op X-ray 2-year post-op CT Post-op X-ray 2-year post-op CT
BonAlive®
BonAlive® granules
BonAlive® granules
Lateral view Anteroposterior view
New bone formationNew bone formation
16
Mechanism of action (osteostimulation*)Osteoblast response to continuous phase macroporous scaffolds under static and dynamic culture conditions.Meretoja VV, Malin M, Seppälä JV, Närhi TO. J Biomed Mater Res. 2008;89A(2):317-325.
Molecular basis for action of bioactive glasses as bone graft substitute.Välimäki VV, Aro HT. Scandinavian Journal of Surgery. 2006;95(2):95-102.
Intact surface of bioactive glass S53P4 is resistant to osteoclastic activity.Wilson T, Parikka V, Holmbom J, Ylänen H, Penttinen R. J Biomed Mater Res. 2005;77A(1):67-74.
Granule size and composition of bioactive glasses affect osteoconduction in rabbit.Lindfors NC, Aho AJ. J Mater Sci: Mater Med. 2003;14(4):265-372.
Osteoblast differentiation of bone marrow stromal cells cultured on silica gel and sol-gel-derived titania.Dieudonné SC, van den Dolder J, de Ruijter JE, Paldan H, Peltola T, van ‘t Hof MA, Hap-ponen RP, Jansen JA. Biomaterials. 2002;23(14):3041-3051.
Histomorphometric and molecular biologic comparison of bioactive glass granules and autogenous bone grafts in augmentation of bone defect healing.Virolainen P, Heikkilä J, Yli-Urpo A, Vuorio E, Aro HT. J Biomed Mater Res. 1997;35(1):9-17.
*non-osteoinduction
Inhibition of bacterial growthAntibacterial effects and dissolution behavior of six bioactive glasses.Zhang D, Leppäranta O, Munukka E, Ylänen H, Viljanen MK, Eerola E, Hupa M, Hupa L. J Biomed Mater Res. 2010;93A(2):475-483.
Bactericidal effects of bioactive glasses on clinically important aerobic bacteria.Munukka E, Leppäranta O, Korkeamäki M, Vaahtio M, Peltola T, Zhang D, Hupa L, Ylänen H, Salonen JI, Viljanen MK, Eerola E. J Mater Sci: Mater Med. 2008;19(1):27-32.
Antibacterial effect of bioactive glasses on clinically important anaerobic bacteria in vitro.Leppäranta O, Vaahtio M, Peltola T, Zhang D, Hupa L, Ylänen H, Salonen JI, Viljanen MK, Eerola E. J Mater Sci: Mater Med. 2008;19(2):547-551.
In situ pH within particle beds of bioactive glasses.Zhang D, Hupa M, Hupa L. Acta Biomaterialia. 2008;4(5):1498-1505.
Factors controlling antibacterial properties of bioactive glasses.Zhang D, Munukka E, Hupa L, Ylänen H, Viljanen MK, Hupa M. Key Engineering Materi-als. 2007;330-332:173-176.
Comparison of antibacterial effect on three bioactive glasses.Zhang D, Munukka E, Leppäranta O, Hupa L, Ylänen H, Salonen J, Eerola E, Viljanen MK, Hupa M. Key Engineering Materials. 2006;309-311:345-348.
Interactions between the bioactive glass S53P4 and the atrophic rhinitis-associated microorganism Klebsiella ozaenae.Stoor P, Söderling E, Grenman R. J Biomed Mater Res. 1999;48(6):869-874.
Antibacterial effects of a bioactive glass paste on oral micro-organisms.Stoor P, Söderling E, Salonen JI. Acta Odontol Scand. 1998;56(3):161-165.
Interactions between the frontal sinusitis-associated pathogen Heamophilus Influenzae and the bioactive glass S53P4.Stoor P, Söderling E, Andersson OH, Yli-Urpo A. Bioceramics. 1995;8:253-258.
References
The reputation of BonAlive® is built on solid clinical evidence• Over 20 peer-reviewed published clinical articles• More than a decade of human prospective randomized clinical data
17
Chronic osteomyelitisThrough the looking glass; bioactive glass S53P4 (BonAlive®) in the treatment of chronic osteomyelitis.McAndrew J, Efrimescu C, Sheehan E, Niall D. Ir J Med Sci. 2013;182(3):509-511.
Clinical Experience on Bioactive Glass S53P4 in Reconstructive Surgery in the Upper Extremity Showing Bone Remodelling, Vascularization, Cartilage Repair and Antibacte-rial Properties of S53P4. Lindfors NC. J Biotechnol Biomaterial. 2011;1(5). (An open access journal.)
Bioactive glass S53P4 as bone graft substitute in treatment of osteomyelitis. Lindfors NC, Hyvönen P, Nyyssönen M, Kirjavainen M, Kankare J, Gullichsen E, Salo J. Bone. 2010;47:212-218.
Preclinical publicationsBioactive glass as bone-graft substitute for posterior spinal fusion in rabbit.Lindfors NC, Tallroth K, Aho AJ. J Biomed Mater Res. 2002;63B(2):237-244.
Tissue response to bioactive glass and autogenous bone in the rabbit spine.Lindfors NC, Aho AJ. Eur Spine J. 2000;9:30-35.
Bioactive glass and calcium carbonate granules as filler material around titanium and bioactive glass implants in the medullar space of the rabbit tibia.Turunen T, Peltola J, Helenius H, Yli-Urpo A, Happonen, R. Clin Oral Impl Res. 1997;8:96-102.
Long term behaviour of bioactive glass cone and granules in rabbit bone.Heikkilä JT, Salonen H, Yli-Urpo A, Aho AJ. Bioceramics. 1996;9:123-126.
Protein adsorption properties of bioactive glasses compared to their behaviour in rabbit tibia.Brink M, Söderling E, Turunen T, Karlsson KH. Bioceramics. 1995;8:471-476.
Bone formation in rabbit cancellous bone defects filled with bioactive glass granules.Heikkilä JT, Aho HJ, Yli-Urpo A, Happonen R, Aho AJ. Acta Orthopaedica. 1995;66(5):463-467.
Orthopaedics & traumaTrauma
Bioactive glass S53P4 and autograft bone in treatment of depressed tibial plateau frac-tures. A prospective randomized 11-year follow-up. Pernaa K, Koski I, Mattila K, Gullichsen E, Heikkilä J, Aho AJ, Lindfors N. J Long-term Eff Med Impl. 2011;21(2):139-148.
Bioactive glass granules: a suitable bone substitute material in the operative treatment of depressed lateral tibial plateau fractures: a prospective, randomized 1 year follow-up study.Heikkilä JT, Kukkonen J, Aho AJ, Moisander S, Kyyrönen T, Mattila K. J Mater Sci: Mater Med. 2011;22(4):1073-1080.
Instrumented spondylodesis in degenerative spondylolisthesis with bioactive glass and autologous bone. A prospective 11-year follow-up.Frantzén J, Rantakokko J, Aro H, Heinänen J, Kajander S, Koski I, Gullichsen E, Kotilainen E, Lindfors N. J Spinal Disorder Tech. 2011;24(7):455-461.
Posterolateral spondylodesis using bioactive glass S53P4 and autogenous bone in instru-mented unstable lumbar spine burst fractures - A prospective 10-year follow-up study.Rantakokko J, Frantzén J, Heinänen J, Kajander S, Kotilainen E, Gullichsen E, Lindfors N. Scan J Surg. 2012;101(1):66–71.
Benign bone tumourA prospective randomized 14-year follow-up study of bioactive glass and autogenous bone as bone graft substitutes in benign bone tumors.Lindfors NC, Koski I, Heikkilä JT, Mattila K, Aho AJ. J Biomed Mater Res. 2010;94B(1):157-164.
Treatment of a recurrent aneurysmal bone cyst with bioactive glass in a child allows for good bone remodelling and growth.Lindfors NC. Bone. 2009;45:398-400.
Bioactive glass and autogenous bone as bone graft substitutes in benign bone tumors.Lindfors NC, Heikkilä J, Koski I, Mattila K, Aho AJ. J Biomed Mater Res. 2009;90B(1):131-136.
mikä ref pitää poistaa?
18
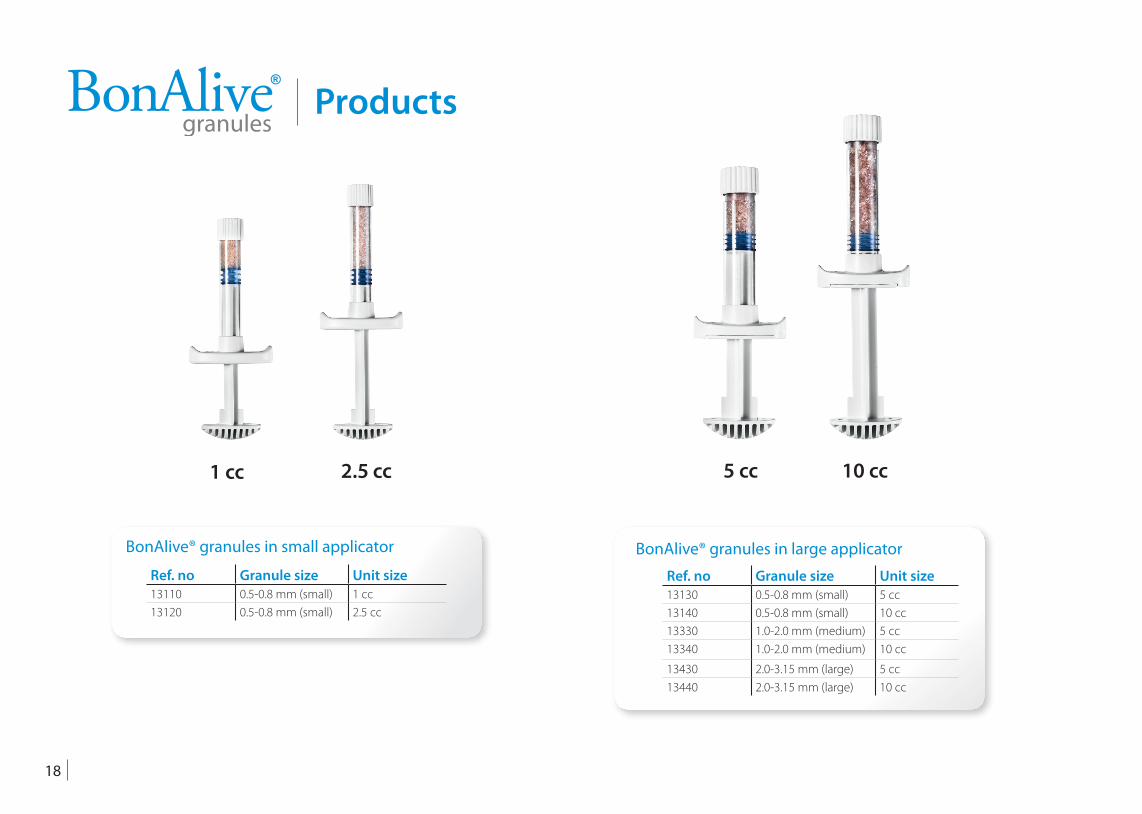
Ref. no Granule size Unit size13110 0.5-0.8 mm (small) 1 cc13120 0.5-0.8 mm (small) 2.5 cc
BonAlive® granules in small applicator
Ref. no Granule size Unit size13130 0.5-0.8 mm (small) 5 cc13140 0.5-0.8 mm (small) 10 cc13330 1.0-2.0 mm (medium) 5 cc13340 1.0-2.0 mm (medium) 10 cc
13430 2.0-3.15 mm (large) 5 cc13440 2.0-3.15 mm (large) 10 cc
BonAlive® granules in large applicator
1 cc 2.5 cc 5 cc 10 cc
Products
19
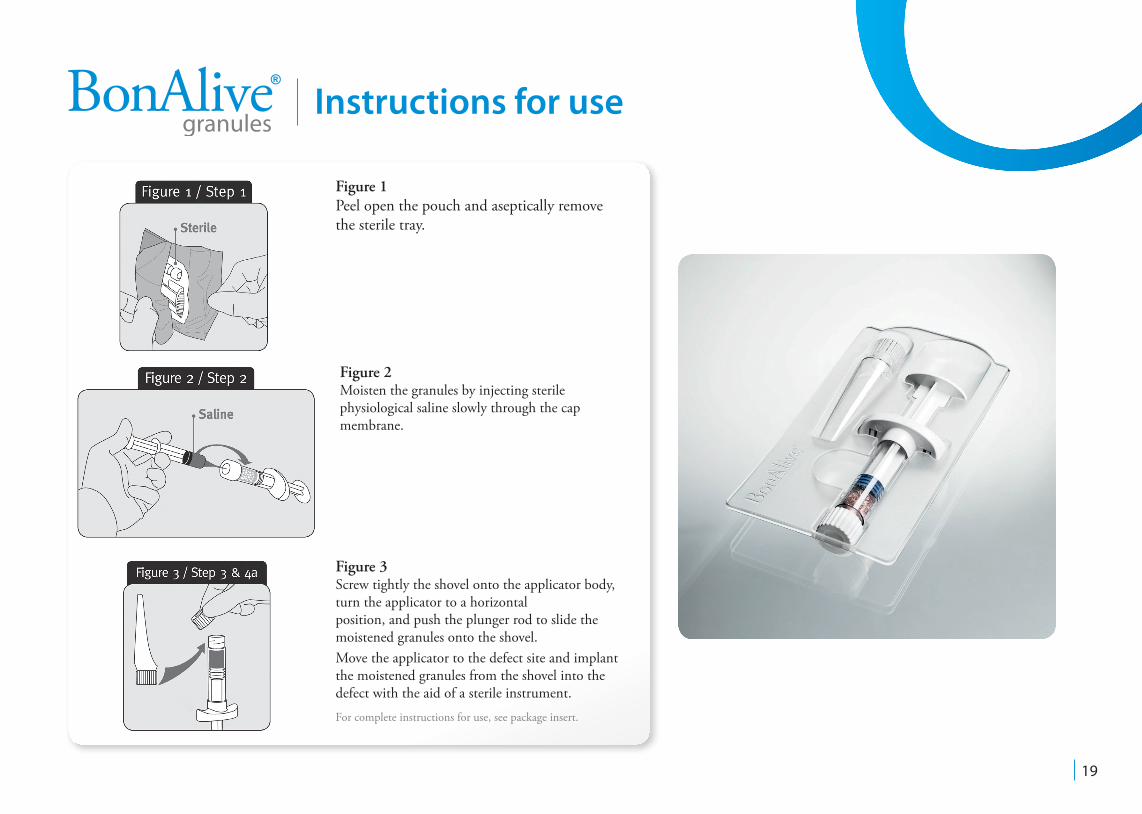
Figure 1Peel open the pouch and aseptically remove the sterile tray.
Figure 2Moisten the granules by injecting sterile physiological saline slowly through the cap membrane.
Figure 3Screw tightly the shovel onto the applicator body, turn the applicator to a horizontal position, and push the plunger rod to slide the moistened granules onto the shovel.Move the applicator to the defect site and implant the moistened granules from the shovel into the defect with the aid of a sterile instrument.
Instructions for use
For complete instructions for use, see package insert.
HeadquartersBonAlive Biomaterials LtdTel. +358 (0)401 77 44 00Fax +358 (0)421 91 77 44 [email protected] 1220750 Turku, Finlandwww.bonalive.com
DistributorsEUROPE
AUSTRIAOlympus Biotech Österreich GmbHTel. 0800 204 [email protected]ße 5/141070 Wien, Austriawww.olympusbiotech.com
BENELUXLeander Healthcare B.V.Tel. +31 6 418 14 [email protected] 1673450 AD Vleuten The Netherlandswww.leanderhealthcare.com
DENMARKMediplast A/STel. +45 4344 [email protected]øjs Allé 174-1762610 Rødovre, Denmarkwww.mediplast.com
FINLANDBonAlive Biomaterials LtdTel. +358 401 77 44 [email protected] 1220750 Turku, Finlandwww.bonalive.com
FRANCEOlympus Biotech Europe SASTel. +33 [email protected] Quai Charles De Gaulle69006 Lyon, Francewww.olympusbiotech.com
GERMANYOlympus Biotech Deutschland GMBHTel. +49 211 690 [email protected] Wall 50,20354 Hamburg, Germanywww.olympusbiotech.com
IRELANDOlympus Biotech InternationalTel. +353 62 585 [email protected] Business ParkLimerick, Irelandwww.olympusbiotech.com
ITALYMedix ItaliaTel. +39 011 [email protected] Roma n. 10110123 Torino, Italywww.medixitaliasrl.it
NORWAYMediplast Innova ASTel. +47 22 09 45 [email protected] 302a1188 Oslo, Norwaywww.mediplast.com
POLANDMedical CommunicationsTel. +48 22 651 97 [email protected]. Powsinska 3402-903, Warszawa, Polandwww.medical.pl
PORTUGALAtos Medical Spain SL.Sucursal em PortugalTel. +351 96 [email protected] da Liberdade, Nº78 - 1ºBVale de Milhaços2855 - 385 CorroiosPortugalwww.atosmedical.se
ROMANIAGTS Solution SRLTel. +40 (21) 256 [email protected], Nicolae Rosu StreetDistrict 3, 033106 Bucharest, Romaniawww.gotosolution.com
SPAINBemed Productos Y Distribuciones, S.L.Tel. +34 94 674 [email protected] Olekari, 46 C - 1º B48100 Munguia, Spain
SWEDENMediplast ABTel. +46 40 671 23 [email protected] 29SE-21376 Malmö, Swedenwww.mediplast.com
SWITZERLANDMedeco-CH SàrlTel. +41 22 307 01 [email protected] de Trélex 81266 Duillier, Switzerlandwww.medeco-ch.com
TURKEYFiksmed Tic. Ltd. StiTel. +90 312 284 15 [email protected] Mah.Muhsin yazicioglu cad asmalibache apt no:7/1 Cukurambar
Ankara, Turkeywww.fiksmed.com.tr
UNITED KINGDOMOlympus Biotech UK LimitedTel. +44 1923 853 [email protected] Gables House30 Letchmore RoadRadlett, Herts, WD7 8HT, Uwww.olympusbiotech.com
MIDDLE EAST/ASIA-PACIFICAUSTRALIADevice Technologies Australia Pty LtdTel. +1 800 429 [email protected]/25 Frenchs Forest RoadFrenchs Forest, NSW 2086, Australiawww.device.com.au
INDIAShreyaas Health CareTel. +91 422 [email protected]. 73, II Floor, Lal Bagathur Colony, Peelamedu641004 Coimbatore, Tamilnadu, Indiawww.shreyaas.net
ISRAELDa-Mor Ltd.Tel. +972 9 954 3616 [email protected] Beeri Street46456 Herzeliya, Israelwww.da-mor.co.il
KINGDOM OF SAUDI-ARABIAHusn Al Emirat EstTel. +966 1 453 [email protected] Box 93341, Riyadh 11673Kingdom of Saudi Arabiawww.alewan.com
MALAYSIAMalex Medical Asia (M) Sdn BhdTel. +603 7880 [email protected], Block E1, Jalan PJU 1/42Dataran Prima, 47301 Petaling JayaSelangor, Malaysiawww.malexmedical.com
NEW ZEALANDDevice Technologies New ZealandTel. +64 9 913 2000 [email protected] Arrenway, AlbanyAuckland, New Zealandwww.device.co.nz
TAIWANChi Fu Trading Co. Ltd.Tel. +886 2 2790 [email protected], Lane 77, Xin Ai Road7th Floor, Neihu DistrictTaipei 11494, Taiwanwww.chifupharma.com
UNITED ARAB EMIRATESBayan Medical Co.Tel. [email protected] 320, Emarat Atrium Bldg,Sheikh Zayed Road Dubai, United Arab Emirateswww.bayanmed.com
AMERICASBRAZILOssis MedicalTel. +55 11 [email protected] Lopes da Silva, 890- Cj.1.30505641-030, São Paulo, SP, Brasilwww.ossis.com.br
CENTRAL AMERICA AND CARIBBEANKaisermed SA de CVTel. +1 954 850 [email protected]
Santa Tecla, LLEl Salvador
CHILEInternational Medical Products ChileTel. +59 9 [email protected] Sucre N° 1389 Ñuñoa Santiago, Chilewww.impchile.cl
AFRICA
SOUTH-AFRICAStratmed Tel. +27 21 68 55 [email protected] Thicket road, Rosebank7705, Cape Town, South-Africawww.stratmed.co.za
OTHER REGION
91316f/2
Contact details
![Cross-kingdom inhibition of bacterial virulence and ......QS reporter strains and the QS autoinducers for each bacterial species [18–20] were incubated in the presence of crude kefir](https://img.pdfslide.net/doc/110x75/6137722b0ad5d20676489fe6/cross-kingdom-inhibition-of-bacterial-virulence-and-qs-reporter-strains.jpg)




























