-
8/11/2019 Injury Patterns in Vertebral Trauma
1/10
State-of-the-Art Emergency and Trauma Radiology 45
Keywords:CT, mechanisms of injury,
radiography, spine, trauma, vertebral injuries
1Department of Diagnostic Radiology, Allegheny
General Hospital, 320 E North Ave., Pittsburgh,
PA 15212-4772. Address correspondence to
R. H. Daffner ([email protected]).
Vertebral injuries, like those to the peripheral skeleton, occur
in a specific
and predictable pattern that is strictly dependent on the
mechanism of injury.
The pattern may be easily recognized by the changes that the
injury produces on
imaging studies. These patterns are referred to as the
fingerprints of the in-
jury. Injuries due to a particular mechanism produce the same
imaging changes
regardless of the location. Recognizing the pattern of the
injury allows one topredict the full extent of that injury.
All skeletal injuries occur in a specific and predictable
pattern that is solely
dependent on the mechanism of injury. Injuries to the vertebral
column obey
the same mechanical principles as those that occur in the
peripheral skeleton.
The pattern of the injury is recognizable by the radiographic or
CT changes pro-
duced. I refer to these patterns as the fingerprints of the
injury [14]. Injuries
due to any particular mechanism will produce the same
radiographic changes
regardless of the location. It matters not whether the injury
has occurred in the
cervical portion of the vertebral column or in the thoracic or
lumbar regions.
The changes due to a particular mechanism will be identical
regardless of the
location (cervical, thoracic, or lumbar). It is important to
recognize the pattern
because then it is easy to predict the full extent of that
injury. The radiographic
changes that an injury produces are typically referred to as the
footprints of
the injury. The fingerprints identify the extent of injury
[14].
The diagnosis of vertebral injuries also relies on the same
principles as those
used for peripheral injuries. It is important to completely
study the suspected
bone(s) involved. In the peripheral skeleton, that means
including the joint
above and below all suspected levels of injury. The vertebral
column, although
consisting of 33 separate bones, functions as a single long
bone. This means
that to completely study the spine it is necessary to include
all structures be-
tween the skull and the sacroiliac joints (the joints above and
below). This is of
practical experience when one considers that multiple
noncontiguous vertebral
injuries occur in approximately 25% of patients [1].
Mechanisms of Injury and Their Radiographic FingerprintsThere
are four basic mechanisms of vertebral injuries: flexion,
extension,
shearing, and rotary. Shearing and rotary injuries are
frequently associated with
some degree of flexion. Flexion injuries occur throughout the
vertebral column.
Extension injuries occur primarily in the cervical region.
Shearing and rotary in-
juries typically occur in the thoracolumbar junction and lumbar
region [5, 6].
Flexion Injuries
Flexion injuries are the most common injuries to the vertebral
column; they
occur in four varieties: simple, burst, distraction, and
dislocation [14, 7, 8].
Injury Patterns inVertebral TraumaRichard H. Daffner1
-
8/11/2019 Injury Patterns in Vertebral Trauma
2/10
46 2008 ARRS Categorical Course
Daffner
All are based on a similar mechanism. The type and extent of
injury depends on the forces involved, including the degree
of flexion and the amount of axial loading. The typical
injury
results from forward flexion when the fulcrum of motion is
approximately through the posterior third of the
intervertebral
disk [1]. In the least severe injury, anterior compression
occursalong the superior portion of the vertebral body
immediately
beneath the flexing vertebra. This produces anterior
compres-
sion of various degrees. Typically, the fracture line
propagates
posteriorly with or without communication to the interverte-
bral disk space. These fractures are referred to as simple
frac-
tures and involve no injury to the posterior structures or to
the
posterior third of the disk.
With an increase in the flexion force or an increase in the
degree of axial loading, the vertebra literally explodes,
driv-
ing fragments posteriorly into the vertebral canal to
produce
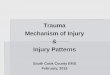
the burst fracture. A variant of this fracture occurs when
the
force is sufficient to split the vertebra sagittally, both
anteriorly
and posteriorly (Fig. 1). If the fulcrum of forward flexion
ismoved anteriorly, as occurs in individuals wearing a lap-type
seat belt only, the primary injuring force is directed at the
pos-
terior structures, with rupture of the interspinous
ligaments,
facet ligaments, ligamenta flava, and, ultimately, the
posterior
longitudinal ligament.
Distraction injuries may take two forms. The first is severe
posterior ligament damage with subsequent widening of the
D
Fig. 1Burst fracture of L3 vertebra in 52-year-old
woman.A,Lateral radiograph shows compression of superior aspect of
L3 and displacement of bone fragment anteriorly. In addition,
segment of superioraspect of posterior vertebral body line has been
displaced posteriorly (arrow).B,Frontal radiograph shows widening
of interpedicle space of L3 (double arrow).C,Sagittal reconstructed
CT image shows this displaced fragment encroaching on vertebral
canal ( arrow).D,Axial CT image shows displaced fragment in
vertebral canal (asterisk).E,Axial image slightly lower than Dshows
sagittal cleavage through spinous process (arrow).
E
A CB
-
8/11/2019 Injury Patterns in Vertebral Trauma
3/10
State-of-the-Art Emergency and Trauma Radiology 47
Vertebral Trauma
interlaminar (or interspinous) space. This pattern is typical
of
the hyperflexion sprain [1, 3] (Fig. 2). Alternatively, the
frac-
ture may extend in a horizontal fashion through the
posterior
elements and through the vertebral body to produce the so-
called Chance-type fracture [9, 10] (Fig. 3). Finally,
severely
forceful flexion injuries can produce a dislocation, which
may
occur with or without associated fractures.
Unilateral (Fig. 4) or bilateral facet locks occur as a
result
of flexion mechanisms. Anterolisthesis resulting from
flexion
injuries is always associated with widening of the
interlaminar
A
Fig. 2Hyperflexion sprain in 22-year-oldman.A,Lateral radiograph
shows slightanterolisthesis of C4 on C5 and widening ofinterlaminar
space (asterisk).
B,T2-weighted MR image shows rupture ofposteriorlongitudinal
ligament and diskherniation (arrow).
B
A C
Fig. 3Chance fracture of L1 in 40-year-old man.A,Frontal view
shows widening of interspinous space (asterisk). Note fracture
through pedicle of L1 on left that extends into transverse process
(arrow).B,Lateral radiograph shows anterior compression of L1 and
posterior distraction.C,Axial CT image shows compression of
anterior portion of vertebral body and naked facet on right side (
arrow). Contiguous sections above andbelow this image (not shown)
showed similar naked facets. Note fragmentation of pedicle on
left.
B
-
8/11/2019 Injury Patterns in Vertebral Trauma
4/10
48 2008 ARRS Categorical Course
Daffner
space, widening of the facet joints (including naked
facets),
and abnormal alignment of the spinolaminar line [1, 3].
Facet abnormalities are common in flexion injuries. Nor-
mally, on a CT scan, the facet joints have the appearance of
a
hamburger. Unilateral or bilateral facet dislocations result
in
the reverse hamburger bun sign [11]. Naked facets may be
easily recognized on CT scans as unopposed bony structures
posteriorly, where one would normally expect to see the
adja-
cent vertebra. This appearance should never occur normally
on
more than one single slice.
Flexion injuries produce the following changes that may be
seen on radiographs or on CT scans: compression, fragmenta-
tion, and burst fractures of vertebral bodies;
anterolisthesis;
wide interlaminar space; teardrop fragments typically from
the anteroinferior margin of the vertebral bodies; facet
abnor-
malities that include fractures or unilateral or bilateral
blocks;
an abnormal posterior vertebral body line [12]; and
narrowing
of the disk space above the level of injury [14]. These
find-
ings are summarized in Appendix 1.
Extension InjuriesExtension injuries occur in three distinct
varieties: simple,
distraction, and dislocation [14, 13, 14]. Extension mecha-
nisms are far more common in the cervical region but may
be seen in the thoracic and lumbar regions. It is not rare
to
encounter the latter in patients with rigid spine disease
(anky-
losing spondylitis or diffuse idiopathic skeletal
hyperostosis
[DISH]) [15] (Fig. 5). Important cervical extension injuries
include the hangmans fracture of C2 and the extension sprain
[1, 13, 14] (Fig. 6).
All extension injuries have in common disruption of the
anterior longitudinal ligament with or without association
of
fracture and a varying degree of injury to the
intervertebral
disk. The most important imaging finding that may be seen on
either radiographs or CT scans is widening of the disk space
(Figs. 5 and 6). This finding is so important that whenever it
is
encountered, patients should be suspected of having an
exten-
sion injury through that level until proven otherwise. Other
ra-
diographic findings include small triangular avulsion
fractures
from the anterior disk margins of the vertebra either above
or
below the level of injury.
Retrolisthesis is typical in severe injuries. In a severe
but
rare form of extension injury, fractures occur through the
neu-
ral arch. Often these are associated with anterolisthesis.
This
may lead to some confusion because anterolisthesis is more
typical of flexion injuries [1, 13, 14]. However, the
mechanism
should be clear when the anterolisthesis is accompanied by
a normal spinolaminar line and normal interlaminar distance.
These two anatomic landmarks are typically abnormal in the
more common flexion-type of injury. Appendix 2 summarizes
the fingerprints of extension injury.
Shearing Injuries
Thoracolumbar injuries typically cluster between T11 and
L2. The reason for this is the facet reorientation that
occurs
from the coronal plane to the sagittal plane. Indeed, at L1,
the
facet joints are oriented at 90, which strongly resists any
kind
of side-to-side or rotary motion [16]. In addition, the
change
from the kyphotic thoracic curve to the lordotic lumbar
curve
and the loss of the stabilizing effects of the ribs increase
the
A CFig. 4Unilateral facet lock at C5C6 in 73-year-old
woman.A,Lateral radiograph shows anterolisthesis of C5 on C6 (
arrow). Note widening of interlaminar space (asterisk).B,Axial CT
image shows locked facet on right (arrow). Note that appearance is
that of a reversed hamburger bun.C,Sagittal reconstructed CT image
shows facet lock (arrow).
B
-
8/11/2019 Injury Patterns in Vertebral Trauma
5/10
State-of-the-Art Emergency and Trauma Radiology 49
Vertebral Trauma
A
C
Fig. 5Extension injuries in patients with rigid
spinedisease.A,Lateral radiograph in 44-year-old man with
ankylosingspondylitis shows widening of T9 disk space (asterisk).
Noteanterior ankylosis and ky photic angulation at
T11T12.B,Sagittal reconstructed CT image in same patient as
inAshows wide disk space (arrow). Kyphotic angulation at
T11T12 is due to flexion injury at that level.C
and
D,Lateral radiograph (C) and sagittal reconstructedimage (D) in
72-year-old man with diffuse idiopathicskeletal hyperostosis (DISH)
show widening of T8 disk space(asterisk). Wide disk space is
hallmark of extension injury.
B
D
mechanical vulnerability of the region to all de-
grees of motion.
Shearing injuries are the result of horizontal
or obliquely directed forces with associated for-
ward or lateral flexion [1, 3, 5, 6, 13]. The most
common cause that we encounter in our practice
is ejection from a motor vehicle in which the indi-vidual
strikes the upper or lower part of the body
while the other half of the body continues moving
in the same direction as the initial ejection. The
result of shearing injuries is a pattern that is quite
different from that seen with either flexion or ex-
tension injuries.
Shearing injuries typically produce imaging
features of lateral distraction and lateral disloca-
tion. The vertebrae may have a windswept appear-
ance (Fig. 7). In addition, this mechanism produces
transverse process or rib fractures. Anterolisthesis
is also typically present. Lateral fragmentation
that is linear in the direction of the deforming
force may be seen on a CT scan (Fig. 7C).
The importance of recognizing shearing frac-
tures is that the injury initially may resemble a
burst fracture. Because these injuries are typically
unstable (see the following text), the treatment is
radically different. Treatment of burst fractures
is directed at providing stability along the sagit-
tal plane. Treatment of shearing injuries must be
directed toward reestablishing stability not only in
the sagittal plane but also in the oblique planes.
It is not difficult to differentiate shearing inju-
ries from burst fractures when one knows the typi-cal signs
produced by each. Shearing injuries typi-
cally have a greater degree of lateral displacement
and a tendency for lateral dislocation. Transverse
process or rib fractures are also hallmarks of this
injury (and of rotary injuries). Furthermore, the
linear oblique and windswept appearance on both
radiographs and CT scans is also typical. Burst
fractures, on the other hand, have little tendency
to dislocate, even along the sagittal plane. If the
-
8/11/2019 Injury Patterns in Vertebral Trauma
6/10
50 2008 ARRS Categorical Course
Daffner
vertebra has been split along the sagittal plane, there will
be
widening of the interpedicle distance reflecting that (Fig.
1).
Finally, on CT, there is a linear sagittal distribution of
frag-
ments [1, 3]. The fingerprints of shearing injuries are listed
in
Appendix 3.
Rotary Injuries
Rotary injuries may be seen in two locations. The most com-
mon location is at the thoracolumbar junction. Once again,
the
unique anatomy of that region sets the stage for these
injuries
to occur when the right mechanism is applied [16]. The
second
location for rotary injuries is the atlantoaxial region,
wherepatients may suffer a pure ligamentous injury referred to
as
atlantoaxial rotary subluxation or frank dislocation in
atlanto-
axial rotary fixation [17]. Rotary injuries to the
thoracolumbar
region are most frequently the result of motor vehicle
crashes
in which an individual is ejected. The mechanism of injury
is
an obliquely directed force to the upper torso with twisting
of the lower torso accompanied by lateral deflection. There
is
generally some degree of forward or lateral flexion in
addition
to the twisting mechanism [1, 3].
The imaging findings of rotary injuries are distinct and
sug-
gestive. There is severe fragmentation of the vertebral
body.
Often, a fragment of bone from the inferior vertebra is torn
from the anterosuperior margin of the vertebral body (Fig.
8).
Because of the severe fragmentation, the vertebra is
frequent-
ly pulverized, leading to the designation of these injuries
as
grinding. Disruption of the posterior vertebral body line
of-
ten leads to this injury being confused with burst
fractures.
Consequently, there is canal encroachment. Like shearing
injuries, transverse process or rib fractures typically
occur.
These features alone serve to differentiate this injury from
burst fractures. There is usually anterolisthesis,
frequentlyposterior distraction, and facet distraction. On CT, the
bone
fragments are displayed in a circular or concentric fashion.
Because of the rotary mechanism, one facet joint is
displaced
anteriorly and the other is displaced posteriorly, allowing
the
viewer to determine the exact direction in which the
rotation
occurred (Fig. 8C).
As with shearing injuries, it is important to differentiate
rotary injuries from burst fractures because the treatment
is
different. Treatment of burst fractures, as previously
mentioned,
A C
Fig. 6Cervical extension sprains.A,Lateral radiograph shows
widening of C5 disk space (asterisk) in 76-year-old man. Note small
avulsed bone fragment from anteroinferior margin of
C5(arrow).B,Lateral radiograph in 62-year-old man shows widening of
C3 disk space ( asterisk) and retrolisthesis of C3 on C4.C,Autopsy
specimen from patient in Bshows torn anterior disk space at C3 and
significant cord hemorrhage ( arrow). These injuries typically
producesevere central cord syndrome.
B
-
8/11/2019 Injury Patterns in Vertebral Trauma
7/10
State-of-the-Art Emergency and Trauma Radiology 51
Vertebral Trauma
is directed to reestablishing stability in the sagittal plane.
On
the other hand, treatment of rotary injuries is directed to
re-
establishing stability in the sagittal, axial, and coronal
planes.
Rotary injuries have a greater degree of separation and agreater
tendency to dislocate. Transverse process or rib frac-
tures are characteristic. Most characteristic is the
concentric
distribution of the bone fragments on a CT. On MRI, the
soft-
tissue injury from rotary mechanisms is much more exten-
sive. Burst fractures, on the other hand, have little
tendency
to dislocate. They may have widening of the interpedicle
dis-
tance, and, on CT, have a linear and sagittal distribution
of
bone fragments. The fingerprints of rotary injury are listed
in
Appendix 4.
Radiographic Assessmentof Vertebral Stability
Stability of the vertebral column is defined as the ability
of
the bones and ligaments that make up the column to protectthe
spinal cord under normal function [1, 18, 19]. Stability de-
pends on the integrity of certain anatomic structures that
will
not permit excessive motion to allow compromise of either
the spinal cord or the nerves. In 1983, Denis [20] created
the
concept of the three-column spine. He defined the anterior
col-
umn as those structures beginning at the anterior
longitudinal
ligament and extending posteriorly to an imaginary line ap-
proximately two thirds of the way through the vertebral body
and intervertebral disk. The middle column extended from
that
A
C
Fig. 7Shearing injury at L4L5 in 68-year-oldman.A,Frontal
radiograph shows windsweptappearance of spine at L4L5. Note loss
ofnormal anatomic boundaries between the twovertebrae.B,Lateral
radiograph shows anterolisthesis of
L4 on L5. Note indistinctness of inferior marginof body of
L4.CandD,Axial CT images show linearoblique distribution of bone
fragments. Notetransverse process fracture on left.
Windsweptappearance is characteristic of shearinginjuries.
B
D
-
8/11/2019 Injury Patterns in Vertebral Trauma
8/10
52 2008 ARRS Categorical Course
Daffner
line to the posterior longitudinal ligament. The posterior
col-
umn extended from the posterior longitudinal ligament to the
supraspinous ligament. Denis was able to show, through bio-
mechanical experiments, that the integrity of the middle
col-
umn was key to overall anatomic stability in the spine. From
a
practical standpoint, disruption of two contiguous zones
(an-terior and middle columns or middle and posterior columns)
produced instability. Disruption of a single column (anterior
or
posterior) did not result in instability.
What, then, are the radiographic signs of instability? There
are five, and they may be seen on radiographs, CT, or MRI:
displacement, widening of the interlaminar (interspinous)
space, widening of the facet joint, widening of the
interpedicle
distance, and an abnormal posterior vertebral body line [1,
18,
19]. Displacement (Fig. 8) generally results in disruption of
all
three columns. Widening of the interlaminar space and widen-
ing of the facet joint are the result of disruption posteriorly
(Fig.
2). Unless the posterior third of the disk has been torn,
widening
of the interlaminar space cannot occur, nor can facet joint
wid-
ening. Widening of the interpedicle distance indicates that
the
vertebra has been split along the sagittal plane (Fig. 1). This
mayoccur with or without an intracanalicular displaced
fragment.
Finally, an abnormality of the posterovertebral body line
(Fig.
1) indicates a disruption to the posterior third of the vertebra
and
the disk. This may occur from a variety of mechanisms.
Although most of these signs of instability occur in combi-
nation with one another, the presence of only one is
sufficient
to make the diagnosis [1, 18, 19]. Indeed, the presence of
these
signs also indicates that the patient has suffered a major
injury.
Major injuries are defined as those that produce neurologic
D
Fig. 8Rotary injury of L1 in 56-year-old man.A,Frontal
radiograph shows severe disruption
of body of L1. Fracture extends through pedicleand transverse
process on left (arrow).B,Lateral radiograph shows anterolisthesis
of
T12 on L1. Note severe fragmentation of L1.C,Sagittal
reconstructed CT image showsanterolisthesis (arrow) of T12 on L1.
Note smallbone fragment from anterosuperior aspect ofL1 in its
normal anatomic position.D,Axial CT image shows naked facet on
leftside (arrow). Note concentric distribution ofbone fragments
anteriorly.E,Axial CT image slightly lower showswidening of left
facet (arrow).
E
A CB
-
8/11/2019 Injury Patterns in Vertebral Trauma
9/10
State-of-the-Art Emergency and Trauma Radiology 53
Vertebral Trauma
deficits or have the potential to do so, or produce instability
or
have the potential to do so. They require surgical
intervention.
Minor injuries, on the other hand, require only symptomatic
and supportive treatment. Examples of major injuries are
burst
fractures, rotary (grinding) injuries, and shearing injuries.
Ex-
amples of minor injuries are spinous process fractures,
isolat-ed articular pillar fractures, and simple compression
fractures
[21]. Appendix 5 is a more complete compendium of major
injuries, and Appendix 6 lists minor injuries. Although this
concept was developed for cervical injuries, the principles
are
identical for thoracic and lumbar injuries as well.
ConclusionVertebral injuries occur in a predictable pattern that
depends
on the mechanism of injury. That pattern constitutes the
finger-
prints of the injury. The imaging findings, or fingerprints
from
any particular mechanism, are identical no matter where they
occur in the vertebral column. It is important to recognize
the
types of injuries because the treatment will be radically
differ-ent for each type.
REFERENCES
1. Daffner RH. Imaging of vertebral trauma,2nd ed. Philadelphia,
PA: Lippincott-
Raven, 1996:95 142
2. Daffner RH, Daffner SD. Vertebral injuries: detection and
implications. Eur J
Radiol 2002; 42:100116
3. Daffner RH, Daffner SD. Vertebral injuries: detection and
implications. In:
Cassar-Pullicino VN, Imhoff H, eds. Spinal trauma: an imaging
approach.Stuttgart, Germany: Thieme, 2006:8199
4. Daffner RH, Deeb ZL, Rothfus WE. Fingerprints of vertebral
trauma: a unifying
concept based on mechanisms. Skeletal Radiol1986; 15:518525
5. Denis F, Burkus JK. Shear fracture dislocations of the
thoracic and lumbar spine
associated with forceful hyperextension (lumberjack paraplegia).
Spine1992;
17:156161
6. Jeanneret B, Ho PK, Magerl F. Burstshearflexiondistraction
injuries of the
lumbar spine.J Spinal Disorders1993; 6:473481
7. Allen BL Jr, Ferguson RL, Lehmann TR, et al. A mechanistic
classification of
closed, indirect fractures and dislocations of the lower
cervical spine. Spine
1982; 7:1278. Ferguson RL, Allen BL Jr. A mechanistic
classification of thoracolumbar spine
fractures. Clin Orthop Rel Res1984; 189:7788
9. Chance GQ. Note on a type of flexion fracture of the spine.
Br J Radiol 1948;
21:452453
10. Smith WS, Kaufer H. Patterns and mechanisms of lumbar
injuries associated
with lap seat belts. J Bone Joint Surg Am1969; 51:239254
11. Daffner SD, Daffner RH. Computed tomography diagnosis of
facet dislocations:
the hamburger bun and reverse hamburger bun signs.J Emerg Med
2002;
23:387394
12. Daffner RH, Deeb ZL, Rothfus WE. The posterior vertebral
body line: importance
in the detection of burst fractures.AJR1987; 148:9396
13. Gehweiler JA Jr, Osborne RL Jr, Becker RF. The radiology of
vertebral trauma .
Philadelphia, PA: Saunders, 1980
14. Holdsworth FW. Fractures, dislocations, and fracture
dislocations of the spine.
J Bone Joint Surg Am1970; 52:15341551
15. Hendrix RW, Melany M, Miller F, et al. Fracture of the spine
in patients with
ankylosis due to diffuse skeletal hyperostosis: clinical and
imaging findings. AJR1994; 162:899904
16. White AA III, Panjabi MM. Clinical biomechanics of the
spine,2nd ed.Philadelphia, PA: Lippincott, 1990
17. Fielding JW, Hawkins RJ. Atlanto-axial rotary fixation:
fixed rotatory subluxation
of the atlanto-axial joint.J Bone Joint Surg Am1977; 59:3744
18. Gehweiler JA Jr, Daffner RH, Osborne RL Jr. Relative signs
of stable and unstable
thoracolumbar vertebral trauma. Skeletal Radiol1981;
7:179183
19. Daffner RH, Deeb ZL, Goldberg AL, et al. The radiologic
assessment of post-
traumatic vertebral stability. Skeletal Radiol1990; 19:10310820.
Denis F. The three-column spine and its significance in the
classification of
acute thoracolumbar spinal injuries. Spine1983; 8:817831
21. Daffner RH, Brown RR, Goldberg AL. A new classification for
cervical vertebral
injuries: influence of CT. Skeletal Radiol2000; 29:125132
APPENDIX 1: Fingerprints of Flexion Injuries
1. Compression, fragmentation, burst of vertebral bodies2.
Teardrop fragments3. Anterolisthesis4. Disrupted posterior
vertebral body line5. Wide interlaminar (interspinous) space6.
Locked facets7. Narrow disk space above involved vertebra
APPENDIX 2: Fingerprints of Extension Injuries
1. Wide disk space below involved vertebra2. Triangular avulsion
fracture anteriorly3. Retrolisthesis4. Neural arch or pillar
fracture5. Anterolisthesis with normal interlaminar space and
spinolaminar line
APPENDIX 3: Fingerprints of Shearing Injuries
1. Windswept appearance2. Lateral distraction3. Lateral
dislocation4. Transverse process or rib fracture5. Linear oblique
(windswept) array of fragments on CT
APPENDIX 4: Fingerprints of Rotary Injuries
1. Rotation2. Dislocation3. Disrupted posterior vertebral body
line4. Facet or pillar fracture or dislocation5. Transverse process
or rib fracture
6. Spinous process fracture7. Rotary array of fragments on
CT
-
8/11/2019 Injury Patterns in Vertebral Trauma
10/10
54 2008 ARRS Categorical Course
Daffner
APPENDIX 5: Major Injuries
1. Hyperflexion a. Hyperflexion sprain b. Hyperflexion
dislocation (1) Without facet lock (2) With unilateral or bilateral
facet lock
c. Comminuted (teardrop) body fracture d. Burst fracture e.
Chance-type fracture f. Hyperflexion fracturedislocation g.
Occipitoatlantal dislocation or subluxation h. Atlantoaxial
dislocation i. Anterior fracturedislocation of dens j. Lateral
fracturedislocation of dens
2. Hyperextension a. Hangmans fracture b. Hyperextension sprain
c. Hyperextension dislocation d. Posterior atlantoaxial
dislocation
3. Shearing injury a. Thoracolumbar shear injury
4. Rotary injury a. Rotary atlantoaxial dislocation (fixation)
b. Rotary atlantoaxial subluxation c. Rotary (grinding)
thoracolumbar injury
5. Cervical axial compression a. Bursting Jeffersons fracture b.
Vertical and oblique fractures of axis body c. Occipital condyle
type 3 fracture
APPENDIX 6: Minor Injuries
1. Hyperflexion a. Spinous process fracture b. Wedge-like
compression of body (simple fracture) c. Transverse process
fracture (isolated) d. Uncinate process fracture (isolated)
e. Articular pillar fracture (isolated) f. Laminar fracture g.
Lateral wedge fracture of body
2. Hyperextension a. Horizontal fracture of anterior arch of
atlas b. Anterior inferior margin of C2 (teardrop) c. Spinous
process fracture d. Posterior arch of atlas fracture (isolated)
3. Shearing injury None
4. Rotary injury None
5. Axial compression
a. Lateral mass of atlas (isolated) b. Occipital condyle types 1
and 2 fractures