Embed Size (px)
Citation preview

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 1/20
Uncontrolled Diabetic coming for
Emergency Laprotomy
Introduction
Diabetes refers to excessive production and excretion of urine.
Mellitus literally means honey and refers to abnormally elevated concentrations of glucose in blood
and urine
Table 344-2 Criteria for the Diagnosis of Diabetes Mellitus
Symptoms of diabetes plus random blood glucose concentration 11.1 mmol/L (200mg/dL)
aor
Fasting plasma glucose 7.0 mmol/L (126 mg/dL) bor
A1C > 6.5%cor
Two-hour plasma glucose 11.1 mmol/L (200 mg/dL) during an oral glucose tolerancetest
d
Uncontrolled / poorly controlled diabetic may usually present with complications
Asian Indians are more prone to diabetes as well as it’s complications
Certain complications like coronary artery disease and Nepropathy are more common
in Indians
Diabetics can present in any scenario
The Annual rate of Diabetic Acidosis was 46 per 10000 individuals with Diabetes. Of
these 87% were on insulin prior to admission and 81% were not Obese.
The youngest children were at greatest risk.
The prevalence of diabetic complications are given below

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 2/20

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 3/20
it as been clearly shown that better glycemic control in diabetics undergoing surgery improves out come
uncontrolled diabetic should not be taken up for elective surgery before correction of complications
CASE STUDY
A male patient aged 17 years came with
Fever with chills & rigors since 3days
SOB since 2days,
Vomitings since morning,3times,
Severe Thirst
Diabetic diagnosed 2 years back & on irregular Insulin treatment.
This case is also presented with severe abdominal pain in the epigastric area .and posted for
emergency laprotomy
O/E : Dehydrated
PR : 152 / mt
BP : 120 / 80 mm of Hg
RR : 38 / min , Tachypnoeic
SpO2 : 91% on Room air
CVS : S1 S2 +
RS : BAE+
Investigations
Hb : 17.4 gm%
TLC : 24.9 cells/ c.mm
Platelets : 4.05 lacs/c.mm
BUN : 29.4 mg/dl
S.creatinine : 0.7 mg/dl

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 4/20
ABG
PaO2 104.5 mm Hg
PaCO2 25.4 mm Hg
pH 7.418
Hco3 (actual) 16.0 mmol/L
Hco3 (std.) 19.1
BE -13.8 mmol/L
BE ecf -15.9 mmol/L
AG 28.1 mmol/l
S.electrolytes :
Na : 139 meq/l K : 2.6meq/l,
Cl : 114 meq/l , Ca : 8.3 meq/l, Mg 1.9 meq/l
BGL : high,
urine ketone bodies : + ve
Management
Correction of Complications
Correction of Dehydration
Correction of Acidosis & electrolytes
Correction of Hyperglycemia
Control of INFECTION
DKA
Common In type 1 DM
Symptoms :
1. Dyspnoea,
2. Abdominal pain,
3. Nausea and vomiting,
4. Dehydration,
5. Coma

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 5/20
Anion-gap metabolic acidosis, elevated plasma and urine ketones (acetoacetate,
beta-hyroxybutyrate), hyperglycemia
DKA –Treatment
1. Fluid resuscitation-NS@ 1L/hr for two hrs. Then 500ml/hr for 4hrs, then 250ml/hr for 4hrs .Add
D5W when plasma glucose 250 mg%
2. Insulin (regular)- 10u IV bolus is optional . 0.1 U/kg/hour infusion and increase or decrease
based on Bl.Sugar level
3. Potassium -when urine output is there
<3 meq - 40meq/hr,
3-4 meq - 30meq/hr,
4-5 meq - 20meq/hr
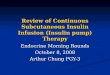
Insulin Infusion Rate (U / DL)Patient BloodGlucose Level(MG/DL)
Algorithm - 1 Algorithm – 2 Algorithm – 3 Algorithm - 4
< 60 = Hypoglycemia (see below for treatment)
< 70 0 0 0 070 – 109 0.2 0.5 1 1.5110 – 119 0.5 1 2 3120 – 149 1 1.5 3 5150 – 179 1.5 2 4 7
180 – 209 2 3 5 9210 – 239 2 4 6 12
240 – 269 3 5 8 16270 – 299 3 6 10 20300 – 329 4 7 12 24
330 – 359 4 8 14 28> 360 6 12 16 28

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 6/20
Hyperosmolar nonketotic coma
Hyperglycemic diuresis -> severe dehydration
Renal failure
Lactic acidosis
Risk of intravascular thromboses
Hyperosmolality with coma ± seizures
Treatment
Fluid resuscitation
Insulin (relatively small doses)
Potassium when urine output.
Hypoglycemia
Diaphoresis, tachycardia, nervousnessPlasma glucose < 50 mg%
Treatment: 50ml of 50% dextrose
If surgery is urgent GIK (glucose- insulin – potassium ) drip is useful to achieve rapid controlled
Anaesthesiologist encounter diabetics for
Incidental surgery
Surgery related to the disease.
Pregnancy
I.C.U

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 7/20
Anaesthetic Implications
Coronary artery disease
Peripheral vascular disease
Cerebrovascular disease
Renal disease
Respiratory and air way changes
Autonomic neuropathy
Cardiovascular system
Increased risk of CAD and MI
Silent myocardial ischemia and infarction
cardiomyopathy in the face of angiographically normal coronary arteries,.

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 8/20
Respiratory and air way changes
Significant decrease in lung volumes and diffusing capacity
Decrease in vital capacity.
Stiff joint syndrome.
Acute unexplained hypoxia in post op period.
Post op respiratory arrest.
Stiff Joint Syndrome
One of four adolescent diabetics
Stiff joints due to nonenzymatic glycosylation of the collagen tissues.
Decreased mobility of the atlanto-occipital joint.
Prayer sign
Palm print sign

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 9/20
Renal System
Diabetic nephropathy -up to 40 –
50% of IDDM
Albuminuria usually precedes a steady decline in renal function
Fluid and electrolyte imbalance
Delayed metabolism and altered excretion of anesthetic drugs
Autonomic Neuropathy
Up to 40% in type I & 17% in type II
Postural hypotension
Profound Intraoperative hypotension with SA requiring vasopressor support
Perioperative cardiorespiratory arrest
Exaggerated pressor response to tracheal intubation
Delayed gastric emptying with increased risk of aspiration
Signs of Autonomic Neuropathy
Lack of sweating
Early satiety
Orthostatic hypotension
Gastric reflux
Lack of heart rate variability with deep inspiration.
Impotence and urinary symptoms of Dysautonomic bladder may be evident.
Dependent oedema
Gustatory sweating

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 10/20
TESTS FOR ANS
• Measuring the beat-to-beat variation in heart rate during breathing,
• Heart rate response to a Valsalva maneuver,
• Orthostatic changes in blood pressure and heart rate.
• B.P response to sustained hand grip
• Changes in the heart rate – Parasympathetic system
• Changes in the blood pressure - Sympathetic system
Preanaesthetic Evaluation
• A thorough search for end-organ complications of Diabetes
• A thorough history and physical Examination
• Severity and type of diabetic state
• Medication for diabetes and control of blood sugar.
• Associated co morbidities
• Air way assessment
Investigations
• Blood Glucose,
• Blood urea ,
• Serum creatinine,
• serum electrolytes (esp-Potassium),
• Recent ECG and CXR
• Urine analysis for sugar and ketones
• Glycosylated Hb (HbA1C) to assess glycemic control

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 11/20
Type of Anaesthesia (Regional Vs General)
Regional anesthesia
Advantages
1. Alleviates stress response to surgery.
2. Decrease in incidence of thrombo embolism
3. Avoidance of aspiration and difficult air way problems.
4. Avoidance of poly pharmacy and their effects on diabetic status
Disadvantages
1. Cardiovascular instability
2. Exacerbation of peripheral neuropathy
3. Increased risk of infection
GA Drugs
Halothane, Methoxyflurane, and Thiopental- Nitrous oxide anesthesia, increase blood glucose
level.
Enflurane and spinal anesthesia.- no increase in bl.glucose level.
.Muscle relaxants and premedicant drugs in common use today are of little concern to diabetics
Overall, the metabolic effects of modern anesthetics are minor compared with the stress of
surgery itself

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 12/20
Perioperative management
The important points to consider when preparing a diabetic patient for surgery include the
- Nature and urgency of surgery, - Adequacy of blood glucose control,
- Treatment regimen used, and - Anticipated time of return to normal
diet.
The aim of perioperative glycaemia control is to avoid Hypoglycaemia, excessive
Hyperglycaemia, Ketoacidosis, and Electrolyte disturbances.
A blood glucose range between 6.7 – 10 mmol /L (120-180 mg %), is widely accepted
Monitoring
• Blood pressure,
• Temperature,
• Pulse oximetry,
• Continuous monitoring of E.C.G
•
Capnogram,
• Frequent determinations of both blood and urine glucose should be made.
• Urine out put
I.V.FLUIDS
On the basis of a preoperative osmotic diuresis, the diabetic patient may reach the operating
room with clinically significant dehydration.
In addition to the usual principles of perioperative fluid management, it is important to note the
amount of glucose administered iv to avoid a massive overdose of glucose.
Patients with diabetes should receive approximately 5 g of glucose per hour (i.e., 5 percent
dextrose solution in water infused at 100 mL per hour) during surgery to prevent the
development of hypoglycemia, ketosis, or protein breakdown

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 13/20
I.V.FLUIDS(cont)
It would be wrong to give large amounts of dextrose (contained in the iv solutions) just because
that patient needed vigorous fluid replacement.
N.S (0.9%NaCl) is the ideal crystalloid ,
R.L increases the blood sugar level after conversion .(k+ is given in the form of KCl)
Basing on the blood loss and Hct value fresh blood should be given
Perioperative fluid management depends up on cardiac and renal status of the patient
.
Targets of Glycemic control
Ideal to keep blood sugar between 120 – 180 mg / dL
In tight control , for selected cases between 80 – 120 mg / dL
To prevent hypoglycemia
Monitoring electrolytes especially potassium
Hemodynamic stability
Insulin therapy
Soluble insulin by I.V route is preferable
Insulin can be given either by
1. fixed rate with glucose infusion
2. separate and adjustable infusion
In well controlled diabetics, Isophane insulin can also be continued.

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 14/20
Diabetic Pts who are not treated with insulin
Minor Surgery + Good Glycemic Control
Replace any long acting sulfonyl ureas
Admit on the day before surgery
On the day of surgery
Operate in the morning if possible
Omit breakfast and oral agents
Avoid glucose containing infusions
Monitor blood glucose 2 nd hrly
Post Operatively
Monitor blood glucose frequently
Restart oral agents with first post op meal
Diabetic Pts who are not treated with insulin
Major Surgery + Poor Glycemic Control
Admit 2-3days before surgery
Stabilize with short acting insulin
On the day of surgery
Operate in morning if possible
Omit break fast and insulin inj
Start iv insulin &glucose( or separate line)
Monitor blood glucose 2ndhrly
Post Operatively
Monitor blood glucose frequently

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 15/20
Transfer to sc insulin if unstable control
Restart oral agents when stabilized
Diabetic patients who are treated with Insulin
Admit 2-3days before surgery
Stabilize control if necessary
On the day of surgery
Operate in morning if possible
Omit break fast and insulin inj
Start iv Insulin & Glucose (GKI or separate lines)
Monitor blood glucose hrly
Post Operatively
Monitor blood glucose frequently
Restart sc insulin with 1st
post op meal
Discontinue iv insulin 2-3 hrs later
GIK
500ML 10%GLUCOSE
10U SOL INSULIN
10MEQ OF POTASSIUM
NON TIGHT CONTROL OF BL.SUGAR
No insulin ,No glucose
Simple & still being followed by many
FBS on the morning of surgery.
Disadv- pre op glucose may be normal but intra oplevel may be high
Suitable only for brief procedure eg-dilatation, curettage & cystoscopy.
Food intake is delayed only by an hour or two

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 16/20
Routine management is restarted at the earliest
NON TIGHT CONTROL OF BL.SUGAR
Partial morning dose of insulin
FBS on the morning of surgery.
Partial morning dose of insulin SC and Dextrose infusion
Dis adv- SC route is not predictable : does not provide good glycemic control.
Not a very popular regimen
TIGHT CONTROL OF BL.SUGAR
To keep glucose between 80-120mg/dl
REGIMEN-1
Preprandial sugar levels on the evening before surgery.
Start infusion , piggyback regular insulin 50u in 250ml 0.9nacl
Flush this line at least 60ml of this sol to prevent adsorption of insulin.
Infusion rate = plasma glucose/150 (100-pt on steroids).
Repeat measurements of glucose 4th
hrly and adjust insulin to achieve plasma glucose of 100-
200 mg/dl
TIGHT CONTROL OF BL.SUGAR
On the day of surgery-use non dextrose containing fluids for intra operative use
Determine plasma glucose 2nd
hrly and infuse insulin accordingly
Frequent change of sol pose an attendant risk of hyponatremia.
If the glucose level are < 90 mg/dl discontinue insulin and estimate the blood glucose level every30 min till glucose is >110mg/dl.
Serum k+ should be checked and adjusted accordingly with particular care for poor renal
function.

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 17/20
TIGHT CONTROL OF BL.SUGAR
TO KEEP GLUCOSE BETWEEN 80-120mg/dl
REGIMEN-2
Fixed rate glucose infusion
Separate and adjustable infusion of insulin to maintain normoglycemia
Insulin requirements vary between 0.5 to 5u/hrly in post op period
Advantages :it is easy to follow ,but requires good communication skills between nurse and
doctor
Sliding scale insulin infusion
GGLLUUCCOOSSEE CCOONNCC IInnssuulliinn uu//hhr r iinnf f uussiioonn r r aattee
<<7700 --
7711--112255 11
112266--116600 11..55
116611--220000 22
220011--330000 33
330011--550000 44
>>550000 66

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 18/20
GHT CONTROL OF BL.SUGAR
The Artificial Pancreas
Close loop controlled:
The glucose and insulin are infusion is determined by an online plasma analyser
Plasma glucose level maintained between 70 -120mg/dl
Very expensive ,require complex supervision and used at present in reseach environment.
Alberti-Thomas regimen
Before operation – stabilize 2-3 days prior to surgery with short-acting insulin (Actrapid).
During operation - Give NO subcutaneous insulin on day of surgery.
Set up an infusion of 10% glucose (500ml) containing Actrapid 10 units plus KCl 1g.
Give it at the rate of 100-125ml/hr.
Check blood glucose and plasma potassium before infusion and after 2-3 hours. Adjust the
amount of insulin as follows:
Blood glucose (mmol L-1) Infusion
< 5 < 90 mg 10% glucose 500ml + insulin 5 units + KCl 1g
5 – 10 90-180 mg 10% glucose 500ml + insulin 10 units + KCl 1g
> 10 >180 mg 10% glucose 500ml + insulin 15 units + KCl 1g
> 20 >360 mg 10% glucose 500ml + insulin 20 units + KCl 1g
Adjust potassium doses according to plasma potassium level.
Disadvantage: Cumbersome and requiring periodacal alternationa
Christian Medical College & Hospital regimen
A burette set is connected to a 5% glucose (500ml) bag, and 100 ml of glucose is filled into the
burette at a time. Short-acting insulin (Actrapid) is added to the 100 ml of fluid in the buretteaccording to the scale given below and this is infused over 1 h.
Blood glucose is measured at the end of the hour which determines the amount of insulin to be
added to the next 100ml of 5% glucose.

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 19/20
Blood glucose mg/dl (mmol L-1) Infusion
<75 (4.1) No insulin; 100ml 5% glucose over 15 min
75-100 (4.1-5.5) No insulin; 100ml 5% glucose over 1h
100-150 (5.5-8.3) 1U Actrapid in 100ml 5% glucose over 1h
150-200 (8.3-11.1) 2U Actrapid in 100ml 5% glucose over 1h
200-250 (11.1-13.8) 3U Actrapid in 100ml 5% glucose over 1h
250-300 (13.8-16.6) 4U Actrapid in 100ml 5% glucose over 1h
>300 (16.6) 4U Actrapid in 100ml normal saline over 1h
POSITIONING
Positioning of the pt is very important.
Injuries to the limbs or nerves are more likely as they are already compromised by diabetic
peripheral vascular disease or neuropathy.
The peripheral nerves may already be partly ischemic and therefore particularly vulnerable to
pressure or stretch injuries.
INTRAOPERATIVE HYPOGLYCEMIC SHOCK
It is virtually impossible to differentiate hypoglycemic shock from other forms of shock
intraoperatively unless supported by low blood glucose concentrations measured
concomitantly.
Treatment lies in administration of glucose, which can be given as a bolus of 50% glucose
followed by a 10% glucose-insulin infusion.

8/12/2019 Insulin Infusion Rate
http://slidepdf.com/reader/full/insulin-infusion-rate 20/20
Blood sugar increases approximately 30 mg/dl for each 7.5-g bolus of dextrose in a 70-kg adult.
POSTOPERATIVE COMPLICATIONS
In addition to the usual complications, the common problems in a diabetic include poor diabetes
control and infection.
A higher incidence of cardiovascular and renal problems and autonomic neuropathy, resulting
in postural hypotension and urinary retention, may be encountered.
Overall morbidity and mortality are increased