Embed Size (px)
Citation preview

Micro-CT Imaging of an Insulin Bolus Infusion Through Continuous Subcutaneous Insulin Infusion (CSII) Sets in Live Swine: Quantitative Comparison of Distribution Patterns in Tissue Over Eight Days.
David Diaz Ph.D.1, Aleksandr Dinesen M.S.1, Abdurizzagh Khalf 1, Gabriella Eisler1, Channy Loeum1, Mathew Thakur Ph.D.1, Marc C Torjman Ph.D.1,Kenneth C Hsu2, Paul J Strasma2, Jeffrey I Joseph D.O.1
1 Jefferson Artificial Pancreas Center, Department of Anesthesiology, Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA; 2Capillary Biomedical, Inc., Irvine, CA
INTRODUCTION
DISCUSSION
RESULTS
METHODS
• Over 1 million people with diabetes use insulin pumps and insert a new continuous subcutaneous insulin infusion (CSII) set every 2–3 days for adequate blood glucose control.
• Insulin absorption from the subcutaneous tissue is slow and varies over time leading to complications such as hyperglycemia, hypogly-cemia and glycemic variability.
• Repeated trauma of insertion contributes to scar tissue formation and may result in infusion site loss.
• Cannula kinking, cannula blockage, and leakage to the skin surface are reported as common infusion set problems.
•Previousstudiesfromthisgroupidentifiedalayerofinflammatorytissue surrounding implanted CSII cannulas which becomes thicker, denser, and more continuous as duration of implant increases. This layer may function as a mechanical barrier, slowing or inhibiting the movement of insulin into adjacent subcutaneous tissue containing capillary and lymph vessels.
• A prototype kink-resistant infusion set cannula was developed using a soft polymer material with multiple ports and compared against commercially available single-port infusion sets in ambulatory large swine.
• Using micro-computer-tomography (micro-CT) we tested the hypothesisthatmultiple-portswouldincreasefluiddispersionfroma CSII cannula, potentially allowing the insulin to reach more functional capillary and lymph vessels.
• Compared with the commercial CSII set, the investigational CSII set withasoft-flexiblepolymercannula,wire-reinforcedwalland multipleportsproducedsignificantlygreatervolumeandsurfacearea of insulin distribution into adjacent vascular tissue.
Research sponsored by Capillary Biomedical, Inc. and supported by JDRF award 2-IND-2016-232-M-X
• Investigational multi-port cannulas demonstrated a larger surface area (p=0.018) and 3D volume (p=0.021) of contrast agent spread into the subcutaneous tissue compared to PTFE cannulas withasingledistalorifice(seeFigure1).
• No differences were observed in leak events (p=0.416) between commercial and investigational sets when evaluating cannulas indwelling for 2 to 8 days (see Figure 2).
•Investigationalcannulashadasignificantlylowerkinkingrate(p=0.035) than commercial PTFE cannulas (0% vs 18% respectively).
• None of the investigational CSII sets with the coil-reinforced polymercannulasandmultipleportsexhibitedakink.
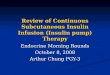
•The70µLbolusofinsulinandx-raycontrastagenttraveledfrom the commercial PTFE cannula’s single distal port and the investigational cannula’s multiple ports into adjacent connective tissue septa along the path of least resistance (see Figure 3).
•Theinsulin/contrastbolusdistendedtheconnectivetissuefibersto form a spherical distribution in commercial infusion sets and a cylindricalorconedistributionwithafew“finger-like”projectionsfor investigational catheters.
• Many of the bolus infusions for PTFE cannulas were associated with high peak tubing pressures (2,000 to 5,000 mm Hg) that remained elevated after completion of the bolus, despite having no evidence of infusion set failure.
•CommercialCSIIinfusionsetswitha6mmpolytetrafluoroethylene(PTFE) cannula (Inset, Unomedical) and investigational sets with a 14 mm coil-reinforced polymer (CRP) cannula and 4 ports (one distaland3proximalportsset2mmapartinahelicalpattern)were inserted in the soft abdominal tissue of ambulatory swine (n=8,47setsintotal).Infusionsetswereexplantedat10minutes,2 days, 4 days, 6 days, and 8 days post-implantation.
• Insulin lispro (U-5) was continuously infused through each CSII sets (7 µL/hour) using an insulin pump with an additional 70 µL bolus one or two times per day with meals.
•Onthefinalstudydate,a70µLbolusofinsulinlispro(U-100)andx-raycontrastagent(Isovue300Iopmidol)wasinfusedthrougheach CSII set.
0 Days 2 Days 6 Days4 DaysCapillary Biomedical Coil-Reinforced Soft Polymer Cannula Design
Commercially Available CSII Set with PTFE Cannula
8 Days
• PK/PD studies in swine and humans are currently underway to determine whether this greater volume and surface area of distribution is able to reach more functional capillary and lymph vessels leading to faster onset/offset and more consistent insulin absorption from dose-to dose.
•Thesoft,flexiblepolymerwire-reinforcedcannulaeliminated kinking, a common early failure mode of commercial CSII sets with a PTFE cannula.
•Insulin/x-raycontrastagentleakedontotheskinsurface,alongthepathofleastresistanceinapproximately10-25%ofthebolusinfusions.
•Insulin/x-raycontrastspreadsefficientlyintoadjacentsubcutaneoustissue immediately after CSII cannula insertion (0 days). Distribution into adjacent vascular tissue on days 2-8 may be slowed and inhibited bythesurroundinglayerofinflammatorytissue.
Figure 3.Representativelongitudinalsequenceofthree-dimensionalmicro-CTimagesillustratingtheextentofinsulin/contrastdispersionintothesubcutaneoustissuesurroundinginvestigationalCSIIsetswithacoil-reinforcedpolymercannula(top)andPTFEcannulaswithasingleorifice(bottom)indwellingfor10minutes,2 days, 4 days, 6 days, and 8 days (left to right).
Figure 1. Evaluation of 3D surface area and volume dispersion measurements froma70µLbolusofinsulin/x-raycontrastagentmixtureinfusedthroughcommercialCSIIsetswithaPTFEcannulaandasingledistalorificeversusinvestigationalCSIIsetswithacoil-reinforcedsoftflexiblepolymer(CRP)andfourportsalongthecannulashaft.Significantlyhigher3Dsurfaceareasandvolumes were achieved with the CRP cannulas.
Figure 2. Evaluation of infusion set leaks and cannula kinks from micro-CT analysis.Thenumberofinfusionsetswithkinkswassignificantlylower(p=0.035) for the investigational CSII sets with a coil-reinforced polymer cannula compared to the commercial CSII sets with a PTFE cannula. The number of sets with leaks onto the skin surface was lower for investigational sets,althoughnotstatisticallysignificantly(p=0.416).
• Pressure was recorded during the bolus using an inline transducer (PendoTECH).
•Tissuewasexcised5minutesafterbolusinfusionandfrozenformicro-CT imaging.
• Specimens were imaged using an Inveon micro-PET/CT imaging scanner (20 µm resolution) to determine the distribution pattern ofinsulin/x-raycontrastagent.
•AMIRA3Dvisualizationsoftware(FEICompany)wasusedtomeasure the surface area and volume of spread of insulin/contrast agent bolus into subcutaneous tissue.
• Failure mode analysis was performed to evaluate the performance of each infusion set group related to cannula kinks and skin surface leakages using the micro-CT images.
•Micro-CTimagingdatawereanalyzedusingANOVAand categoricaldatausingtheFisherExactTestperformedwiththeSystat software (ver. 13).
0
50
100
150
200
250
300
350
Mea
n ±
SEM
CRP
PTFE
* p=0.018 vs PTFE+ p=0.021 vs PTFE
*
+
Surface area (mm2) Volume (mm3)
0
10
20
30
40
50
60
70
80
90
100
No Leak Leak
sisylanA TC orci
M rep skaeLC
annu
la(%
of C
annu
las)
CRP
PTFE
p=0.416 (CRP vs PTFE)
0
20
40
60
80
100
No Kink Kinked
sisylanA TC orci
M rep skniKC
annu
la(%
of C
annu
las)
CRP
PTFE
*p=0.035
*
• Micro-CT images of infusions with high internal pressures often revealedlessthan70µLofinsulin/x-raycontrastagentdeliveredintothe subcutaneous tissue, despite having no insulin pump occlusion alarm. In clinical practice, a diabetic patient may believe a full bolus ofinsulinwasdelivered,whenasignificantlylowervolumeofinsulinwould have actually been delivered into the subcutaneous tissue.
• This variability of actual insulin delivery into the subcutaneous tissue may be a major cause of variable insulin PK/PD in patients managing their diabetes in the real-world. Results from this research have guidedthedesignanddevelopmentofanext-generationinsulin infusion set.
• Clinical translation of this investigational CSII set could result in a morereliableinsulindeliverysystemthatsignificantlyimprovesbloodglucosecontrol,simplifies/reducestheburdenofdiabetesmanagement, improves the quality of life of people with diabetes andbenefitsclinicaloutcomes.