Embed Size (px)
Citation preview

Insurance authorIzatIon - sIgnature on FIle
I hereby authorize my health care provider to affix my name to all insurance submissions,
documents, and/or information requested by my insurance company(s) related to any and all
health benefits due to me and my dependents.
I also authorize payment of healthcare benefits otherwise payable to me, directly to my
doctor as listed above. I agree to be held responsible for all charges and services not paid by
my insurance company.
The Signature on File (SOF) is valid from this date and expires in thirty-six months.A photocopy of this authorization may act as an original.
Today’s Date Signature of Patient or Insured

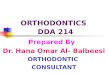
ADA Dental Claim Form HEADER INFORMATION
1. Type of Transaction (Mark all applicable boxes)
Statement of Actual Services Request for Predetermination/Preauthorization
0 EPSDT/Title XIX
2. Predetermination/Preauthorization Number POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3)
12. Policyholder/Subscriber Name, (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION O'Connor, Kevin
3. Company/Plan Name, Address, City, State, Zip Code 43 W. Cherbourg
CSEA EMPLOYEE BENEFIT FUND Cheektowaga, NY 14227
PO BOX 489 LATHAM NY 12110-0489
13. Date of Birth (MM/DD/CCYY) 114. Gender 115. Policyholder/Subscriber ID (SSN or ID#)
2/26/1972 [X] M 0 F 055006804
OTHER COVERAGE 16. Plan/Group Number 117. Employer Name
4. Other Dental or Medical Coverage? 00 No(Skip5-11) 0 Yes (Complete 5-11) 999999 Unknown
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) PATIENT INFORMATION
18. Relationship to Policyholder/Subscriber in #12 Above 119. Student Status
6. Date of Birth (MM/DD/CCYY) 7. Gender 18. Policyholder/Subscriber ID (SSN or ID#) Osei! 0 Spouse [X] Dependent Child nother lxl FTS 0 PTS
oM nF 20. Name, (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code
9. Plan/Group Number 10. Patient's Relationship to Person Named in #5 O'Connor, Jackson
Osei! n Spouse 0 Dependent lxl Other 1896 Como Park Blvd Lancaster, NY 14086
11 Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code
21. Date of Birth (MM/DD/CCYY) 122. Gender 123. Patient ID/Account# (Assigned by Dentist)
7/26/2002 OO M n F 904100
RECORD OF SERVICES PROVIDED
24. Procedure Date 25. Area 26 27. Tooth Number(s) 28. Tooth 29. Procedure (MM/DD/CCYY) of Oral Tooth or Letter(s) Surface Code 30. Description 31. Fee
Cavity System
1 D9310 Orthodontic Consultation
2 D0330 Panographic X-ray 95.00
3 D0340 Cephalometric X-ray 95.00
4 D0470 Study Models 105.00
5 D0350 Photographs 95.00
6 D8080 Comprehensive Orthodontic Treatment 1275.00
7 D8670 Active Orthodontict Tx $175 x 24 months 4200.00
8 D8999 Passive orthodontic Treatment 175.00
9
10
MISSING TEETH INFORMATION Permanent Primary 32. Other
1 2 3 4 5 6 7 8 I 9 10 11 12 13 14 15 16 A B c D I F G H I J Fee(s)
34. (Place an 'X' on each missing tooth) 25 I 24 P lo 16040.00 32 31 30 29 28 27 26 23 22 21 20 19 18 17 T s R Q N M L K 33. Total Fee
35. Remarks
active ortho treatment 20/24 months Class II Div I malocclusion
AUTHORIZATIONS ANCILLARY CLAIM/TREATMENT INFORMATION 36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all 38. Place of Treatment
139. R~~(s~ ~~~~f 9Fl charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or [XJ Provider's Office 0 Hospital 0 0 the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a
portion of such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health information to carry out payment activities in connection with this claim 40. Is Treatment for Orthodontics? 41. Date Appliance Placed (MM/DD/CCYY)
x Signature On File 2/5/2014 0 No (Skip 41-42) [XJ Yes (Complete 41-42)
- ·- siqnature Date 42.Months of Treatment 143. Replacement of Prosthesis? 44. Date Prior Placement (MM/DD/CCYY)
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the Remaining [X] No 0 Yes (Complete 44)
below named dentist or dental entity 45. Treatment Resulting from
x Signature On File 2/5/2014 0 Occupational illness/injury 0 Auto accident 0 Other accident
Subscriber signature Date 46. Date of Accident (MM/DD/CCYY) I 47. Auto Accident State
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting TREATMENT DENTIST AND TREATMENT LOCATION INFORMATION claim on behalf of the patient or insured/subscriber) 53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require
48. Name, Address, City, State, Zip Code multiple visits) or have been completed
Amy Richter D.M.D. M.S. PC x Amy Richter 2/5/2014
8650 Sheridan Drive Williamsville, NY 14221
Signed (Treating Dentist) Date
54. NPI 1619319464 I 55. License Number 053875
56. Address, City, State, Zip Code I 56A Provider 1223X0400X Specialty Code
49. NPI 150. License Number 151. SSN or TIN 8650 Sheridan Drive 1619319464 053875 272192328 Williamsville, NY 14221
52 ~~~~er 716 631-9924 I 52A Additional 57 Phone 158. Additional Provider ID Number Provider ID
© 2006 American Dental Assoc1at1on J400 (Same as ADA Dental Claim Form - J401, J402, J403, J404)