Embed Size (px)
Citation preview

Insurance Underwritten ByFreedom Life Insurance Company of America
PPT-Sales-PC-PM-ANC-TX-0317

A Little About Us: USHEALTH Advisors, LLC
Excellent Reputation
10 Stevie Awards in 4 Years
A+ BBB Rating
Freedom Life Insurance Company of America& National Foundation Life Insurance Company Over 50 Years of Collective Industry Experience
Rated A+ by BBB*
Rated B Positive by AM Best 2014 Report
Over 15 Million Customers Served**
Over 1 Billion dollars in Paid Claims**
Average claim processed in 10 calendar days***
USHEALTH Group, Inc.
*http://www.bbb.org/fort-worth/business-reviews/insurance-services/ushealth-group-inc-in-fort-worth-tx-205821197**Customer Service and Claims information by insurance subsidiaries of USHEALTH Group***2013 Analysis of Claims Processing Time and by insurance subsidiaries of USHEALTH Group

Have You Reviewed All Your Options?
1. Group Insurance
2. ACA Plan on the Exchange (a.k.a. Market Place)
3. ACA Plan off the Exchange (Carrier Direct)
4. NO Insurance – Pay the Shared Responsibility Tax
5. PremierChoice Specified Disease/Sickness and Accident with riders combined with the Shared Responsibility Tax
1. Unaffordable Premiums
2. Large Upfront Deductibles
3. Limited Provider Access (Restricted Networks with Providers that take your insurance)
4. Poor Customer Service
4 Problems Consumers May Have With Health Insurance:
USHA has received 10 Awards in 4 Years from the American Business Awards for Product Innovation and Top Quality Customer Service.

Except for Emergencies
https://www.healthcare.gov/choose-a-plan/plantypes/USHA-IG-RPN-0116

AIBC Membership
• Professional Life– Finance Talk
– Tax Talk
• Personal Life– LifeLock
– Roadside Assistance
• Health & Well-Being– Blanket Accident Excess Medical Expense &
Accidental Death and Dismemberment (AD&D) Coverage
– Blanket Group Specified Disease/Illness & Accident Insurance

Blanket Insurance Coverage BenefitsCoverage commences for Members immediately following the receipt, by the association, of the Membership enrollment application and the payment by the Member of the first month’s dues and continues as long as dues are paid, subject to the company’s right to adjust future premiums and cancel coverage. Coverage is underwritten and administered by National Foundation Life Insurance Company in AL, AR, AZ, CO, DE, GA, IA, IN, KY, LA, MO, MS, MT, NC, NE, OH, OK, PA, SC, TN, TX, UT and WY. (Freedom Life Insurance Company of America in IL, MI, VA and WV). This coverage is not available to members who are residents of any otherstates. Coverage is subject to the definitions, terms, limitations and exclusions contracted in the blanket policy.
LOSS - Percentage of Maximum BenefitLoss of Life 100%Loss of two or more Limbs 100%Loss of Speech and Loss of Hearing (both ears) 100%Loss of Sight (both eyes) 100%Loss of one Limb 50%Loss of Speech 50%
Loss of Hearing (both ears) 50%Loss of Sight (one eye) 50%Loss of one Hand 50%Loss of one Foot 50%Loss of Hearing (one ear) 25%Loss of Thumb and Index Finger (same hand) 25%
*The Maximum Benefit reduces by fifty percent (50%) at age sixty-five (65).**Eligible Dependent Children of Primary Member means an unmarried dependent child of the Primary Insured who is under the age of nineteen (19) years (twenty-four (24) if enrolled as a Full-Time Student).
Excess Medical Expense and Accidental Death and Dismemberment (AD&D) Coverage

Note: The Excess Medical Expense Coverage Benefit is payable for expenses under this plan in excess of coverage under any other valid insurance coverage, accident medical expense benefits or health benefit plan coverage, including but not limited to coverage or benefit entitlement under or pursuant to an uninsured/under insured motorist coverage, personal injury protection coverage under any automobile policy, comprehensive major medical insurance, hospital/medical surgical insurance, other indemnity health insurance, health coverage under an HMO or PPO plan, workers compensation medical expense benefits, FELA medical expense benefits, Jones Act medical expense benefits, Medicaid and Medicare.
Blanket Group Specified Disease/Illness & Accident Insurance
Benefits also include - 50% of expenses incurred for an Inherited Metabolic Disorder, Up To $5,000 and a Membership Year Maximum up to $15 for each of the following: Outpatient Diabetes Equipment, Outpatient Diabetes Self-Management Training, and Outpatient Diabetes Supplies.
The Blanket Group Specified Disease/Illness and Accident Insurance forms BLKACCUP2-2014-P-FLIC/BLKACCUP2-2014-P-NFL; and BLKSDUP2-2014-P-FLIC/BLKSDUP2-2014-P-NFL are underwritten and issued by Freedom Life Insurance Company of America and National Foundation Life Insurance Company and issued to AIBC.
Blanket Insurance Coverage Benefits, cont’dExcess Medical Expense and AD & D Coverage
Coverage commences for Members immediately after application and payment of the first month’s dues.
*The individual mandate under the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or be subject to payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year (See page 51 of this brochure for details). The PremierChoice Specified Disease/Sickness Plans and Accident Plans are insurance plans which provide benefits on an expense incurred basis up to a maximum daily/monthly/annual amount for covered services and are neither “essential health benefits plans” under the ACA, traditional major medical insurance plans, nor Workers Compensation plans under state law. PremierChoice Specified Disease/Sickness Plans and Accident Plans are “excepted benefit plans” under the ACA, but are not considered “minimum essential coverage” under it. Therefore, unless an Insured under one of our PremierChoice Specified Disease/Sickness Plans and/or Accident Plans has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s “shared responsibility payment” (See page 51 of this brochure for details).
**The Premium Rate Guarantee Period does not apply to any rate change due to: change of address; addition of Insureds; change of benefits or options; change of Mode Of Premium Payment; group policy coverage, benefits, limitation or exclusion changes; or any future requirements of any federal or state law.
• No Calendar Year Deductibles to Satisfy! You receive “first dollar” benefit payments under each of the PremierChoice Specified Disease/Sickness and Accident Plans without first having to satisfy any calendar year deductible, which is different from ACA essential health benefit plans and many other plans that require the Insured to first satisfy a calendar year deductible for network providers, and a separate calendar year deductible for non-network providers, before applicable medical expenses are eligible for payment.
• First Dollar coverage, up to the applicable benefit amount, available under both the PremierChoice Specified Disease/Sickness & the Accident Plans for Outpatient Doctor Office Visits! Special “rollover” feature in each plan; if You don’t use Your benefits, You don’t lose them.
• Buy more coverage, if You need it, without additional underwriting! Ask Your Agent about the Optional Single Step-Up Rider, the Optional Double Step-Up Rider and the Optional Medical Inflation Protection & Guaranteed Insurability Rider (MIGI Rider).
• Any Doctor, Any Hospital! But You can stretch Your dollars further by choosing an In-Network Provider.
• Neither the PremierChoice Specified Disease/Sickness Plan with the MIGI Rider nor the PremierChoice Accident Plan with the Optional Medical Inflation Protection Rider are ACA essential health benefits plans. However, while these are in full force and effect, You have the right to purchase additional coverage under Our PremierMed Short Term Medical-Surgical Expense Plan with no additional underwriting, if You are not covered under an ACA plan of “minimal essential coverage”, as a bridge to Your purchase of ACA essential health benefits coverage.*
• Each plan pays in addition to any coverage You have in force.
• Automatically Locks in Your rates for 15 months at no extra charge!**
• 24 hour coverage, on or off the job. Coverage You can depend on when You need it the most.

The PremierChoice Specified Disease/Sickness and Accident Plansallow You to receive first dollar payments for expenses incurred, up to a benefit maximum for covered healthcare services.1
This supplements an essential health benefits plan under which You must first satisfy a deductible every year beforeYou are eligible to receive benefit payments. 1You will be responsible for charges that exceed Your Specified Disease/Sickness Plan and/or Accident Plan benefit amount and the network discount.

You Need to KNOW You are Covered forSpecified Diseases/Sicknesses from Head to Toe!!
• Acute Myocardial Infarction(Acute Heart Attack)
• Adrenal Hypofunction(Addison’s Disease)
• Amyotrophic Lateral Sclerosis(Lou Gehrig’s Disease)
• Arteriosclerosis• Bacterial Infection• Brain and Nervous System
Disease• Cancer• Cardiovascular Disease• Complications of Pregnancy
• Poliomyelitis• Pulmonary Disease• Rheumatoid Arthritis• Reproductive System Disease• Sickle Cell Anemia• Skin Disease• Sleep Apnea• Toxic Epidermal Necrolysis• Toxic Shock Syndrome (TSS)• Viral Infection
PremierChoice Specified Disease/Sickness Plan Covers the Following Diseases and Illnesses1
• CVA (Stroke)• Cystic Fibrosis• Diabetes• Endocrine System Disease• Gastrointestinal Disease• Hypertension• Influenza• Inherited Metabolic Disorder• Kidney and Urinary Tract
Disease• Life Threatening Cancer
• Liver and Biliary Tract Disease• Multiple Sclerosis• Muscular Dystrophy• Musculoskeletal Disease• Obstructive Sleep Apnea• Ophthalmology Disease• Osteoarthritis• Osteomyelitis• Osteoporosis• Otolaryngology Disease
1Subject to Exclusions and Limitations of the plan (see slides 47-51).
The PremierChoice Specified Disease/Sickness Plan provides benefits for covered Specified Diseases/Sicknesses, but unlike a major medical plan, it does not cover accidental bodily injuries or wellness exams. If accident coverage is appropriate for You and/or Your family, please ask Your agent for details on available options.

Non-Fatal Injuries Resulted in Over $111 Billion in Medical Costs.1
When Accidents Happen Count on Your PremierChoice Accident Plan to Cover Your Accidental Bodily Injury Medical Costs.2
Accidental Bodily Injuries such as:
• Fractures
• Cuts & Punctures
• Back Injuries
• Burns
• Sports Injuries
• Head Injuries
• Knee Injuries
• Bone Injuries
• Ligament & Tendon Injuries
Accidental Injuries Covered 24/7 On or Off the Job!
1Centers for Disease Control and Prevention Data and Statistics: Cost of Injury Reports, Unintentional Non-Fatal Injuries, U.S., both sexes, all ages, most recent data available as of October, 2014.2Subject to Exclusions and Limitations of the plan (see slides 47-51). The PremierChoice Accident Plan provides benefits for covered Accidents, but unlike a major medical plan, it does not cover Specified Diseases/Sicknesses or wellness exams. If Specified Disease/Sickness coverage is appropriate for You and/or Your family, please ask Your agent for details on available options.

The individual mandate under the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, orbe subject to payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year(See slide 51 of this presentation for details). The PremierChoice Specified Disease/Sickness Plans and Accident Plans are insurance plans which provide benefitson an expense incurred basis up to a maximum daily/monthly/annual amount for covered services and are neither “essential health benefits plans” under theACA, traditional major medical insurance plans, nor Workers Compensation plans under state law. PremierChoice Specified Disease/Sickness Plans and AccidentPlans are “excepted benefit plans” under the ACA, but are not considered “minimum essential coverage” under it. Therefore, unless an Insured under one ofour PremierChoice Specified Disease/Sickness Plans and/or Accident Plans has an exemption from the ACA’s individual mandate or maintains “minimumessential coverage” under the ACA, the Insured will be subject to the ACA’s “shared responsibility payment” (See slide 51 of this presentation for details).
*Not available on PremierChoice Specified Disease/Sickness Plan 1 and PremierChoice Accident Plan 1
**Not available on PremierChoice Specified Disease/Sickness Plans 1 & 2 and PremierChoice Accident Plans 1 & 2
Specified Disease/Sickness PlanOutpatient Daily/Monthly Benefits• Doctor Office Visit• Prescription Drugs• X-Ray • Labs• Spinal Manipulation Office Visit • Emergency Room• Emergency Air/Ground Ambulance• Specialty Radiology
• CAT Scan• PET Scan• MRI
• Radiation Therapy• Oral Chemotherapy• IV Chemotherapy• Urgent Care Facility• Diabetes Equipment, Supplies & Training• Outpatient Medical Foods• Outpatient Surgeon Benefit*• Surgery Facility*• Kidney Dialysis
Specified Disease/Sickness PlanHospital Confinement Daily Benefits• Hospital Room & Board• ICU Room & Board• Hospital Miscellaneous Expenses• Increased Critical Hospital Miscellaneous
Expenses for Specified Diseases/Sicknesses:
• Coronary Artery By-pass• Coma• Heart Attack• Life Threatening Cancer• Stroke
• Inpatient Surgeon Benefit**
Accident PlanOutpatient Daily/Monthly Benefits• Doctor Office Visit• Prescription Drugs• X-Ray • Labs• Spinal Manipulation Office Visit • Emergency Room• Emergency Air/Ground Ambulance• Specialty Radiology
• CAT Scan• MRI
• Urgent Care Facility• Orthotic & Prosthetic Devices• Outpatient Surgeon Benefit*• Surgery Facility*
Accident PlanHospital Confinement Daily Benefits• Hospital Room & Board• ICU Room & Board• Hospital Miscellaneous Expenses• Increased Critical Hospital Miscellaneous
Expenses for Bodily Injury:• Coma• Severe Burn
• Inpatient Surgeon Benefit**
We will pay expenses incurred for covered services up to the maximum amount listed on a daily/monthly/annual basis (see slides 16-19 for plan options & amounts) for the following covered medical and surgical services. Terms, conditions, limitations and exclusions may apply.

As marked below, the following benefits apply to the Specified Disease/Sickness Plan. As marked below, the following benefits apply separately to the Accident Plan. Benefits for covered Specified Diseases/Sicknesses and Accidents are payable based on expenses incurred, up to the amount shown below. (Example: With Specified Disease/Sickness Plan 1, You get three (3) Doctor Office Visits. With Accident Plan 1, You get three (3) Doctor Office Visits.)
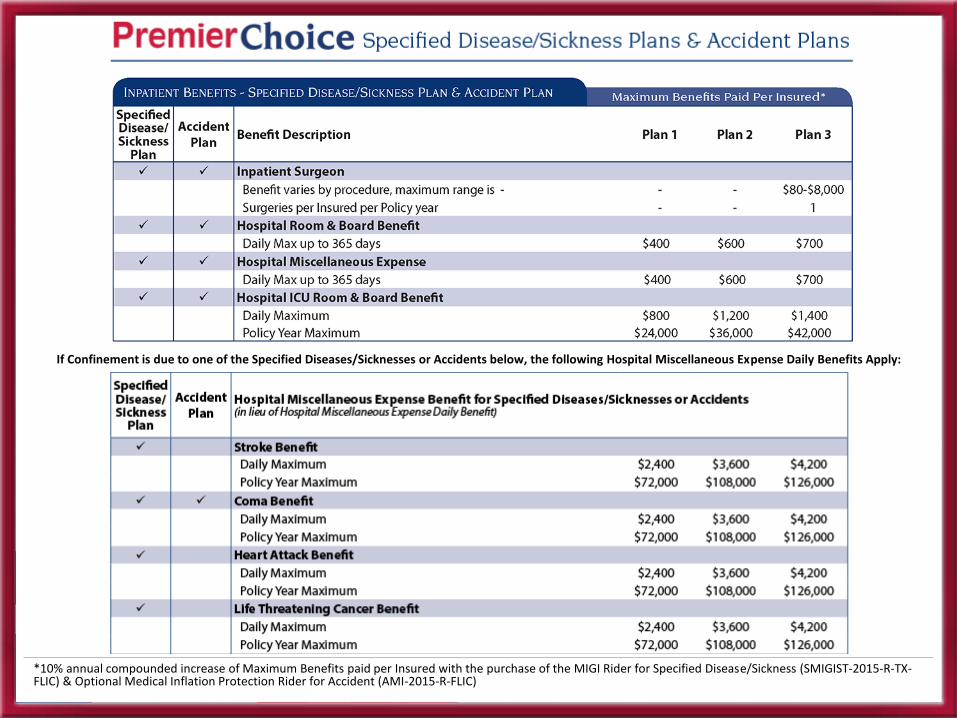
*10% annual compounded increase of Maximum Benefits paid per Insured with the purchase of the MIGI Rider for Specified Disease/Sickness (SMIGIST-2015-R-TX-FLIC) & Optional Medical Inflation Protection Rider for Accident (AMI-2015-R-FLIC)**Only available on the Specified Disease/Sickness Plan.

*10% annual compounded increase of Maximum Benefits paid per Insured with the purchase of the MIGI Rider for Specified Disease/Sickness (SMIGIST-2015-R-TX-FLIC) & Optional Medical Inflation Protection Rider for Accident (AMI-2015-R-FLIC)
Coverage also included under the Specified Disease/Sickness Plan with a Daily/Policy Year Maximum up to $15 for each of the following: Outpatient Diabetes Equipment, Outpatient Diabetes Self-Management Training, and Outpatient Diabetes Supplies.
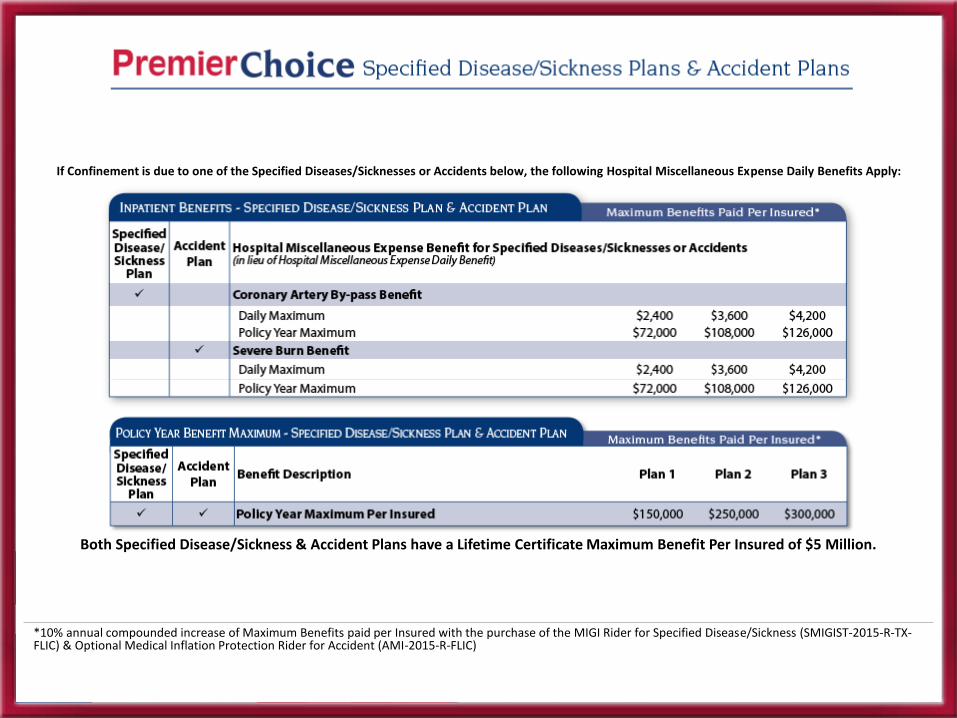
*10% annual compounded increase of Maximum Benefits paid per Insured with the purchase of the MIGI Rider for Specified Disease/Sickness (SMIGIST-2015-R-TX-FLIC) & Optional Medical Inflation Protection Rider for Accident (AMI-2015-R-FLIC)
If Confinement is due to one of the Specified Diseases/Sicknesses or Accidents below, the following Hospital Miscellaneous Expense Daily Benefits Apply:
*10% annual compounded increase of Maximum Benefits paid per Insured with the purchase of the MIGI Rider for Specified Disease/Sickness (SMIGIST-2015-R-TX-FLIC) & Optional Medical Inflation Protection Rider for Accident (AMI-2015-R-FLIC)
If Confinement is due to one of the Specified Diseases/Sicknesses or Accidents below, the following Hospital Miscellaneous Expense Daily Benefits Apply:
Both Specified Disease/Sickness & Accident Plans have a Lifetime Certificate Maximum Benefit Per Insured of $5 Million.

Recap Benefits1. No Deductible, First Dollar Benefits
2. PremierChoice Specified Disease/Sickness & Accident Plans provide access to the PHCS Limited Benefit Plan Network to reduce cost and maximize benefits
3. Rates guaranteed for up to 15 Months**
4. Optional Single Step-Up 1 or Double Step-Up2 Riders
5. Optional MIGI Rider3 for PremierChoice Specified Disease/Sickness Plans & Optional Medical Inflation Protection Rider4 for PremierChoice Accident Plans allows the Insured to purchase additional coverage later without additional underwriting
6. 24 Hour “On the Job” Coverage for Self-Employed
7. Portable in case you change jobs or move states
8. Customize your plan to meet your needs and budget
9. Add additional Supplemental Coverages
1UP2STEPUP1-R-FLIC 2UP2STEPUP2-R-FLIC3SMIGIST-2015-R-TX-FLIC4AMI-2015-R-FLIC
**The Premium Rate Guarantee Period does not apply to any rate change due to: change of address; addition of Insureds; change of benefits or options; change of Mode Of Premium Payment; group policy coverage, benefits, limitation or exclusion changes; or any future requirements of any federal or state law.
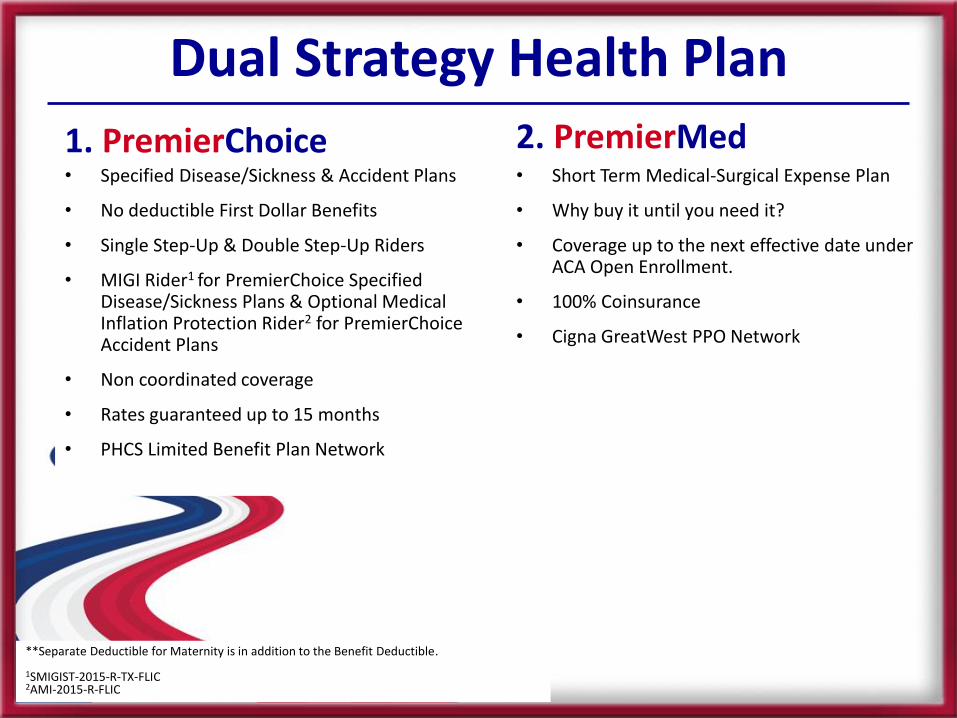
Dual Strategy Health Plan2. PremierMed• Short Term Medical-Surgical Expense Plan
• Why buy it until you need it?
• Coverage up to the next effective date under ACA Open Enrollment.
• 100% Coinsurance
• Cigna GreatWest PPO Network
1. PremierChoice• Specified Disease/Sickness & Accident Plans
• No deductible First Dollar Benefits
• Single Step-Up & Double Step-Up Riders
• MIGI Rider1 for PremierChoice Specified Disease/Sickness Plans & Optional Medical Inflation Protection Rider2 for PremierChoiceAccident Plans
• Non coordinated coverage
• Rates guaranteed up to 15 months
• PHCS Limited Benefit Plan Network
**Separate Deductible for Maternity is in addition to the Benefit Deductible.
1SMIGIST-2015-R-TX-FLIC2AMI-2015-R-FLIC


The individual mandate under the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year (Seeslide 59 of this presentation for details). The PremierMed Short Term Medical-Surgical Expense Plan is an insurance plan which provides benefits for a limitedduration for covered services and is neither an “essential health benefits plan” under the ACA, a traditional major medical insurance plan, nor a WorkersCompensation plan under state law. The PremierMed Short Term Medical-Surgical Expense Plan is “Short Term Medical-Surgical Insurance” and is not considered“minimum essential coverage” under the ACA. Therefore, unless an Insured under our PremierMed Short Term Medical-Surgical Expense Plan has an exemptionfrom the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s “shared responsibilitypayment” (See slide 59 of this presentation for details).
With the purchase of the PremierChoice Specified Disease/Sickness Plan and Our MIGI Rider, You have the one-time right to obtain additional coverageunder Our PremierMed Short Term Medical-Surgical Expense Plan without additional medical underwriting or evidence of Insurability. Under the MIGI RiderYou can exercise this option when You decide You need it, anytime, even in the middle of a claim. This unique option is intended to help You bridge the gapbetween the PremierChoice Specified Disease/Sickness and Accident Plans and the earliest of the following dates: (i) the earliest possible effective date ofcoverage for an ACA “qualified health plan” that could be purchased by You through a state or federal administered health insurance exchange in Your stateof residence, (ii) the effective date of Your coverage under any health plan that constitutes “minimum essential coverage” under federal law, and (iii) thedate coverage under the PremierMed Short Term Medical-Surgical Expense Plan otherwise terminates under the termination of coverage section of suchplan.The PremierMed Short Term Medical-Surgical Expense Plan provides coverage as of the Issue Date for Pre-existing Conditions, disclosed on the originalPremierChoice Specified Disease/Sickness application or that manifest during the period of PremierChoice Specified Disease/Sickness Plan coverage,provided they are not otherwise limited or excluded by the PremierMed Short Term Medical-Surgical Expense Plan or any riders, amendments, orendorsements attached to the PremierMed Short Term Medical-Surgical Expense Plan.

The individual mandate under the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year (Seeslide 59 of this presentation for details). The PremierMed Short Term Medical-Surgical Expense Plan is an insurance plan which provides benefits for a limitedduration for covered services and is neither an “essential health benefits plan” under the ACA, a traditional major medical insurance plan, nor a WorkersCompensation plan under state law. The PremierMed Short Term Medical-Surgical Expense Plan is “Short Term Medical-Surgical Insurance” and is not considered“minimum essential coverage” under the ACA. Therefore, unless an Insured under our PremierMed Short Term Medical-Surgical Expense Plan has an exemptionfrom the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s “shared responsibilitypayment” (See slide 59 of this presentation for details).
1Separate Deductible for Out of Network is in addition to the Benefit Deductible.2Separate Deductible for Maternity is in addition to the Benefit Deductible, up to a Maximum Maternity Benefit amount of $6,000.3Applies to each Subsequent Plan.4Based upon initial and 3 subsequent 90 day Plans. Does not include the Separate Maternity Deductible or the Failure to Pre-Authorize Treatment Deductible.
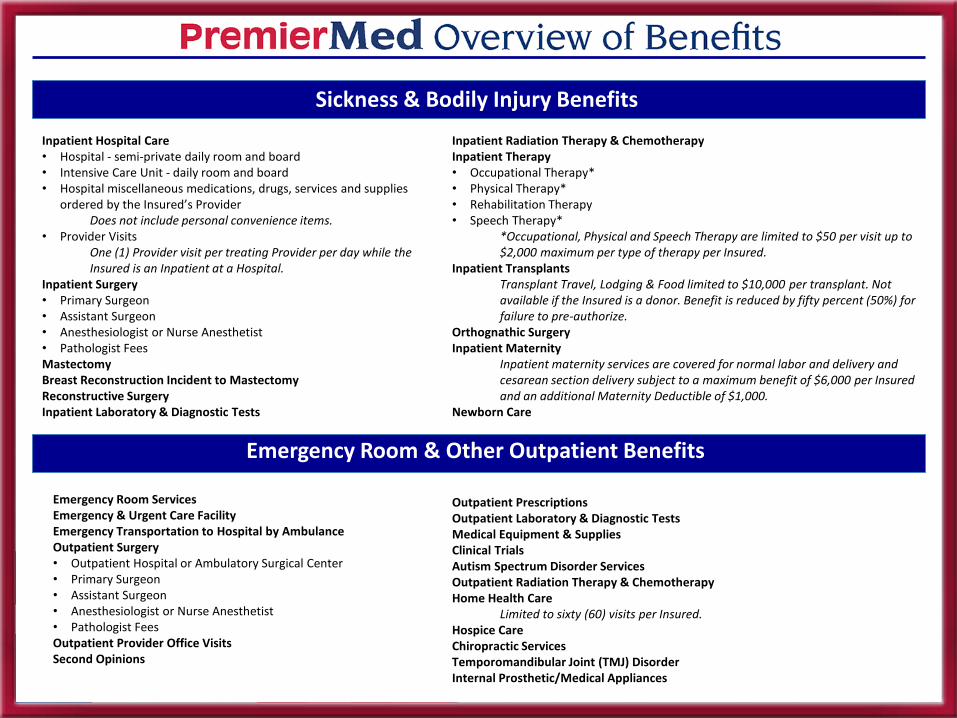
Emergency Room & Other Outpatient Benefits
Inpatient Hospital Care• Hospital - semi-private daily room and board • Intensive Care Unit - daily room and board • Hospital miscellaneous medications, drugs, services and supplies
ordered by the Insured’s ProviderDoes not include personal convenience items.
• Provider VisitsOne (1) Provider visit per treating Provider per day while the Insured is an Inpatient at a Hospital.
Inpatient Surgery• Primary Surgeon • Assistant Surgeon • Anesthesiologist or Nurse Anesthetist • Pathologist FeesMastectomyBreast Reconstruction Incident to MastectomyReconstructive SurgeryInpatient Laboratory & Diagnostic Tests
Inpatient Radiation Therapy & ChemotherapyInpatient Therapy• Occupational Therapy* • Physical Therapy* • Rehabilitation Therapy • Speech Therapy*
*Occupational, Physical and Speech Therapy are limited to $50 per visit up to $2,000 maximum per type of therapy per Insured.
Inpatient TransplantsTransplant Travel, Lodging & Food limited to $10,000 per transplant. Not available if the Insured is a donor. Benefit is reduced by fifty percent (50%) for failure to pre-authorize.
Orthognathic SurgeryInpatient Maternity
Inpatient maternity services are covered for normal labor and delivery and cesarean section delivery subject to a maximum benefit of $6,000 per Insured and an additional Maternity Deductible of $1,000.
Newborn Care
Emergency Room ServicesEmergency & Urgent Care FacilityEmergency Transportation to Hospital by AmbulanceOutpatient Surgery• Outpatient Hospital or Ambulatory Surgical Center • Primary Surgeon • Assistant Surgeon • Anesthesiologist or Nurse Anesthetist • Pathologist FeesOutpatient Provider Office VisitsSecond Opinions
Outpatient PrescriptionsOutpatient Laboratory & Diagnostic TestsMedical Equipment & Supplies Clinical TrialsAutism Spectrum Disorder ServicesOutpatient Radiation Therapy & ChemotherapyHome Health Care
Limited to sixty (60) visits per Insured.Hospice CareChiropractic ServicesTemporomandibular Joint (TMJ) DisorderInternal Prosthetic/Medical Appliances
Sickness & Bodily Injury Benefits
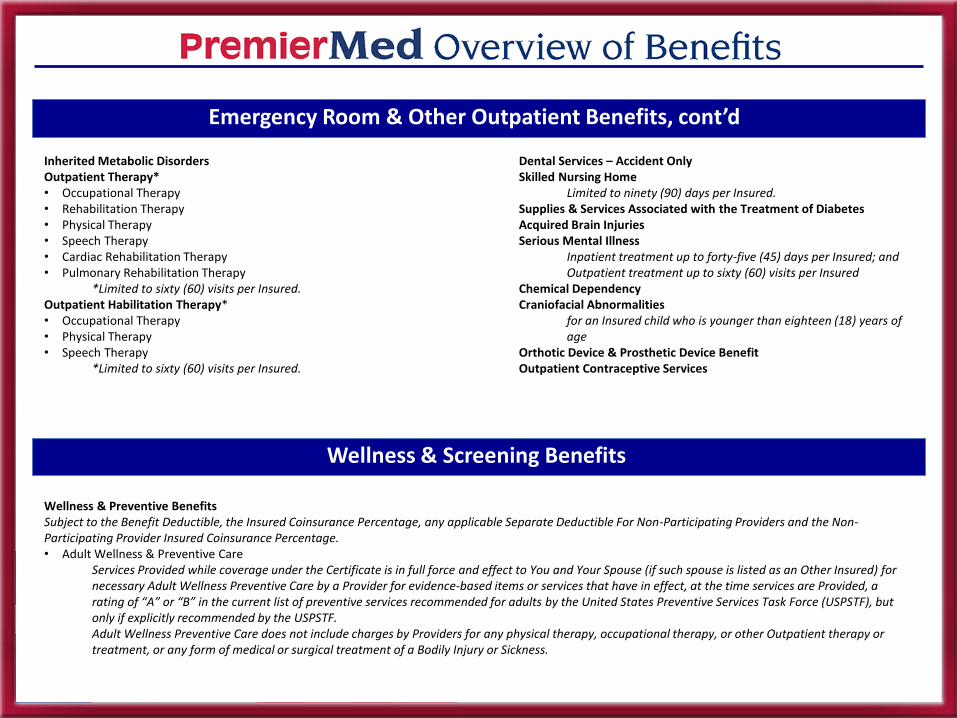
Emergency Room & Other Outpatient Benefits, cont’d
Inherited Metabolic DisordersOutpatient Therapy*• Occupational Therapy• Rehabilitation Therapy• Physical Therapy• Speech Therapy• Cardiac Rehabilitation Therapy• Pulmonary Rehabilitation Therapy
*Limited to sixty (60) visits per Insured.Outpatient Habilitation Therapy*• Occupational Therapy• Physical Therapy• Speech Therapy
*Limited to sixty (60) visits per Insured.
Dental Services – Accident OnlySkilled Nursing Home
Limited to ninety (90) days per Insured.Supplies & Services Associated with the Treatment of DiabetesAcquired Brain InjuriesSerious Mental Illness
Inpatient treatment up to forty-five (45) days per Insured; and Outpatient treatment up to sixty (60) visits per Insured
Chemical DependencyCraniofacial Abnormalities
for an Insured child who is younger than eighteen (18) years of age
Orthotic Device & Prosthetic Device BenefitOutpatient Contraceptive Services
Wellness & Screening Benefits
Wellness & Preventive BenefitsSubject to the Benefit Deductible, the Insured Coinsurance Percentage, any applicable Separate Deductible For Non-Participating Providers and the Non-Participating Provider Insured Coinsurance Percentage.• Adult Wellness & Preventive Care
Services Provided while coverage under the Certificate is in full force and effect to You and Your Spouse (if such spouse is listed as an Other Insured) for necessary Adult Wellness Preventive Care by a Provider for evidence-based items or services that have in effect, at the time services are Provided, a rating of “A” or “B” in the current list of preventive services recommended for adults by the United States Preventive Services Task Force (USPSTF), but only if explicitly recommended by the USPSTF.Adult Wellness Preventive Care does not include charges by Providers for any physical therapy, occupational therapy, or other Outpatient therapy or treatment, or any form of medical or surgical treatment of a Bodily Injury or Sickness.

Wellness & Screening Benefits, cont’d
• Childhood Wellness & Preventive CareServices Provided while coverage under the Certificate is in full force and effect by a Provider to each infant, child, and adolescent Insured for Medically Necessary Childhood Wellness Preventive Care for evidence-based items or services that have in effect, at the time services are Provided, a rating of “A” or “B” at ages recommended by the United States Preventive Services Task Force (USPSTF), but only if explicitly recommended by the USPSTF. Childhood Wellness Preventive Care also includes evidence-informed preventive care and screenings Provided for the appropriate age in the comprehensive guidelines supported by the Health Resources and Services Administration and by the American Academy of Pediatrics (AAP) and Bright Futures. Immunizations provided for children through their sixth (6th) birthday are not subject to any deductible or coinsurance.Childhood Wellness Preventive Care does not include charges by Providers for any physical therapy, occupational therapy, or other Outpatient therapy or treatment, or any form of medical or surgical treatment of a Bodily Injury or Sickness.
Screening & Examination BenefitsSCREENING AND EXAMINATION BENEFITS are subject to all applicable definitions, exclusions, limitations, and other provisions contained in the Certificate, as well as any riders, endorsements, or amendments attached hereto. We promise to pay to or on behalf of each Insured the Company Insurance Percentage of the amount of professional fees and other applicable medical diagnostic or treatment expenses and charges that constitute Covered Expenses incurred by each Insured while coverage under the Certificate is in full force and effect for the following described SCREENING AND EXAMINATION BENEFITS, but only after (i) each of the applicable deductibles has been first satisfied by deduction from such Covered Expenses and applied to the applicable Insured for payment and (ii) the applicable Insured Coinsurance Percentage for the Covered Expenses remaining after satisfaction of all applicable deductibles is, likewise, satisfied by deduction from the remaining Covered Expenses and applied to the applicable Insured for payment:• Mammography Screening
One Mammogram, every twelve (12) months, for female Insureds age thirty-five (35) and over; or non-routine screening Provided more frequently than above is covered based on recommendation of the Insured’s Provider.
• Prostate Cancer ScreeningAnnual examination for male Insureds age forty (40) or older who are asymptomatic or who are under forty (40) and have a family history of prostate cancer or another risk factor.
• Routine Annual Physical ExaminationLimited to one (1) visit for the duration of the Certificate for Insureds ages four (4) and up with examination performed by a Participating Provider.
• Newborn Hearing ScreeningServices Provided while coverage under the Certificate is in full force and effect by a Hospital or a Provider for (i) one hearing screening test for newborn children through the date that the child is thirty (30) days of age and (ii) diagnostic follow-up care related to the hearing screening at birth through the date the child is twenty-four (24) months of age. This Benefit has no dollar limit and is not subject to any otherwise applicable deductible under the Certificate; but is subject to the Insured Coinsurance Percentage shown on the Certificate Schedule for Participating Providers and Non-Participating Providers as applicable based on the Provider utilized.

Wellness & Screening Benefits, cont’d
Screening & Examination Benefits, cont’d
• Osteoporosis ScreeningServices Provided during the Benefit Period for a medically accepted bone mass measurement to detect low bone mass and determine the Insured’s risk of osteoporosis and fractures associated with osteoporosis to an Insured who is: a postmenopausal female Insured who is not receiving estrogen replacement therapy; an Insured with: a) vertebral abnormalities; b) primary hyperparathyroidism; or c) a history of bone fractures; or an Insured who is: a) receiving long-term glucocorticoid therapy; or being monitored to assess the response to or efficacy of an approved osteoporosis drug therapy.
• Cervical Cancer ScreeningServices Provided during the Benefit Period for a pap smear screening or liquid based cytology test annually for female Insureds over age eighteen (18) for cancer and human papillomavirus detection.
• Cardiovascular Disease ScreeningServices Provided during the Benefit Period for early detection tests for cardiovascular disease for each Insured: 1) who is: a) male and older than 45 years of age but younger than 76; b) female and older than 55 years of age but younger than 76; 2) who: a) is diabetic; or b) has a risk of developing coronary heart disease based on the Framingham Heart Study coronary prediction algorithm that is intermediate or higher. Services include the following noninvasive screening tests for atherosclerosis and abnormal artery structure and function every five (5) years: 1) computed tomography (CT) scanning measuring coronary artery calcification; or 2) ultrasonography measuring carotid intima-media thickness and plaque.
• Colorectal Cancer ScreeningServices Provided to Insureds age fifty (50) and older while coverage under the Certificate is in full force and effect for a fecal occult blood test and flexible sigmoidoscopy every five (5) years or a colonoscopy every ten (10) years.

Additional Optional Coverage
• IncomeProtectorShort Term Accident Disability Insurance
• PremierVisionVision Insurance
• LifeProtector10 Year Term Life Insurance
• MedGuard5 Year Term Life Insurance with Accelerated Death Benefit
• Accident ProtectorSupplemental Excess Accident Insurance
• SecureDentalDental Insurance

vFilling The Gap Between Health Coverage & Life Insurance
Critical Illness Statistics:
• Men have a 1-in-2 lifetime risk of getting cancer. Women have a 1-in-3 lifetime risk.1
• There are 14.5 million cancer survivors in the U.S.2
• 735,000 heart attacks occur each year — that’s one every43 seconds!3
• About 795,000 Americans will have a stroke this year —that’s one every 40 seconds!4
1www.cancer.org/cancer/cancerbasics/lifetime-probability-of-developing-or-dying-from-cancer2www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf3From the Heart Disease and Stroke Statistics - 2015 Update http://circ.ahajournals.org/content/early/2014/12/18/CIR.00000000000001524www.heart.org/idc/groups/ahamah-public/@wcm/@sop/@smd/documents/downloadable/ucm_470704.pdf
* CRTIL-06-C-TX-FLIC. Limitations and Exclusions apply. The MedGuard Plan has a separate brochure. If interested in this coverage, please see the MedGuardbrochure and Certificate for complete details.

Filling The Gap Between Health Coverage & Life Insurance
Benefits are reduced by 50% at age 65.Benefits are reduced by the amount of the Critical Illness Benefit paid.
*CRTIL-06-C-TX-FLIC. Limitations and Exclusions apply. The MedGuard Plan has a separate brochure. If interested in this coverage, please see the MedGuardbrochure and Certificate for complete details.

You can use the cash for any purpose You deem necessary, such as helping to:
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year(See slide 53 of this presentation for details). The MedGuard Plan is a life insurance plan with an accelerated death benefit rider, which pays the designatedpercentage of the Plan’s death benefit to the Insured upon the diagnosis of a covered critical condition or receipt of a covered critical surgery, as such it is not“health insurance coverage” under the ACA, Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered“minimum essential coverage” under the ACA. Therefore, unless an Insured under the MedGuard Plan has an exemption from the ACA’s individual mandate ormaintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment. (See slide 53 of thispresentation for details).
*CRTIL-06-C-TX-FLIC. Limitations and Exclusions apply. The MedGuard Plan has a separate brochure. If interested in this coverage, please see the MedGuardbrochure and Certificate for complete details.
Health coverage provides benefits for medical treatment but doesn’t includebenefits for non-medical expenses. Traditional life insurance pays benefits afterdeath. What if You survive a critical illness? Where will You find the financialresources to cover non-medical costs during Your recovery?
*

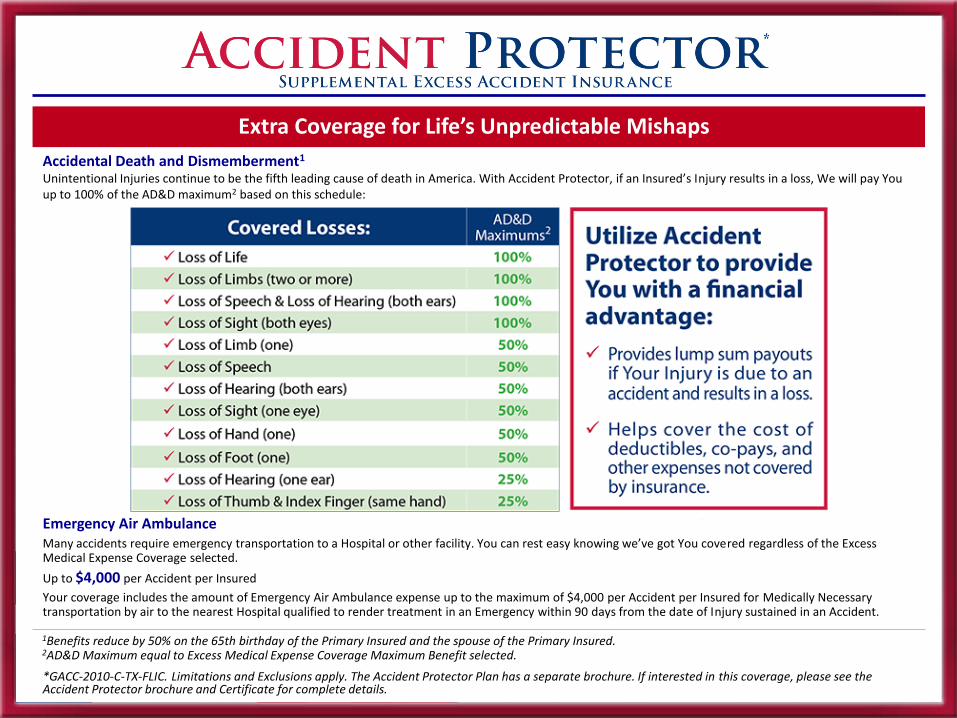
Extra Coverage for Life’s Unpredictable Mishaps
FACTS:• In 2010, nonfatal injuries cost society more than $471 billion in productivity losses and over $111 billion in medical costs.1
• More than 29 million people are treated in emergency rooms for injuries each year.2
• Each year, nearly 9.2 million children aged 0 to 19 years are seen in emergency rooms for injuries.3
• More than 2.8 million people hospitalized with injuries each year.4
1Finkelstein E, Corso PS, Miller TR. The incidence and economic burden of injuries in the United States. New York, NY: Oxford University Press.2NCIPC: Web-based Injury Statistics Query and Reporting System (WISQARS)3Centers for Disease Control and Prevention Safe Kids Fact sheet4NCHS. National hospital discharge survey: National health statistics reports, no. 29. Atlanta, GA; 2010.
*GACC-2010-C-TX-FLIC. Limitations and Exclusions apply. The Accident Protector Plan has a separate brochure. If interested in this coverage, please see the Accident Protector brochure and Certificate for complete details.**Benefits are subject to Your Excess Medical Expense Deductible per Accident per Insured.
Accident Protector pays You up to the Excess Medical Expense Coverage for the remaining amount of medical expenses incurred per Insured per Accident.
Excess Medical Expenses Coverage may include: Medically Necessary treatment by a physician, nurse or dentist; hospital room and board; outpatient surgery; ambulance; dental work to sound natural teeth; drugs; medicines; diagnostic tests and x-rays; oxygen; casts; splints; crutches; blood; plasma; and rental of durable medical equipment for a covered Accident or Injury. Benefits are subject to Your Excess Medical Expense Deductible per Accident per Insured.
Extra Coverage for Life’s Unpredictable Mishaps
Accidental Death and Dismemberment1
Unintentional Injuries continue to be the fifth leading cause of death in America. With Accident Protector, if an Insured’s Injury results in a loss, We will pay You up to 100% of the AD&D maximum2 based on this schedule:
Emergency Air AmbulanceMany accidents require emergency transportation to a Hospital or other facility. You can rest easy knowing we’ve got You covered regardless of the Excess Medical Expense Coverage selected.
Up to $4,000 per Accident per Insured
Your coverage includes the amount of Emergency Air Ambulance expense up to the maximum of $4,000 per Accident per Insured for Medically Necessary transportation by air to the nearest Hospital qualified to render treatment in an Emergency within 90 days from the date of Injury sustained in an Accident.
1Benefits reduce by 50% on the 65th birthday of the Primary Insured and the spouse of the Primary Insured.2AD&D Maximum equal to Excess Medical Expense Coverage Maximum Benefit selected.
*GACC-2010-C-TX-FLIC. Limitations and Exclusions apply. The Accident Protector Plan has a separate brochure. If interested in this coverage, please see the Accident Protector brochure and Certificate for complete details.

The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or be subject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year (See slide 54 of this presentation for details). The Accident Protector Plan is an excess medical expense coverage insurance plan which provides coverage for the remaining amount of medical expenses incurred per Insured per covered accident, as such it is not “health insurance coverage” under the ACA, Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered “minimum essential coverage” under the ACA. Therefore, unless an Insured under the Accident Protector Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment. (See slide 54 of this presentation for details).
We give You the option to select coverage that fits Your budget and needs. Choose Your coverage amount from the list below:
When it Comes to Accidents … You Can’t Be Too Careful.
*GACC-2010-C-TX-FLIC. Limitations and Exclusions apply. The Accident Protector Plan has a separate brochure. If interested in this coverage, please see the Accident Protector brochure and Certificate for complete details.

Everyone Deserves A Healthy Smile
SecureDental Offers 3 Plans:
Premium Plan*Deductibles: $50 for an Individual; $150 for a Family; Additional Orthodontic Deductible $150 per InsuredCovers Preventive Care, Basic Care, Major Care & Orthodontic CareCalendar Year Maximum Per Insured $1,500; Orthodontic Calendar Year Maximum Per Insured $400Saver Plus Plan*Deductibles: $50 for an Individual; $150 for a Family Covers Preventive Care, Basic Care & Major Care, with Orthodontic Care Services discounted at participating providers.Calendar Year Maximum Per Insured $1,000
Saver Plan* Deductibles: $50 for an Individual; $150 for a Family Covers Preventive Care & Basic Care, with Major Care & Orthodontic Care Services discounted at participating providers.Calendar Year Maximum Per Insured $500
Preventive CareBenefits include: Initial & Periodic oral examinations, Intraoral X-rays, with/without bitewings, Prophylaxis (cleaning of the teeth) with/without oral examination... and more
Basic CareBenefits include: Amalgam, silicate cement, acrylic or plastic fillings, Simple tooth Extractions, Oral Surgery ... and more
Major Care(Covered on Premium Plan & Saver Plus Plans. For Saver Plan, Insured(s) receive discounted services at participating providers for Major Care.)Benefits include: Single Crown restorations, Dentures, including fixed or removable prosthetic devices, complete Dentures, upper & lower, Root Canal Therapy, including treatment plan & follow-up care ... and more
Orthodontic Care(Covered on Premium Plan. For Saver Plus Plan & Saver Plans, Insured(s) receive discounted services at participating providers for Orthodontic Care.)Benefits include: Comprehensive Orthodontic Treatment of the adult dentition, Comprehensive Orthodontic Treatment of the adolescent dentition,Orthodontic retention (removal of appliances, construction & placement of retainer(s)) ... and moreSee Brochure for a complete listing of SecureDental Benefits
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year(See slide 57 of this presentation for details). The SecureDental Plan provides benefits for dental only coverage, but it is not Workers Compensation coverageunder state law or an “essential health benefits” under the ACA and it is not considered “minimum essential coverage” plan under the ACA. Therefore, unless anInsured under the SecureDental Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, theInsured will be subject to the ACA’s shared responsibility payment. (See slide 57 of this presentation for details).
*DENTAL-2013-C1-TX-FLIC. Limitations, Waiting Periods and Exclusions apply. SecureDental has a separate brochure. If interested in this coverage, please see the SecureDental brochure and Certificate for complete details.
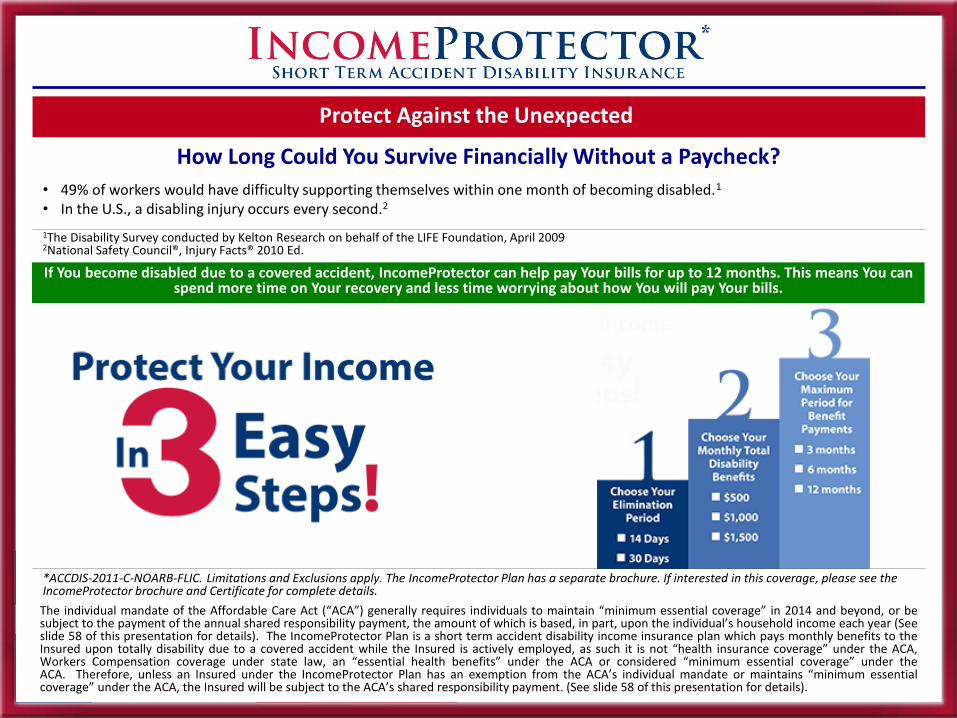
Protect Against the Unexpected
How Long Could You Survive Financially Without a Paycheck?
• 49% of workers would have difficulty supporting themselves within one month of becoming disabled.1
• In the U.S., a disabling injury occurs every second.2
1The Disability Survey conducted by Kelton Research on behalf of the LIFE Foundation, April 20092National Safety Council®, Injury Facts® 2010 Ed.
If You become disabled due to a covered accident, IncomeProtector can help pay Your bills for up to 12 months. This means You can spend more time on Your recovery and less time worrying about how You will pay Your bills.
*ACCDIS-2011-C-NOARB-FLIC. Limitations and Exclusions apply. The IncomeProtector Plan has a separate brochure. If interested in this coverage, please see the IncomeProtector brochure and Certificate for complete details.
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year (Seeslide 58 of this presentation for details). The IncomeProtector Plan is a short term accident disability income insurance plan which pays monthly benefits to theInsured upon totally disability due to a covered accident while the Insured is actively employed, as such it is not “health insurance coverage” under the ACA,Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered “minimum essential coverage” under theACA. Therefore, unless an Insured under the IncomeProtector Plan has an exemption from the ACA’s individual mandate or maintains “minimum essentialcoverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment. (See slide 58 of this presentation for details).

Let Us Help You See the World More Clearly
The PremierVision Plan is designed to be easy to use, while helping You save money.
1Limited to one (1) Comprehensive Eye Examination every twelve (12) months from the last date of service, per Insured.2In lieu of Corrective Contact Lenses, limited to one (1) purchase every twelve (12) months from the last date of service, per Insured. In no event will Benefits be payable for both glasses and corrective contact lenses.3 In lieu of Corrective Standard Lenses and Frames, limited to one (1) purchase every twelve (12) months from the last date of service, per Insured. In no event will Benefits be payable for both glasses and corrective contact lenses.
*VISION-2015-C1-TX-FLIC. Limitations and Exclusions apply. The PremierVision Plans have a separate brochure. If interested in this coverage, please see the PremierVision brochure and Certificate for complete details.

Let Us Help You See the World More Clearly
*VISION-2015-C1-TX-FLIC. Limitations and Exclusions apply. The PremierVision Plans have a separate brochure. If interested in this coverage, please see the PremierVision brochure and Certificate for complete details.
The PremierVision Plan is designed to be easy to use, while helping You save money.
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year.The PremierVision Plan provides benefits for vision only coverage, but it is not Workers Compensation coverage under state law or an “essential health benefits”under the ACA and it is not considered “minimum essential coverage” plan under the ACA. Therefore, unless an insured under the PremierVision Plan has anexemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the insured will be subject to the ACA’s sharedresponsibility payment. For additional information on the individual mandate, “shared responsibility payment”, exemptions from the mandate and other mattersconcerning the ACA, please visit www.healthcare.gov, the federal government’s website.

Provide Peace of Mind for Your Loved Ones
*10TERM-P-TX-FLIC. Limitations and Exclusions apply. The LifeProtector Plan has a separate brochure. If interested in this coverage, please see the LifeProtectorbrochure and Policy for complete details.
• Odds of dying as a consequence of heart disease – 1 in 51
• Odds of dying as a consequence of cancer – 1 in 71
• Total odds of dying, any cause – 1 in 1 (100%)1
1National Safety Council
Most Americans need life insurance, and many who already have it may need to update their coverage.
LifeProtector is the Right Choice!Providing peace of mind for Your family is essential. If something unforeseen were to happen to You, would Your family be taken care of financially? With America’s Choice LifeProtector, You can help provide the financial security Your family needs and deserves.
Advantages of America’s Choice LifeProtector
ConvenientLifeProtector is a great option to add to Your portfolio.
Pure & SimpleProvides protection to help with obligations like mortgage, car payment, childcare or educational expenses and other obligations.
Peace of MindProvides protection in the event of unforeseen death.
Not Taxable to BeneficiariesProvides valuable life insurance benefits that in most instances are free from income tax for the beneficiary.
EconomicalWith premium payment options from $10 to $50, all in $5 increments, it’s easy to find an economical solution to Your life insurance needs
$10 $15 $20 $25 $30 $35 $40 $45 $50

• war, or any act of war, regardless of whether war is actually declared;• serving in one of the branches of the armed forces of any foreign
country or any international authority;• such Insured Member being intoxicated or under the influence of
alcohol or any drug, narcotic or hallucinogens, unless administered via a prescription and on the advice of a Provider, and taken in accordance with the limits of such advice;
• intentionally self-inflicted Bodily Injury;• suicide or any attempt thereat, while sane;• Sickness;• travel by or participation in aviation, except as a fare-paying passenger
traveling on a regular scheduled commercial airline flight;• engaging in and being charged with any felony criminal offense;• a Bodily Injury occurring outside the borders of the United States of
America or its territories;• the unintended or accidental results of any surgery or operation
performed either for cosmetic purposes or in an attempt to surgically treat any Sickness;
• intentional inhalation or ingestion of any poison, gas or fumes;• expenses Incurred for the diagnosis, care or treatment of Mental and
Emotional Disorders, Alcoholism, and Drug Addiction/Abuse;• participating, as driver or passenger, in any competition, race or speed
contest, including sanctioned practice thereof, of any land or water vehicle;
• expenses Incurred as a result of a Bodily Injury that are in excess of the Usual and Customary expenses Incurred for Medically Necessary treatment of such Bodily Injury;
• expenses Incurred for the Medically Necessary treatment of a Bodily Injury for which the Insured Member has no legal liability and responsibility for payment;
• expenses Incurred for the Medically Necessary treatment of a Bodily Injury that are covered under any other valid insurance coverage, accident medical expense benefits or health benefit plan coverage (e.g. uninsured/underinsured motorist coverage, personal injury protection coverage under any automobile policy, comprehensive major medical insurance, hospital/medical surgical insurance, other indemnity health insurance, health coverage under an HMO or PPO plan, workers compensation medical expense benefits, FELA medical expense benefits, Jones Act medical expense benefits, Medicaid and Medicare);
• a scheduled Benefit under Accidental Death & Dismemberment Coverage or an expense under Excess Medical Expense Coverage that exceeds the amount of the Lifetime Policy Maximum Benefit;
• the operation by such Insured Member of any motor vehicle without the permission/consent of the owner of such vehicle;
• the operation by such Insured Member of any motor vehicle without a valid operator’s license/permit; and
• bacterial or viral infection, except such infection occurring with or through a cut or wound in the skin sustained in an Accident or the accidental ingestion of contaminated material.
Association BLANKET GROUP EXCESS MEDICAL EXPENSE AND AD&D – Limitations at a Glance
In addition to any other provisions of the Blanket Group Policy Benefits and coverage are limited as follows:• Coverage for AD&D and Excess Medical Expense commences on the Primary Insured Effective Date for each Primary Insured;• The Lifetime Policy Maximum Benefit is as shown on the preceding page;• The AD&D Maximum Benefit for the Primary Insured is as shown on the preceding page;• The AD&D Maximum Benefit for the Spouse of Primary Insured is as shown on the preceding page;• The AD&D Maximum Benefit for the Children of Primary Insured is as shown on the preceding page;• The Excess Medical Expense Coverage Maximum Benefit is as selected in writing by the Blanket Group Policyholder prior to the Issue Date;• The maximum dollar amount recoverable by an Insured for AD&D is the applicable AD&D Maximum Benefit, regardless of the number of Accidents or Bodily
Injuries sustained by an Insured; and • The applicable AD&D Maximum Benefit and the Excess Medical Expense Coverage Maximum Benefit automatically reduce by fifty percent (50%) on the sixty-
fifth (65th) birthday of the Primary Insured and Spouse of Primary Insured.
Association BLANKET GROUP EXCESS MEDICAL EXPENSE AND AD&D Non-Covered Items at a Glance
The Blanket Group Policy does not provide any Benefit, coverage or payment for any loss caused by, in whole or in part, contributed to or resulting from, directly or indirectly, any of the following incidents, events, occurrences or activities involving such Insured Member:
Association Blanket Group Specified Disease/Illness - Limitations At A Glance
Coverage under the Blanket Group Specified Disease/Illness Insurance Policy is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every Section of the Blanket Group Specified Disease/Illness Insurance Policy, as well as the following limitations and waiting periods:
• Any treatment, medical service, surgery, medication, equipment, claim, loss or expense received, purchased, leased or otherwise incurred as a result of an Insured’s Pre-existing Condition is not covered under the Blanket Group Specified Disease/Illness Insurance Policy unless such treatment, medical service, surgery, medication, equipment, claim, loss or expense constitutes Covered Expenses incurred by such Insured more than twelve (12) months after the Issue Date, and such treatment, medical service, surgery, medication, equipment, claim, loss or expense are not otherwise limited or excluded by the Blanket Group Specified Disease/Illness Insurance Policy or any riders, endorsements, or amendments attached to the Blanket Group Specified Disease/Illness Insurance Policy;
• Covered Medical Services Benefits under the Blanket Group Specified Disease/Illness Insurance Policy for any Insured who is eligible for or has coverage under Medicare, and/or amendments thereto, regardless of whether such Insured is enrolled in Medicare shall be limited to only the Usual and Customary Expenses for services, supplies, care or treatment covered under the Blanket Group Specified Disease/Illness Insurance Policy that are not or would not have been payable or reimbursable by Medicare and/or its amendments (assuming such enrollment), subject to all provisions, limitations, exclusions, reductions and maximum benefits set forth in the Blanket Group Specified Disease/Illness Insurance Policy;
• Any Covered Medical Services payable under the Blanket Group Specified Disease/Illness Insurance Policy will be reduced by fifty percent (50%) when the applicable Insured is age sixty-five (65) or older, based on the Insured’s most recent birthday, on the date the Benefit becomes payable; and
• In no event will the total amount of benefits payable for any one Insured exceed the Lifetime Policy Maximum Per Insured.
Pre-existing Condition means a condition, whether physical or mental and regardless of the cause: 1. for which medical advice, diagnosis care or treatment wasrecommended or received during the twelve (12) month period immediately preceding the effective date of coverage under the Blanket Group SpecifiedDisease/Illness Insurance Policy for the Insured incurring the expense; or 2. which Manifested during the twelve (12) month period immediately preceding theeffective date of coverage under the Blanket Group Specified Disease/Illness Insurance Policy for the Insured incurring the expense.

b• any cost item, charge or expense which does not constitute Covered
Expenses; • any Bodily Injuries suffered by an Insured; • any disease, ailment, illness or sickness that is not a Specified
Disease/Illness; • any medical care, service, treatments, procedures, or supplies received,
provided to, or incurred by an Insured before the Blanket Group Specified Disease/Illness Insurance Policy Issue Date and the Primary Insured Effective Date;
• any treatments, care, procedures, services or supplies which are not specifically enumerated in the SPECIFIED DISEASE/ILLNESS BENEFITS AND CLAIM PROCEDURES section of the Blanket Group Specified Disease/Illness Insurance Policy;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured after an Insured’s coverage under the Blanket Group Specified Disease/Illness Insurance Policy terminates, regardless of when the sickness or disease occurred;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which exceed the Lifetime Insurance Policy Maximum Per Insured;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured and contained on a billing statement to the Insured which exceeds the amount of the Maximum Allowable Charge;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which You or Your covered family members are not required to pay;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members are not legally liable for payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members were once legally liable for payment, but from which liability the Insured and/or family members were forgiven and released by the applicable Provider without payment or promise of payment;
Association Blanket Group Specified Disease/Illness - Non-Covered Items At A GlanceCoverage under the Blanket Group Specified Disease/Illness Insurance Policy is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every Section of the Blanket Group Specified Disease/Illness Insurance Policy. In addition, the Blanket Group Specified Disease/Illness Insurance Policy does not provide coverage for the amount of any professional fees or other medical expenses or charges for treatments, care, procedures, services or supplies incurred for the diagnosis, care or treatment charged to an Insured or any payment obligation for Us under the Blanket Group Specified Disease/Illness Insurance Policy for any of the following, all of which are excluded from coverage:
• Specified Diseases/Illnesses due to any act of war (whether declared or undeclared);
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured from any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured as a result of experimental procedures or treatment methods not approved by the American Medical Association or other appropriate medical society;
• drugs or medication not used for a Food and Drug Administration (“FDA”) approved use or indication;
• administration of experimental drugs or substances or investigational use or experimental use of Prescription Drugs except for any Prescription Drug prescribed to treat a covered chronic, disabling, life-threatening Specified Disease/Illness, but only if the investigational or experimental drug in question: (a) has been approved by the FDA for at least one indication; and (b) is recognized for treatment of the indication for which the drug is prescribed in: (1) a standard drug reference compendia; or (2) substantially accepted peer-reviewed medical literature. (c) drugs labeled “Caution – limited by Federal law to investigational use”;
• any professional and medical services Provided an Insured in treatment of a Specified Disease/Illness caused or contributed to by such Insured's being intoxicated or under the influence of any drug, narcotic or hallucinogens unless administered on the advice of a Provider, and taken in accordance with the limits of such advice;
• any eyeglasses, contact lenses, radial keratotomy, lasik surgery, hearing aids and exams for their prescription or fitting;
• any Cochlear implants; • Specified Disease/Illness while serving in one of the branches of the
armed forces of the United States of America; • Specified Disease/Illness while in a foreign country and serving on
active duty in one of the branches of the armed services of the United States of America;

• Specified Disease/Illness while serving on active duty in the armed forces of any foreign country or any international authority;
• any voluntary abortions, abortifacients or any other drug or device that terminates a pregnancy;
• any services Provided by You or a Provider who is a member of an Insured's family;
• any medical condition excluded by name or specific description by either the Blanket Group Specified Disease/Illness Insurance Policy or any riders, endorsements, or amendments attached to the Blanket Group Specified Disease/Illness Insurance Policy;
• any cosmetic surgery or reconstructive procedures, except for Medically Necessary cosmetic surgery or reconstructive procedures performed under the following circumstances: (i) where such cosmetic surgery is incidental to or following surgery resulting from Bacterial Infection or Viral Infection, (ii) to correct a normal bodily function in connection with the treatment of a covered Specified Disease/Illness, or (iii) such cosmetic surgery constitutes Breast Reconstruction that is incident to a Mastectomy; provided any of the above occurred while the Insured was covered under the Blanket Group Specified Disease/Illness Insurance Policy;
• Prescription Drugs or other medicines and products used for cosmetic purposes or indications;
• Outpatient Prescription Drugs that are dispensed by a Provider, Hospital or other state-licensed facility;
• Prescription Drugs produced from blood, blood plasma and blood products, derivatives, Hemofil M, Factor VIII, and synthetic blood products, or immunization agents, biological or allergy sera, hematinics, blood or blood products administered on an Outpatient basis;
• Prescription Drugs that are classified as anabolic steroids or growth hormones;
• allergy kits intended for future emergency treatment of possible future allergic reactions;
• replacement of a prior filled Prescription for Prescription Drugs that was covered and is replaced because the original Prescription was lost, stolen or damaged;
• Prescription Drugs that are classified as psychotherapeutic drugs, including antidepressants;
• any treatment, care, procedures, services or supplies for breast reduction or augmentation or complications arising from these procedures;
• any treatment, care, procedures, services or supplies for voluntary sterilization, reversal or attempted reversal of a previous elective attempt to induce or facilitate sterilization;
• any treatment, care, procedures, services or supplies for treatment of infertility, including fertility hormone therapy and/or fertility devices for any type of fertility therapy, artificial insemination or any other direct conception;
Association Blanket Group Specified Disease/Illness - Non-Covered Items At A Glance, cont’d
• any treatment, care, procedures, services or supplies for any operation or treatment performed, Prescription or medication prescribed in connection with sex transformations or any type of sexual or erectile dysfunction, including complications arising from any such operation or treatment;
• any treatment, care, procedures, services or supplies (including Prescription Drugs) incurred for the diagnosis, care or treatment of Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD);
• any treatment, care, procedures, services or supplies for appetite suppressants, including but not limited to, anorectics or any other drugs used for the purpose of weight control, or services, treatments, or surgical procedures rendered or performed in connection with an overweight condition or a condition of obesity or related conditions;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Mental, Nervous and Emotional Disorders;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of autism spectrum disorder;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Alcoholism, addiction to illegal drugs or substances, and/or abuse of illegal drugs or substances;
• any treatment care, procedures, services or supplies incurred for the diagnosis, care or treatment of cirrhosis of the liver;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of routine maternity or any other expenses related to normal labor and delivery, including routine nursery charges and well-baby care;
• any contraceptives, oral or otherwise, whether medication or device, regardless of intended use;
• any fluoride products; • any intentional misuse or abuse of Prescription Drugs, including
Prescription Drugs purchased by an Insured for consumption by someone other than such Insured;
• any programs, treatment or procedures for tobacco use cessation; • any charges for blood, blood plasma, or derivatives that has been
replaced; • compounded Prescription Drugs; • level one controlled substances; • any treatment, care, procedures, services or supplies of
Temporomandibular Joint Disorder (TMJ) and CraniomandibularDisorder (CMD);
• any treatment received outside of the United States; • any services or supplies for personal convenience, including Custodial
Care or homemaker services, except as provided for in the Blanket Group Specified Disease/Illness Insurance Policy; and
• any spinal manipulations.

bAssociation Blanket Group Accident - Limitations At A GlanceCoverage under the Blanket Group Accident Only Insurance Policy is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every Section of the Blanket Group Accident Only Insurance Policy, as well as the following limitations and waiting periods:• Any treatment, medical service, surgery, medication, equipment, claim, loss or expense received, purchased, leased or otherwise incurred as a result of an
Insured’s Pre-existing Condition is not covered under the Blanket Group Accident Only Insurance Policy unless such treatment, medical service, surgery, medication, equipment, claim, loss or expense constitutes Covered Expenses incurred by such Insured more than twelve (12) months after the Effective Date, and such treatment, medical service, surgery, medication, equipment, claim, loss or expense are not otherwise limited or excluded by the Blanket Group Accident Only Insurance Policy or any riders, endorsements, or amendments attached to the Policy;
• Covered Medical Services Benefits under the Blanket Group Accident Only Insurance Policy for any Insured who is eligible for or has coverage under Medicare, and/or amendments thereto, regardless of whether such Insured is enrolled in Medicare shall be limited to only the Usual and Customary Expenses for services, supplies, care or treatment covered under the Policy that are not or would not have been payable or reimbursable by Medicare and/or its amendments (assuming such enrollment), subject to all provisions, limitations, exclusions, reductions and maximum benefits set forth in the Policy;
• Any Covered Medical Services payable under the Blanket Group Accident Only Insurance Policy will be reduced by fifty percent (50%) when the applicable Insured is age sixty-five (65) or older, based on the Insured’s most recent birthday, on the date the Benefit becomes payable; and
• In no event will the total amount of benefits payable for any one Insured exceed the Lifetime Policy Maximum Per Insured.
Pre-existing Condition means a Bodily Injury: 1. for which medical advice, diagnosis, care or treatment was recommended or received during the twelve (12)month period immediately preceding the effective date of coverage under this Blanket Group Accident Only Insurance Policy for the Insured incurring theexpense; or 2. resulting from an Accident that occurred before the Effective Date for the Insured incurring the expense.
Association Blanket Group Accident - Non-Covered Items At A GlanceCoverage under the Blanket Group Accident Only Insurance Policy is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every Section of the Blanket Group Accident Only Insurance Policy. In addition, the Blanket Group Accident Only Insurance Policy does not provide coverage for the amount of any professional fees or other medical expenses or charges for treatments, care, procedures, services or supplies incurred for the diagnosis, care or treatment charged to an Insured or any payment obligation for Us under the Blanket Group Accident Only Insurance Policy for any of the following, all of which are excluded from coverage:
• any cost item, charge or expense which does not constitute Covered Expenses;
• any disease, ailment, illness or sickness suffered by an Insured, except a covered Bacterial Infection;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured before the Blanket Group Accident Only Insurance Policy Issue Date and the Primary Insured Effective Date;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured after an Insured’s coverage under the Blanket Group Accident Only Insurance Policy terminates, regardless of when the Bodily Injury occurred;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which exceed the Lifetime Insurance Policy Maximum Per Insured;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured and contained on a billing statement to the Insured which exceeds the amount of the Maximum Allowable Charge;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which You or Your covered family members are not required to pay;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members are not legally liable for payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members were once legally liable for payment, but from which liability the Insured and/or family members were forgiven and released by the applicable Provider without payment or promise of payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured from any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured as a result of experimental procedures or treatment methods not approved by the American Medical Association or other appropriate medical society;
• Bodily Injury due to any act of war (whether declared or undeclared); • services provided by any state or federal government agency, including the
Veterans Administration unless, by law, an Insured must pay for such services;
• drugs or medication not used for a Food and Drug Administration (“FDA”) approved use or indication;

• administration of experimental drugs or substances or investigational use or experimental use of Prescription Drugs except for any Prescription Drug prescribed to treat a covered chronic, disabling, life-threatening Bodily Injury, but only if the investigational or experimental drug in question: (a) has been approved by the FDA for at least one indication; and (b) is recognized for treatment of the indication for which the drug is prescribed in: (1) a standard drug reference compendia; or (2) substantially accepted peer-reviewed medical literature. (c) drugs labeled “Caution – limited by Federal law to investigational use”;
• intentionally self-inflicted Bodily Injury, suicide or any suicide attempt while sane or insane;
• Bodily Injury while serving in one of the branches of the armed forces of the United States of America;
• Bodily Injury while in a foreign country and serving on active duty in the United States Army, Navy, Marine Corps or Air Force Reserves or the National Guard;
• Bodily Injury while serving on active duty in the armed forces of any foreign country or any international authority;
• voluntary abortions, abortifacients or any other drug or device that terminates a pregnancy;
• any medical condition excluded by name or specific description by either the Blanket Group Accident Only Insurance Policy or any riders, endorsements, or amendments attached to the Blanket Group Accident Only Insurance Policy;
• any loss to which a contributing cause was the Insured's being engaged in an illegal occupation or illegal activity;
• participation in aviation, except as fare-paying passenger traveling on a regular scheduled commercial airline flight;
• any Injury which was caused or contributed by an Insured racing any land or water vehicle;
• Prescription Drugs or other medicines and products used for cosmetic purposes or indications;
• Prescription Drugs that are classified as psychotherapeutic drugs, including antidepressants;
• Outpatient Prescription Drugs that are dispensed by a Provider, Hospital or other state-licensed facility;
• Prescription Drugs produced from blood, blood plasma and blood products, derivatives, Hemofil M, Factor VIII, and synthetic blood products, or immunization agents, biological or allergy sera, hematinics, blood or blood products administered on an Outpatient basis;
• level one controlled substances; • Prescription Drugs that are classified as anabolic steroids or growth
hormones; • compounded Prescription Drugs; • allergy kits intended for future emergency treatment of possible future
allergic reactions;• replacement of a prior filled Prescription for Prescription Drugs that was
covered and is replaced because the original Prescription was lost, stolen or damaged;
Association Blanket Group Accident - Non-Covered Items At A Glance, cont’d
• any eyeglasses, contact lenses, radial keratotomy, lasik surgery, hearing aids and exams for their prescription or fitting;
• any Cochlear implants; • any services Provided by You or a Provider who is a member of an
Insured's family; • any medical condition excluded by name or specific description by either
the Blanket Group Accident Only Insurance Policy or any riders, endorsements, or amendments attached to the Blanket Group Accident Only Insurance Policy;
• any cosmetic surgery or reconstructive procedures, except for Medically Necessary cosmetic surgery or reconstructive procedures performed under the following circumstances: (i) where such cosmetic surgery is incidental to or following surgery resulting from Bacterial Infection or (ii) to correct a normal bodily function in connection with the treatment of a covered Bodily Injury;
• any treatment, care, procedures, services or supplies for breast reduction or augmentation or complications arising from these procedures;
• any treatment, care, procedures, services or supplies for voluntary sterilization, reversal or attempted reversal of a previous elective attempt to induce or facilitate sterilization;
• any treatment, care, procedures, services or supplies for treatment of infertility, including fertility hormone therapy and/or fertility devices for any type of fertility therapy, artificial insemination or any other direct conception;
• any treatment, care, procedures, services or supplies for any operation or treatment performed, Prescription or medication prescribed in connection with sex transformations or any type of sexual or erectile dysfunction, including complications arising from any such operation or treatment;
• any treatment, care, procedures, services or supplies for appetite suppressants, including but not limited to, anorectics or any other drugs used for the purpose of weight control, or services, treatments, or surgical procedures rendered or performed in connection with an overweight condition or a condition of obesity or related conditions;
• any treatment, care, procedures, services or supplies (including Prescriptions) incurred for the diagnosis, care or treatment of Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD);
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Mental, Nervous and Emotional Disorders;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of autism;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of alcoholism, addiction to illegal drugs or substances, and/or abuse of illegal drugs or substances;
• any treatment care, procedures, services or supplies incurred for the diagnosis, care or treatment of cirrhosis of the liver;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of routine maternity or any other expenses related to normal labor and delivery, including routine nursery charges and well-baby care;
Association Blanket Group Accident - Non-Covered Items At A Glance, cont’d• any contraceptives, oral or otherwise, whether medication or device, regardless of intended use; • any fluoride products;• any intentional misuse or abuse of Prescription Drugs, including Prescription Drugs purchased by an Insured for consumption by someone other than such
Insured; • any programs, treatment or procedures for tobacco use cessation; • any charges for blood, blood plasma, or derivatives that has been replaced; • any treatment, care, procedures, services or supplies of Temporomandibular Joint Disorder (TMJ) and Craniomandibular Disorder (CMD); • any treatment received outside of the United States; and • any services or supplies for personal convenience, including Custodial Care or homemaker services, except as provided for in the Blanket Group Accident
Only Insurance Policy.
PremierChoice Specified Disease/Sickness Plan Waiting Periods & Limitations
Coverage under the PremierChoice Specified Disease/Sickness Plan is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every section of the PremierChoice Specified Disease/Sickness Plan, as well as the following limitations and waiting periods:• The PremierChoice Specified Disease/Sickness Plan provides coverage as of the Issue Date for Pre-existing Conditions, disclosed on the application, provided they
are not otherwise limited or excluded by the PremierChoice Specified Disease/Sickness Plan or any riders, amendments, or endorsements attached to the PremierChoice Specified Disease/Sickness Plan. The PremierChoice Specified Disease/Sickness Plan does not cover expenses for Pre-existing Conditions that are not disclosed on the application, unless the expenses are incurred more than twelve (12) months after the Insured’s coverage has been in effect, and are not otherwise limited or excluded by the PremierChoice Specified Disease/Sickness Plan or any riders, amendments, or endorsements attached to the PremierChoiceSpecified Disease/Sickness Plan; and
• Any Specified Disease/Sickness loss or expense which is incurred before the expiration of six (6) months from the Issue Date which results from the diagnosis, care or treatment of hernia, Reproductive System Disease, hemorrhoids, varicose veins, tonsils and/or adenoids, or otitis media shall be covered under the PremierChoice Specified Disease/Sickness Plan at fifty percent (50%) of any applicable benefit amount specified on the PremierChoice Specified Disease/Sickness Plan Schedule, provided that (i) such Specified Diseases/Sicknesses are not otherwise limited or excluded by the PremierChoice Specified Disease/Sickness Plan or any riders, endorsements, or amendments attached to the PremierChoice Specified Disease/Sickness Plan, and (ii) such Specified Disease/Sickness is not a Preexisting Condition.
PremierChoice Accident Plan Waiting Periods & Limitations
• Pre-existing Condition means a Bodily Injury for which medical advice, diagnosis, care or treatment was recommended or received during the twelve (12) month period immediately preceding the effective date of coverage under the PremierChoice Accident Plan for the Insured incurring the expense; or resulting from an Accident that occurred before the Issue Date for the Insured incurring the expense;
• The PremierChoice Accident Plan provides coverage as of the Issue Date for Pre-existing Conditions, disclosed on the application, provided they are not otherwise limited or excluded by the PremierChoice Accident Plan or any riders, amendments, or endorsements attached to the PremierChoice Accident Plan; and
• However, the PremierChoice Accident Plan does not cover expenses for Pre-existing Conditions that are not disclosed on the application, unless the expenses are incurred more than twelve (12) months after the Insured’s coverage has been in effect, and are not otherwise limited or excluded by the PremierChoice Accident Plan or any riders, amendments, or endorsements attached to the PremierChoice Accident Plan.
PremierChoice Non-WaiverExpenses that are mistakenly or erroneously paid by Us under any section or provision of the PremierChoice Specified Disease/Sickness Plan or PremierChoiceAccident Plan shall not constitute a waiver of or modification to any conditions, terms, definitions or limitations contained in the PremierChoice Specified Disease/Sickness Plan or PremierChoice Accident Plan, specifically including, but not by way of limitation, the definition of Specified Diseases/Sicknesses, Specified Disease/Sickness, Accidents, Accident, Medical Necessity or Covered Expenses, the limitation of coverage under the PremierChoice Specified Disease/Sickness Plan or PremierChoice Accident Plan for Pre-existing Conditions, as well as any exclusion, limitation and/or exclusionary riders which may be attached to the PremierChoice Specified Disease/Sickness Plan or PremierChoice Accident Plan, or otherwise operate to alter, amend, affect, abridge or modify the PremierChoiceSpecified Disease/Sickness Plan or PremierChoice Accident Plan to which it is attached.

• any cost item, charge or expense which does not constitute Covered Expenses;
• any Bodily Injuries suffered by an Insured; • any disease, ailment, illness or sickness that is not a Specified
Disease/Sickness; • any medical care, service, treatments, procedures, or supplies received,
provided to, or incurred by an Insured before the PremierChoiceSpecified Disease/Sickness Plan Issue Date;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured after an Insured’s coverage under the PremierChoice Specified Disease/Sickness Plan terminates, regardless of when the sickness or disease occurred;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which exceed the Lifetime Certificate Maximum Per Insured;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured and contained on a billing statement to the Insured which exceeds the amount of the Maximum Allowable Charge;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which You or Your covered family members are not required to pay;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members are not legally liable for payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members were once legally liable for payment, but from which liability the Insured and/or family members were forgiven and released by the applicable Provider without payment or promise of payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured from any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured as a result of experimental procedures or treatment methods not approved by the American Medical Association or other appropriate medical society;
• any eyeglasses, contact lenses, radial keratotomy, lasik surgery, hearing aids and exams for their prescription or fitting;
• any Cochlear implants; • any voluntary abortions, abortifacients or any other drug or device that
terminates a pregnancy;
PremierChoice Specified Disease/Sickness Plan Non-Covered ItemsCoverage under the PremierChoice Specified Disease/Sickness Plan is limited as provided by the definitions, terms, conditions, limitations, and exclusions contained in each and every section of the PremierChoice Specified Disease/Sickness Plan. In addition, the PremierChoice Specified Disease/Sickness Plan does not provide coverage for professional and medical services Provided to an Insured or any payment obligation for Us for any of the following, all of which are excluded from coverage:
• any medical condition excluded by name or specific description by either the PremierChoice Specified Disease/Sickness Plan or any riders, endorsements, or amendments attached to the plan;
• any cosmetic surgery or reconstructive procedures, except for Medically Necessary cosmetic surgery or reconstructive procedures performed under the following circumstances: (i) where such cosmetic surgery is incidental to or following surgery resulting from Bacterial Infection or Viral Infection, (ii) to correct a normal bodily function in connection with the treatment of a covered Specified Disease/Sickness, or a congenital defect that qualifies as a Specified Disease or (iii) such cosmetic surgery constitutes Breast Reconstruction that is incident to a Mastectomy; provided any of the above occurred while the Insured was covered under the PremierChoice Specified Disease/Sickness Plan;
• any treatment, care, procedures, services or supplies for breast reduction or augmentation or complications arising from these procedures;
• any treatment, care, procedures, services or supplies for voluntary sterilization, reversal or attempted reversal of a previous elective attempt to induce or facilitate sterilization;
• any treatment, care, procedures, services or supplies for treatment of infertility, including fertility hormone therapy and/or fertility devices for any type of fertility therapy, artificial insemination or any other direct conception;
• any treatment, care, procedures, services or supplies for any operation or treatment performed, Prescription or medication prescribed in connection with sex transformations or any type of sexual or erectile dysfunction, including complications arising from any such operation or treatment;
• any treatment, care, procedures, services or supplies for appetite suppressants, including but not limited to, anorectics or any other drugs used for the purpose of weight control, or services, treatments, or surgical procedures rendered or performed in connection with an overweight condition or a condition of obesity or related conditions;
• any treatment, care, procedures, services or supplies (including Prescription Drugs) incurred for the diagnosis, care or treatment of Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD);
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Mental, Nervous and Emotional Disorders;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of autism spectrum disorder;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Alcoholism, addiction to illegal drugs or substances, and/or abuse of illegal drugs or substances;

PremierChoice Specified Disease/Sickness Plan Non-Covered Items, cont’d
PremierChoice Accident Plan Non-Covered ItemsCoverage under the PremierChoice Accident Plan is limited as provided by the definitions, terms, conditions, limitations, and exclusions contained in each and every section of the PremierChoice Accident Plan. In addition, the PremierChoice Accident Plan does not provide coverage for professional and medical services Provided to an Insured or any payment obligation for Us for any of the following, all of which are excluded from coverage:
• any cost item, charge or expense which does not constitute Covered Expenses;
• any disease, ailment, illness or sickness suffered by an Insured, except a covered Bacterial Infection;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured before the PremierChoice Accident Plan Issue Date;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured after an Insured’s coverage under the PremierChoice Accident Plan terminates, regardless of when the Bodily Injury occurred;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which exceed the Lifetime Certificate Maximum Per Insured;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured and contained on a billing statement to the Insured which exceeds the amount of the Maximum Allowable Charge;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured, which You or Your covered family members are not required to pay;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members are not legally liable for payment;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured for which the Insured and/or any covered family members were once legally liable for payment, but from which liability the Insured and/or family members were forgiven and released by the applicable Provider without payment or promise of payment;
• any treatment care, procedures, services or supplies incurred for the diagnosis, care or treatment of cirrhosis of the liver;
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of routine maternity or any other expenses related to normal labor and delivery, including routine nursery charges and well-baby care;
• any fluoride products; • any intentional misuse or abuse of Prescription Drugs, including
Prescription Drugs purchased by an Insured for consumption by someone other than such Insured;
• any programs, treatment or procedures for tobacco use cessation; • any charges for blood, blood plasma, or derivatives that has been
replaced; • any treatment, care, procedures, services or supplies of
Temporomandibular Joint Disorder (TMJ) and Craniomandibular Disorder (CMD);
• any treatment received outside of the United States, except as provided for in the EXTRATERRITORIAL MEDICAL EXPENSES provision; and
• any services or supplies for personal convenience, including Custodial Care or homemaker services, except as provided for in the PremierChoiceSpecified Disease/Sickness Plan.
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured from any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services;
• any medical care, service, treatments, procedures, or supplies received, provided to, or incurred by an Insured as a result of experimental procedures or treatment methods not approved by the American Medical Association or other appropriate medical society;
• any eyeglasses, contact lenses, radial keratotomy, lasik surgery, hearing aids and exams for their prescription or fitting;
• any Cochlear implants; • any medical condition excluded by name or specific description by either
the PremierChoice Accident Plan or any riders, endorsements, or amendments attached to the plan;
• any cosmetic surgery or reconstructive procedures, except for Medically Necessary cosmetic surgery or reconstructive procedures performed under the following circumstances: (i) where such cosmetic surgery is incidental to or following surgery resulting from Bacterial Infection or (ii) to correct a normal bodily function in connection with the treatment of a covered Bodily Injury;
• any treatment, care, procedures, services or supplies for breast reduction or augmentation or complications arising from these procedures;
• any treatment, care, procedures, services or supplies for voluntary sterilization, reversal or attempted reversal of a previous elective attempt to induce or facilitate sterilization;
• any treatment, care, procedures, services or supplies for treatment of infertility, including fertility hormone therapy and/or fertility devices for any type of fertility therapy, artificial insemination or any other direct conception;

PremierChoice Accident Plan Non-Covered Items , cont’d
• any treatment, care, procedures, services or supplies for any operation or treatment performed, Prescription or medication prescribed in connection with sex transformations or any type of sexual or erectile dysfunction, including complications arising from any such operation or treatment;
• any treatment, care, procedures, services or supplies for appetite suppressants, including but not limited to, anorectics or any other drugs used for the purpose of weight control, or services, treatments, or surgical procedures rendered or performed in connection with an overweight condition or a condition of obesity or related conditions;
• any treatment, care, procedures, services or supplies (including Prescriptions) incurred for the diagnosis, care or treatment of Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD);
• any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Mental, Nervous and Emotional Disorders; • any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of autism; • any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of Alcoholism, addiction to illegal drugs or substances,
and/or abuse of illegal drugs or substances; • any treatment care, procedures, services or supplies incurred for the diagnosis, care or treatment of cirrhosis of the liver; • any treatment, care, procedures, services or supplies incurred for the diagnosis, care or treatment of routine maternity or any other expenses related to
normal labor and delivery, including routine nursery charges and well-baby care; • any fluoride products; • any intentional misuse or abuse of Prescription Drugs, including Prescription Drugs purchased by an Insured for consumption by someone other than
such Insured; • any programs, treatment or procedures for tobacco use cessation; • any charges for blood, blood plasma, or derivatives that has been replaced; • any treatment, care, procedures, services or supplies of Temporomandibular Joint Disorder (TMJ) and Craniomandibular Disorder (CMD); • any treatment received outside of the United States, except as provided for in the EXTRATERRITORIAL MEDICAL EXPENSES provision; and • any services or supplies for personal convenience, including Custodial Care or homemaker services, except as provided for in the PremierChoice Accident
Plan
vPremierChoice - ACA Individual Mandate & Shared Responsibility Payment
The individual mandate under the ACA generally requires individuals to have “minimum essential coverage” in 2014 and beyond, or be subject to payment of an annual “shared responsibility payment”, the amount of which is based, in part, upon the individual’s household income each year. The ACA’s “shared responsibility payment” has also been referred to from time to time as a tax and as a penalty, and is payable to the federal government. Specified Disease/Sickness and Accident Plans are exempt from the coverage and rating mandates of the ACA, and therefore are not considered “minimum essential coverage” under the ACA. If an individual (a) does not receive an ACA exemption annually from the federal government for the individual mandate, or (b) does not maintain “minimum essential coverage” under the ACA for 9 or more consecutive months during each year, (including coverage under one of the following types of plans (i) an employer sponsored group health plan, (ii) a grandfathered health plan, (iii) a non-grandfathered health plan for which the government has granted a waiver of the individual mandate, or (iv) an ACA essential health benefits plan), he will be subject to the ACA’s annual “shared responsibility payment”, even if covered under one of the PremierChoice Specified Disease/Sickness or Accident Plans. For additional information on the individual mandate, “shared responsibility payment”, exemptions from the mandate and other matters concerning the ACA, please visit www.healthcare.gov, the federal government’s website.
PremierChoice - Premium Rate AdjustmentsWe will not raise Your premium rates on an individual basis due to Your personal claims experience on either plan. We may raise Your premium rates on Your Renewal Premium Class for all Certificates in Your state on both plans. Renewal Premiums are calculated based on a variety of factors, some of which are each plan of coverage, age, sex, place of residence, number of dependents, past claims experience of Your Renewal Premium Class, and other reasons permitted by state law. Rates for individuals of the same sex and age may vary by Issue Date. Insureds are always free to request and apply for new underwritten coverage on this or other available plans.
PremierChoice - Renewability and TerminationCoverage under each plan is guaranteed renewable to age 65 or in the event You become a Medicare enrollee.Your coverage will end on the earlier of the following: the premium due date in the month following the date the applicable Group Insurance Policy is terminated by the Group Policyholder; with respect to Your Spouse who is covered, the premium due date in the month following the effective date of Your divorce decree or annulment; with respect to Your children who are covered, the premium due date in the month following Your child reaching the limiting age as defined by Your state; the due date of any unpaid premium (subject to the grace period); the date You terminate coverage by notifying Us; We are required by an appropriate regulatory authority to non-renew or cancel the group policy; We cease offering and renewing the same form of coverage as the Certificate in Your state; the date We receive due proof that fraud or intentional misrepresentation of material fact existed in applying for coverage or filing a claim; the Primary Insured terminated membership in the association which is the Group Policyholder; the month following attainment of age 65 for You or Your Spouse or in the event You or YourSpouse, are eligible for Medicare; or the total amount of any benefit payments made by Us are equal to the lifetime maximum.

MedGuard Limitations at a Glance
• For each Insured, Benefits payable under the Group Policy and Certificate for all Specified Critical Illness Events or Specified Critical Illness Surgery combined will not exceed the Total Benefit Amount that applies to the Insured. We will reduce what We pay for a claim so that the amount that We pay, when combined with amounts for all claims We have previously paid for the same Insured does not exceed the Total Benefit Amount that was in effect for that Insured on the date of the most recent Specified Critical Illness Event or Specified Critical Illness Surgery.
• We will pay the Benefits for any Specified Critical Illness Event or Specified Critical Illness Surgery that First Occurs after the first 30 days immediately following the Issue Date, or as a result of diagnostic testing performed after the first 30 days immediately following the Issue Date, except for the limited Benefit amount shown in the Certificate Schedule for the 1st through 30th day for any Specified Critical Illness Event or Specified Critical Illness Surgery other than Life Threatening Cancer. Life Threatening Cancer will be limited to the amount shown on the Certificate Schedule during the first 90 days immediately following the Issue Date.
MedGuard Non-Covered Items at a Glance
No Benefits shall be payable under the Group Policy or Certificate for any loss caused by, in whole or in part, contributed to or resultingfrom, directly or indirectly, any of the following incidents, events, occurrences or activities involving any Insured for:• participating in a felony, riot or insurrection; • intentionally causing a self-inflicted injury; • committing or attempting to commit suicide while sane or insane, within two (2) years from the Insured’s Issue Date; • engaging in any illegal activity; • serving in the armed forces or an auxiliary unit of the armed forces of any country; • war or any act of war, even if war is not declared, during military service; • a diagnosis which is made outside the United States, unless a Definitive Diagnosis of a Specified Critical Illness Event or a Specified Critical Illness
Surgery is confirmed in the United States; • an Insured being intoxicated or under the influence of alcohol or any drug, narcotic or hallucinogens unless administered via a prescription and on
the advice of a Doctor and taken in accordance with the limits of such advice. An Insured is conclusively determined to be intoxicated by drug or alcohol if (i) a chemical test administered in the jurisdiction where the loss or cause of loss occurred is at or above the legal limit set by that jurisdiction or (ii) the level of alcohol was such that a person’s coordination, ability to reason, was impaired, regardless of the legal limit set by that jurisdiction;
• with respect to Critical Illness-Accelerated Death Benefit Payment section V.B. of the Certificate, any Specified Critical Illness Event or Specified Critical Illness Surgery suffered, diagnosed and/or sustained by an Insured prior to the Issue Date; and
• with respect to Critical Illness-Accelerated Death Benefit Payment section V.B. of the Certificate, any medical condition that is not a Specified Critical Illness Event or Specified Critical Illness Surgery.

MedGuard - ACA Individual Mandate & Shared Responsibility PaymentThe individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or be subject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year. The MedGuard Plan is a life insurance plan with an accelerated death benefit rider, which pays the designated percentage of the Plan’s death benefit to the Insured upon the diagnosis of a covered critical condition or receipt of a covered critical surgery, as such it is not “health insurance coverage” under the ACA, Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered “minimum essential coverage” under the ACA. Therefore, unless an Insured under the MedGuard Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment.
No Benefits are payable for any loss caused by:• Injury due to any act of war (whether declared or undeclared);• services provided by any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services,
except Medicaid;• intentionally self-inflicted Injury;• suicide or any suicide attempt while sane or insane;• serving in one of the branches of the armed forces of any foreign country or any international authority;• services provided by You or a Provider who is a member of an Insured’s Family;• an Injury occurring outside the borders of the United States of America or its territories;• any loss to which a contributing cause was the Insured’s being engaged in an illegal occupation or attempting to commit assault or illegal activity;• participation in hang gliding, paragliding, hot air ballooning or any other form of aviation, except as a fare-paying passenger traveling on a regularly
scheduled commercial airline flight;• participating, as driver or passenger, in any competition, race or speed contest, including sanctioned practice thereof, of any land or water vehicle;• Mental and Emotional Disorders;• for the purposes of the Emergency Air Ambulance Benefit, the Insured’s medical condition was not sufficiently acute or severe upon arrival at the Hospital
to result in an Inpatient admission and Confinement in the Hospital immediately following the Insured’s evaluation and treatment in the emergency room of such Hospital;
• an Insured being intoxicated or under the influence of alcohol or any drug, narcotic or hallucinogens unless administered via a prescription and on the advice of a Provider, and taken in accordance with the limits of such advice. An Insured is conclusively determined to be intoxicated by drug or alcohol if: (i) a chemical test administered in the jurisdiction where either the Accident occurred or the Insured was medically treated is at or above the legal limit set by that jurisdiction; or (ii) the level of alcohol was such that a person’s coordination and/or ability to reason was impaired, regardless of the legal limit set by that jurisdiction;
• Sickness;• expenses incurred for the diagnosis, care or treatment of Mental and Emotional Disorders, alcoholism, or drug addiction/abuse; • the unintended or accidental results of any procedure, surgery or operation performed either for cosmetic purpose or in an attempt to surgically treat any
Sickness, or any elective procedure not Medically Necessary, including but not limited to organ donation and elective sterilization; • intentional inhalation or ingestion of any poison, gas or fumes; • services that are not Medically Necessary; • expenses incurred as the result of an Injury that are in excess of the Usual and Customary expenses incurred for Medically Necessary treatment of such
Injury;
Accident Protector - Non-Covered Items at a Glance

• participating, as driver or passenger, in any competition, race or speed contest, including sanctioned practice thereof, of any land or water vehicle;
• Mental and Emotional Disorders;• for the purposes of the Emergency Air Ambulance Benefit the Insured’s medical condition
was not sufficiently acute or severe upon arrival at the Hospital to result in an Inpatient admission and Confinement in the Hospital immediately following the Insured’s evaluation and treatment in the emergency room of such Hospital;
• an Insured being intoxicated or under the influence of alcohol or any drug, narcotic or hallucinogens unless administered via a prescription and on the advice of a Provider, and taken in accordance with the limits of such advice. An Insured is conclusively determined to be intoxicated by drug or alcohol if: () a chemical test administered in the jurisdiction where either the Accident occurred or the Insured was medically treated is at or above the legal limit set by that jurisdiction; or (ii) the level of alcohol was such that a person’s In addition to any other provisions of the Certificate, Benefits and coverage are limited as follows: • The amount of the Calendar Year Maximum Dental Benefit Per Insured shall not exceed the sum of $500 for the Saver Plan, $1,000 for the Saver Plus Plan, and $1,500 for the Premium Plan, with an additional $400 Calendar Year Maximum Orthodontic Benefit per Insured and Lifetime Maximum Orthodontic Benefit Per Insured of $1,000 on the Premium Plan. • No Benefits are payable under the BASIC DENTAL CARE provision unless they are incurred at least six (6) months after the Issue Date. • No Benefits are payable under the MAJOR DENTAL CARE provision unless they are incurred at least twelve (12) months after the Issue Date. • No Benefits are payable under the ORTHODONTIC DENTAL EXPENSES provision unless they are incurred at least twelve (12) months after the Issue cosmetic purpose, gas or fumes; and
• services that are not Medically Necessary.
Accident Protector - ACA Individual Mandate & Shared Responsibility Payment
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond,or be subject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s householdincome each year. The Accident Protector Plan is an excess medical expense coverage insurance plan which provides coverage for the remaining amount of medical expenses incurred per Insured per covered accident, as such it is not “health insurance coverage” under the ACA, Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered “minimum essential coverage” under the ACA. Therefore, unless an Insured under the Accident Protector Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment.
SecureDental – Limitations at a GlancePremium, Saver Plus & Saver Plans LimitationsIn addition to any other provisions of the Certificate, Benefits and coverage are limited as follows:• The amount of the Calendar Year Maximum Dental Benefit Per Insured shall not exceed the sum of $500 for the Saver Plan, $1,000 for the Saver Plus Plan,
and $1,500 for the Premium Plan, with an additional $400 Calendar Year Maximum Orthodontic Benefit per Insured and Lifetime Maximum Orthodontic Benefit Per Insured of $1,000 on the Premium Plan.
• No Benefits are payable under the BASIC DENTAL CARE provision unless they are incurred at least six (6) months after the Issue Date. • No Benefits are payable under the MAJOR DENTAL CARE provision unless they are incurred at least twelve (12) months after the Issue Date. • No Benefits are payable under the ORTHODONTIC DENTAL EXPENSES provision unless they are incurred at least twelve (12) months after the Issue Date.
• expenses incurred for the Medically Necessary treatment of an Injury for which the Insured has no legal liability and responsibility for payment; • expenses incurred for the Medically Necessary treatment of an Injury that are covered under any other valid insurance coverage, accident medical
expense benefits or health benefit plan coverage (e.g. uninsured/underinsured motorist coverage, personal injury protection coverage under any automobile policy, comprehensive major medical insurance, hospital/medical surgical insurance, other indemnity health insurance, health coverage under an HMO or PPO plan, workers’ compensation medical expense benefits, FELA medical expense benefits, Jones Act medical expense benefits, Medicaid and Medicare;
• the operation by an Insured of any motor vehicle without the permission/consent of the owner of such vehicle; • the operation by an Insured of any motor vehicle without a valid operator’s license/permit;• bacterial or viral infection, except such infection occurring with or through a cut or wound in the skin sustained in an Accident or the accidental ingestion
of contaminated material; • participation in a riot, civil commotion or insurrection;• actively serving in the armed forces, including the National Guard and Army Reserve;• Injury from being arrested or incarcerated or caused while incarcerated in a penal institution or government detention facility;• engaging in bungee jumping, parachuting, rock climbing, para-sailing, para-kiting, mountaineering, or as driver or passenger on an off-road ATV vehicle, or
any other hazardous avocation; • Injuries from raising, caring for, handling or working with dangerous animals; and• participation in rodeo or equestrian events, semi-professional or professional sports or any other hazardous activity for wage, compensation profit.
Accident Protector - Non-Covered Items at a Glance, cont’d

SecureDental - Non-Covered Items at a GlancePremium, Saver Plus and Saver Plans Non-Covered ItemsCoverage under the Certificate is limited as provided by the definitions, terms, conditions, limitations, and exclusions contained in each and every section of the Certificate. In addition, the Certificate does not provide coverage for professional and dental services Provided to an Insured or any payment obligation for Us under the Certificate for any of the following, all of which are excluded from coverage:
• treatments, care, procedures, services or supplies received before the Certificate Issue Date;
• covered Dental Expenses that exceed the amount of the Calendar Year Maximum Dental Benefit Per Insured;
• Prescription Drugs; • any professional services for which the Insured and/or any covered family
member are not legally liable for payment; • any professional services for which the Insured and/or any covered family
member were once legally liable for payment, but from which liability the Insured and/or family member were released;
• Dental Injury or Dental Sickness due to any act of war (whether declared or undeclared);
• services provided by any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services;
• any dental conditions for which the covered Insured has received or is entitled to receive compensation for that particular dental condition under any Worker’s Compensation or Occupational Disease Law;
• expenses incurred for oral hygiene instructions, a plaque control program or dietary instructions;
• expenses incurred for dental care which is not customarily performed, which is experimental in nature or which is not considered acceptable by the American Dental Association or Federal Drug Administration;
• any professional and dental services provided an Insured in treatment of a Dental Sickness or Dental Injury caused or contributed to by such Insured’s being intoxicated or under the influence of any drug, narcotic or hallucinogens unless administered on the advice of a provider, and taken in accordance with the limits of such advice;
• intentionally self-inflicted Dental Injury, suicide or any suicide attempt while sane or insane;
• Dental Sickness or Dental Injury while serving in one of the branches of the armed forces of the United States of America:
• Dental Sickness or Dental Injury while in a foreign country and serving on active duty in the United States Army, Navy, Marine Corp or Air Force Reserves or the National Guard;
• Dental Sickness or Dental Injury while serving on active duty in the armed forces of any foreign country or any international authority;
• any dental condition excluded by name or specific description by either the Certificate or any riders, endorsements, or amendments attached to the Certificate;
• any loss to which a contributing cause was the Insured’s being engaged in an illegal occupation or illegal activity;
• participation in aviation, except as fare-paying passenger traveling on a regular scheduled commercial airline flight;
• cosmetic surgery or cosmetic dentistry, except for Dentally Necessary cosmetic surgery which is incidental to or following surgery resulting from trauma or infection to correct a normal bodily function;
• Temporomandibular Joint Disorder (TMJ) and Craniomandibular Disorder (CMD);
• treatment received outside of the United States; • treatment on or to the teeth or gums for cosmetic purposes, including
charges for personalizations, characterizations or Dentures; • replacement of lost or stolen prosthetics; • restorative services (i.e. the initial placement of a complete or Partial
Denture or for Fixed Bridgework) or Endodontic therapy if it involves the replacement of one or more natural teeth missing on the Issue Date of the Certificate or when initial preparations were started prior to the Issue Date as shown on the Certificate Schedule;
• restorative services for one (1) or more natural teeth missing on the Issue Date as shown on the Certificate Schedule of the Certificate will be considered Covered Dental Service if incurred five (5) years after the Issue Date;
• dental services performed in a hospital and any related expenses; • replacement of an appliance or prosthetic device, Crown, cast restoration
or a Fixed Bridge within five (5) years after the date it was last placed. This exclusion does not apply if replacement is due to accidental Dental Injury received while covered under the Certificate;
• treatment of cleft palate, except for a newborn child covered under the Certificate from birth, andontia or mandibular prognathicism;

SecureDental - Non-Covered Items at a GlancePremium, Saver Plus and Saver Plans Non-Covered Items, cont’d
• general anesthesia, except as specifically provided in the COVERED DENTAL EXPENSES section; • placement of bone grafts or extra-oral substances in the treatment of periodontal disorders; • the use of unilateral, removable prosthetics; • charges incurred by an Insured due to broken or cancelled appointments; • Crowns for teeth that are restorable by other means or for the purpose of periodontal splinting;• Crowns, fillings or appliances that are used to correct (splint) teeth, or change or alter the way the teeth meet, including altering the vertical dimension,
restoring the bite (occlusion) or for cosmetic purposes; • orthognathic surgery; and • expenses which exceed 100% of those actually incurred by the covered Insured.
SecureDental - Non-Covered Items at a GlanceAdditional Premium Plan Non-Covered Items
• any expenses for treatments, care, procedures, services or supplies which are not Covered Dental Expenses or Covered Orthodontic Expenses incurred by a covered Insured, and which are not specifically enumerated in the COVERED DENTAL EXPENSES or COVERED ORTHODONTIC EXPENSES section of the Certificate;
• Covered Dental Expenses or Covered Orthodontic Expenses received after the Certificate terminates, regardless of when the condition originated; • Covered Orthodontic Expenses that exceed the amount of the Calendar Year Maximum Orthodontic Benefit per Insured; • any treatments, care, procedures, services or supplies which are not specifically enumerated in the COVERED DENTAL EXPENSES or COVERED
ORTHODONTIC EXPENSES sections of the Certificate and any optional coverage rider attached to the Certificate; and • Orthodontic diagnosis or treatment, except as provided in the COVERED ORTHODONTIC EXPENSES provision.
SecureDental - Non-Covered Items at a GlanceAdditional Saver Plus & Saver Plans Non-Covered Items
• any expenses for treatments, care, procedures, services or supplies which are not Covered Dental Expenses incurred by a covered Insured, and which are not specifically enumerated in the COVERED DENTAL EXPENSES section of the Certificate;
• Covered Dental Expenses received after the Certificate terminates, regardless of when the condition originated; • any treatments, care, procedures, services or supplies which are not specifically enumerated in the COVERED DENTAL EXPENSES sections of the Certificate
and any optional coverage rider attached to the Certificate; and • Orthodontic diagnosis or treatment.
SecureDental - Non-Covered Items at a GlanceAdditional Saver Plan Non-Covered Items
• Implants, including any appliances and/or Crowns and the surgical insertion or removal of Implants.

v
vt
• Injury due to any act of war (whether declared or undeclared); • intentionally self-inflicted Injury; • suicide or any suicide attempt while sane or insane; • serving in one of the branches of the armed forces of any foreign
country or any international authority; • an Injury occurring outside the borders of the United States of America
or its territories except as provided in the Foreign Travel Benefit provision of the Certificate;
• any Injury while engaging, committing, or attempting to commit a felony or illegal occupation or while being arrested or incarcerated;
• participation in hang gliding, paragliding, hot air ballooning or any other form of aviation, except as a fare-paying passenger traveling on a regularly scheduled commercial airline flight;
• participating, as driver or passenger, in any competition, race or speed contest, including sanctioned practice thereof, of any land or water vehicle;
• engaging in bungee jumping, parachuting, rock climbing, parasailing, parakiting, surfing, mountaineering, skateboarding, or any other hazardous avocation;
• participation in rodeo or equestrian events, semi-professional or professional sports or any other hazardous activity for wage, compensation, or profit;
• participating in intercollegiate sports or club sports activities; • Injuries from raising, caring, handling or working with dangerous
animals; • Mental and Emotional Disorders;
• an Insured being intoxicated or under the influence of alcohol or any drug, narcotic or hallucinogens unless administered via a prescription and on the advice of a Provider, and taken in accordance with the limits of such advice. An Insured is conclusively determined to be intoxicated by drug or alcohol if: (i) a chemical test administered in the jurisdiction where either the Accident occurred or the Insured was medically treated is at or above the legal limit set by that jurisdiction; or (ii) the level of alcohol or drug was such that a person’s coordination and/or ability to reason was impaired, regardless of the legal limit set by that jurisdiction;
• sickness; • the unintended or accidental results of any surgery or operation
performed either for cosmetic purposes or in an attempt to surgically treat any sickness;
• the unintended or accidental result of any procedure, surgery or operation performed for cosmetic purpose or in an attempt to surgically treat any sickness, or any elective procedures not medically necessary, including but not limited to organ donation and elective sterilization;
• intentional inhalation or ingestion of any poison, gas or fumes; • the operation by an Insured of any motor vehicle without the
permission/consent of the owner of such vehicle; • the operation by an Insured of any motor vehicle without a valid
operator’s license/permit; • bacterial or viral infection, except such infection occurring with or through
a cut or wound in the skin sustained in an Accident or the accidental ingestion of contaminated material;
• participating as a driver or passenger on a motorcycle, or an off-road or ATV vehicle;
• actively serving in any armed forces, including National Guard or Army Reserves; and
• Injuries from being arrested or incarcerated or caused while incarcerated in penal institution or government detention facility.
SecureDental - ACA Individual Mandate & Shared Responsibility Payment
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond,or be subject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year. The SecureDental Plan provides benefits for dental only coverage, but it is not Workers Compensation coverage under state law or an “essential health benefits” under the ACA and it is not considered “minimum essential coverage” plan under the ACA. Therefore, unless an Insured under the SecureDental Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment.
IncomeProtector - Non-Covered Expenses at a GlanceNo Benefits shall be payable under the Certificate for any loss caused by, in whole or in part, contributed to or resulting from, directly or indirectly, any ofthe following incidents, events, occurrences or activities involving any Insured:

IncomeProtector - ACA Individual Mandate & Shared Responsibility Payment
The individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or besubject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year. The IncomeProtector Plan is a short term accident disability income insurance plan which pays monthly benefits to the Insured upon totally disability due to a covered accident while the Insured is actively employed, as such it is not “health insurance coverage” under the ACA, Workers Compensation coverage under state law, an “essential health benefits” under the ACA or considered “minimum essential coverage” under the ACA. Therefore, unless an Insured under the IncomeProtector Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the Insured will be subject to the ACA’s shared responsibility payment.
PremierVision - Limitations at a Glance - Insurance BenefitsCoverage under the PremierVision Plan is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every Section of thePremierVision Plan, as well as the following limitations:• in no event will coverage exceed the lesser of: (i) the actual cost of Covered Vision Expenses or materials, (ii) the negotiated fee for services rendered by a
Participating Provider, or (iii) the Allowance as shown on the PremierVision Plan Schedule when services are rendered by a Participating Provider or a Non-Participating Provider;
• if the Participating Provider’s or Non-Participating Provider’s charge is less than the Allowance specified on the PremierVision Plan Schedule, We will only pay up to the Participating Provider’s or Non-Participating Provider’s charge; and
• materials covered by the PremierVision Plan that are lost or stolen will only be replaced at the intervals stated on the PremierVision Plan Schedule.
PremierVision - Non-Covered Items at a Glance - Insurance BenefitsCoverage under the PremierVision Plan is limited as provided by the definitions, terms, conditions, limitations, and exclusions contained in each and everysection of the PremierVision Plan. In addition, the PremierVision Plan does not provide coverage for professional and vision services Provided to an Insuredor any payment obligation for Us under the PremierVision Plan for any of the following, all of which are excluded from coverage:
• orthoptic or vision training and any associated supplemental testing; • plano lenses; • lens coating; • two pair of glasses, in lieu of bifocals or trifocals; • medical or surgical treatment of the eyes; • any type of corrective vision surgery, including LASIK surgery; • any eye examination, or any corrective eyewear, required by an employer
as a condition of employment; • any services or supplies when paid under any Worker’s Compensation or
similar law; • Tier 4 Premium Progressive Lenses; • photochromic transition or polycarbonate lenses; • lenticular lenses; • sub-normal vision aids or non-prescription lenses; • service rendered or supplies purchased outside the U.S. or Canada, unless
the Insured resides in the U.S. or Canada and the charges are incurred while on a business or pleasure trip;
• eyeglasses when the change in prescription is less than .5 Diopter; • experimental or investigational or non-conventional treatment or device; • eyeglass lens treatments, including “add-ons”, UV coating, anti-reflective
coating, scratch resistant coating, tinting or edge polishing;
• oversized lenses; • lost or broken lenses, Frames, glasses, or contact lenses will not be
replaced until twelve (12) months after the last date of service; • medically necessary Contact Lenses; • high index lenses of any material type; • fitting for Corrective Contact Lenses; • follow-up visits; • charges incurred after the PremierVision Plan has terminated or coverage
has ended; • any expenses for treatments, care, procedures, services or supplies which
are not Covered Vision Expenses incurred by an Insured and which are not specifically enumerated in the VISION EXPENSE BENEFITS AND CLAIM PROCEDURES section of the PremierVision Plan;
• treatments, care, procedures or supplies received before the PremierVision Plan Issue Date;
• any professional services for which the Insured and/or any covered family member are not legally liable for payment;
• any professional services for which the Insured and/or any covered family member were once legally liable for payment, but from which liability the Insured and/or family member were released;

PremierVision - Non-Covered Items at a Glance, cont’d - Insurance Benefits• services provided by any state or federal government agency, including the Veterans Administration unless, by law, an Insured must pay for such services; • charges that are payable or reimbursable by either: a) a plan or program of any governmental agency (except Medicaid); or b) Medicare Part A, Part B
and/or Part D (If the applicable Insured does not enroll in Medicare, We will estimate the charges that would have been paid if such enrollment had occurred);
• cosmetic items; • broken appointment fees; • refitting or change in lens design after the initial fitting; and • expenses which exceed 100% of those actually incurred by the Insured
PremierVision - ACA Individual Mandate & Shared Responsibility PaymentThe individual mandate of the Affordable Care Act (“ACA”) generally requires individuals to maintain “minimum essential coverage” in 2014 and beyond, or be subject to the payment of the annual shared responsibility payment, the amount of which is based, in part, upon the individual’s household income each year The PremierVision Plan provides benefits for vision only coverage, but it is not Workers Compensation coverage under state law or an “essential health benefits” under the ACA and it is not considered “minimum essential coverage” plan under the ACA. Therefore, unless an insured under the PremierVision Plan has an exemption from the ACA’s individual mandate or maintains “minimum essential coverage” under the ACA, the insured will be subject to the ACA’s shared responsibility payment. For additional information on the individual mandate, “shared responsibility payment”, exemptions from the mandate and other matters concerning the ACA, please visit www.healthcare.gov, the federal government’s website
LifeProtector- Suicide
If the Insured dies by suicide while sane or insane, within two (2) years of the Issue Date of the Policy, the Death Benefits payable will be limited to an amount equal to premiums paid.
PremierMed - ACA Individual Mandate & Shared Responsibility Payment
The individual mandate under the ACA generally requires individuals to have “minimum essential coverage” in 2014 and beyond, or be subject to payment of an annual “shared responsibility payment”, the amount of which is based, in part, upon the individual’s household income each year. The ACA’s “shared responsibility payment” has also been referred to from time to time as a tax and as a penalty, and is payable to the federal government. Short term medical plans are exempt from the coverage and rating mandates of the ACA, and therefore are not considered “minimum essential coverage” under the ACA. If an individual (a) does not receive an ACA exemption annually from the federal government for the individual mandate, or (b) does not maintain “minimum essential coverage” under the ACA for 9 or more consecutive months during each year, (including coverage under one of the following types of plans (i) an employer sponsored group health plan, (ii) a grandfathered health plan, (iii) a non-grandfathered health plan for which the government has granted a waiver of the individual mandate, or (iv) an ACA essential health benefits plan), he will be subject to the ACA’s annual “shared responsibility payment”, even if covered under the PremierMed Short Term Medical-Surgical Expense Plan. For additional information on the individual mandate, “shared responsibility payment”, exemptions from the mandate and other matters concerning the ACA, please visit www.healthcare.gov, the federal government’s website.

coverage:
Coverage under the PremierMed Short Term Medical-Surgical Expense Plan is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every section of the PremierMed Short Term Medical-Surgical Expense Plan, as well as the following limitations and waiting periods:• Any loss or expense incurred as a result of an Insured’s Pre-existing Condition is not covered under the PremierMed Short Term Medical-Surgical Expense
Plan;1
• If, as the result of an Emergency Sickness or an Emergency Bodily Injury, services are rendered for an Insured by a Non-Participating Provider when a Participating Provider was not reasonably available in connection with either (i) on an Outpatient basis in the emergency room of a Hospital or (ii) an Emergency Inpatient admission to a Hospital, then the Covered Expenses incurred will be reimbursed by Us as if such Non-Participating Provider were a Participating Provider, up to the point when the Insured can be safely transferred to a Participating Provider. If the Insured refuses or is unwilling to be transferred to the care of a Participating Provider after such Insured can be safely transferred, then reimbursement shall thereafter be reduced to the Company’s Insurance Percentage for Non-Participating Providers;
• Insureds have the right to obtain Prescriptions from the pharmacy of their choice. However, if an Insured: (i) uses a Non-Participating Pharmacy to fill a Prescription or (ii) does not present his/her correct ID card when the Prescription is filled at a Participating Pharmacy, then such Insured must pay the applicable pharmacy in full and file a claim form with the Company for reimbursement. In either event, the Insured will be reimbursed by the Company at the discounted or negotiated rate for such Prescription that would have been paid to a Participating Pharmacy by the Company under the PremierMed Short Term Medical-Surgical Expense Plan if the Insured had used a Participating Pharmacy and properly presented the correct ID card at the time the Prescription was filled; and
• Because the Benefit Deductible under the PremierMed Short Term Medical-Surgical Expense Plan is calculated on the basis of Covered Expenses, it is possible that every dollar an Insured pays for Prescription Drugs at a Participating Pharmacy may not apply toward meeting the applicable Benefit Deductible.
PremierMed– Limitations At A Glance
1Pre-existing Conditions that Manifested after the effective date of coverage under the PremierChoice Specified Disease/Sickness and Accident are waived when the PremierMed Short Term Medical-Surgical Expense Plan is purchased via the MIGI Rider (SMIGIST-2015-R-TX-FLIC)
PremierMed - Non-Covered Items At A GlanceCoverage under the PremierMed Short Term Medical-Surgical Expense Plan is limited as provided by the definitions, limitations, exclusions, and terms contained in each and every section of the PremierMed Short Term Medical-Surgical Expense Plan. In addition, the PremierMed Short Term Medical-Surgical Expense Plan does not provide coverage for expenses charged to an Insured or any payment obligation for Us under the PremierMed Short Term Medical-Surgical Expense Plan for any of the following, all of which are excluded from coverage:
• the amount of any professional fees or other medical expenses or charges for treatments, care, procedures, services or supplies which do not constitute Covered Expenses;
• Covered Expenses incurred before the PremierMed Short Term Medical-Surgical Expense Plan Issue Date;
• Covered Expenses incurred after the expiration of the Schedule Termination Date, regardless of when the condition originated; except as Provided in the EXTENSION OF BENEFITS provision;
• Covered Expenses that are not incurred while coverage under the PremierMed Short Term Medical-Surgical Expense Plan is in full force and effect for the applicable Insured that incurred such expenses;
• any professional fees or other medical expenses incurred for the diagnosis, care or treatment of Mental and Emotional Disorders and Substance Abuse, except as specifically enumerated in the SICKNESS AND BODILY INJURY BENEFITS section of the PremierMed Short Term Medical-Surgical Expense Plan;
• the amount of any professional fees or other medical expenses contained on a billing statement to an Insured which exceed the amount of the Maximum Allowable Charge;
• any professional fees or other medical expenses for treatments, care, procedures, services or supplies which are not specifically enumerated in the SICKNESS AND BODILY INJURY BENEFITS or WELLNESS AND SCREENING BENEFITS sections of the PremierMed Short Term Medical-Surgical Expense Plan and any optional coverage rider attached to the PremierMed Short Term Medical-Surgical Expense Plan;

• Covered Expenses You or Your covered family members are not required to pay, which are covered by other insurance, or that would not have been billed if no insurance existed;
• any professional fees or expenses for which the Insured and/or any covered family member are not legally liable for payment;
• any professional fees or expenses for which the Insured and/or any covered family member were once legally liable for payment, but from which liability the Insured and/or family member were released;
• treatment of the teeth, the surrounding tissue or structure, including the gums and tooth sockets of adult Insureds. This exclusion does not apply to treatment: (a) due to Dental Injury to natural teeth (treatment must be Provided within ninety (90) days of the date of the Dental Injury) or (b) for malignant tumors;
• Bodily Injury or Sickness due to any act of war (whether declared or undeclared) or participation in an act of terrorism;
• services provided by any state or federal government agency, including the Veterans Administration, unless, by law, an Insured must pay for such services;
• Covered Expenses that are payable under any motor vehicle no fault law insurance policy or certificate;
• drugs or medication not used for a Food and Drug Administration (FDA) approved use or indication;
• any Bodily Injury or Sickness covered by any Workers’ Compensation insurance coverage, or similar coverage underwritten in connection with any Occupational Disease Law, or Employer’s Liability Law, regardless of whether You file a claim for benefits thereunder;
• administration of experimental drugs or substances, or investigational use or experimental use of Prescription Drugs, except for any Prescription Drug prescribed to treat a covered chronic, disabling, life-threatening Sickness or Bodily Injury, but only if the investigational or experimental drug in question: a) has been approved by the FDA for at least one indication; and b) is recognized for treatment of the indication for which the drug is prescribed in: 1) a standard drug reference compendia; 2) substantially accepted peer-reviewed medical literature; or 3) drugs labeled “Caution –limited by Federal law to investigational use”. c) experimental procedures or treatment methods not approved by the American Medical Association or other appropriate medical society;
• eyeglasses, contact lenses, radial keratotomy, lasik surgery, hearing aids and exams for their prescription or fitting;
• cochlear implants;
PremierMed - Non-Covered Items At A Glance, Cont’d
• any professional fees or other medical expenses incurred by an Insured which were caused or contributed to by such Insured’s being intoxicated or under the influence of any drug, narcotic or hallucinogens unless administered on the advice of a Provider, and taken in accordance with the limits of such advice;
• intentionally self-inflicted Bodily Injury, suicide, or any suicide attempt, while sane or insane;
• serving in one of the branches of the armed forces of the United States or of any foreign country or any international authority;
• voluntary abortions, abortifacients or any other drug or device that terminates a pregnancy;
• any medical condition excluded by name or specific description by either the PremierMed Short Term Medical-Surgical Expense Plan or any riders, endorsements, or amendments attached to the PremierMed Short Term Medical-Surgical Expense Plan;
• any loss to which a contributing cause was the Insured’s being engaged in or attempting to engage in an illegal occupation or illegal activity;
• participation in aviation, except as fare-paying passenger traveling on a regular scheduled commercial airline flight;
• any Bodily Injury caused or contributed to while racing a land or water vehicle, or participation in hazardous avocation including, but not limited to, martial arts, boxing, hang gliding, paragliding, sky diving, hot air ballooning, mountain/cliff climbing, organized competitive sports, ATV riding, or snowmobiling;
• cosmetic surgery or reconstructive procedures, except for Medically Necessary cosmetic surgery or reconstructive procedures performed under the following circumstances: (i) where such cosmetic surgery is incidental to or following surgery resulting from trauma or infection, (ii) to correct a normal bodily function or congenital defect, or (iii) such cosmetic surgery constitutes Breast Reconstruction that is incident to a Mastectomy, provided any of the above occurred while the Insured was covered under the PremierMed Short Term Medical-Surgical Expense Plan and while coverage under the PremierMed Short Term Medical-Surgical Expense Plan is in full force and effect;
• charges for breast reduction or augmentation or complications arising from these procedures;
• Prescription Drugs or other medicines and products used for cosmetic purposes or indications;
• fertility hormone therapy and/or fertility devices for any type of fertility therapy, artificial insemination or any other direct conception;

• voluntary sterilization, reversal or attempted reversal of a previous elective attempt to induce or facilitate sterilization; • any operation or treatment performed, Prescription or medication prescribed in connection with sex transformations, or any type of sexual or erectile
dysfunction, including complications arising from any such operation or treatment;• appetite suppressants, including but not limited to, anorectics or any other drugs used for the purpose of weight control, or services, treatments, or surgical
procedures rendered or performed in connection with an overweight condition or a condition of obesity or related conditions; • Prescriptions, treatment or services for behavioral or learning disorders, Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD);• Prescription Drugs that are immunosuppressants; • any professional fees or other medical expenses incurred as the result of a Bodily Injury which was caused or contributed by an Insured racing any air, land or
water vehicle; • drugs prescribed for the treatment of any disease, illness or condition that has been excluded from coverage by exclusionary rider, limitation or exclusion; • Prescription Drugs that are classified as psychotherapeutic drugs, including antidepressants; • Outpatient Prescription Drugs that are dispensed by a Provider, Hospital or other state-licensed facility; • Prescription Drugs produced from blood, blood plasma and blood products, derivatives, Hemofil M, Factor VIII, and synthetic blood products, or
immunization agents, biological or allergy sera, hematinics, blood or blood products administered on an Outpatient basis; • level one controlled substances; • Prescription Drugs used to treat or cure hair loss or baldness; • Prescription Drugs that are classified as anabolic steroids or growth hormones except as Provided in the Benefit;• compounded Prescription Drugs; • fluoride products; • allergy kits intended for future emergency treatment of possible future allergic reactions; • replacement of a prior filled prescription for Prescription Drugs that was covered and is replaced because the original prescription was lost, stolen or
damaged; • Prescription Drugs, which have an over the counter equivalent that may be obtained without a Prescription, even though such Prescription Drugs were
prescribed by a Provider; • any intentional misuse or abuse of Prescription Drugs, including Prescription Drugs purchased by an Insured for consumption by someone other than such
Insured unless such purchase was made in accordance with the written instructions of the prescribing Provider for the treatment or control of diabetes;• Prescription Drugs that are classified as anti-fungal medication used for treatment of onychomycosis; • programs, treatment or procedures for tobacco use cessation; • Prescription Drugs that are classified as tobacco cessation products;• charges for blood, blood plasma, or derivatives that has been replaced; and• services or supplies for personal convenience, including Custodial Care or homemaker services, except as provided for in the PremierMed Short Term
Medical-Surgical Expense Plan.
PremierMed - Non-Covered Items At A Glance, Cont’d