Embed Size (px)
Citation preview

1
Integrating Psychological Approaches
Into the Behavioral Management of
Modifiable Risk Factors
Alan Rozanski, M.D.January 30, 2013
• No disclosures
1. Define the rationale for integrating psychological approaches
2. Insights from Behavioral Cardiology
3. Illustrate practical principles and interventions
4. Discuss feasibility issues
Goals

2
• CVD mortality decreased by ~60%
• Decreased prevalence of myocardial infarction
• Decreased severity of infarction
• Decrease in stroke
• Decrease in frequency and severity of myocardial ischemia
Favorable trends
•Remains #1 killer•Reliance on Rx’s isincreasingly costly
•Adverse trends inprevention
CVD mortality by 60%PrevaIance of MISeverity of MIprevalance of stroke Ischemia
Favorable trends
Challenges
J Am Coll Cardiol 2012; 59: 2125-43

3
PATIENT EMPOWERMENT
Collaborativegoal setting
More effective education
Collaborative Rx planning
Patient self-management
Patient-centered cardiovascular care
a
“A vital component of PCC is educating and motivating patients to become better
stewards of their health and more active participants in the management of their
diseases”.
1. Define the rationale for integrating psychological approaches
2. Insights from Behavioral Cardiology
3. Illustrate practical principles and interventions
4. Discuss feasibility issues
Goals

4
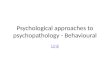
Psychosocial Risk Factors
1. Negative emotions2. Negative thought patterns3. Chronic stress4. Poor social support5. Poor sleep 6. Inadequate R&R
Ovarian dysfunction
EVOKED CENTRAL RESPONSES
ANS Dysfunction
Insulin resistance
Central obesity
Metabolic syndrome
Inflammation
Platelet activation
Endothelial dysfunction
bone density
CNS changes
Depression• ���� HPA
• ���� SNS
DEPRESSIONANXIETYSTRESS
LONELINESS
POOR DIETWEIGHT GAINSEDENTARY
SMOKING
DRIVE

5
• Epidemiology
• Pathophysiological study
• Study of behavioral consequences
• Little translation into cardiac practice
The “big disconnect”
Potential for clinical translation
• Vast field of Medical Psychology • This field has identified and developed
applicable evidence-based interventions• Applied psychology is commonly used in
many non-medical fields

6
1. Define the rationale for integrating psychological approaches
2. Insights from Behavioral Cardiology
3. Illustrate practical principles and interventions
4. Discuss feasibility issues
Goals
• John, a 55 yo very busy executive • Intermediate FRS• Moderately overweight• Highly sedentary • Increasing job stress• CAC scan: score = 180
Case example
• John, a 55 yo very busy executive • Intermediate FRS• Moderately overweight• Highly sedentary • Increasing job stress• CAC scan: score = 180
How do we get John to start and maintain anexercise program?
Case example

7
MOTIVATION EXECUTION MAINTENANCE
3 Components of goal attainment
Presentation of risk
�FRS Biomarkers Bayesian analysis Exercise ECG Stress echo Stress nuclear �CAC scanning Carotid imaging CT angiography
Presentation of risk
�FRS Biomarkers Bayesian analysis Exercise ECG Stress echo Stress nuclear �CAC scanning Carotid imaging CT angiography
Does the presentation of risk information motivate patients?

8
DESIGN OF THE EISNER TRIAL
2,137 volunteers with RFs,but no clinical disease
No scan group(n=713)
Scan group(n=1,424)
2:1 randomization
One time risk factorconsultation
4 YEAR CLINIC VISIT
One time RF consultationincluding scan result
4 YEAR CLINIC VISIT
RESULTS OF THE EISNER TRIAL
Compared to the no-scan group, the scan group showed net favorable change in:
– Systolic BP (p=0.02)
– LDL (p=0.04)
– Framingham score (p=0.003)

9
IMPACT ON
PHYSICIAN
IMPACTON
PATIENTS
RISK INFORMATION
RISKINFORMATION
BEHAVIORAL CHANGE
Enhancing Motivation
1. Motivational interviewing2. Self-efficacy3. Autonomy

10
• Express empathy• Elicit discrepancy between desired goals and
actual behavior(s) • “Roll” with resistance • Support self-efficacy
Motivational interviewing(Miller and Rollnick)
“Personal goal setting is influenced by self-
appraisal of capabilities.
The stronger the perceived self-efficacy, the higher the goal challenges people set for themselves
and the firmer is their commitment to them”.
SELF-EFFICACY
1997
People set goals and initiate new behaviors in
accordance with what they BELIEVE they can
accomplish
SELF-EFFICACY

11
20
15
10
5
Min
ute
s/ D
ay
30
25
Low Intensity
ModerateIntensity
HighIntensity
Prescription according to self-efficacy
AHA/ ACSM
Guidelines
20
15
10
5
Min
ute
s/ D
ay
30
25
Low Intensity
ModerateIntensity
HighIntensity
Prescription according to self-efficacy
AHA/ ACSM
Guidelines
John
PROMOTION OF AUTONOMY
EXTERNALMOTIVATION
INTERNAL MOTIVATION

12
PROMOTION OF AUTONOMY
EXTERNALMOTIVATION
INTERNAL MOTIVATION
• Stronger initiative• Relapse less likely
PauseProvide
information
• John, why would you like to exercise?
MOTIVATION EXECUTION MAINTENANCE
Not sufficient

13
MOTIVATION IS NOT SUFFICIENT(Shearan et al, 2002)
• Meta-analysis of 10 meta-analytic studies• 422 studies, involving 82, 107 participants
Intentions accounted for Only 28% of the variation in
behavior
MOTIVATION EXECUTION MAINTENANCE
~70% of variation
MOTIVATION EXECUTION MAINTENANCE
To make inspiration stick, you must root it to action
~70% of variation

14
IN THE DOCTOR’S OFFICE
• Establish risk for CAD• Counsel John on the importance of exercise • Motivate John to exercise • Prescribe an exercise program that is agreeable
Intertemporal discounting
In the “moment”….
There is a universal tendency toovervalue present goals
and undervalue future goals
TEMPORAL DISCOUNTING
NEXTDAY @ WORK
IN THE DOCTOR’S OFFICE

15
FuturePresent
Overcoming temporal discounting
• Make risk present-centered
• Make highly specific action plans
• Promote self-monitoring
• Automaticize the behavior
Future Present
FUTURE
RISK
PRESENT
EVIDENCE
THEORETICAL CONCRETE

16
Overcoming temporal discounting
• Make risk present-centered
• Make highly specific action plans
• Promote self-monitoring
• Automaticize the behavior
SPECIFICITY OF PLANS
MOTIVATION
GOAL
PLAN
SPECIFIC ACTION
BE HEALTHY
START EXERCISING REGULARLY
DAILY WALKS
WALK FOR 15 MINUTES AT LUNCH BREAKS
Telephone: 221-3399 State Reg. No
Name ______________________ Age____Address___________________ Date_____
Walk for 15 minutes @ 12:30 PM on weekdays
Dispense As Written

17
Overcoming temporal discounting
• Make risk present-centered
• Make highly specific action plans
• Promote self-monitoring
• Automaticize the behavior
• Promote self-awareness
• Platform for feedback
Future Present
Monitor baseline steps for one
week
Increase by X steps/wk

18
avata et al, JAMA 2007; 298: 2296-2304)
• 26 studies (8 randomized, 18 observational)
• Mean step increase:– 2,491 in the RCTs
– 2,183 in the observational studies
• Decreased body mass index
• Decline in systolic blood pressure
(Bravata et al, JAMA 2007; 298: 2296-2304)
Overcoming temporal discounting
• Make risk present-centered
• Make highly specific action plans
• Promote self-monitoring
• Automaticize the behavior
NEWPRACTICE
• Mindful & uncomfortable
HABIT
• Automatic
vs

19
WORKLUNCH
BREAK
Too much to doToo tiredToo stressedNot in the mood
PRACTICE HABIT
Implementation Intentions(developed by Dr. Peter Gollwitzer)
• Identify an EXTERNALstimulus (X) to cue behavior
• “X” can be a place, a situation, or a time

20
Implementation Intentions(developed by Dr. Peter Gollwitzer)
• Identify an EXTERNALstimulus (X) to cue behavior
• “X” can be a place, a situation, or a time
• Use the following formulation:
When it is “X”, I will do “Y”
“WHEN I HAVE MY LUNCH BREAK, I WILL TAKE A 15 MINUTE WALK”
John’s Implementation Intentions
X= Lunch breakY= Walking
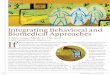
Mental contrasting & Implementation Intentions(Stadler et al, AM J Prev Med 2009, 36:29)
Baseline
3840
56
103
49
One week 16 weeks
12096
ExerciseInformation MCII group
MIN
OF
EX
ER
CIS
E/ w
eek
256 women30-50 years

21
Impact of Implementation Intentions(Gollwitzer & Sheeran, Advances in EP Social Psych, 2006)
Meta-analysisN=94 studies
8,461 participants
Implementation intentions have a medium to large
impact on goal achievement
MOTIVATION EXECUTION MAINTENANCE
Maintaining health behaviors
• Feedback
• Social support
• Contingency plans
• Stress management

22
• Facilitates objective assessment & adjustments
• Provides emotional support
• Motivational
FEEDBACK
Feedback
• Arrange for on-going feedback
• Creative opportunities– Web-based support/ follow-up
– Smart phone technologies
– Office staff
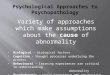
Predictors of Patient Adherence(Dimatteo MR, Health Psychology 2004; 23:207)
Social network-support
Practical social support
Emotional support
Unidimensional social support
Family cohesiveness
Married
Living with someone
No. of studies
29
11
27
14
51
17
Odds ratio
3.60 [2.55, 5.19]
1.83 [1.27, 2.66]
2.35 [1.76, 3.03]
3.03 [1.99, 4.52]
1.27 [1.12, 1.43]
1.38 [1.04, 1.83]

23
Social support
• Know your local hospital and community support resources
• Patient support groups
Contingency plans
StoppingStaying on the playing
fieldvs
StressTime pressureChanging prioritiesUnexpected eventsIllness
Contingency plans
Base plan• Walk every day
for 15 minutes
Contingencyplan
• Walk for 15 minutes/ weekends

24
• Coping issues
• Emotional problems
• R&R
• Sleep hygiene
• Exercise
Screen
For
Stress
1. Define why we need to integrate psychological approaches
2. Overview of Behavioral Cardiology
3. Illustrate psychological principles and interventions
4. Discuss feasibility
Goals
Feasibility
• Evidence-based
• Practical to render
• Does not require special psychological expertise

25
Time Allocation in Primary Care Offices( Tai-Seale et al, HSR 2007; 42: 1871)
n= 392 videotapesn= 392 videotapes
Median length of visits
Median # of topics
Time on chief complaint
Time on other topics
15.7 minutes
6
~ 5 minutes
~ 1 minute
Physicians
Office Staff
Behavioralspecialists or
programs
Health care delivery
Alan Rozanski, M.D.