Embed Size (px)
Citation preview
Intensive Early Intervention Services Using Applied Behavior Analysis for Young Children with
Autism Spectrum Disorders: Provider and Parent Perspective
Nan Perrin
&
Lisa Smith
Background
• O. Ivar Lovaas at UCLA began intervention research with children with autism around the 1970s
• He found that children with autism could reach a normal range of functioning
• Research continued with children with autism or PDD-NOS at various intellectual levels
• Research involved treatment, minimal treatment (less than 10 hours per week), and control groups
• Familial stress has been measured
Rationale
• The incidence of autism has increased• Children with autism show deficits in
communication, social interaction, and learning from the environment
• Children may engage in repetitive or aberrant behavior
• Spontaneous recovery of skills is not often the case
• A normal developmental trajectory has been reached in some children
Recommended Practices
• Surgeon General
• National Research Council, Educating Children with Autism
• National Standards Project
National Standards Project
• Treatment selection is complicated and should be made by a team of individuals who can consider the unique needs and history of the individual with Autism Spectrum Disorder (ASD) along with the environments in which he or she lives.
• Strongly encourages individuals choosing interventions select an evidence-based practice approach. (National Autism Center, 2009)
Evidence-based Practice
• “Evidence-based practice is a widely-accepted way of ensuring that recipients of early intervention, education, health care, and human services receive the best possible care.”
• “Practices are considered "evidence-based" when multiple research studies using the same or similar practices are related to the same or similar results or findings.”
• “Replication of the same effects across studies strengthens our ability to relate a specific practice to a specific outcome.”
• www.researchtopractice.info
Why is research important?
• Intervention could be harmful.
• Resources are limited and inefficient interventions can waste it.– Can waste time, money, and effort
• If we focus energy and time on inefficient interventions we may not have energy or time for the effective ones.
Types of Evidence
• Assertion
• Anecdotal
• Observational
• Correlational
• Case Study • Experimental
– Single-Subject Manipulation– Group Design Testing
How do we know if a practice is evidence-based?
• We review the literature. – How do you know if something is research
based?• Multiple Exemplars• Don’t just take the information at face value –
especially with the widespread availability of information on the web.
• Often in peer reviewed journals, popular press does not always require stringency.
What does that mean to all of us?
• Importance of documentation of skills and progress.
• Importance of asking professionals with whom you are working, what is the research base behind this intervention– What outcomes can we expect?– How will we know if this is working for my child?– How often will we review this procedure?
Recommendations for Treatment Selection
• Utilize Research findings in combination with other factors to select intervention techniques.
• Previous examples of comprehensive reviews include New York State Department of Health (1999) and the National Research Council (2001).
Established TreatmentsThe National Standards Project identified 11 treatments as Established
(i.e., they were established aseffective) for individuals with Autism Spectrum Disorders (ASD).
Established• Treatments are those for which several well-controlled studies have
shown• the intervention to produce beneficial effects. There is compelling
scientific• evidence to show these treatments are effective; however, even
among• Established Treatments, universal improvements cannot be
expected to• occur for all individuals on the autism spectrum.
The following interventions are Established Treatments:• ◖◖ Antecedent Package• ◖◖ Behavioral Package• ◖◖ Comprehensive Behavioral Treatment for Young
Children• ◖◖ Joint Attention Intervention• ◖◖ Modeling• ◖◖ Naturalistic Teaching Strategies• ◖◖ Peer Training Package• ◖◖ Pivotal Response Treatment• ◖◖ Schedules• ◖◖ Self-management• ◖◖ Story-based Intervention Package
Emerging Treatments
• A large number of studies fall into the “Emerging” level of evidence.
• These treatments deserve further research.
The following treatments have been identified as falling into the Emerging level of evidence:
• ◖◖ Augmentative and Alternative Communication Device {14 studies}• ◖◖ Cognitive Behavioral Intervention Package {3 studies}• ◖◖ Developmental Relationship-based Treatment {7 studies}• ◖◖ Exercise {4 studies}• ◖◖ Exposure Package {4 studies}• ◖◖ Imitation-based Interaction {6 studies}• ◖◖ Initiation Training {7 studies}• ◖◖ Language Training (Production) {13 studies}• ◖◖ Language Training (Production & Understanding) {7 studies}• ◖◖ Massage/Touch Therapy {2 studies}• ◖◖ Multi-component Package {10 studies}• ◖◖ Music Therapy {6 studies}• ◖◖ Peer-mediated Instructional Arrangement {11 studies}• ◖◖ Picture Exchange Communication System {13 studies}• ◖◖ Reductive Package {33 studies}• ◖◖ Scripting {6 studies}• ◖◖ Sign Instruction {11 studies}• ◖◖ Social Communication Intervention {5 studies}• ◖◖ Social Skills Package {16 studies}• ◖◖ Structured Teaching {4 studies}• ◖◖ Technology-based Treatment {19 studies}• ◖◖ Theory of Mind Training {4 studies}
» (NAC, 2009)
• National Standards Project argues that unless compelling reasons exist to do otherwise, intervention services should be comprised of Established Treatments and they should be delivered following the specifications outlined in the literature (e.g., appropriate use of resources, staff to student ratio, following the prescribed procedures, etc.). (NAC, 2009)
What is Early Intensive Behavioral Intervention?
• Based on Applied Behavior Analysis– Prompting– Shaping– Reinforcement
• Used with children with Autism and related disorders
• Purpose is to decrease aberrant behavior and increase socially appropriate behavior
• Attempts to remove behavioral characteristics of autism
Applied Behavior Analysis (ABA)
• A discipline devoted to the understanding and improvement of human behavior.
It’s not just about M&Ms
Some Components of ABA
• Discrete Trial Teaching
• Shaping
• Fading
• Reinforcement
• Prompting
• Chaining
• Applied: Socially significant, immediately important to individual or society in the natural environment.
• Behavioral: socially valid, observable and measurable.
• Analytical: yields convincing, reproducible, and conceptually sensible demonstrations of how to accomplish specific behavioral changes (Baer, Wolf, & Risley, 1987). Uses proven standards of intervention that have been experimentally demonstrated. Data driven decision making to achieve progress.
Key Components
• Begin early in child’s life
• Large number of hours per week
• Long duration
• Often takes place in the child’s home
• One-on-one instruction from a therapist, teacher, and/or parent
Lisa Smith
• A mother of seven children, ages five to twenty-one. Two of Lisa’s children have special needs. Lisa’s son, Tate, is eight years old and was diagnosed on the autism spectrum at age two and a half. For the past five and a half years Lisa has spent much of her time learning about autism spectrum disorders and advocating for her son.
What autism looked like in my toddler:
Toys and play were not typical.
There were strange attachments to objects.
Interaction with other children was nonexistent with the exception of siblings.
What autism looked like at age two and a half:
• Language had regressed.• He became withdrawn from most of the family.• There was anxiousness in unfamiliar surroundings.• Stereotypic behaviors began.
– Echolalia
– Hand-flapping
– Running without a purpose
– Tossing cloth and watching it fall
– Fanning pages of books
– Watching reflection in doors, mirrors, screens
The Diagnosis:• Initially, I found autism on the internet.
• The Pediatrician
• The Developmental Pediatrician
Early Intervention:• Infants and Toddlers
• Research Based Therapy– Behavior Consulting– In Home ABA: discrete trial and incidental
teaching
• Preschool– Public (free)– Private (costly)
Hard Work and Growth: • Language recovery
• Play Skills
• Academics
• Social Skills
Some remaining challenges:
•Finding appropriate activities that interest children with autism is challenging.•Public schools have been a real challenge
Educating the educators is a must.Educating the other students about autism is a must.
•Prompt dependence•Outings•Behaviors
Stereotypic BehaviorsAnxieties
Positives from our life with autism:
•Our family is educated, compassionate and involved with people with special needs.•People we have met along the way are a huge part of our life now.•Educating others about autism has helped our community.
General Description
• Intervention takes place in a secluded or private setting and involves time at the table and play
• Targeted skills are determined by team• Focus on skills the child does not do or at least
not consistently• Follows a developmental progression• Therapists are trained in behavioral techniques• Specific strategies are used to address problem
behavior• Intervention is overseen by a behavior analyst• Periodic team meetings are often held
General Description
• A discrete trial format is used for teaching(instruction-response-consequence)– A short, concise instruction is given– The child is prompted to respond, if needed– The child is reinforced for responding– The materials are removed and new materials are
placed for the next trial• Trials are repeated until the child responds more
independently • A target is continued until it meets the criterion
for mastery• Parents are trained to generalize skills to the
natural environment
Discrete Trial Teaching
• Consists of creating specific opportunities for a child to respond to a stimulus, and then delivering a consequence based on their response topography.
• Stimulus – Response – Consequence
• Stimulus (Sd) – (Discriminative Stimulus) descriptive statement that sets the occasion for a child to perform an action.
• Response – Behavior that is measurable and observable.
• Consequence – An event or stimulus following a response that increases or decreases the likelihood for the behavior to occur again.
• Inter-trial interval – a pause that separates trials from each other
Preschool Age Child
• Video of child
• Video of teaching during play
• Video of benchmarking
Shaping
• Taking advantage of related responses the child already has, reinforces them, and then only reinforces successive (closer and closer) approximations of the desired behavior or response
Prompting
• Something that aids the child in completing the desired skill or behavior• Types of Response Prompts
• Verbal—most difficult to fade• Gestural• Modeling• Physical• Positional cues
• Stimulus prompts • Pictures• Cues• Placement of objects
• Task analyzing behaviors and teaching: backward chaining, forward chaining, total task teaching
• Errorless prompting is typically most successful for children with autism
• Prompt Dependence
Early Intensive Intervention – Home and Center Based
• Individualized Programming– Assessment and development of an individualized treatment plan,
teaching programs, and data systems concentrating on the areas of communication, socialization, play skills, safety skills, personal care, and school preparation skills
• Intensive One-on-One Teaching– 30-40 hours per week; some teaching is done in child’s home and
community; some teaching might be done in a typical classroom• Training and Oversight
– Provided by professionals with expertise in applied behavior analysis and developmental and child psychology
• Parent Training and Involvement– Participation encouraged and actively supported, including periodic
team meetings and program planning• Documentation of Progress
– Data collection on the individual teaching goals with progress monitored
How to build an effective team!
Team Collaboration
Who should be involved?
Family
Individual
Teachers
ParaprofessionalsRelated Service
Personnel
IndividualsCircle of Support
Importance of developing relationships
Surgeon General Report
– Thirty years of research demonstrated the efficacy of applied behavioral methods
– Lovaas and colleagues (Lovaas, 1987; McEachin et al., 1993)
– A number of other research groups have provided at least a partial replication of the Lovaas model
Some additional references
• Kansas Best Practices Report
• National Autism Standards Project
What the research about Early Intensive Behavioral Intervention
tells us…• Intervention is most successful if begun at a young age,
between 2.5 and 4 years old• Intensive Intervention appears to be much more effective
than less intensive intervention (most success is with children who have 25-40 hours per week, 5-8 hours per day)
• Long term intervention appears to be needed (probably 2 to 4 years at a minimum)
• Behavioral programs have demonstrated a high degree of effectiveness in increasing functional skills and replacing challenging behavior.
• Both the Surgeon General and the Center for Disease Control have identified Behavioral Intervention as an effective intervention for children with autism.
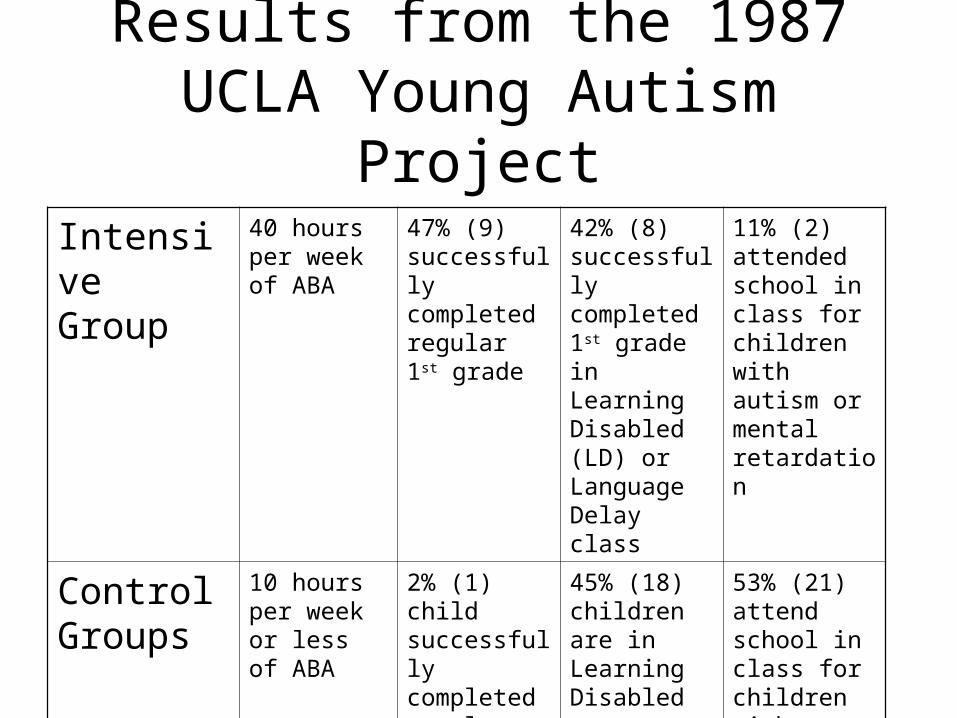
Results from the 1987 UCLA Young Autism Project
Intensive Group
40 hours per week of ABA
47% (9) successfully completed regular 1st grade
42% (8) successfully completed 1st grade in Learning Disabled (LD) or Language Delay class
11% (2) attended school in class for children with autism or mental retardation
Control Groups
10 hours per week or less of ABA
2% (1) child successfully completed regular 1st grade
45% (18) children are in Learning Disabled or Language Delay class.
53% (21) attend school in class for children with autism or mental retardation.
Provider Challenges in Serving Children with ASDs
Families request supportFamilies request support• Diagnostic challenges Diagnostic challenges
Waiting list, referral, responsiveness of doctorWaiting list, referral, responsiveness of doctor
The child gets the diagnosisThe child gets the diagnosis• Problem identified = solutionProblem identified = solution
Oops – forgot to mention this is not paid for Oops – forgot to mention this is not paid for
• Helping parents navigate the maze of servicesHelping parents navigate the maze of services
Gaps in Services Which direction to send families?
Too old Too young
Too rich
Too poor
Not enough need
Too much of
a disability
Cost Savings
– Jacobson, Mulick & Green (1998) completed a cost-benefit analysis of EIBI utilizing Pennsylvania.
– They estimate cost savings from $187,000-$203,000 per child for ages 3-22 and $656,000-$1,082,000 per child for ages 3-55.
– This only takes into consideration the saved expenditures, not the improvement in quality of life and the corresponding benefit of economic self-sufficiency.
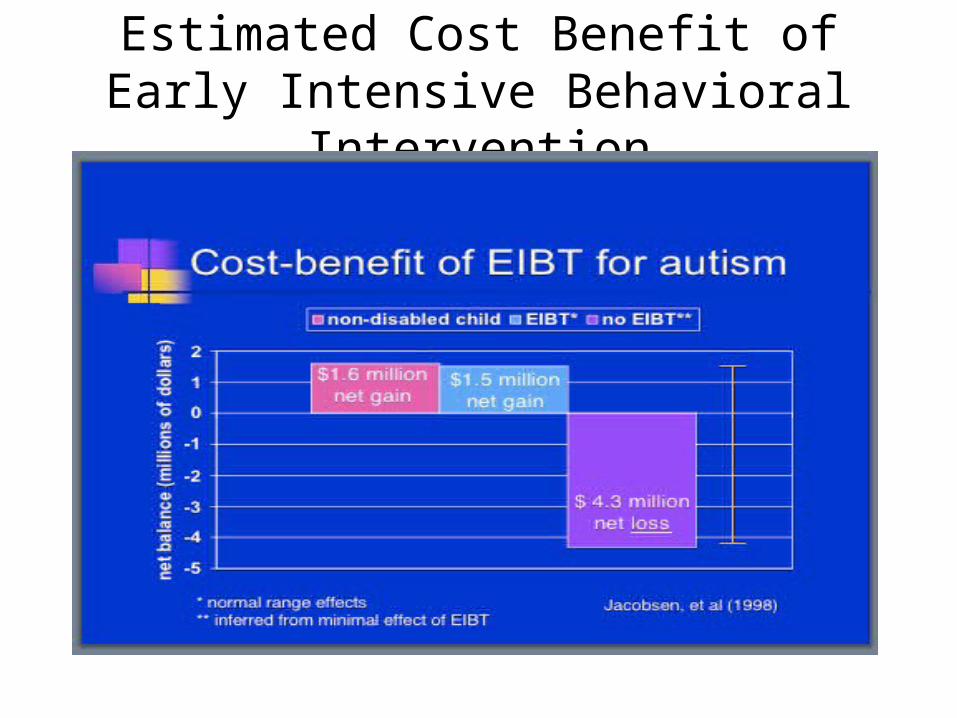
Estimated Cost Benefit of Early Intensive Behavioral Intervention
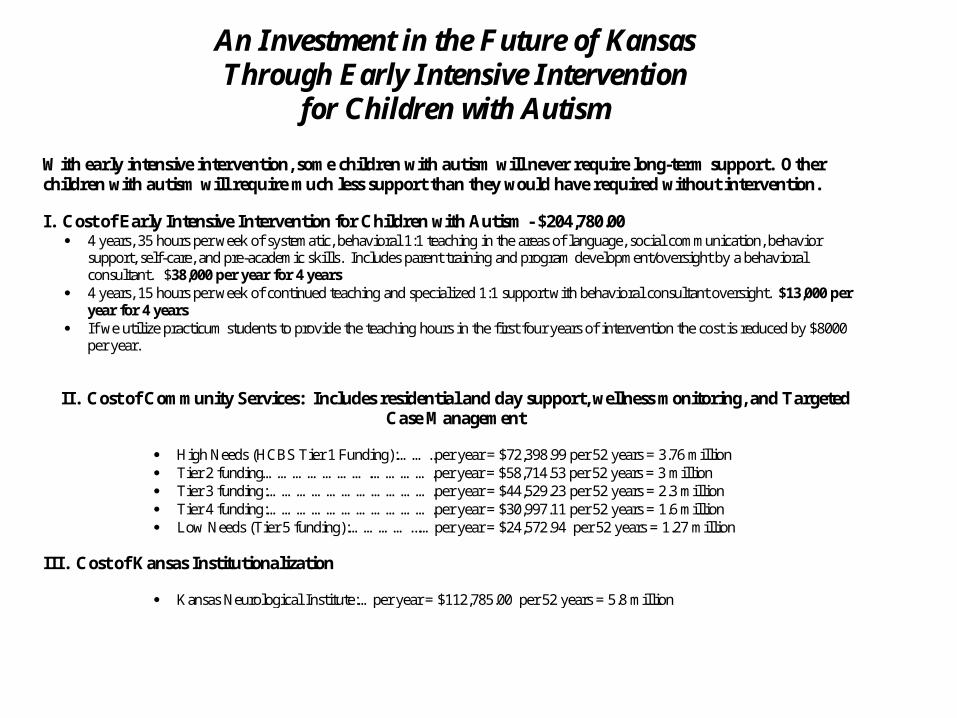
An Investment in the Future of Kansas Through Early Intensive Intervention
for Children with Autism
With early intensive intervention, some children with autism will never require long-term support. Other children with autism will require much less support than they would have required without intervention. I. Cost of Early Intensive Intervention for Children with Autism - $204,780.00
4 years, 35 hours per week of systematic, behavioral 1:1 teaching in the areas of language, social communication, behavior support, self-care, and pre-academic skills. Includes parent training and program development/oversight by a behavioral consultant. $38,000 per year for 4 years
4 years, 15 hours per week of continued teaching and specialized 1:1 support with behavioral consultant oversight. $13,000 per year for 4 years
If we utilize practicum students to provide the teaching hours in the first four years of intervention the cost is reduced by $8000 per year.
II. Cost of Community Services: Includes residential and day support, wellness monitoring, and Targeted Case Management
High Needs (HCBS Tier 1 Funding):……..per year = $72,398.99 per 52 years = 3.76 million Tier 2 funding………………….………….per year = $58,714.53 per 52 years = 3 million Tier 3 funding:…………………………….per year = $44,529.23 per 52 years = 2.3 million Tier 4 funding:…………………………….per year = $30,997.11 per 52 years = 1.6 million Low Needs (Tier 5 funding):…………...…per year = $24,572.94 per 52 years = 1.27 million
III. Cost of Kansas Institutionalization
Kansas Neurological Institute:…per year = $112,785.00 per 52 years = 5.8 million
Resources• Community Living Opportunities www.clokansas.org• National Autism Center, National Standards Project
http://www.nationalautismcenter.org/affiliates/reports.php• Kansas Institute for Positive Behavior Supports www.kipbs.org• Association for Positive Behavior Supports www.apbs.org• PBS Kansas www.pbskansas.org
Presenter Information• Nan Perrin, MA, BCBA – ECAP Director, Community Living
Opportunities, Inc. [email protected]• Lisa Smith – parent – [email protected]