Embed Size (px)
Citation preview

DOI: 10.1212/WNL.0b013e3181c677e1 2009;73;2126-2127 Neurology
Jack Puymirat, Yves Giguère, Jean Mathieu and Jean-Pierre Bouchard FAMILIES WITH MYOTONIC DYSTROPHY TYPE 1
INTERGENERATIONAL CONTRACTION OF THE CTG REPEATS IN 2
This information is current as of January 5, 2010
http://www.neurology.org/cgi/content/full/73/24/2126located on the World Wide Web at:
The online version of this article, along with updated information and services, is
All rights reserved. Print ISSN: 0028-3878. Online ISSN: 1526-632X. since 1951, it is now a weekly with 48 issues per year. Copyright © 2009 by AAN Enterprises, Inc.
® is the official journal of the American Academy of Neurology. Published continuouslyNeurology
at CHUQ PAV ST FRANCOIS D'ASSISE on January 5, 2010 www.neurology.orgDownloaded from

carrying a splice acceptor site mutation (IVS9-2A�T) inALS2 causes infantile-onset ascending spastic paralysis(IAHSP). Neurogenetics 2009;10:59–64.
5. Mintchev N, Zamba-Papanicolaou E, Kleopa KA, et al. Anovel ALS2 splice-site mutation in a Cypriot juvenile-onset primary lateral sclerosis family. Neurology 2009;72:28–32.
6. Kress JA, Kuhnlein P, Winter P, et al. Novel mutation inthe ALS2 gene in juvenile amyotrophic lateral sclerosis.Ann Neurol 2005;58:800–803.
7. Eymard-Pierre E, Yamanaka K, Haeussler M, et al. Novelmissense mutation in ALS2 gene results in infantile as-cending hereditary spastic paralysis. Ann Neurol 2006;59:976–980.
INTERGENERATIONAL CONTRACTION OF THECTG REPEATS IN 2 FAMILIES WITH MYOTONICDYSTROPHY TYPE 1Myotonic dystrophy type 1 (DM1) is an autosomaldominant multisystemic disorder caused by the ex-pansion of an unstable CTG trinucleotide repeat atchromosome region 19q13.3.1 The number of CTGrepeats is unstable in the abnormal range and usuallyincreases in size in successive generations, in associa-tion with anticipation.2,3 A decrease in the CTG re-peat size during transmission from parents to childcan also occur in about 6.4% of transmissions,most frequently during paternal transmissions(10%).4 In the French-Canadian DM1 popula-tion, intergenerational contractions occur in about7.4% of transmissions, all in cases of paternaltransmission. We report here 2 French-CanadianDM1 families with paternal transmission, bothoriginating from the Saguenay-Lac St-Jean, in
which all affected children display CTG contrac-tions. Although it was already reported that inter-generational contractions could be observed inseveral sibs in a same family, it was not notedwhether this occurred in all affected sibs.4 Overall,these observations support the existence of a pater-nal factor that prevents CTG expansion.
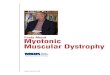
Case reports. The pedigree of the 2 families andSouthern blot analysis are shown in the figure.
Family A. No clinical information was available forI-1. II-4 was diagnosed with DM1 at age 38. He hadthe classic manifestations of the disease with distalmuscle weakness and wasting, myotonia, and cata-racts, with a Muscular Impairment Rating Scale(MIRS) of 3.5 Molecular analysis by Southern blotrevealed a CTG repeat size of about 500. His son anddaughter were evaluated at age 32 and 36. The son
Figure Family tree and Southern blot
Pedigree of family (A, B). (C, D) Southern blot analysis. The DNA (3–5 �g) was digested with EcoRV/HindIII, electrophoresed on 0.8% agarose gels, trans-ferred onto nylon membrane (Hybond, Amersham), and probed overnight with radiolabeled FNU428 probe, as previously described.7 The sizes of hybridizedfragments were determined from the autoradiographs containing the 1 kb DNA ladder (N32325, New England Biolabs) as markers.
Jack Puymirat, MD, PhDYves Giguere, MD, PhDJean Mathieu, MD, MScJean-Pierre Bouchard,
MD, FRCPC
2126 Neurology 73 December 15, 2009 at CHUQ PAV ST FRANCOIS D'ASSISE on January 5, 2010 www.neurology.orgDownloaded from

had myotonia and hypersomnia but no muscle weak-ness, whereas the daughter was clinically asymptom-atic, with an MIRS of 1. Molecular analysis revealeda CTG repeat size of 360 and 260 repeats for theson and the daughter. The brother of II-4, II-5was diagnosed with DM1 at age 48. He had mus-cle weakness and wasting, myotonia, a first-degreeheart block, and cataracts, which had been ex-tracted at age 30. The MIRS was 4. Molecularanalysis revealed a CTG repeat size of 630. His sonand daughter were diagnosed with DM1 at age 25and 27. Both were clinically asymptomatic, with aMIRS of 1. Molecular analysis revealed a CTGrepeat size of 260 repeats for both children. A newevaluation of the daughter at age 42 revealed thatshe was still clinically asymptomatic.
Family B. I-1 was diagnosed with DM1 at age 50.He had the classic manifestations of the disease withdistal muscle weakness and wasting, myotonia, cata-racts, and an MIRS of 3. Molecular analysis revealeda CTG repeat size of 500. I-1 had 4 affected childrenwho were diagnosed with DM1 at age 30, 34, 35,and 36. All were clinically asymptomatic with anMIRS of 1. Molecular analysis revealed a CTGrepeat size of 250 for all 4 children. Subjects II-5and II-6 both have 2 affected children. All wereclinically asymptomatic with a CTG repeat size of210 at age 10 (III-9), 5 (III-10), 7 (III-12), and 5(III-13).
Discussion. We report 2 DM1 families with pater-nal transmission in which a CTG repeat size contrac-tion was observed in all affected descendants. Infamily A, the contraction was observed in all affectedchildren from 2 branches and, in family B, a contrac-tion was observed in all affected children and hasremained stable in the next generation. There is onlyone reported case in which a CTG repeat size con-traction in one child was associated with a concomi-tant expansion in the brother, during paternaltransmission.6 In this latter study, however, a possi-ble bias may exist because of the weak differences inthe size of the CTG repeats between the father andthe children (833 for the father and 500, 667, and
1,000 for the children) and because the molecularanalysis was performed at different times.
This observation raises the possibility that, incases of paternal transmission, when a contraction isobserved in a sibling, intergenerational contractionscould be observed in all affected sibs, in differentbranches of the same family, and could remain stableacross further generations. Because this is of majorimportance for genetic counseling, this needs to beconfirmed in a large number of similar families.
From the Departments of Human Genetics (J.P.) and Medical Biol-ogy (Y.G.), Centre Hospitalier Universitaire de Quebec; Neuromus-cular Clinic (J.M.), Carrefour de Sante de Jonquiere, Quebec; andthe Department of Neurological Sciences (J.-P.B.), Hopital del’Enfant-Jesus, Quebec, Canada.
Disclosure: Dr. Puymirat reports no disclosures. Dr. Bouchardserved on a scientific advisory board for Merck Serono; served as aconsultant for Teva Pharmaceutical Industries Ltd.; and has re-ceived research support from Sanofi-Aventis and Biogen Idec. Drs.Mathieu and Giguere report no disclosures.
Received January 12, 2009. Accepted in final form September 23, 2009.
Address correspondence and reprint requests to Dr. Jack Puymirat,Department of Human Genetics, CHUQ, 2705 Blvd Laurier,Quebec, G1V4G2, Canada; [email protected]
Copyright © 2009 by AAN Enterprises, Inc.
1. Harper PS. Myotonic Dystrophy. London: W.B. Saun-
ders; 2001.
2. Hunter A, Tsilfidis C, Mettler G, et al. The correlation of
age of onset with CTG trinucleotide repeat amplification
in myotonic dystrophy. J Med Genet 1992;29:774–779.
3. de Die-Smulders CE, Howeler CJ, Mirandolle JF, et al.
Anticipation resulting in elimination of the myotonic dys-
trophy gene: a follow up study of one extended family.
J Med Genet 1994;31:595–601.
4. Ashizawa T, Anvret M, Baiget M, et al. Characteristics of
intergenerational contractions of the CTG repeat in myo-
tonic dystrophy. Am J Hum Genet 1994;54:414–423.
5. Mathieu J, Boivin H, Meunier D, Gaudreault M, Begin P.
Assessment of a disease-specific muscular impairment rating
scale in myotonic dystrophy. Neurology 2001;56:336–340.
6. Lopez de Munain A, Cobo AM, Saenz A, et al. Frequency
of intergenerational contractions of the CTG repeats in
myotonic dystrophy. Genet Epidemiol 1996;13:483–487.
7. Arsenault E, Prevost C, Lescault A, Laberge C, Puymirat J,
Mathieu J. Clinical characteristics of myotonic dystrophy
type 1 patients with small CTG expansions. Neurology
2006;66:1248–1250.
CONGENITAL NULL MUTATIONS OF THEFOLR1 GENE: A PROGRESSIVE NEUROLOGICDISEASE AND ITS TREATMENTFolate-receptor alpha (FOLR1) is of central importancefor folate transport across the blood–brain barrier viathe choroid plexus. Autoantibodies against folate recep-tors were identified as the cause of the infantile-onsetcerebral folate deficiency (CFD) syndrome.1 In addi-tion, FOLR1 is important for neural tube closure dur-
ing embryogenesis.2,3 Here we report siblings withcompound heterozygosity for 2 FOLR1 mutationscausing congenital CFD.
Clinical presentation. A 5-year-old boy developednormally until the age of 30 months. Thereafter,resting and intention tremor evolved, followed byataxia, progressive speech disturbances and loss ofmotor capabilities, general hypotonia, apathy, and
Supplemental data atwww.neurology.org
H. Cario, MDH. Bode, MDK.-M. Debatin, MDT. Opladen, MDK. Schwarz, MD
Neurology 73 December 15, 2009 2127 at CHUQ PAV ST FRANCOIS D'ASSISE on January 5, 2010 www.neurology.orgDownloaded from

DOI: 10.1212/WNL.0b013e3181c677e1 2009;73;2126-2127 Neurology
Jack Puymirat, Yves Giguère, Jean Mathieu and Jean-Pierre Bouchard FAMILIES WITH MYOTONIC DYSTROPHY TYPE 1
INTERGENERATIONAL CONTRACTION OF THE CTG REPEATS IN 2
This information is current as of January 5, 2010
& ServicesUpdated Information
http://www.neurology.org/cgi/content/full/73/24/2126including high-resolution figures, can be found at:
Subspecialty Collections
seshttp://www.neurology.org/cgi/collection/trinucleotide_repeat_disea
Trinucleotide repeat diseases http://www.neurology.org/cgi/collection/all_genetics
All Genetics rognosishttp://www.neurology.org/cgi/collection/natural_history_studies_p
history studies (prognosis)Natural http://www.neurology.org/cgi/collection/muscle_disease
Muscle disease ehttp://www.neurology.org/cgi/collection/all_neuromuscular_diseas
All Neuromuscular Diseasefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.neurology.org/misc/Permissions.shtmlor in its entirety can be found online at: Information about reproducing this article in parts (figures, tables)
Reprints http://www.neurology.org/misc/reprints.shtml
Information about ordering reprints can be found online:
at CHUQ PAV ST FRANCOIS D'ASSISE on January 5, 2010 www.neurology.orgDownloaded from