Embed Size (px)
Citation preview

1276
Internal Carotid Artery DissectionAfter Remote Surgery
Iatrogenic Complications of Anesthesia
Daniel B. Gould, MD; Kathleen Cunningham, BS
Background Subintimal dissection with acute occlusion ofthe internal carotid artery resulting in acute cerebral infarc-tion has not been reported as an iatrogenic complication ofgeneral anesthesia.
Case Descriptions An anesthetist stretched the neck of a44-year-old man by anchoring an anesthesia mask posterior tothe angle of the jaw with overlying fingers as the patientstruggled during an insufficient inhalational mask anesthetic.A 33-year-old man received an endotracheal anesthetic with-out struggle, but as he was turned from a supine to a prone
No report in the literature links the position of ananesthetized patient's head and neck or theforcible holding of an anesthesia mask to a
struggling (insufficiently anesthetized) patient with thecomplication of carotid artery intimal tearing, dissec-tion, and occlusion. The complication of carotid arteryocclusion and cerebral infarction typically is delayedafter the initial carotid artery injury and the beginningof dissection1-2 and may therefore divert attention fromthe physical rendering of a general anesthetic as thecause of such events. The following accounts describethe circumstances preceding these adverse events.
Case ReportsCase 1
A 44-year-old man weighing 185 lb, normotensive andwithout systemic disease, underwent surgical removal ofa cactus thorn from his hand. An initial 5 mg atracuriumand 350 mg thiopental followed by 100 mg succinylcho-line was administered intravenously. An anesthesiamask was held in place on the patient's face by theanesthetist's left hand. Laryngoscopy, attempted once,could not expose the larynx, although the patient'sanatomy was normal. Tracheal intubation was not pur-sued. Oxygenation was well maintained, as confirmed bypulse oximetry. Nitrous oxide (50%) and inspired en-flurane (2%) were administered through the mask, withan oral airway in place. Upon surgical incision thepatient moved strenuously. Assisted ventilation throughthe mask was maintained, while the patient producedhigh-pitched vocalization, another manifestation of a
Received February 18, 1994; final revision received March 22,1994; accepted March 22, 1994.
From the Department of Anesthesiology, St. Louis (Mo) Re-gional Medical Center (D.B.G.), and Meyer and Williams, Attor-neys at Law, PC (K.C.), Jackson, Wyo.
Correspondence to Daniel B. Gould, MD, 515 North MosleyRoad, Creve Coeur, MO 63141.
position, his head and neck were not immobilized to rotatewith his torso during the move. The next day both patientssuffered acute cerebral infarctions secondary to ICA dissec-tions and occlusions (angiographically demonstrated).
Conclusions Stretching the soft neck tissues of anesthetizedpatients can cause internal carotid artery dissection and acutecerebral infarction. (Stroke. 1994;25:1276-1278.)
Key Words • anesthesiainfarction • dissection
carotid arteries cerebral
light plane of anesthesia. The patient's head (ie, oc-ciput) was firmly restrained on the operating tableunder the anesthesia mask held by the anesthetist's lefthand. Sufentanil and more atracurium were given intra-venously to deepen the anesthesia.
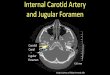
After surgery the patient awakened and complained ofpain on the left side of his neck. No external abnormal-ities were apparent, and he was released from thehospital. Eleven hours later he suddenly became aphasicand had right hemiparesis and right central facial palsy.On his immediate return to the hospital, carotid angiog-raphy was performed that demonstrated an occluded leftinternal carotid artery. The pattern of a conical, taperinglumen produced by subintimal dissection started at thelevel of the third cervical vertebra; flow ceased at C-2(see Figure). No filling of the left carotid siphon was seenfrom antegrade flow or from collateralized filling retro-grade to the ophthalmic artery. The aortic arch and othercervical vessels were normal; computed tomography(CT) of the head also appeared normal.
Heparin therapy was given after transfer to anotherhospital. Right-sided hemiparesis resolved in 2 days;intellectual function and fluent speech did not recover.CT of the brain then revealed acute infarction of the lefttemporal and parietal lobes in the territory supplied bythe middle cerebral artery. Repeat carotid arteriography6 days after the acute event demonstrated persistentocclusion of the left internal carotid artery and collateralblood supply to the left cerebral hemisphere from theanterior and posterior communicator branches. The pa-tient requires continuous custodial care.
Case 2A 33-year-old normotensive man, 6' 6" tall, with un-
confirmed suspicion of Klinefelter syndrome (XXY chro-mosome and variants) and symptomatic lumbar discherniation, was anesthetized for lumbar laminectomy inthe prone position. Laryngoscopy and tracheal intuba-
by guest on July 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Gould and Cunningham ICA Dissection After Remote Surgery 1277
...,-. I
Selective left carotid arteriogram (patient 1) demonstrating sub-intimal dissection of the left internal carotid artery manifested byan elongated, conical, tapered stenosis beginning at the level ofthe third cervical vertebra and cessation of flow at the petrousportion of that vessel.
tion were unremarkable; hemodynamics remained stablethroughout the anesthesia. The patient's recovery fromthe anesthetic was uneventful until the next day, when hesuddenly developed right hemiparesis.
Left internal carotid artery dissection was confirmedby immediate angiography; CT of the brain showedischemic infarction of the territory of the left middlecerebral artery. The patient has a permanent righthemiparesis and Broca's aphasia.
DiscussionThe mechanism of hyperextension of the neck with
axial rotation of the head and neck is the proposedmechanism of injury to the carotid artery that causesthe dissections described above. In case 1 the forcefulrestraint of the patient's head as his torso strainedagainst the operating table may well have stretched theinternal carotid artery "across the transverse process ofthe third cervical vertebra or the bony mass of the firstand second cervical vertebrae. This results in rupture ofthe intima and media at the level of the third cervicalvertebra with preservation of the more elastic adventi-tia."2 The fourth and fifth fingers of the left handholding the anesthesia mask might also directly trauma-tize the artery, as they anchor the mask by extendingover the mandible and encroaching on the carotidbifurcation.
In case 2 the tracheal intubation entailed no apparentdifficulties, and an adequate depth of anesthesia wasmaintained. Unrecognized movement of the neck whenthe patient was turned to the prone position or when thehead and neck were positioned with the patient prone(such as 90° axial rotation or extension instead offlexion) may have caused internal carotid artery dam-age. The potential for injury to the carotid artery existsfrom "cervical rotation and hyperextension,"3 perhapsenhanced for anesthetized patients unprotected by nor-
mal muscle tone. Reports of patients with Klinefeltersyndrome with ruptured cerebral aneurysms,4-5 coupledwith a propensity for gravitational leg ulcers at an earlyage, "lend support to the concept of a more fundamen-tal vascular abnormality" in this disorder.5 The secondpatient might have been at increased risk from anesthe-sia positioning because of this constitutional factor.5
The possibility that tracheal intubation might pro-duce carotid artery dissection3 or vertebral artery dis-section1-6 also has been suggested. The case report of a44-year-old woman with left internal carotid arterydissection and cerebral infarction attributes the catas-trophe to childbirth.7 However, her hemiparesis oc-curred 3 hours after general anesthesia for cesareansection.
A wide variety of physical stresses on the carotidartery capable of causing its dissection have been iden-tified.1-8 Manual manipulation of the neck has causedcarotid artery9 and vertebral artery10 dissection. Voli-tional strenuous neck movement also can produce ca-rotid artery dissection.11 The complaint of neck pain,voiced by the patient described above in case 1, isinfrequent in this entity; headache is a commonlyexperienced symptom.12 Although one survey of carotiddissection reports "an excellent or complete recovery"in 85% of the cases,12 a larger series emphasizes thelikelihood of significant morbidity.13 Spontaneous dis-sections of cervical internal carotid arteries, causingcranial nerve palsies, have recently been reported.14-15
Catastrophic cerebral infarction was not a feature ofthese patients.1415 The yearly incidence of spontaneousinternal carotid artery dissection is estimated to be 2.6per 100 000.16 Only one third of those affected in thesurvey16 had ischemic strokes, and the majority of thesepatients made a complete neurological recovery.16
Intraoperative brain infarctions carry a graver prog-nosis. Postsurgical infarctions of the brain stem andcerebellum arising in cardiovascular surgical subjectsfrom cardiac or aortic embolization, or in noncardiovas-cular surgical subjects from "position-related vertebralartery thromboses," produced severe neurological im-pairment in all cases.17
Two examples of acute dissection of left internalcarotid arteries with irreversible ischemic cerebral in-farction from occlusion following general anesthesia arenewly presented. Vigilance against operating room con-ditions capable of causing carotid artery intimal tearsrecommends itself. Surveillance for the briefly delayedclinical presentation of this complication will define itstrue incidence as a complication of mask anesthesiaadministration and the turning and malpositioning of ananesthetized patient (possibly with an additional riskfactor, as in case 2) lying prone on the operating roomtable.
References1. Hart RG, Easton JD. Dissections. Stroke. 1985; 16:925-927. Edi-
torial.2. Crissey MM, Bernstein EF. Delayed presentation of carotid
intimal tear following blunt craniocervical trauma. Surgery. 1974;75:543-549.
3. Zelenock GB, Kazmers A, Whitehouse WM, Graham LAM,Erlandson, Cronenwett JL, Lindenauer SM, Stanley JC. Extra-cranial internal carotid artery dissections. Arch Surg. 1982;117:425-432.
4. Price WH, Steers AJW, Wilson J. Subarachnoid haemorrhage andKlinefelter syndrome. Lancet. 1982;2:380. Letter.
by guest on July 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1278 Stroke Vol 25, No 6 June 1994
5. Monk B. Vascular abnormality in Klinefelter syndrome'7 Lancet.1982;2:491. Letter.
6. Caplan LR, Zarins CK, Hemmati M. Spontaneous dissection ofthe extracranial vertebral arteries. Stroke. 1985;16:1030-1038.
7. Wiebers DO, Mokri B. Internal carotid artery dissection afterchildbirth. Stroke. 1985;16:956-959.
8. Reddy K, Furer M, West M, Hamonic M. Carotid artery dissectionsecondary to seatbelt trauma: case report. / Trauma 1990;30:630-633.
9. Beatty RA. Dissecting hematoma of the internal carotid arteryfollowing chiropractic cervical manipulation. J Trauma. 1911;Y1:248-249.
10. Sherman DG, Hart RG, Easton JD. Abrupt changes in headposition and cerebral infarction. Stroke. 1981;12:2-6.
11. Jackson MA, Hughes RC, Ward SP, Mclnnes EG. 'Headbanging'and carotid dissection. Br Med J. 1983;287:1262.
12. Mokri B, Sundt TM, Houser OW, Piepgras DG. Spontaneousdissection of the cervical internal carotid artery. Ann Neurol. 1986;19:126-138.
13. Bogousslavsky J, Despland P-A, Regli F. Spontaneous carotiddissection with acute stroke. Arch Neurol. 1987;44:137-140.
14. Mokri B, Schievink WI, Olsen KD, Piepgras DG. Spontaneousdissection of the cervical internal carotid artery. Arch OtolaryngolHead Neck Surg. 1992;118:431-435.
15. Schievink WI, Mokri B, Garrity JA, Nichols DA, Piepgras DG.Ocular motor nerve palsies in spontaneous dissection of thecervical internal carotid artery. Neurology. 1993;43:1938-1941.
16. Schievink WI, Mokri B, Whisnant JP. Internal carotid artery dis-section in a community. Stroke. 1993;24:1678-1680.
17. Tettenborn B, Caplan LR, Sloan MA, Estol CJ, Pessin MS, DeWittLD, Haley C, Price TR. Postoperative brainstem and cerebellarinfarcts. Neurology. 1993;43:471-477.
by guest on July 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from
D B Gould and K Cunninghamanesthesia.
Internal carotid artery dissection after remote surgery. Iatrogenic complications of
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.25.6.1276
1994;25:1276-1278Stroke.
http://stroke.ahajournals.org/content/25/6/1276World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 6, 2018http://stroke.ahajournals.org/
Dow
nloaded from