Embed Size (px)
Citation preview

186
who desire to master the fundamentals of medicine-in order that they may the better see their way intreatment.To many the Westminster scheme will appear to
he merely an interesting experiment directed towardsthe placing of the teaching of pathology upon a newbasis. Actually it is far more. This and all other
plans of a like nature must stand or fall, not as theyaffect the teaching and study of pathology, but as
they influence the teaching and practice of medicineas a whole.
Annotations.
INTERNAL MIGRATION AND THE DEATH-RATE." Ne quid nimis.
"
IN a valuable though admittedly inconclusive inquiry, 1pursued in a thoroughly scientific way, Mr. A. B. Hillhas thrown new light on the problem as to whateffect migration of young persons produces on therelative death-rates of urban and rural areas. The
general facts obtainable from the Registrar-General’sreports and quoted in Mr. Hill’s report are fairly wellknown. Thus, in recent years the total urban death-rate for males is in excess of the rural at all ages under75, but closely approximates to the rural rate at theage-periods 20-25 and 25-30 years. For females theurban death-rates fall below the rural rates at ages20-30 years and occasionally also at ages 30-35.Similarly there is a higher death-rate in the ruralcounties from pulmonary tuberculosis at the ages ofadolescence and in early manhood and womanhood,which partially explains the difference between totaldeath-rates in urban and rural areas. The reportbefore us seeks answers to the question why thisshould be, points out the difficulties inherent in theusual explanations which are offered, and throws lighton the contention which has been advanced on goodauthority that much of the decline in the urban death-rate from phthisis is ascribable to urban migrationof the more vigorous units of population and not merelyto improved and more abundant food, to betterhousing, and to diminished dissemination of infection.
Briefly stated, the facts elicited, although notwarranting dogmatic statement, appear to show thatthe high general death-rates from all causes in therural parts of Essex in adolescence and early adultlife are caused by corresponding high death-ratesfrom phthisis, and that this has some relation to themigration into towns of adolescents of both sexes.The report recognises the need for evidence showing,as far as is possible, the life-history of migrants ; andby securing the cooperation of clergy and others inEssex, returns have been received from some 55
villages, relating to 402 males and 367 females, ofwhom about one-half were migrants. It appearslikely, in view of the information thus secured, thatmigrants have found prosperity in the town, and thattheir return sick to their rural homes is relativelyrare. One explanation of the excessive rural death-rates at certain ages can, therefore, probably beruled out. But it does not follow that the homekeepers-with a high death-rate in early adult life-hadintrinsically worse lives. Hence an attempt is madein the report to assess their conditions in rural lifeas to work, to housing and environment, and todiet. No special evil condition in rural work isrevealed ; and although rural housing and sanitationare often unsatisfactory, this cannot be held responsiblefor the high mortality in early adult life, in view ofthe fact, not mentioned in this report but revealedby the Census figures, that there is terribly greaterprevalence of overcrowding in its worst forms intowns than in rural districts.Much valuable information is given as to rural
1 Internal Migration and its Effects upon the Death-rates with Special Reference to the County of Essex. By A. B. Hill;B.Sc. Medical Research Council, Special Report Series, 95, 3s. 6d,
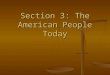
dietaries, and this part of the report especially deservesstudy by the social worker. Two-thirds of the incomeof the Essex families investigated was spent on food,and expenditure on boots must have meant oftengoing short of food. This would appear to havepossible direct bearing on the excessive phthisismortality in early adult life. It is pointed out in thereport that the diet would probably be most defectiveduring the first 12 or 14 years of married life, whenthe father is the only wage-earner, and that thiscorresponds roughly with the period at which ruraldeath-rates are high ; but as against this the curvesof growth and weight of Essex children show nosigns of malnutrition or lack of growth. If the Essexdietary is, as appears probable, below a desirable levelfor rural workers, the low phthisis death-rates whichare lower than those for London except at ages 20-25for males and at ages 10-35 for females (see figurebelow), do not appear to be consistent with the viewthat malnutrition has borne a large part in theresult. It appears highly improbable that the effect
Phthisis, 1901-10.* In ten rural registration areas in Essex.
of deficient food, even though the deficiency weregreatest at these ages, would be limited to adolescenceand early adult life. Nor can the " worse housingconditions " in rural districts, to which attention isdrawn, be held to explain these differences, for surelytheir effect would not be shown to such a preponderantextent in early adult life ; and as has been pointedout, room-famine is much greater in towns than inrural districts. In towns, furthermore, the oppor-tunities of gross and repeated infection are much morenumerous than in rural districts.The report is a careful review of a difficult and
intricate problem, presenting many variables, someof them elusive in nature. It should be studied by allsocial workers as a competent statement of methodsof investigation, of ways for overcoming these, andof caution in deducing results.





















![[Philip D. Curtin] Death by Migration](https://img.pdfslide.net/doc/110x75/55cf9b6f550346d033a610eb/philip-d-curtin-death-by-migration.jpg)





