Embed Size (px)
Citation preview

Saudi Pharmaceutical Journal (2013) 21, 277–280
King Saud University
Saudi Pharmaceutical Journal
www.ksu.edu.sawww.sciencedirect.com
ORIGINAL ARTICLE
Intervention to reduce the use of unsafe
abbreviations in a teaching hospital
* Corresponding author. Address: Director of Medication Safety
Research Chair, Vice Dean for Academic Affairs, College of Pharmacy,
King Saud University, P.O. Box 2475, Riyadh 11451, Saudi Arabia.
Tel.: +966 530039008.
E-mail address: [email protected] (H. Aljadhey).
Peer review under responsibility of King Saud University.
Production and hosting by Elsevier
1319-0164 ª 2012 King Saud University. Production and hosting by Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.jsps.2012.10.006
Mashael Alshaikh a, Ahmed Mayet b,c, Mansour Adam b, Yusuf Ahmed b,
Hisham Aljadhey b,c,*
a King Khalid University Hospital, King Saud University, Saudi Arabiab Medication Safety Research Chair, College of Pharmacy, King Saud University, Saudi Arabiac Clinical Pharmacy Department, College of Pharmacy, King Saud University, Saudi Arabia
Received 4 August 2012; accepted 28 October 2012Available online 16 November 2012
KEYWORDS
Unsafe abbreviations;
Medications
Abstract Objectives: To determine the effectiveness of a two-phase intervention designed to
reduce the use of unsafe abbreviations.
Methods: An observational prospective study was conducted at the King Khalid University
Hospital in Riyadh, Saudi Arabia during May–September 2009. A list of unsafe abbreviations
was formulated based on the recommendations of the Institute for Safe Medication Practices.
The first 7000 medication orders written at the beginning of each period were collected. Phase
one of the intervention involved educating health care professionals about the dangers of using
unsafe abbreviations. In the second phase of the intervention, a policy was approved that prohibited
the use of unsafe abbreviations hospital-wide. Then, another educational campaign targeted toward
prescribers was organized. Descriptive statistics are used in this paper to present the results.
Results: At baseline, we identified 1980 medication abbreviations used in 7000 medication orders
(28.3%). Three months after phase one of the intervention, the number of abbreviations found in
7000 medication orders had decreased to 1489 (21.3%). Six months later, after phase two of the
intervention, the number of abbreviations used had decreased to 710 (10%). During this phase,
the use of all abbreviations had declined relative to the baseline and phase one use levels. The
decrease in the use of abbreviations was statistically significant in all three periods (P < 0.001).
Conclusion: The implementation of a complex intervention program reduced the use of unsafe
abbreviations by 65%.ª 2012 King Saud University. Production and hosting by Elsevier B.V. All rights reserved.
1. Introduction
Approximately 5% of the medication errors reported in theUnited States are attributed to the use of unsafe abbreviations(Brunetti et al., 2007). Unsafe abbreviations are also known as
error-prone abbreviations because orders may be misinter-preted, resulting in patient harm (Koczmara et al., 2005).

278 M. Alshaikh et al.
Focusing on the word ‘‘error’’ draws attention to the questionof prevention: the issue of what can be performed to minimizemistakes and improve patient safety. In managing the use of
medications within hospitals, we aim to ensure that the ‘‘fiverights’’ are achieved: that the correct patient receives the rightdosage of the right drug via the correct route at the right time
(Benjamin, 2003). Techniques used to prevent medication er-rors in hospitals include the use of information technologyand automation, the establishment of medication safety pro-
grams, and the participation of pharmacists in the medicationmonitoring process (Committee on Identifying and Medica-tion Errors, 2006; Bates et al., 1998; Poon et al., 2006; Cohenet al., 2005; Vira et al., 2006; Nester and Hale, 2002; Bond
et al., 2000, 1999, 2002; McFadzean et al., 2003; Strunket al., 2008). However, low-cost solutions such as the non-use of unsafe abbreviations may also help to prevent medica-
tion errors.An abbreviation can be misinterpreted for a variety of rea-
sons. It may have more than one meaning, it may be unfamil-
iar to the reader, or if poorly written, it may be mistaken foranother abbreviation (Cohen, 2007). When simple abbrevia-tions are either inadvertently misused by prescribers or misun-
derstood by pharmacists and/or nurses, the wrong drug can beadministered. For example, ‘‘MS’’ can be used as an abbrevi-ation for either magnesium sulfate or morphine sulfate. Theuse of the abbreviation ‘‘u’’ is also responsible for numerous
medication errors (Institute of Safe Medication Practices.USP-ISMP Medicati, 1971). This abbreviation, which standsfor ‘‘units’’, is often used for high-alert drugs such as Heparin
and Insulin, which require special instructions and precau-tions. If a prescriber writes in a prescription that ‘‘4u’’ of reg-ular insulin are to be administered but the ‘‘u’’ looks like a 4 to
the nurse or pharmacist, the patient might be administered 44units of Insulin instead of 4 units (Paparella, 2004).
The Joint Commission and the Institute for Safe Medica-
tion Practices publish a ‘‘do not use’’ list of unsafe abbrevia-tions, symbols, acronyms and dose designations (Brunetti,2007; Lucci, 2004). In the United States, several studies haveimplemented interventions designed to reduce the use of unsafe
abbreviations (Garbutt et al., 2008; Abushaiqa et al., 2007;Myers et al., 2011). To our knowledge, however, no studyhas been conducted in another country that has evaluated
interventions intended to reduce the use of unsafe abbrevia-tions. The objectives of the current study were thus to estimatethe prevalence of the use of unsafe abbreviations and to deter-
mine the effectiveness of a two-phase intervention program de-signed to reduce the use of unsafe abbreviations in a teachinghospital in Riyadh, Saudi Arabia.
2. Methods
2.1. Design and setting
This observational prospective study was conducted in threephases: a baseline phase, a phase three months after the inter-
vention, and a phase six months after the intervention. We col-lected the first 7000 medication orders written at the beginningof each period (usually during approximately one week).
This study was conducted at the King Khalid UniversityHospital in Riyadh, Saudi Arabia. This is a tertiary teaching
hospital affiliated with King Saud University. With more than1000 beds, the hospital generally averages 800 patients in non-intensive care and more than 100 patients in surgical, medical
and cardiac intensive care units (ICUs). The patient popula-tion is comprised predominantly of local citizens. Medicalcare service is provided by attending physicians, registrars,
medical residents, interns, and students. The study was con-ducted over a six-month period in 2009 (May through Septem-ber). Ethical approval for this study was obtained from the
Institutional Review Board (IRB) at the King Khalid Univer-sity Hospital.
2.2. Baseline use of unsafe abbreviations
Based on the recommendations of the Institute for Safe Medi-cation Practices, a list of unsafe abbreviations was formulated(Institute for Safe Medication Practices. ISMP Error-Prone,
2011). This list included the use of ‘‘U’’ for units, ‘‘lg’’ formicrograms, ‘‘QOD’’ for every other day, ‘‘MS’’ for MorphineSulfate or Magnesium Sulfate, trailing zeros after a decimal
point, the symbol ‘‘>’’ for greater than, apothecary units asa substitute for metric units, the symbol ‘‘@’’ for ‘‘at’’, ‘‘CC’’for mL, ‘‘IU’’ for ‘‘international units’’, and ‘‘DC’’ for ‘‘discon-
tinue’’ or ‘‘discharge’’. The first 7000 medication orders werecollected and examined for the presence of any of these abbre-viations. Research assistants with a background in health (aspharmacy technicians or nurses) conducted the analysis of the
orders. All abbreviations found were marked and recorded ina data collection sheet.
2.3. Intervention
Three months after the baseline data on the use of unsafeabbreviations had been collected, the phase one intervention
commenced. The aim was to educate health care professionalsabout the danger of using unsafe abbreviations. The interven-tion included posters in all wards, medical chart dividers, in-
service education programs in all wards, and a medicationsafety day attended by the hospital’s physicians. Three monthsafter the start of the intervention, the use of unsafe abbrevia-tions was assessed using the same methodology as was used
during the baseline phase. A critical step during phase twoof the intervention was the approval of a policy prohibitingthe use of unsafe abbreviations hospital-wide; the hospital
administration distributed this policy to prescribers. Phasetwo also included another educational campaign for prescrib-ers. Three months later, another assessment of the use of un-
safe abbreviations was conducted.
2.4. Data analysis
Data were collected on the types of abbreviations used and thenumber of abbreviations per medication order. Information onprescriber rank was collected for a subset of the baseline data.Descriptive statistics were used to present the results. Tukey
and Bonferroni were used to compare the use of unsafe abbre-viations in the different periods. Version 17 of the StatisticalPackage for Social Science (SPSS) software was used for the
analysis.
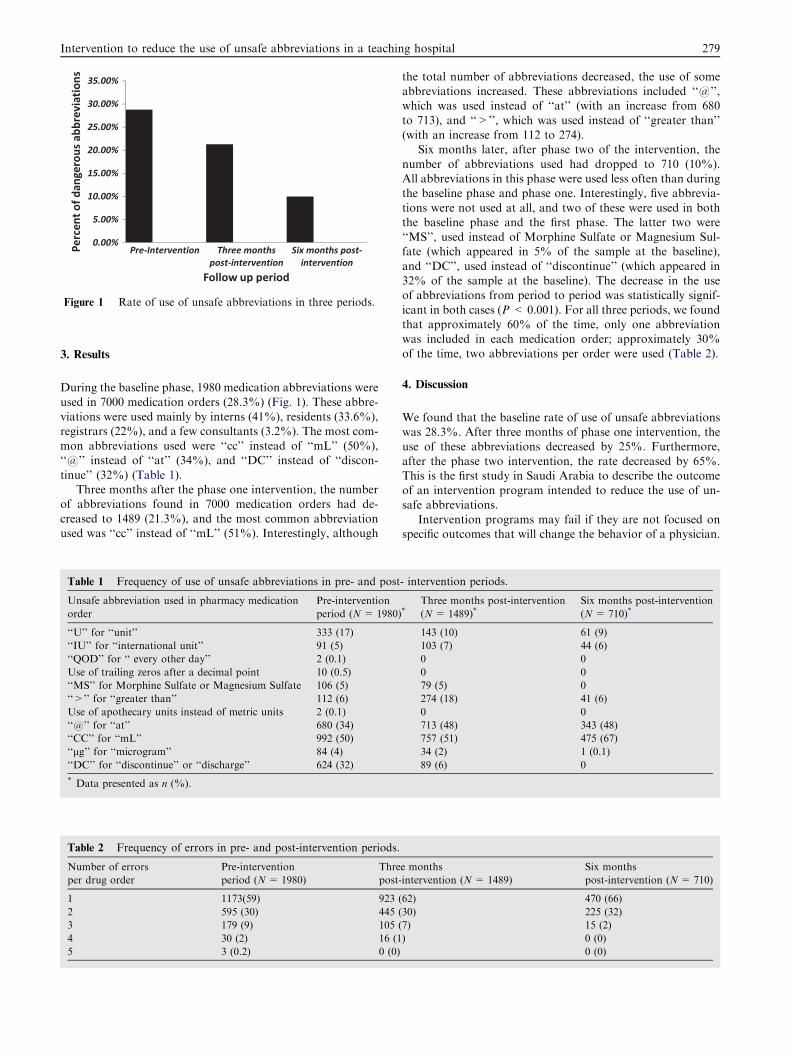
Figure 1 Rate of use of unsafe abbreviations in three periods.
Intervention to reduce the use of unsafe abbreviations in a teaching hospital 279
3. Results
During the baseline phase, 1980 medication abbreviations wereused in 7000 medication orders (28.3%) (Fig. 1). These abbre-
viations were used mainly by interns (41%), residents (33.6%),registrars (22%), and a few consultants (3.2%). The most com-mon abbreviations used were ‘‘cc’’ instead of ‘‘mL’’ (50%),‘‘@’’ instead of ‘‘at’’ (34%), and ‘‘DC’’ instead of ‘‘discon-
tinue’’ (32%) (Table 1).Three months after the phase one intervention, the number
of abbreviations found in 7000 medication orders had de-
creased to 1489 (21.3%), and the most common abbreviationused was ‘‘cc’’ instead of ‘‘mL’’ (51%). Interestingly, although
Table 1 Frequency of use of unsafe abbreviations in pre- and post
Unsafe abbreviation used in pharmacy medication
order
Pre-intervention
period (N = 1980)
‘‘U’’ for ‘‘unit’’ 333 (17)
‘‘IU’’ for ‘‘international unit’’ 91 (5)
‘‘QOD’’ for ‘‘ every other day’’ 2 (0.1)
Use of trailing zeros after a decimal point 10 (0.5)
‘‘MS’’ for Morphine Sulfate or Magnesium Sulfate 106 (5)
‘‘>’’ for ‘‘greater than’’ 112 (6)
Use of apothecary units instead of metric units 2 (0.1)
‘‘@’’ for ‘‘at’’ 680 (34)
‘‘CC’’ for ‘‘mL’’ 992 (50)
‘‘lg’’ for ‘‘microgram’’ 84 (4)
‘‘DC’’ for ‘‘discontinue’’ or ‘‘discharge’’ 624 (32)
* Data presented as n (%).
Table 2 Frequency of errors in pre- and post-intervention periods.
Number of errors
per drug order
Pre-intervention
period (N= 1980)
Thre
post-
1 1173(59) 923 (
2 595 (30) 445 (
3 179 (9) 105 (
4 30 (2) 16 (1
5 3 (0.2) 0 (0)
the total number of abbreviations decreased, the use of someabbreviations increased. These abbreviations included ‘‘@’’,which was used instead of ‘‘at’’ (with an increase from 680
to 713), and ‘‘>’’, which was used instead of ‘‘greater than’’(with an increase from 112 to 274).
Six months later, after phase two of the intervention, the
number of abbreviations used had dropped to 710 (10%).All abbreviations in this phase were used less often than duringthe baseline phase and phase one. Interestingly, five abbrevia-
tions were not used at all, and two of these were used in boththe baseline phase and the first phase. The latter two were‘‘MS’’, used instead of Morphine Sulfate or Magnesium Sul-fate (which appeared in 5% of the sample at the baseline),
and ‘‘DC’’, used instead of ‘‘discontinue’’ (which appeared in32% of the sample at the baseline). The decrease in the useof abbreviations from period to period was statistically signif-
icant in both cases (P < 0.001). For all three periods, we foundthat approximately 60% of the time, only one abbreviationwas included in each medication order; approximately 30%
of the time, two abbreviations per order were used (Table 2).
4. Discussion
We found that the baseline rate of use of unsafe abbreviationswas 28.3%. After three months of phase one intervention, theuse of these abbreviations decreased by 25%. Furthermore,
after the phase two intervention, the rate decreased by 65%.This is the first study in Saudi Arabia to describe the outcomeof an intervention program intended to reduce the use of un-safe abbreviations.
Intervention programs may fail if they are not focused onspecific outcomes that will change the behavior of a physician.
- intervention periods.
*Three months post-intervention
(N= 1489)*Six months post-intervention
(N= 710)*
143 (10) 61 (9)
103 (7) 44 (6)
0 0
0 0
79 (5) 0
274 (18) 41 (6)
0 0
713 (48) 343 (48)
757 (51) 475 (67)
34 (2) 1 (0.1)
89 (6) 0
e months
intervention (N = 1489)
Six months
post-intervention (N= 710)
62) 470 (66)
30) 225 (32)
7) 15 (2)
) 0 (0)
0 (0)

280 M. Alshaikh et al.
For example, an educational intervention intended to reduceprescribing errors in a teaching hospital did not decrease theuse of unsafe abbreviations (Garbutt et al., 2008). However,
unsafe abbreviations were reduced in another study that em-ployed an intervention similar to ours that was designed specif-ically to prevent the use of these abbreviations. The latter
study was conducted in 2003 in a 340-bed training hospitalin the United States. As in our study, abbreviations droppedafter three months (by 16%) and after sixth months (by
62%); additionally, when the program was extended to eightmonths, the use of unsafe abbreviations decreased by 83%(Abushaiqa et al., 2007). In another study, the use of comput-erized alerts reduced the use of unsafe medication abbrevia-
tions (Myers et al., 2011).The current study has several limitations that should be
considered. We did not qualitatively and quantitatively assess
the factors that contribute to the use of unsafe abbreviations.However, this may not be an important issue given that thegoal of our study was to assess an intervention intended to re-
duce the use of abbreviations. Second, we did not examine theoutcomes of using these unsafe abbreviations, or more specif-ically, whether they negatively affected patient care.
The results of the current study have important implica-tions for practice and research. When designing interventionsintended to change the behavior of health care providers,researchers should be sure to use several tools. This study also
emphasizes the importance of policy and regulations in chang-ing behavior. It will be easier for hospitals to implement poli-cies that prevent the use of abbreviations in medication orders
when the hospital in question is preparing for accreditation. InSaudi Arabia, the requirements instituted by the Ministry ofHealth stipulating that all hospitals must be accredited by
the Central Board of Accreditation for Healthcare Institutionswill aid in eliminating the practice of writing medicationabbreviations.
One advantage of using information technology in healthcare is that it can prevent medication errors. For example,the use of computerized physician order entry may eliminatethe use of abbreviations and consequently prevent errors.
One study in the United States reported that using computer-ized physician order entry reduced the rate of serious medica-tion errors by 55% (Bates et al., 1998).
In conclusion, the implementation of a complex interven-tion program reduced the use of unsafe abbreviations by65%. The use of computerized physician order entry will help
in eliminating medication errors caused by abbreviation use.
Acknowledgment
We acknowledge the support from the Medication Safety Re-search Chair at the King Saud University and support from
the National Plan for Science and Technology (09-BIO708-02).
References
Abushaiqa, M.E., Zaran, F.K., Bach, D.S., Smolarek, R.T., Farber,
M.S., 2007. Educational interventions to reduce use of unsafe
abbreviations. Am J Health Syst Pharm 64 (11), 1170–1173.
Aspden, P., Wolcott, J., Bootman, J.L., 2006. Committee on identi-
fying and preventing medication errors. In: Preventing Medication
Errors. Institute of Medicine National Academy Press, Washing-
ton, DC.
Bates, D.W., Leape, L.L., Cullen, D.J., et al., 1998. Effect of
computerized physician order entry and a team intervention on
preventing serious medication errors. JAMA 280 (15), 1311–1316.
Benjamin, D.M., 2003. Reducing medication errors in increasing
patient safety: case studies in clinical pharmacology. J Clin
Pharmacol 43 (7), 768–783.
Bond, C.A., Raehl, C.L., Franke, T., 1999. Clinical pharmacy services
and hospital mortality rates. Pharmacotherapy 19 (5), 556–564.
Bond, C.A., Raehl, C.L., Franke, T., 2000. Clinical pharmacy services,
pharmacy staffing, and the total cost of care in United States
hospitals. Pharmacotherapy 20 (6), 609–621.
Bond, C.A., Raehl, C.L., Franke, T., 2002. Clinical pharmacy services,
hospital pharmacy staffing, and medication errors in United States
hospitals. Pharmacotherapy 22 (2), 134–147.
Brunetti, L., 2007. Abbreviations formally linked to medication errors.
Healthcare benchmarks Quality Improvement 14 (11), 126–128.
Brunetti, L., Santell, J.P., Hicks, R.W., 2007. The impact of abbre-
viations on patient safety. Jt Comm J Qual Pt Saf 33, 576e83.
Cohen, M.R., 2007. Medication Errors, second ed. American Phar-
macists Association, Washington, DC.
Cohen, M.M., Kimmel, N.L., Benage, M.K., Cox, M.J., Sanders, N.,
Spence, D., Chen, J., 2005. Medication safety program reduces
adverse drug events in a community hospital. Qual Saf Health Care
14 (3), 169–174.
Garbutt, J., Milligan, P.E., McNaughton, C., Highstein, G., Water-
man, B.M., Dunagan, W.C., et al., 2008. Reducing medication
prescribing errors in a teaching hospital. Jt Comm J Qual Pt Saf 34
(9), 528–536.
Institute for Safe Medication Practices. ISMP Error-Prone Abbrevi-
ations List. http://www.ismp.org/tools/errorproneabbrevia-
tions.pdf (accessed 2011, September 26).
Institute of Safe Medication Practices. USP-ISMP Medication Error
Reporting Program reports received 1971- present. Huntingdon
Valley (PA): The Institute.
Koczmara, C., Jelincic, V., Dueck, C., 2005. Dangerous abbreviations:
‘U’ can make a difference! Dymanics 16 (3), 11–15.
Lucci, S.M., 2004. Joint Commission on Accreditation of Health care
Organizations’ dangerous abbreviations list What Effect Does This
Have on HowWeWork? J Am Assoc Med Transcr 23 (4), 214–217.
McFadzean, E., Isles, C., Moffat, J., Norrie, J., Stewart, D., 2003. Is
there a role for a prescribing pharmacist in preventing prescribing
errors in a medical admission unit? Pharm J 270, 896–899.
Myers, J.S., Gojraty, S., Yang, W., Linsky, A., Airan-Javia, S.,
Polomano, R.C., 2011. A randomized-controlled trial of comput-
erized alerts to reduce unapproved medication abbreviation use. J
Am Med Inform Assoc 18 (1), 17–23.
Nester, T.M., Hale, L.S., 2002. Effectiveness of a pharmacist acquired
medication history in promoting patient safety. Am J Health Sys
Pharm 59 (22), 2221–2225.
Paparella, S., 2004. Avoiding dangerous abbreviations and dose
expressions. J Emerg Nurs 30 (1), 54–58.
Poon, E.G., Cina, J.L., Churchill, W., Patel, N., Featherstone, E.,
Rothschild, J.M., Keohane, C.A., Whittemore, A.D., Bates, D.W.,
Gandhi, T.K., 2006. Medication dispensing errors and potential
adverse drug events before and after implementing bar code
technology in the pharmacy. Ann Intern Med 145 (6), 426–434.
Strunk, L.B., Matson, A.W., Steinke, D., 2008. Impact of a pharmacist
on medication reconciliation on patient admission to a veterans
affairs medical center. Hosp Pharm 43 (8), 643–649.
Vira, T., Colquhoun, M., Etchells, E., 2006. Reconcilable differences:
correcting medication errors at hospital admission and discharge.
Qual Saf Health Care 15 (2), 122–126.