Embed Size (px)
Citation preview

Gut 1997; 40: 602-607
L-arginine in low concentration improves rat
intestinal water and sodium absorption from oralrehydration solutions
R A Wapnir, M A Wingertzahn, S Teichberg
Department ofPediatrics andLaboratories,North ShoreUniversity Hospital,New York UniversitySchool ofMedicine,Manhasset,New York 11030, USAR A WapnirM A WingertzahnS TeichbergCorrespondence to:Dr Raul A Wapnir,Department of Pediatrics,North Shore,University Hospital,Manhasset,New York 11030, USA.
Accepted for publication23 January 1997
AbstractBackground-The nitric oxide (NO) pre-
cursor L-arginine has been shown toproduce variable effects on intestinalabsorptive function, including ion trans-port.Aims-To determine whether there is an
optimal concentration of L-arginine, pro-
moting proabsorptive effects from oralrehydration solutions (ORS) with 90 or
60mM sodium.Subjects and methods-In vivo perfusionof rat jejunum with determination of netwater absorption, unidirectional fluidexchanges, sodium and calcium trans-port, and glucose absorption.Results-L-Arginine (1 mM) added to the90 mM sodium ORS increased intestinalabsorption of both sodium and water.Higher concentrations of L-arginine (2 to10 mM) lacked this stimulatory effect. At20 mM, L-arginine decreased sodiumabsorption below baseline. With a 60 mMsodium ORS, 2 mM L-arginine had a
maximal fluid and electrolyte proabsorp-tive effect. At 20 mM L-arginine, net waterabsorption was indistinguishable fromthat obtained in the absence ofL-arginine,and lower than with 2 mM L-arginine.Sodium absorption remained raisedabove baseline in perfusions with 10 and 20mM L-arginine. Morphologically, villifrom perfusions with increased absorptionshowed a large expansion of intercellularand lamina propria intercellular spaces.Conclusions-Low concentrations of L-arginine seem to stimulate water andelectrolyte absorption by the small in-testine. This effect is consistent with NOinduced vasodilation, whereas higherL-arginine concentrations may be vaso-
constrictive and thereby reverse fluid andelectrolyte transport.(Gut 1997; 40: 602-607)
Keywords: L-arginine, nitric oxide, oral rehydrationsolutions, sodium absorption.
Nitric oxide (NO) is known to have multiplephysiological roles.' 2 In the gastrointestinalsystem NO can act as an inflammatorymediator, a regulator of intestinal ion trans-port, and as an inducer of soluble guanylatecyclase, which effects the relaxation of gastro-intestinal smooth muscle.3 Production ofNOcontributes to the preservation of vascular
integrity in endotoxin generated gut damage.6It has been postulated that endogenous NOregulates the integrity of the intestinal mucosa7and decreases mucosal permeability due toreperfusion injury.'
Several studies suggest that NO may havefavourable effects on transport in the smallintestine during normal and pathophysio-logical states. NO donor compounds stimulateelectrolyte transport in the guinea pig intestinein vitro.9 Both L-arginine and the NO donorsodium nitroprusside reduce water andelectrolyte secretion in isolated rabbit ileum.'"NO also reduces cholera toxin induced fluidsecretion in the rat, as deduced from thesystemic administration of L-arginine."1Similarly, inhibition of NO production seemsto be beneficial in experimental colitis.'2However, under certain circumstances, NOproduction leads to colonic electrolytesecretion. '3The principal physiological precursor ofNO
is L-arginine, a non-essential amino acid whichis metabolically processed by the urea cycle.'4The effects of L-arginine are stereospecific, thenatural L-isomer being the active form. NO issynthesised via NO synthase (NOS). Threeisozymes have been identified: two constitutive(NOS-I and NOS-III; cNOS) and an inducibleform (NOS-II; iNOS).'5 Known inhibitors ofiNOS, such as NG-nitro-L-arginine methylester (L-NAME), are stereospecific.'6 L-NAME can also modulate water transport inrat jejunum.'7 In the intestine it seems as if thedominant effects of NO vary according to thelocalisation of NO generators or NOinhibitors.
Oral rehydration solutions (ORS) haveundergone numerous modifications in searchof a formulation that would be effective in thereplacement of water and electrolyte losses indiarrhoea as well as reducing the purging rate,providing a direct inducement for use at homeby medically untrained care givers.'8 Aminoacids have been the most often tested lowmolecular weight additives to experimentalORS. L-alanine, glycine, and L-glutaminehave reached the stage of clinical trials.However, results with these amino acids havegenerally fallen below expectations. Otheradditives - namely, starch hydrolysates,especially from rice or glucose polymers - havegained greater acceptance and are probablymore effective.'9-21 Because NO may stimulateintestinal water and electrolyte absorption, theaddition of the NO precursor L-arginine toORS is of potential value. The goal of the
602
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from

L-arginine in oral rehydration solutions
present study was to determine the con-
centration of L-arginine in ORS that wouldproduce a maximal enhancement of absorp-tion, using a standard in vivo perfusion modelin rats.
Methods
EXPERIMENTAL PROTOCOL
Sprague-Dawley male rats (Zivic-Miller Labs,Pittsburgh, PA, USA) weighing 70 to 90 g were
allowed to acclimatise for at least 48 hours andthen fasted overnight before laparotomy.Briefly, under urethane anaesthesia (intra-peritoneal, 1-3 g/kg), a 15-30 cm segment ofthe jejunum immediately distal to the ligamentof Treitz, was identified and cannulated withflexible, plastic tubing at the proximal anddistal ports. The experimental ORS describedbelow, prewarmed to enter the perfusedsegment at 37°C, were delivered with a
peristaltic pump (Harvard Instruments,Boston, MA, USA, model 1203) at a rate of10-12 ml/h. The precise pumping rate was
determined by measuring the rate of flowbefore and after the perfusion. Approximately2 1iCi/l (= 74 MBq/l, NEN-Dupont, Boston,MA, USA) of tritiated water (3H20) was addedto all solutions to determine water influx U[Ifrom lumen to serosa. Based on previousdeterminations, the recirculation of the markerwas estimated to be negligible during thecourse of the experiment. Water secretion(serosa to mucosa efflux) [jel was estimated bycalculating the difference between influx andnet water absorption. The algorithms appliedto compute rates of absorption have beenpublished previously.22 Groups of 12 rats wereperfused simultaneously, and several solutionswere tested in the same experiment tominimise interexperimental variation. Thetotal number of rats used for each treatmentappears in the legend of the figures and in thetables. After a one hour equilibration, per-fusates were collected for eight 15 minuteperiods and analysed for net water absorption,unidirectional fluid movement, net sodiumabsorption, calcium secretion into the per-fusate, and glucose absorption. The rate of netwater absorption was computed by theformula:
(Inflow rate [rlmin])-(Outflow rate [ml/min])15 (min)XIL (cm)
The rate of water influx U[j, also expressed ini.l/minxcm, was calculated as follows:('H,O dpmoRsXInflow rate [mi/mn])-('H,O dpm_,,XOutflow rate [mi/min]) 1000
'H20 dpmoRsXIL (cm)
Electrolyte and glucose absorption werecomputed and expressed in nmol/minx cm:
([Solute[eRsXInflow rate [mi/min])-([Solute[).,,,xOutflow rate [mi/min]) xf
IL (cm)
where IL=intestinal length (cm); f=dilutionfactorX 1000.The assay results of each collection fraction
were averaged and only one value was taken foreach rat.Once the perfusion ended, the rats were
killed by exsanguination from the abdominal
aorta. The intestinal segment between thecannulae was extended with a 4 g weight andmeasured. Tritiated water was counted in a
Beckman LS-3800 ,B-scintillation counter;sodium and calcium were determined byatomic absorption spectrophotometry (Spec-trAA 10, Varian Instruments Inc, Sunnyvale,CA, USA) against external standards, andosmolality was measured by vapour pressure
changes (Model 5500, Wescor Inc, Logan,UT, USA). Free glucose was determinedenzymatically (Sigma 510). Nitrite accumu-
lation in the perfusates was quantified by a
method based on the Griess reaction.'2 Theprotocol for this study was approved by theInstitutional Animal Care and UtilizationCommittee.The basal WHO-ORS contained sodium
chloride (30 or 60 mM) and trisodium citrate(10 mM), making a total sodium concentrationof either 60 or 90 mM, potassium chloride(20 mM) and glucose (111 mM=20 g/l).L-arginine (Sigma, St Louis, MO, USA) was
added to the solutions at a 0 5, 1-0, 2-0, 10-0,or 20 mM concentration. Table I presents theosmolality of the basal and modified ORS.Results are expressed as means (SEM).
LIGHT AND ELECTRON MICROSCOPY
For study by light and electron microscopy thejejunum was fixed by perfusion through thelumen with 2% glutaraldehyde in 0 05 Mcacodylate buffer (pH 7 3) at room tem-perature, followed by immersion in the same
buffer at 4°C for two to 18 hours. The tissuewas then rinsed in cold buffer, dissected intowell oriented fragments to include regionsspanning from the serosal surface to villus tip.Tissue fragments were postfixed in 2%buffered osmium tetroxide at 4°C for twohours, treated with 1% tannic acid in 0-1 Mcacodylate, rinsed in buffer, dehydrated in a
series of ethanol dilutions, and embedded ineffapoxy resin (E Fullam, Schenectady, NY,USA). One micrometre thick plastic sections,stained with toluidine blue, were examined bylight microscopy. Thin sections were studiedand stained with uranyl acetate and leadcitrate, on a JEOL-JEM 1 00CXII electronmicroscope.
Samples from both the 60 mM and 90 mMsodium ORS perfusions were studied by lightand electron microscopy in the absence ofL-arginine, at the concentration of maximalsodium and water absorption for each ORSand at the highest L-arginine concentrationused (20 mM). Light microscopical studieswere done "blind" to assess histologicaldifferences and to compare the relative amount
TABLE I Mean osmolality (mOsmlkg) of basal ORS andthose containing arginine
L-Arginine (mM)
0 05 10 2-0 100 20-0
90mM sodium 307 311 319 324 365 37760 mM sodium 271 276 279 271 296 308
The values correspond to two to four measurements per group.
603
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from

Wapnir, Wingertzahn, Teichberg
of tannic acid stained material adherent to themicrovillus brush border under the variousexperimental conditions.
STATISTICAL ANALYSISFor transport studies, the significance of thedifferences among means was assessed bythe Kruskal-Wallis test with non-parametricmultiple contrasts.23 A test for trend wasapplied to determine L-arginine concentrationversus dependent variable outcomes.24 Theminimum level of significance was set atp<0 05.
Results
WATER AND ELECTROLYTE ABSORPTIONThe addition of a low concentration ofL-arginine enhanced water and electrolyteabsorption from both the 90 mM and 60 mMsodium ORS (Figs 1 and 2). When L-argininewas added to the 90 mM sodium ORS at a 1mM concentration, there was a significantincrease in the absorption of both sodium andwater (Fig 1). A lower concentration ofL-arginine (0-5 mM) produced no alterationsover baseline. An increase in L-arginineconcentration to 2 or 10 mM dissipated thestimulatory effect. The addition of 20 mML-arginine resulted in sodium absorption rateslower than the baseline. For both net water andsodium absorption the uptake at the threehighest concentrations of L-arginine was
400 - -N 4.0 r
0 0rz E 20lN43 :
CLo30 3Z
L-arginine (mM)Figure 1; Mean (SEM) rates ofsodium and net waterabsorption during perfusions of90mM sodium ORScontaining variable concentrations ofL-arginine. *p<O0S0;**p<0.01 compared with 0 mM L-arginine. +p<0 05;++p<001; +++p<0 0001 compared with maximalabsorption rates (1 mM L-arginine). The number ofanimals is that shown in Table II.
350NE- 300 3.0 0
H"'- 0 0
-50 Iz20
L-arginine (mM)
Figure 2: Rates ofsodium and net water absorption during
perfusions with 60mM sodium ORS containing variable
concentrations of L-arginine. *p<0.OS; **p<0.01;
****p<0 0001 compared with 0mM L-arginine.
++p<001; +++p<0 001; ++++p<0 0001 compared with
maximal absorption rates (2 mM L-arginine). Other
features are as in Fig 1.
significantly lower than the peak valuesobtained with the addition of 1 mML-arginine.
In ORS perfusions containing 60 mMsodium, L-arginine exerted its maximumproabsorptive effect on water and sodiumabsorption at 2 mM (Fig 2). At thisconcentration of L-arginine net transport ofthe electrolyte was absorptive. At lowerL-arginine concentrations, the values obtainedfor sodium transport were indicative of abalance in sodium movement to and from thelumen, with modest mean secretory values at1 mM L-arginine. Net water absorption at 2mM and at 10 mM L-arginine remained higherthan baseline. However, when L-arginine wasincreased to 20 mM, net water absorptionbecame indistinguishable from that obtained inthe absence of L-arginine, and lower than atthe maximum effective concentration of 2 mML-arginine. Sodium absorption remainedhigher than baseline in perfusions with 10 mMand 20 mM L-arginine.
WATER FLUXESWith the 90 mM sodium ORS, L7J, asdetermined by the disappearance of tritiatedwater, was increased with 1 mM L-arginineand decreased with 20 mM L-arginine,paralleling net water absorption data (TableII). Water efflux [Je] also declined with 20 mML-arginine as well as at 2 mM L-arginine. Theratio [Ji]/[e] was unaffected by the L-arginineconcentration.
In 60 mM sodium ORS perfusions (TableII) [i] increased at 2 mM L-arginine,paralleling net water absorption, and a declinein [Je] was evident at 20 mM. The [Yi]/[e]ratio peaked at 2 mM and remained raised at10 mM and 20 mM L-arginine. With 2 mML-arginine, this ratio was greater than at 0 5mM and 10 mM L-arginine. The trendtoward a higher ratio as the concentrationof L-arginine increased was consistent withthe decline in water [je]. Despite thelower osmolality of the 60 mM sodiumORS, baseline water net absorption, uni-directional fluxes, and flux ratios were in-distinguishable from those of the 90 mMsodium ORS.
GLUCOSE, CALCIUM, AND NITRITE STUDIESL-Arginine, in concentrations ranging from1 to 20 mM, generally stimulated glucoseabsorption from both the 90 and 60 mMsodium ORS (Table III).No relation was evident between calcium
secretion and water and sodium data. Calciumwas secreted under all perfusion conditions,but was greater with 60 mM than 90 mMsodium (Table III). With the 90 mM sodiumORS, calcium secretion was maximal at20 mM L-arginine. With the 60 mMsodium ORS, calcium secretion was maxi-mal at 10 mM L-arginine. Calcium releaseinto the lumen was about three orders ofmagnitude smaller than sodium absorptionrates.
604
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from

L-arginine in oral rehydration solutions
TABLE II Unidirectional waterfluxes
L-Arginine (mM)
0 0-5 1.0 2-0 10 0 20-0
Perfusions with 90 mM sodium:Influx [JJ] (jLl/minxcm) 5-12 (0-26) 5-33 (0 38) 6-80 (0 53)* 4-83 (0 28) 5-01 (0-36) 3-75 (0-19)++++n 12 13 14 13 11 12Efflux LRI] (,ul/minxcm) 3-65 (0-23) 3-78 (0 39) 3 95 (0 32) 3 04 (0-17)+ 3-37 (0-29) 2-61 (0-018)**++[JJ/R] 1-42 (0-06) 1-42 (0 07) 1-78 (0-11) 1 64 (0-13) 1-55 (0 11) 1 48 (0-08)Perfusions with 60 mM sodium:Influx [J] (il/minxcm) 4-80 (0-31) 5-22 (0 46) 4-80 (0-21) 5-65 (0 23)* 5 50 (0 28) 4-39 (0 19)n 12 11 13 12 11 14Efflux LR] (p.l/minxcm) 3-20 (0 23) 3-52 (0 34) 3-23 (0 19) 2-60 (0-18) 2-98 (0-27) 2-44 (0-14)**LJYU/] 1-53 (0 08) 1-5 (0 06)++++ 1 51 (0 07)++++ 2-26 (0-14)**** 1 91 (0-08)*** 1-83 (0 06)**
*p<0-05; **p<0-01; ***p<0 001; ****p<0-0001 v 0 mM L-arginine.+p<005; ++p<0 01; ++++p<0 0001 v highest value.Data expressed as means (SEM).
TABLE III Glucose and cakium transport in the presence ofL-arginine
L-Arginine (mM)
0 05 1.0 2-0 100 20-0
[Na] (mM)
90 60 90 60 90 60 90 60 90 60 90 60
Glucose 39 3 30-1 38-1++ 27-3+ 60-2** 48.9** 55-1** 44-0 58.8** 54 6*** 59.9*** 50-6**(nmol/minxcm) (3 0) (5-6) (4-0) (3 8) (6 5) (5-6) (4-4) (3-6) (4-7) (4-1) (3 8) (3-7)(n) (12) (12) (13) (11) (14) (13) (13) (12) (11) (11) (12) (14)Calcium -58 -198 -78 -216 -80 -238 -131 -202 -75 -269*+ -110** -190(pmol/minxcm) (17) (24) (13) (36) (18) (14) (39) (16) (22) (20) (18) (11)
*p<0-05; **p<0-01; ***p<0 001; v 0 mM L-Arginine.+p<0Q05; ++p<0 001 v highest value.Data expressed as means (SEM).
Nitrite measured in the outflow of theperfusates containing 90 mM sodium showedno direct relation with the concentration ofL-arginine present. The baseline value of 13-3(1 6) pmol/minxcm only increased to 30 3(7 7) pmol/minxcm at 10 mM L-arginine.Nitrite production and release was notdetermined in perfusions with 60 mMsodium.
MORPHOLOGICAL FINDINGSLight microscopical studies of jejunal villifocused on the extracellular space of villusmucosa and lamina propria histologicalcompartments. Generally, morphological
49%v;;s^x~~~~~ . BWfX4 tTi<
+,~~~~~~~~~~~~~~~~~~~4
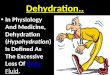
Figure 3: Light photomicrographs of 1 ,um sections of typicaljejunal viiifrom preparationsperfused with a 90 mM sodium ORS without L-arginine (A), with the addition of 1 mML-arginine (B), and with 20mM L-arginine (C). Note the dilation of intercellular spacesbetween enterocytes on the villus mucosa and of the lamina propria with the 1 mML-arginine 90 mM sodium ORS (B), compared with the L-arginine free perfusion (A).This increase in extrecellular space is no longer evident when the L-arginine concentration israised to 20 mM. Originally X450.
changes of jejunal villi reflected L-arginineinduced water and sodium transport alter-ations from perfusion experiments. Jejunal villiperfused with an L-arginine free 90 mMsodium ORS showed some dilation of inter-cellular spaces between enterocytes and laminapropria (Fig 3A). The addition of 1 mML-arginine to the 90 mM sodium ORSperfusion led to a greatly increased expansionof the mucosal and lamina propria intercellularspaces, a finding consistent with the stimula-tion of water and sodium translocation fromthe lumen across the mucosa (Fig 3B). Bycontrast, in ORS perfusions with 20 mML-arginine, mucosal and lamina propria inter-cellular spaces were reduced and were notreadily distinguishable from villi in L-argininefree perfusions (Fig 3C). The pattern ofmorphological findings with the 60 mMsodium ORS paralleled those seen with 90 mMsodium (Figs 4A, B, and C). With the 60 mMsodium ORS, intercellular space expansionwas most evident at 2 mM L-arginine (Fig 4B),but was reduced in jejunum perfused with 20mM L-arginine (Fig 4C).There was no evidence of structural damage
to jejunal villi, or of changes in the number ofgoblet cells under any of the perfusionconditions. The amount of tannic acid positivematerial adherent to the brush border variedbetween animals, but no effect produced by thediffering L-arginine perfusion conditions wasdistinguishable. When examined by electronmicroscopy villus absorptive cells from 90 mMand 60 mM sodium ORS perfusions werenormal in appearance and unaltered by theaddition of L-arginine at the concentrationproducing maximal proabsorptive effect (Figs5A and B).
605
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from

Wapnir, Wingertzahn, Teichberg
4. C
Figure 4: Light photomicrographs of typicaljejunal villi perfused with a 60mM sodiumORS, with no added L-arginine (A), with 2 mM L-arginine (B), and with 20mML-arginine (C). The pattern ofchanges in the amount ofmucosal and lamina propriaintercellular space is similar to that seen with the 90 mM sodium ORS. With the 60 mMsodium ORS, dilation of the intercellular spaces on the villus mucosa and lamina propria ismost pronounced in 2 mM L-arginine perfusions (B). The expansion of the extracellularspaces is then reduced when L-arginine is perfused at 20 mM (C). Originally X 450.
DiscussionThe results indicate that the addition ofrelatively low concentrations of L-arginine(1-2 mM) to an ORS can induce positiveincrements in the rates of sodium and water
absorption, when tested in an in vivo jejunalperfusion system in the rat. This effect was
seen in ORS with 90 mM as well as 60 mMsodium. These physiological transport datawere paralleled by morphological studies
4:N
MV
tADr_iJ
N~ ~ ~ ~ ~ ~ ~~M
::~~~~~~~~~~A "k. I ;N@:
Figure 5: Electron micrographs ofportions of absorptive epithelial cellsfrom jejunalpreparations perfused with 1 mM L-arginine in a 90mM sodium ORS (top, A) and 2mML-arginine in a 60mM sodium ORS (bottom, B). There is no evidence ofdamage to theorganelles of the absorptive epithelium. Microvilli (MV), mitochondria(M) and Golgiapparatus (G), all appear intact. Nucleus is at (N). The dilated lateral intercellular spacesare at (S). A originally X 13 300, B originally X 11 000.
showing expansion of the intercellular spacesafter perfusion with low concentrations ofL-arginine, a finding consistent with increasedwater and electrolyte absorption.By contrast with the present data, earlier
studies with L-arginine indicated induction ofwater secretion in the rat small intestine.'7 25 26However, those secretory effects occurred at arelatively high (20 mM) concentration of theamino acid; lower L-arginine concentrationswere apparently not tested. In the presentstudy, increasing the concentration of L-arginine to 20 mM also produced a decreasein electrolyte absorption with the 90 mMsodium preparations. These results are com-parable with those reported earlier with aglucose free solution containing 140 mMsodium.'7 25 26 It should be noted that L-arginine retained its proabsorptive effect up toa 10 mM concentration when the ORScontained 60 mM sodium. The enhancementof sodium uptake from the 60 mM ORS wasremarkable in that it greatly exceeded theequilibrium point for sodium transport intothe jejunum, which is in the 60-65 mMrange, as documented in rodent27 and humanstudies.28Amino acids generally tend to increase water
and sodium absorption in the small intestine,as a consequence of the sodium cotransportmechanism involved in the translocation ofmany natural amino acids across epithelia.This explanation is not tenable for L-argininefor several reasons. In the present study theeffect of this amino acid was not concentrationdependent, whereas a dose-response relationwith water and electrolyte absorption has beenfound in animal experiments with L-alanineand L-glutamine in animals29-31 and inhumans.20 32The sodium cotransport linkage isalso not applicable, as the y+ system involvedin L-arginine transport is considered to be afacilitated diffusion process dependent on adifferential in membrane potential. ' Aminoacids are not uniformly proabsorptive. Glycine,initially postulated as a stimulatory additive, isineffective at high concentrations; this isprobably due to inappropriate sodium: aminoacid stoichiometry and increased osmolality.3Moreover, the transport enhancing effects ofL-arginine shown in the experiments presentedhere took place at concentrations one order ofmagnitude below those attempted in trials witheither L-alanine or L-glutamine. As L-arginineconcentration increased to 20 mM, thereduction in absorptive capacity made evidentby the decrease in Lf] and JeJ is consistentwith vasoconstrictive effects linked to NOunder certain circumstances.
Perfusion of ORS with L-arginine had amodest proabsorptive role in regard to glucoseat concentrations of the amino acid generallyhigher than those altering water and sodiumabsorption, particularly in perfusions with 60mM sodium. As both the 90 mM and 60 mMsodium ORS contained 111 mM glucose(20 g/l), the overriding proportion of thetransport is likely to occur by solvent drag.Therefore, this result is compatible withglucose entry into the enterocyte after water
606
1..I...Ii
:P, ::,..-% Wl,N. ". ,
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from

L-arginine in oral rehydration solutions
movement with rapid removal into thecirculation.Calcium is normally secreted into the
intestinal lumen during perfusions withsolutions which do not contain this element.Whereas the presence of citrate in the ORS inour study may impair calcium absorption, itdoes not alter secretion of the cation.34 Insolutions which omit calcium, such as thoseused in these experiments, a leakage of thiscation into the lumen as sodium enters thecell is therefore expected, and consistentwith sodium-calcium exchange across mem-branes.35 36 This was clearly the case here,although no correlation was found betweenwater or sodium absorption and calciumsecretion. Osmolality may also play a part inthis process, as secretory rates of calcium werehigher in experiments with 60 mM sodiumthan with 90 mM sodium. In view of theseresults it cannot be argued that a calcium-sodium exchange is putatively modulated byNO.The present experimental model has been
extensively used in previous investigationsintended to compare the effectiveness of ORSwith variable concentrations of solutes,osmolality, or additives, with the ultimategoal of improving their effectiveness insodium transport and water retention inhumans.27 29 30 3 Positive ORS studies onrodents38 have subsequently been applied toclinical trials, especially in infantile diarrhoeaof various aetiologies. In a clinical study,39 theORS which best reduced stool volume ininfants and children with diarrhoea was thesame which produced the highest rates ofwaterabsorption in the rat. Similarly, the greatestdecrease in sodium losses in the faecesparalleled maximal sodium experimental ab-sorption rates in the experimental model.
We thank Mr Jeffrey Moyse for his assistance in the preparationof photographic material. This work was supported in part bya National Institutes of Health (USA) grant HD29255.
1 Marletta MA. Nitric oxide: biosynthesis and biologicalsignificance. Trends Biol Sci 1989; 14: 488-92.
2 Anggard E. Nitric oxide: mediator, murderer and medicine.Lancet 1994; 343: 1199-206.
3 Ignarro U. Biological actions and properties ofendothelium-derived nitric oxide formed and releasedfrom artery and vein. Circ Res 1989; 65: 1-2 1.
4 Stark ME, Szurszewski JH. Role of nitric oxide ingastrointestinal and hepatic function and disease.Gastroenterology 1992; 103: 1928-49.
5 Mayer B. Regulation of nitric oxide synthase and solubleguaninyl cyclase. Cell Biochem Funct 1994; 12: 166-77.
6 Hutcheson IR, Whittle BJR, Boughton-Smith NK. Role ofnitric oxide in maintaining vascular integrity inendotoxin-induced acute intestinal damage in the rat. BrJ7Pharmacol 1990; 101: 815-20.
7 Raul F, Galluser M, Schleiffer R, Gosse F, Hasselman M,Seiler N. Beneficial effect of L-arginine on intestinalepithelial restitution after ischemic damage in rats.Digestion 1995; 56: 400-5.
8 Alican I, Kubes P. A critical role for nitric oxide in intestinalbarrier function and dysfunction. Am 7 Physiol 1996; 270:G225-37.
9 MacNaughton WK. Nitric oxide-donating compoundsstimulate electrolyte transport in the guinea pig intestinein vitro. LifeSci 1993; 53: 585-93.
10 Barry MK, Aloisi JD, Pickering SP, Yeo CJ. Nitric oxidemodulates water and electrolyte transport in the ileum.Ann Surg 1994; 219: 382-8.
11 Turvill JL, Farthing MJG. Nitric oxide (NO) mediatescholera toxin (CT)-induced secretion in rat smallintestine in vivo. Gastroenterology 1996; 110: A368.
12 Hogaboam CM, Jacobson K, Collins SM, BlennerhassetMG. The selective beneficial effects of nitric oxideinhibition in experimental colitis. Am J Physiol 1995; 268:G673-84.
13 Tamai H, Gaginella TS. Direct evidence for nitric oxidestimulation of electrolyte secretion in the rat colon. FreeRadical Research Communications 1993; 19: 229-39.
14 Cynober L, Le Boucher J, Vasson M-P. Argininemetabolism in mammals. Nutr Biochem 1995; 6: 402-13.
15 Kerwin JF Jr, Lancaster JR Jr, Feldman PL. Nitric oxide:a new paradigm for second messengers. J Med Chem1995; 38: 4343-62.
16 Moncada S, Higgs A. The L-arginine-nitric oxide pathway.NEnglJ3Med 1993; 329: 2002-12.
17 Mourad FH, O'Donnell LJD, Andre EA, Bearcroft CP,Clark ML, Farthing MJG. Effect of local and systemicadministration of L-arginine and nitro L-arginine methylester (L-NAME) on water transport and histologicchanges in rat jejunum. Gastroenterology 1995; 108:A309.
18 Avery ME, Snyder JD. Oral therapy for acute diarrhea. Theunderused simple solution. N Engl J7 Med 1990; 323:891-4.
19 Sarker SA, Majid N, Mahalanabis D. Alanine- and glucose-based hypo-osmolar oral rehydration solution in infantswith persistent diarrhoea: a controlled trial. Acta PaediatrScand 1995; 84: 775-80.
20 Bhan MK, Mahalanabis D, Fontaine 0, Pierce NK. Clinicaltrials of improved oral rehydration salt formulations: areview. Bull WHO 1994; 72: 945-55.
21 Goldberg ED, Saltzman JR. Rice inhibits intestinalsecretions. Nutr Rev 1996; 54: 36-7.
22 Go JT, Harper RG, Sia CG, Teichberg S, Wapnir RA. Oralrehydration solutions: increased water and sodiumabsorption by addition of a viscosity-enhancing agent ina rat model of chronic osmotic diarrhea. J PediatrGastroenterol Nutr 1994; 19: 410-6.
23 Zar JH. Biostatistical analysis. 2nd edn. Englewood Cliffs,NJ: Prentice-Hall, 1984: 185-205.
24 Cuzick J. A Wilcoxon-type test for trend. Stat Med 1985;4: 87-90.
25 Mourad FH, Andre EA, O'Donnell LJD, Bearcroft CP,Clark ML, Farthing MJG. L-arginine and intestinal watersecretion: is nitric oxide the missing link? Gastroenterology1994; 106: A256.
26 Mourad FH, O'Donnell LJD, Andre EA, Bearcroft CP,Owen RA, Clark ML, Farthing MJG. L-Arginine, nitricoxide, and intestinal secretion: studies in rat jejunum invivo. Gut 1996; 39: 539-44.
27 Lifshitz F, Wapnir RA. Oral hydration solutions:experimental optimization of water and sodiumabsorption.JPediatr 1985; 106: 383-9.
28 Gisolfi CV, Summers RW, Schedl HP, Bleiler TL. Intestinalwater absorption from select carbohydrate solutions inhumans. 7Appl Physiol 1992; 73: 2142-50.
29 Wapnir RA, Zdanowicz MM, Teichberg S, Lifshitz F. Oralhydration solutions in experimental osmotic diarrhea:enhancement by alanine and other amino acids andoligopeptides. Amj Clin Nutr 1988; 47: 84-90.
30 Wapnir RA, Zdanowicz MM, Teichberg S, Lifshitz F.Alanine stimulation of water and sodium absorption in amodel of secretory diarrhea. J Pediatr Gastroenterol Nutr1990; 10: 213-21.
31 Rhoads JM, Keku EO, Quinn J, Woosley J, Lecce J.L-glutamine stimulates jejunal sodium and chlorideabsorption in pig-rotavirus enteritis. Gastroenterology1991; 100: 683-99.
32 Bhan MK, Chea Woo E, Fontaine 0, Maulen-Radovan I,Pierce NF, Ribeiro H Jr. Multicentre evaluation ofreduced osmolality oral rehydration salts solution. Lancet1995; 345: 282-5.
33 Bhan MK, Sazawal S, Bhatnagar S, Bhandari N, Guha DK,Aggarwal SK. Glycine, glycyl-glycine and maltodextrinbased oral rehydration solution. Acta Paediatr Scand 1990;79: 518-26.
34 Rumenapf G, Schwill PO. The influence of citrate on theduodenal absorption of calcium in the rat. Calcif Tissue Int1988; 42: 326-30.
35 Donowitz M. Ca2l in the control of active intestinal Na andCl transport: involvement in neurohormonal action. AmJ3Physiol 1983; 245: G165-77.
36 Blaustein MP, Goldman WF, Fontana G, Krueger BK,Santiago EM, Steele TD, Weiss DN, Yarowski PJ.Physiological roles of the sodium-calcium exchanger innerve and muscle. Ann NYAcad Sci 1991; 639: 254-74.
37 Wapnir RA, Teichberg S, Go JT, Wingertzahn MA, HarperRG. Oral rehydration solutions: enhanced sodiumabsorption with gum arabic. Y Am Coll Nutr 1996; 15:377-82.
38 Wapnir RA, Litov RE, Zdanowicz MM, Lifshitz F.Improved water and sodium absorption from rice syrupsolids-based oral rehydration solutions in a rat animalmodel of osmotic diarrhea. JPediatr 1991; 118: S53-61.
39 Pizarro D, Posada G, Sandi L, Moran JR. Rice-based oralelectrolyte solutions for the management of infantilediarrhea. N EnglJ Med 1991; 324: 517-21.
607
on Decem
ber 23, 2021 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.5.602 on 1 May 1997. D
ownloaded from





![[PRODUCT LIS T] - IMPERIA LIFE SCIENCES · Pirenoxine Sodium Eye Drops Taurine Eye Drops . 13 DECONGESTANT Xylometazoline Nasal Spray DEHYDRATION TREATMENT Oral Rehydration Salts](https://img.pdfslide.net/doc/110x75/5d25d3b488c993b3788b9278/product-lis-t-imperia-life-pirenoxine-sodium-eye-drops-taurine-eye-drops.jpg)