Embed Size (px)
Citation preview
CASE REPORT
Intramuscular diffuse-type tenosynovial giant cell tumorof the deltoid muscle in a child
Seong Jong Yun & Su Yeon Hwang & Wook Jin &
Sung Jig Lim & So Young Park
Received: 9 October 2013 /Revised: 7 February 2014 /Accepted: 19 February 2014# ISS 2014
Abstract Tenosynovial giant cell tumors (GCTs) typicallyform in the joints or extra-articular soft tissues such as thetendon sheath, and are benign tumors that commonly occur inthe hands or wrists in the third to fifth decades of life.However, the diffuse type of extra-articular GCT arisingwithin muscle is a rare soft tissue tumor, especially in apediatric patient. In this report, we describe the magnet-ic resonance imaging and sonographic findings of a rarecase of intramuscular diffuse-type GCT in the deltoidmuscle of a 9-year-old boy.
Keywords Diffuse-type giant cell tumor . Child . Deltoidmuscle .Magnetic resonance imaging . Sonography
Introduction
Tenosynovial giant cell tumors (GCTs) are benign soft tissuetumors that arise from the synovium of the joints, bursae, andtendon sheath [1]. These tumors are classified into two forms:localized and diffuse (Fig. 1). Localized-type family of tumorscan be divided into intra-articular and extra-articular forms,
termed localized pigmented villonodular synovitis (PVNS)and GCTs of the tendon sheath, respectively. Diffuse-typefamily of tumors also can be divided into intra-articular andextra-articular forms, termed conventional PVNS and diffuse-type GCT, respectively [1, 2].
Localized-type tenosynovial GCTs are frequent, indolent,and arise from the synovium of the joint, bursa, or tendonsheath. In contrast, the less frequent diffuse-type tenosynovialGCTs are locally aggressive and commonly affect peri-articular soft tissue, but on rare occasions these lesions canbe intramuscular [1, 3]. The yearly incidence of diffuse-typetenosynovial GCTs is two per 1,000,000 in patients under theage of 40 with an equal gender distribution [2]. Extra-articulardiffuse-type GCT (Dt-GCT) for only 5∼15 % of all diffuse-type tenosynovial GCTs and pediatric cases are rare. More-over, Dt-GCTs are typically found in the lower extremities,not in the upper extremities [3]. Despite the rarity of intramus-cular Dt-GCTs, it is important to know that they infiltratesurrounding the soft tissue and have a high recurrence rate[1], requiring complete surgical resection and follow-up.
We report magnetic resonance imaging (MRI) and sono-graphic findings of a rare case of intramuscular Dt-GCTof thedeltoid muscle in a 9-year-old boy. We also discuss the sig-nificance of identifying this benign soft tissue tumor and theimaging differential diagnosis.
Case report
A 9-year-old boy visited our institution with a right shouldermass first noted 6 months prior to presentation. Upon physicalexamination, it appeared to be a non-tender soft tissue massmeasuring about 2.0×6.0 cm in size. The mass was fixed tothe muscle. The patient had no prior history of trauma, includ-ing surgery.
S. J. YunDepartment of Radiology, Kyung Hee University Hospital atGangdong, Kyung Hee University School of Medicine, 149Sangil-dong, Kangdong-gu, Seoul 134-727, South Korea
S. Y. Hwang :W. Jin (*) : S. Y. ParkDepartment of Radiology, Kyung Hee University Hospital atGangdong, 149 Sangil-dong, Kangdong-gu, Seoul 134-727, SouthKoreae-mail: [email protected]
S. J. LimDepartment of Pathology, Kyung Hee University Hospital atGangdong, 149 Sangil-dong, Kangdong-gu, Seoul 134-727, SouthKorea
Skeletal RadiolDOI 10.1007/s00256-014-1854-1
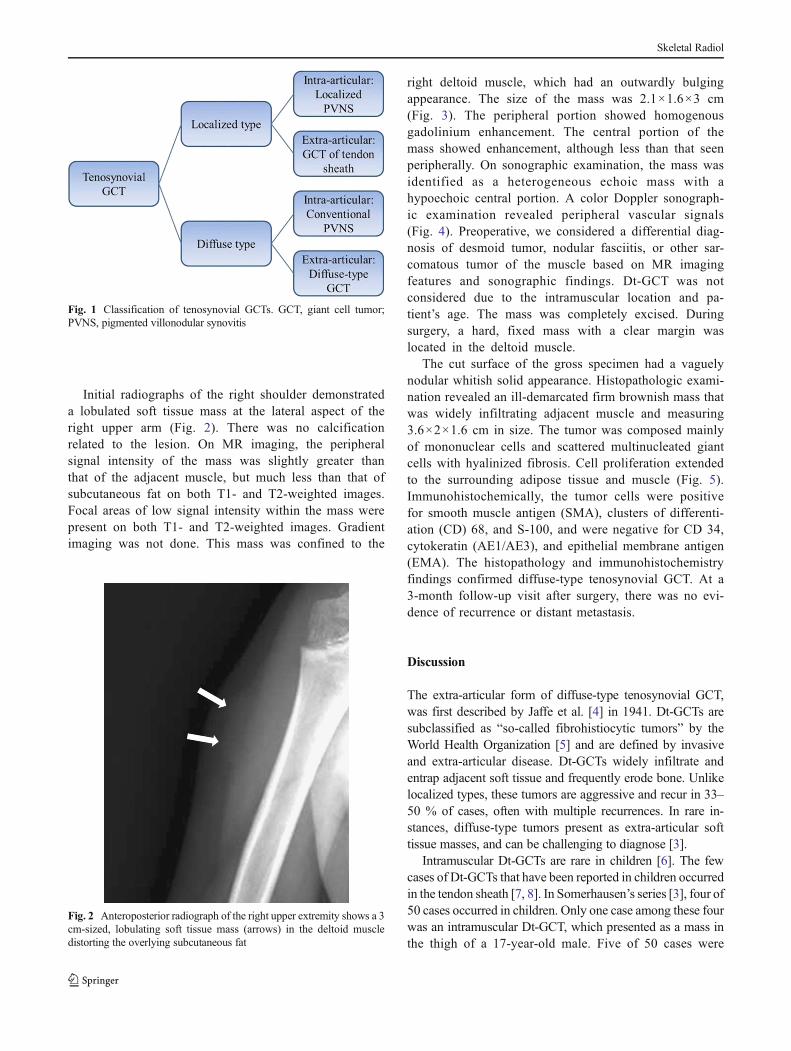
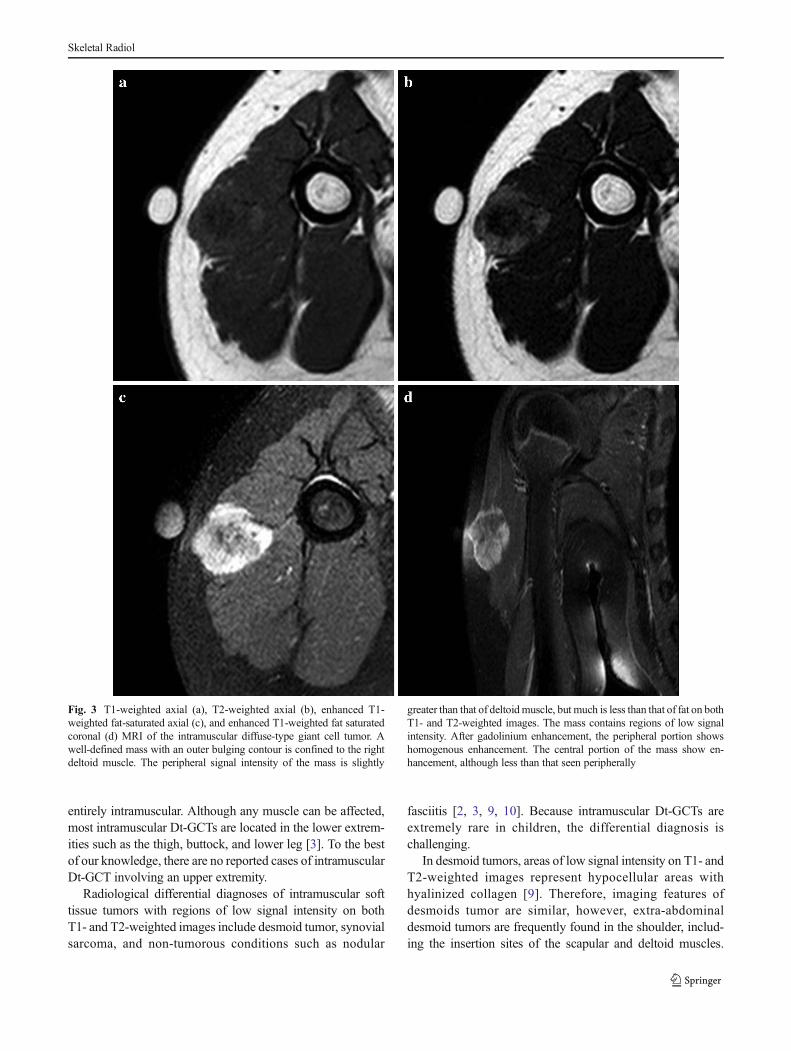
Initial radiographs of the right shoulder demonstrateda lobulated soft tissue mass at the lateral aspect of theright upper arm (Fig. 2). There was no calcificationrelated to the lesion. On MR imaging, the peripheralsignal intensity of the mass was slightly greater thanthat of the adjacent muscle, but much less than that ofsubcutaneous fat on both T1- and T2-weighted images.Focal areas of low signal intensity within the mass werepresent on both T1- and T2-weighted images. Gradientimaging was not done. This mass was confined to the
right deltoid muscle, which had an outwardly bulgingappearance. The size of the mass was 2.1×1.6×3 cm(Fig. 3). The peripheral portion showed homogenousgadolinium enhancement. The central portion of themass showed enhancement, although less than that seenperipherally. On sonographic examination, the mass wasidentified as a heterogeneous echoic mass with ahypoechoic central portion. A color Doppler sonograph-ic examination revealed peripheral vascular signals(Fig. 4). Preoperative, we considered a differential diag-nosis of desmoid tumor, nodular fasciitis, or other sar-comatous tumor of the muscle based on MR imagingfeatures and sonographic findings. Dt-GCT was notconsidered due to the intramuscular location and pa-tient’s age. The mass was completely excised. Duringsurgery, a hard, fixed mass with a clear margin waslocated in the deltoid muscle.
The cut surface of the gross specimen had a vaguelynodular whitish solid appearance. Histopathologic exami-nation revealed an ill-demarcated firm brownish mass thatwas widely infiltrating adjacent muscle and measuring3.6×2×1.6 cm in size. The tumor was composed mainlyof mononuclear cells and scattered multinucleated giantcells with hyalinized fibrosis. Cell proliferation extendedto the surrounding adipose tissue and muscle (Fig. 5).Immunohistochemically, the tumor cells were positivefor smooth muscle antigen (SMA), clusters of differenti-ation (CD) 68, and S-100, and were negative for CD 34,cytokeratin (AE1/AE3), and epithelial membrane antigen(EMA). The histopathology and immunohistochemistryfindings confirmed diffuse-type tenosynovial GCT. At a3-month follow-up visit after surgery, there was no evi-dence of recurrence or distant metastasis.
Discussion
The extra-articular form of diffuse-type tenosynovial GCT,was first described by Jaffe et al. [4] in 1941. Dt-GCTs aresubclassified as “so-called fibrohistiocytic tumors” by theWorld Health Organization [5] and are defined by invasiveand extra-articular disease. Dt-GCTs widely infiltrate andentrap adjacent soft tissue and frequently erode bone. Unlikelocalized types, these tumors are aggressive and recur in 33–50 % of cases, often with multiple recurrences. In rare in-stances, diffuse-type tumors present as extra-articular softtissue masses, and can be challenging to diagnose [3].
Intramuscular Dt-GCTs are rare in children [6]. The fewcases of Dt-GCTs that have been reported in children occurredin the tendon sheath [7, 8]. In Somerhausen’s series [3], four of50 cases occurred in children. Only one case among these fourwas an intramuscular Dt-GCT, which presented as a mass inthe thigh of a 17-year-old male. Five of 50 cases were
Fig. 1 Classification of tenosynovial GCTs. GCT, giant cell tumor;PVNS, pigmented villonodular synovitis
Fig. 2 Anteroposterior radiograph of the right upper extremity shows a 3cm-sized, lobulating soft tissue mass (arrows) in the deltoid muscledistorting the overlying subcutaneous fat
Skeletal Radiol
entirely intramuscular. Although any muscle can be affected,most intramuscular Dt-GCTs are located in the lower extrem-ities such as the thigh, buttock, and lower leg [3]. To the bestof our knowledge, there are no reported cases of intramuscularDt-GCT involving an upper extremity.
Radiological differential diagnoses of intramuscular softtissue tumors with regions of low signal intensity on bothT1- and T2-weighted images include desmoid tumor, synovialsarcoma, and non-tumorous conditions such as nodular
fasciitis [2, 3, 9, 10]. Because intramuscular Dt-GCTs areextremely rare in children, the differential diagnosis ischallenging.
In desmoid tumors, areas of low signal intensity on T1- andT2-weighted images represent hypocellular areas withhyalinized collagen [9]. Therefore, imaging features ofdesmoids tumor are similar, however, extra-abdominaldesmoid tumors are frequently found in the shoulder, includ-ing the insertion sites of the scapular and deltoid muscles.
Fig. 3 T1-weighted axial (a), T2-weighted axial (b), enhanced T1-weighted fat-saturated axial (c), and enhanced T1-weighted fat saturatedcoronal (d) MRI of the intramuscular diffuse-type giant cell tumor. Awell-defined mass with an outer bulging contour is confined to the rightdeltoid muscle. The peripheral signal intensity of the mass is slightly
greater than that of deltoidmuscle, but much is less than that of fat on bothT1- and T2-weighted images. The mass contains regions of low signalintensity. After gadolinium enhancement, the peripheral portion showshomogenous enhancement. The central portion of the mass show en-hancement, although less than that seen peripherally
Skeletal Radiol
Desmoid tumors typically present in young adults, with a fewcases reported in children [11]. Intramuscular nodular fasciitisis very rare in the pediatric population. Furthermore, nodularfasciitis lesions typically involve the head and neck in chil-dren. It typically has an increased signal intensity on T2-weighted images [10]. Synovial sarcomas are the most com-mon non-rhabdomyosarcomatous soft tissue sarcomas in chil-dren. Synovial sarcomas might mimic GCT because thesetumors usually have heterogeneous signal intensity on T2-weighted images due to intra-tumoral hemorrhage. Character-istic findings including the presence of soft tissue calcifica-tions, fluid-fluid levels, and hemorrhage are helpful for diag-nosis of synovial sarcoma rather than GCT [12].
MRI findings of Dt-GCT include prominent low signalintensity on T2-weighted images and a “blooming” artifactdue to abundant hemosiderin on gradient-echo images; thesefindings are nearly pathognomonic of Dt-GCT [13, 14]. Mi-croscopically, Dt-GCTs are identical to other forms of
tenosynovial GCTs in terms of the underlying cell population,comprising large histiocytoid cells with abundant eosinophiliccytoplasm and eccentric vesicular nuclei, smaller mononucle-ar stromal cells with oval or reniform nuclei, osteoclast-likegiant cells, and xanthoma cells. Most Dt-GCTs are infiltrative,and cystic changes and multi-lobulation are observed in somecases [1, 3]. These masses are slow-growing, painless lesionsthat can be treated with surgical excision. Despite the benignnature of these tumors, the clinical outcomes of Dt-GCTs areunclear because of their rarity. The recurrence rate of intra-muscular Dt-GCTs is low compared to those of other types of
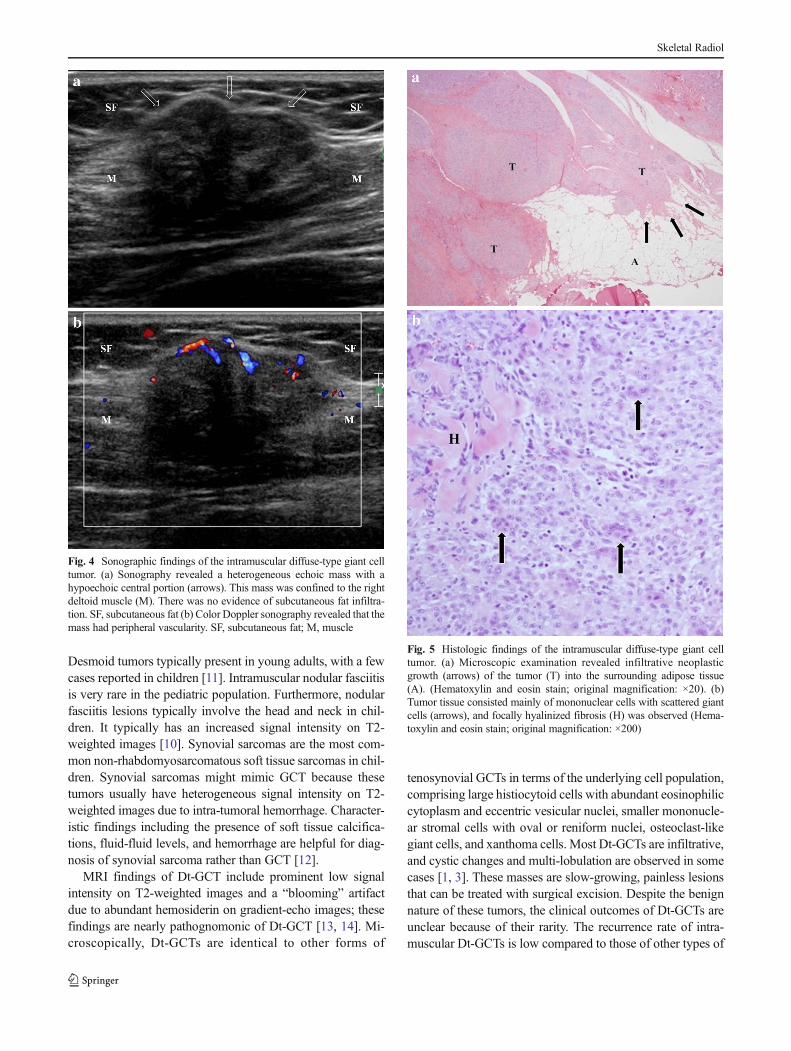
Fig. 4 Sonographic findings of the intramuscular diffuse-type giant celltumor. (a) Sonography revealed a heterogeneous echoic mass with ahypoechoic central portion (arrows). This mass was confined to the rightdeltoid muscle (M). There was no evidence of subcutaneous fat infiltra-tion. SF, subcutaneous fat (b) Color Doppler sonography revealed that themass had peripheral vascularity. SF, subcutaneous fat; M, muscle
Fig. 5 Histologic findings of the intramuscular diffuse-type giant celltumor. (a) Microscopic examination revealed infiltrative neoplasticgrowth (arrows) of the tumor (T) into the surrounding adipose tissue(A). (Hematoxylin and eosin stain; original magnification: ×20). (b)Tumor tissue consisted mainly of mononuclear cells with scattered giantcells (arrows), and focally hyalinized fibrosis (H) was observed (Hema-toxylin and eosin stain; original magnification: ×200)
Skeletal Radiol

intra-articular diffuse-type tenosynovial GCTs, because it ispossible to completely excise the mass [3].
In summary, we reported a case of intramuscular Dt-GCTin a child. Because of the unusual location and the patient’sage, diagnosis based on imaging findings was challenging.The present case may be instructive for differential diagnosesof primary intramuscular tumors.
References
1. Lucas DR. Tenosynovial giant cell tumor: case report and review.Arch Pathol Lab Med. 2012;136(8):901–6.
2. van der Heijden L, Gibbons CL, Dijkstra PD, et al. Themanagement of diffuse-type giant cell tumour (pigmentedvillonodular synovitis) and giant cell tumour of tendon sheath(nodular tenosynovitis). J Bone Joint Surg Br. 2012;94(7):882–8.
3. Somerhausen NSA, Fletcher CD. Diffuse-type giant cell tumor:clinicopathologic and immunohistochemical analysis of 50 caseswith extraarticular disease. Am J Surg Pathol. 2000;24(4):479–92.
4. Jaffe HL, Lichtenstein L, Sutro CJ. Pigmented villonodular synovitis,bursitis and tenosynovitis. Arch Pathol. 1941;31(3):731–65.
5. Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. WHOclassification of tumours of soft tissue and bone. 4th ed. Lyon:IARC; 2013.
6. Oliveira AM, Dei Tos AP, Fletcher CD, Nascimento AG. Primarygiant cell tumor of soft tissues: a study of 22 cases. Am J Surg Pathol.2000;24(2):248–56.
7. Hulse N, Watson SJ. Giant cell tumour of tendon sheath in a child: acase report. Hand Surg. 2005;10(1):97–100.
8. Gholve PA, Hosalkar HS, Kreiger PA, Dormans JP. Giant cell tumorof tendon sheath: largest single series in children. J Pediatr Orthop.2007;27(1):67–74.
9. Vandevenne J, De Schepper A, De Beuckeleer L, et al. New conceptsin understanding evolution of desmoid tumors: MR imaging of 30lesions. Eur Radiol. 1997;7(7):1013–9.
10. Mazura JC, Matrai C, Spigland N, Brill PW, Kovanlikaya A.Intramuscular nodular fasciitis of the rectus abdominis muscle in an11-year-old girl. Skeletal Radiol. 2013;42(1):147–50.
11. Kransdorf MJ, Jelinek JS, Moser Jr RP, et al. Magnetic resonanceappearance of fibromatosis. Skeletal Radiol. 1990;19(7):495–9.
12. Stein-Wexler R. Pediatric soft tissue sarcomas. Semin Ultrasound CTMR. 2011;32(5):470–88.
13. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, FlemmingDJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008;28(5):1493–518.
14. Sanghvi D, Purandare N, Jambhekar N, Agarwal M, Agarwal A.Diffuse-type giant cell tumor of the subcutaneous thigh. SkeletalRadiol. 2007;36(4):327–30.
Skeletal Radiol