Embed Size (px)
Citation preview
AUDIT
doi: 10.1111/j.1478-5153.2012.00514.x
Introducing delirium screeningin a cardiothoracic critical care unitLiz Shaughnessy
ABSTRACTAim: To share an experience of introducing Delirium scoring into a Cardiothoracic Critical Care Unit and the lessons learnt.Background: Delirium has serious consequences leading to increased length of stay in hospital, the possible development of dementia withthe associated need for long-term care and even death. It is therefore vital that the Critical Care nurses are able to prevent, recognize andmanage delirium.Data sources and methods: 108 patients who were admitted over a 6 week period were audited and their delirium score, documentationand treatment plans were reviewed.Results: 21% of patients experienced delirium during their stay on Cardiothoracic Critical Care and hypoactive delirium was the mostprevalent subtype. Of the three patients who stayed more than 20 days on critical care all suffered with delirium at some point during theirstay. Documentation of delirium by both Nursing and Medical staff occurred in less than 50% of patients.Conclusions: The introduction of delirium scoring and audit of its practice has highlighted the incidence of delirium in critically ill patientsand has resulted in;
• Improved quality of care by development of a delirium care bundle• Improved recognition of delirium• Instigation of practices to prevent and treat delirium
Key words: Critical care nursing • Clinical audit
INTRODUCTIONDelirium in intensive care unit (ICU) patients is not newor unfamiliar although it has been known by differentterms for many years such as ICU psychosis or acuteconfusional state. However, the prevention, recogni-tion and treatment of delirium has been more recentlyhighlighted by work carried out by Ely (2004), Page(2009) and a recent National Institute for Health andClinical Excellence (NICE) publication (2010) whichemphasized the long-term effects delirium can haveon its sufferers. As nurses in Critical Care, we are wellaware of multi-organ failure and the importance ofmonitoring and acting on our findings. We diligentlymonitor urine output and are aware of its significanceas an indicator of renal function but the importanceof delirium as an indicator of brain dysfunction has
Author: L Shaughnessy, RGN, ENB 100, ENB998, Diploma in Nursing,PGCE, Practice Teacher, Clinical Nurse Educator, Cardiothoracic CriticalCare, Essex Cardiothoracic Centre, Basildon Hospital, Basildon, Essex SS165NL, UKAddress for correspondence: L Shaughnessy, Cardiothoracic CriticalCare, Essex Cardiothoracic Centre, Basildon Hospital, Nethermayne,Basildon, Essex SS16 5NL, UKE-mail: [email protected]
been misunderstood and the treatment of deliriumoverlooked.
Delirium is an acute confusional state characterizedby fluctuating mental status, inattention and eitherdisorganized thinking or altered level of consciousnessWalters (2008) (Figure 1). It can be classified into sub-types of hypermotoric, hypomotoric and can also beenseen as a mixture of the two. The hyperactive deliriouspatient is familiar to all Critical Care Nurses, the patientwho self extubates, removes lines and becomes com-bative. However, identifying the hypoactive patientmay be more difficult and requires a screening toolas the significance of identifying these patients cannotbe underestimated. A hypomotoric delirious patientmay sit quietly for some time but go on to develophypermotoric delirium which can be far more difficultto manage, thus making early recognition important.Of even more significance are the findings of Ely (2004)that hypomotoric delirium is far more prevalent in crit-ical care and is associated with worse outcomes thanthose who suffer hypermotoric delirium. Identifyingthe hypomotoric delirious patient is difficult withoutan adequate screening tool as the hypomotoric suf-ferer may appear withdrawn, exhausted or apathetic
© 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses 1

Introducing delirium screening in a cardiothoracic critical care unit
and
and/or
1. Acute onset of mental status changesor a fluctuating course
2. Inattention
3. Disorganised Thinking
4. Altered level ofconsciousness
Figure 1 Confusion Assessment Method for ICU (CAM-ICU).
and may go unrecognized. Therefore as highlighted byGirard et al. (2008) and Page (2009) routine 12 hourlydelirium assessment is essential in the detection of thissub-group.
NICE (2010) highlight the serious consequencesdelirium can have leading to increased length of stay inhospital, the development of dementia with the asso-ciated need for long-term care and even death. It istherefore vital that the Critical Care nurse is able toprevent, recognize and manage delirium.
Identifying both predisposing and precipitating fac-tors associated with delirium and also being aware ofpreventative measures (Table 1) will allow the Criti-cal Care Nurse to plan and adapt care and also allowthe implementation of interventions to minimize theimpact a stay in Critical Care can have on cognitivefunction.
BACKGROUNDIn February 2010, delirium scoring was introducedonto the Cardiothoracic Critical Care Unit using theConfusion Assessment Method–ICU score (CAM-ICU) as recommended by NICE (2010). The CAM-ICUscore is a bedside test which takes 1–2 min to under-take and has been shown to be a very reliable methodof detecting delirium in both self-ventilating and intu-bated ICU patients Ely (2004).
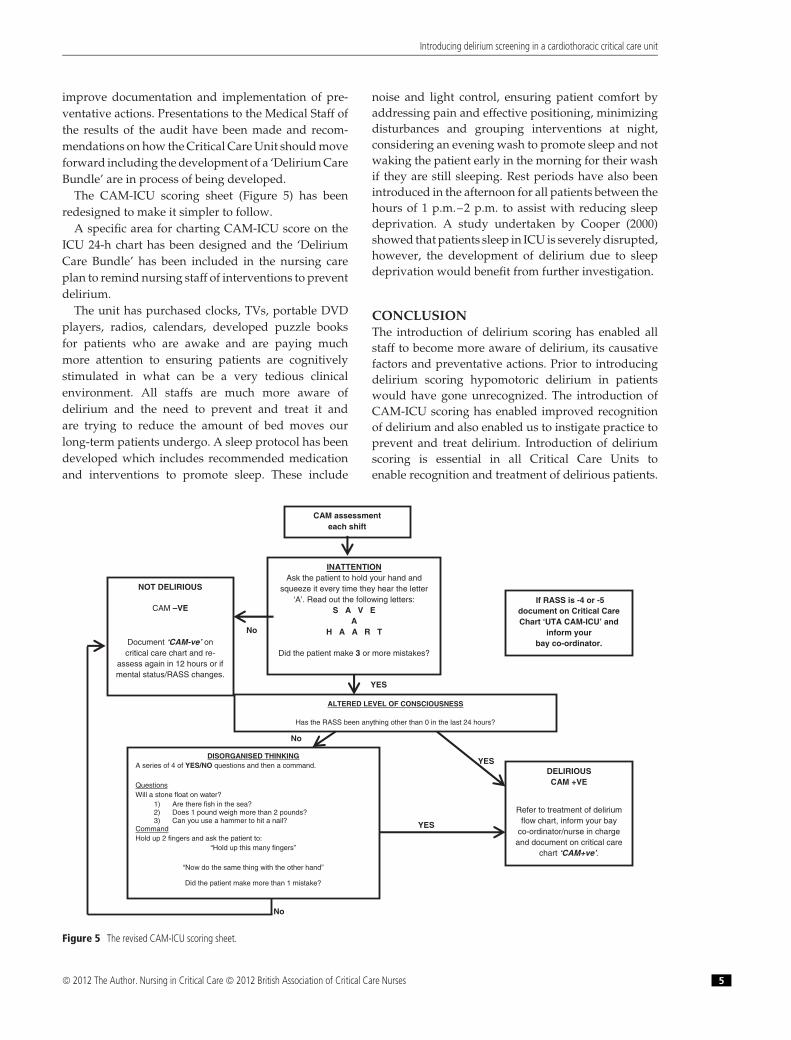
The CAM-ICU comprises of a test for inattention,asking a patient to squeeze the clinicians hand on theletter ‘A’ when reading a series of 10 letters, the clinicianthen reads out ‘SAVEAHAART’. The patient is allowedtwo mistakes. The next part of the CAM-ICU looks fordisorganized thinking by asking four simple yes/noquestions followed by a command, they are allowedone mistake. The patient is delirious if they have inat-tention and either disorganized thinking or an alteredlevel of consciousness. Conscious level can be assessedin a number of ways, the Richmond Agitation SedationScore (RASS) is used on the Cardiothoracic CriticalCare and a score of anything but alert is classed as analtered level of consciousness. If delirious the patient istermed CAM positive. The CAM-ICU score does not,
Table 1 Predisposing and Precipitating factors associated with Delirium (Nice2010)
Predisposing factorsAge > 65 years oldPre-existing cognitive impairment
Severe illnessCurrent hip fracturePrecipitating factorsSurgeryDehydrationConstipationHypoxiaInfectionImmobilityPainPoor nutritionSleep deprivationNeurological diseaseDeliriogenic drugsPreventative measuresProvide clockOrientationMobilizeAdequate nutrition/hydrationAddress constipationEncourage sleepDrug overhaulAddress hearing and sight impairmentAddress painCognitively stimulating activities
however, identify patient’s type of delirium but this canbe distinguished by the patient’s level of consciousness.
The introduction of a change in practice of thislevel requires determination and it was realized itwas going to be challenging. To enable this change inpractice posters were positioned around the unit withwords such as delirium, inattention and disorganizedthinking as recommended by Page (2010).
The subject was introduced on Team Days focusingon delirium, its prevention, treatment and the CAM-ICU scoring tool. Videos of the CAM-ICU score beingundertaken were shown and then staffs were askedto assess each other. Each member of staff received acopy of the NICE guidance (2010) and then a copy ofthe CAM-ICU score was positioned at all bed areasfor reference. A flowchart was designed to aid staffin identifying factors which could precipitate delir-ium and ways of preventing it. Included were factorswhich the medical staff would need to consider anda guideline for drug administration should this beindicated (Figure 2) (Borthwick et al. 2006, Hua et al.2006, Kalisvaart et al. 2005, Pun and Ely 2007). Thiswas approved by the Lead ICU Anaesthetist and ICUPharmacist.
2 © 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses
Introducing delirium screening in a cardiothoracic critical care unit
CAM- ICU ASSESSMENT EACH SHIFT
CAM NEGATIVE
CAM POSITIVE
SUPPORTIVE PREVENTATIVE MEASURES
• Re-orientate• Ensure Hydration• Assess/Manage Pain• Address Constipation• Mobilise• Reduce Noise• Familiar Nurse• Minimise Bed Moves• Address Sensory Impairment• Promote Sleep• Use orientating Stimuli• Remove Non-essential Invasive • Equipment
RASS -3 TO 0HYPOMOTORIC
RASS +1 OR +2HYPERMOTORIC
RASS +3 OR +4SEVERE
HYPERMOTORIC
CONSIDER REGULAR HALOPERIDOL
CONSIDER REGULARHALOPERIDOL
CONSIDER INITIALDOSE OF MIDAZOLAM
THEN REGULARHALOPERIDOL
*Consider oral Olanzapine OD as an alternative to Haloperidol in those patients with known Parkinson’s Disease or Dementia or if no response or adverse reactions to Haloperidol.***Refer to Management of Acute Alcohol Withdrawal and Wernicke’s Encephalopathy Protocol.**** Consider Nicotine patch.
DELIRIUM FLOWCHART
MEDICAL CONSIDERATIONS CONTRIBUTING TO DELIRIUM• Drug Overhaul
RanitidineBenzodiazepinesAntidepressantsOpioidsSteroidsPenicillins
• Infection• Renal Failure• Hypoxia• Withdrawal
Alcohol *** Tobacco ****Benzodiazepines
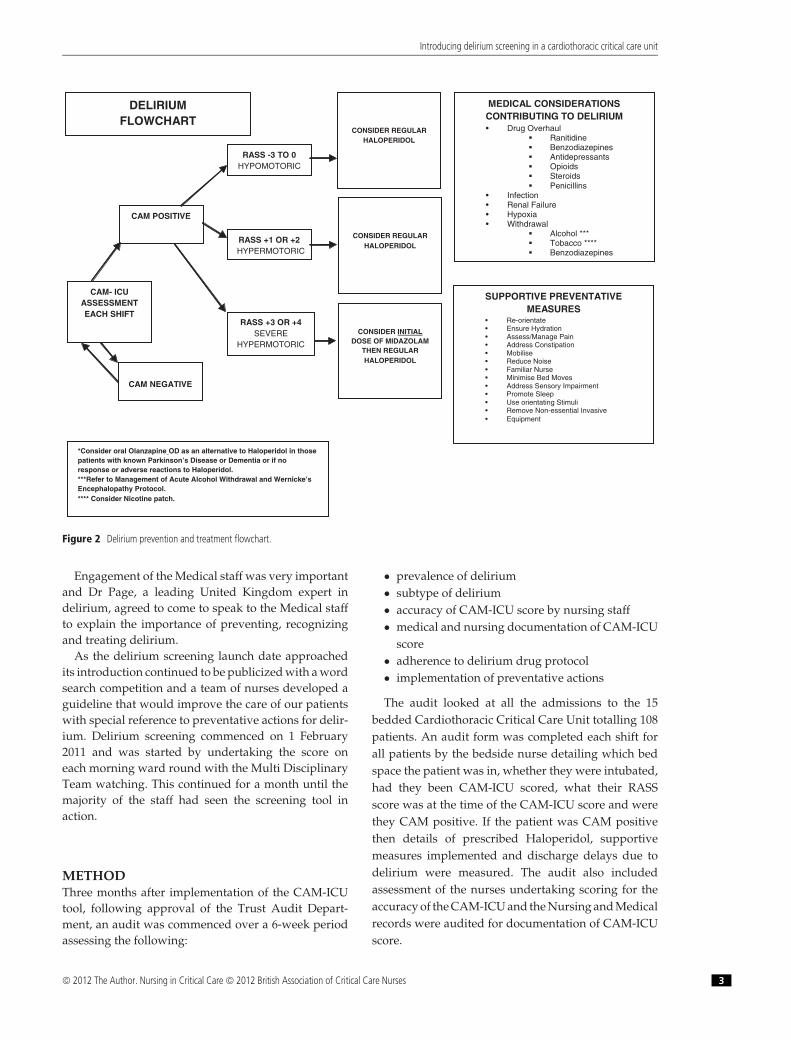
Figure 2 Delirium prevention and treatment flowchart.
Engagement of the Medical staff was very importantand Dr Page, a leading United Kingdom expert indelirium, agreed to come to speak to the Medical staffto explain the importance of preventing, recognizingand treating delirium.
As the delirium screening launch date approachedits introduction continued to be publicized with a wordsearch competition and a team of nurses developed aguideline that would improve the care of our patientswith special reference to preventative actions for delir-ium. Delirium screening commenced on 1 February2011 and was started by undertaking the score oneach morning ward round with the Multi DisciplinaryTeam watching. This continued for a month until themajority of the staff had seen the screening tool inaction.
METHODThree months after implementation of the CAM-ICUtool, following approval of the Trust Audit Depart-ment, an audit was commenced over a 6-week periodassessing the following:
• prevalence of delirium• subtype of delirium• accuracy of CAM-ICU score by nursing staff• medical and nursing documentation of CAM-ICU
score• adherence to delirium drug protocol• implementation of preventative actions
The audit looked at all the admissions to the 15bedded Cardiothoracic Critical Care Unit totalling 108patients. An audit form was completed each shift forall patients by the bedside nurse detailing which bedspace the patient was in, whether they were intubated,had they been CAM-ICU scored, what their RASSscore was at the time of the CAM-ICU score and werethey CAM positive. If the patient was CAM positivethen details of prescribed Haloperidol, supportivemeasures implemented and discharge delays due todelirium were measured. The audit also includedassessment of the nurses undertaking scoring for theaccuracy of the CAM-ICU and the Nursing and Medicalrecords were audited for documentation of CAM-ICUscore.
© 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses 3
Introducing delirium screening in a cardiothoracic critical care unit
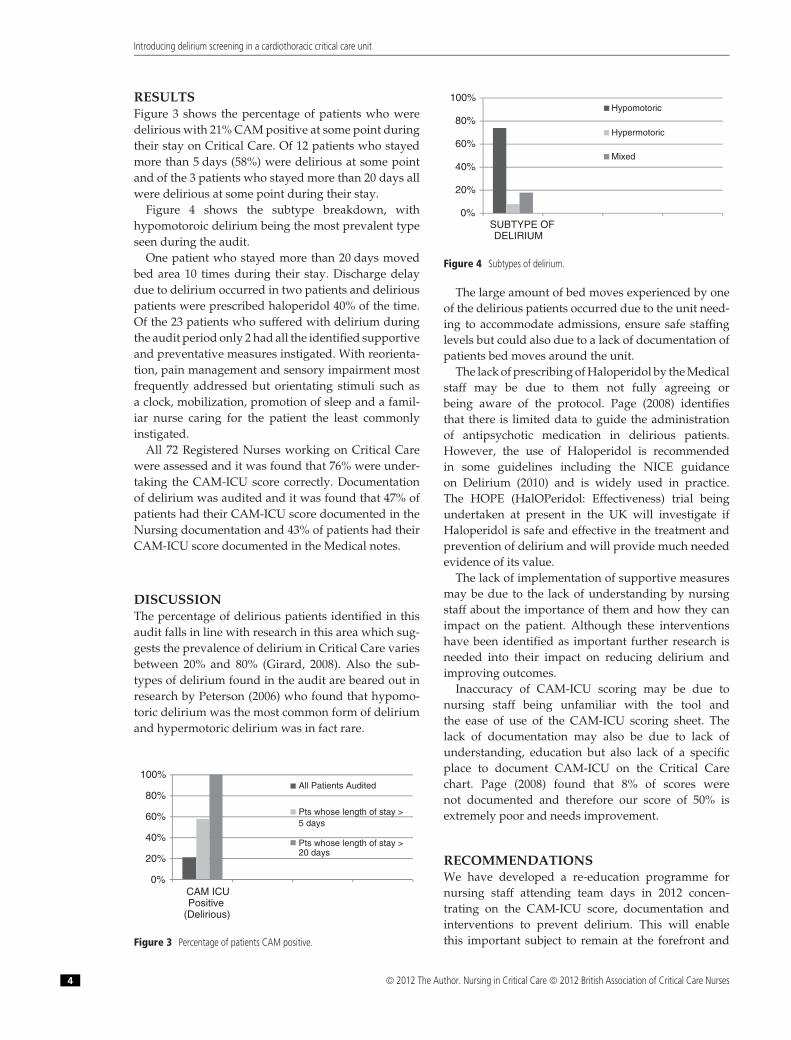
RESULTSFigure 3 shows the percentage of patients who weredelirious with 21% CAM positive at some point duringtheir stay on Critical Care. Of 12 patients who stayedmore than 5 days (58%) were delirious at some pointand of the 3 patients who stayed more than 20 days allwere delirious at some point during their stay.
Figure 4 shows the subtype breakdown, withhypomotoroic delirium being the most prevalent typeseen during the audit.
One patient who stayed more than 20 days movedbed area 10 times during their stay. Discharge delaydue to delirium occurred in two patients and deliriouspatients were prescribed haloperidol 40% of the time.Of the 23 patients who suffered with delirium duringthe audit period only 2 had all the identified supportiveand preventative measures instigated. With reorienta-tion, pain management and sensory impairment mostfrequently addressed but orientating stimuli such asa clock, mobilization, promotion of sleep and a famil-iar nurse caring for the patient the least commonlyinstigated.
All 72 Registered Nurses working on Critical Carewere assessed and it was found that 76% were under-taking the CAM-ICU score correctly. Documentationof delirium was audited and it was found that 47% ofpatients had their CAM-ICU score documented in theNursing documentation and 43% of patients had theirCAM-ICU score documented in the Medical notes.
DISCUSSIONThe percentage of delirious patients identified in thisaudit falls in line with research in this area which sug-gests the prevalence of delirium in Critical Care variesbetween 20% and 80% (Girard, 2008). Also the sub-types of delirium found in the audit are beared out inresearch by Peterson (2006) who found that hypomo-toric delirium was the most common form of deliriumand hypermotoric delirium was in fact rare.
0%
20%
40%
60%
80%
100%
CAM ICUPositive
(Delirious)
All Patients Audited
Pts whose length of stay >5 days
Pts whose length of stay >20 days
Figure 3 Percentage of patients CAM positive.
0%
20%
40%
60%
80%
100%
SUBTYPE OFDELIRIUM
Hypomotoric
Hypermotoric
Mixed
Figure 4 Subtypes of delirium.
The large amount of bed moves experienced by oneof the delirious patients occurred due to the unit need-ing to accommodate admissions, ensure safe staffinglevels but could also due to a lack of documentation ofpatients bed moves around the unit.
The lack of prescribing of Haloperidol by the Medicalstaff may be due to them not fully agreeing orbeing aware of the protocol. Page (2008) identifiesthat there is limited data to guide the administrationof antipsychotic medication in delirious patients.However, the use of Haloperidol is recommendedin some guidelines including the NICE guidanceon Delirium (2010) and is widely used in practice.The HOPE (HalOPeridol: Effectiveness) trial beingundertaken at present in the UK will investigate ifHaloperidol is safe and effective in the treatment andprevention of delirium and will provide much neededevidence of its value.
The lack of implementation of supportive measuresmay be due to the lack of understanding by nursingstaff about the importance of them and how they canimpact on the patient. Although these interventionshave been identified as important further research isneeded into their impact on reducing delirium andimproving outcomes.
Inaccuracy of CAM-ICU scoring may be due tonursing staff being unfamiliar with the tool andthe ease of use of the CAM-ICU scoring sheet. Thelack of documentation may also be due to lack ofunderstanding, education but also lack of a specificplace to document CAM-ICU on the Critical Carechart. Page (2008) found that 8% of scores werenot documented and therefore our score of 50% isextremely poor and needs improvement.
RECOMMENDATIONSWe have developed a re-education programme fornursing staff attending team days in 2012 concen-trating on the CAM-ICU score, documentation andinterventions to prevent delirium. This will enablethis important subject to remain at the forefront and
4 © 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses
Introducing delirium screening in a cardiothoracic critical care unit
improve documentation and implementation of pre-ventative actions. Presentations to the Medical Staff ofthe results of the audit have been made and recom-mendations on how the Critical Care Unit should moveforward including the development of a ‘Delirium CareBundle’ are in process of being developed.
The CAM-ICU scoring sheet (Figure 5) has beenredesigned to make it simpler to follow.
A specific area for charting CAM-ICU score on theICU 24-h chart has been designed and the ‘DeliriumCare Bundle’ has been included in the nursing careplan to remind nursing staff of interventions to preventdelirium.
The unit has purchased clocks, TVs, portable DVDplayers, radios, calendars, developed puzzle booksfor patients who are awake and are paying muchmore attention to ensuring patients are cognitivelystimulated in what can be a very tedious clinicalenvironment. All staffs are much more aware ofdelirium and the need to prevent and treat it andare trying to reduce the amount of bed moves ourlong-term patients undergo. A sleep protocol has beendeveloped which includes recommended medicationand interventions to promote sleep. These include
noise and light control, ensuring patient comfort byaddressing pain and effective positioning, minimizingdisturbances and grouping interventions at night,considering an evening wash to promote sleep and notwaking the patient early in the morning for their washif they are still sleeping. Rest periods have also beenintroduced in the afternoon for all patients between thehours of 1 p.m.–2 p.m. to assist with reducing sleepdeprivation. A study undertaken by Cooper (2000)showed that patients sleep in ICU is severely disrupted,however, the development of delirium due to sleepdeprivation would benefit from further investigation.
CONCLUSIONThe introduction of delirium scoring has enabled allstaff to become more aware of delirium, its causativefactors and preventative actions. Prior to introducingdelirium scoring hypomotoric delirium in patientswould have gone unrecognized. The introduction ofCAM-ICU scoring has enabled improved recognitionof delirium and also enabled us to instigate practice toprevent and treat delirium. Introduction of deliriumscoring is essential in all Critical Care Units toenable recognition and treatment of delirious patients.
YES
YES
No
No
No
INATTENTIONAsk the patient to hold your hand and
squeeze it every time they hear the letter ‘A’. Read out the following letters:
S A V E A
H A A R T
Did the patient make 3 or more mistakes?
YES
DISORGANISED THINKINGA series of 4 of YES/NO questions and then a command.
QuestionsWill a stone float on water?
1) Are there fish in the sea? 2) Does 1 pound weigh more than 2 pounds? 3) Can you use a hammer to hit a nail?
CommandHold up 2 fingers and ask the patient to:
“Hold up this many fingers”
“Now do the same thing with the other hand”
Did the patient make more than 1 mistake?
DELIRIOUS CAM +VE
Refer to treatment of delirium flow chart, inform your bay
co-ordinator/nurse in charge and document on critical care
chart ‘CAM+ve’.
NOT DELIRIOUS
CAM –VE
Document ‘CAM-ve’ on critical care chart and re-
assess again in 12 hours or if mental status/RASS changes.
CAM assessmenteach shift
ALTERED LEVEL OF CONSCIOUSNESS
Has the RASS been anything other than 0 in the last 24 hours?
If RASS is -4 or -5 document on Critical Care Chart ‘UTA CAM-ICU’ and
inform yourbay co-ordinator.
Figure 5 The revised CAM-ICU scoring sheet.
© 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses 5

Introducing delirium screening in a cardiothoracic critical care unit
Interventions to prevent and treat delirium are easy toimplement and assist in improving the quality of careprovided to patients in Critical Care.
ACKNOWLEDGEMENTSThe author would like to acknowledge the follow-ing colleagues for their contribution to data collec-tion, the overall implementation of Delirium Scoring
and preparation of the article for publication: SianMorgan – Matron Cardiothoracic Critical Care; ClareSumner – Administrative Assistant CardiothoracicCritical Care; Debbie Brown – Audit Clerk Cardio-thoracic Critical Care; Phillipa Maslen-Jones – Sister,Cardiothoracic Critical Care; Claire Lashmar – Sister,Cardiothoracic Critical Care; Staff of CardiothoracicCritical Care; Dr Y Shouman – Consultant Anaes-thetist.
WHAT IS KNOWN ABOUT THIS TOPIC
• Delirium has serious consequences leading to increased length of stay, possible development of dementia and even death.• Delirium can be classified into subtypes of hypermotoric, hypomotoric and can also been seen as a mixture of the two.
WHAT THIS PAPER ADDS
• Introduction of delirium screening is challenging but worthwhile in the ICU environment.• Auditing practice identifies areas that are compliant with treatment guidelines and areas in need of review in order to improve compliance.• Continued education assists in ensuring high quality care for patients in critical care.
REFERENCESBorthwick M, Bourne R, Craig M, Egan A, Oxley J (2006).
Detection, prevention and treatment of delirium in criticallyill patients. UKCPA. http://www.ics.ac.uk/intensive_care_professional/standards_and_guidelines/ukcpa_delirium_2006 (accessed 28/10/11).
Cooper AB, Thornley K, Bryan Young G, Sluksky A, Stewart HalyP (2000). Sleep in critically ill patients requiring mechanicalventilation. Chest; 117: 809–818.
Ely W. (2004). Delirium as a predicator of mortality inmechanically ventilated patients in the intensive care unit.Journal of the American Medical Association; 291 (14): 1753–1762.
Girard TD, Pandharipande PP, Ely EW. (2008). Delirium in theIntensive care. Critical Care. http://ccforum.com/content/12/S3/S3 (accessed 28/10/11).
Hua H, Wei D, Hui Y (2006). Olanzapine and haloperidol forsenile delirium: a randomised controlled observation. ChineseJournal of Clinical Rehabilitation; 10 (42): 188–190.
Kalisvaart K, Pun BT, Dittus RS, Thomason JW, Jackson JC,Shintani AK, Ely EW (2006). Haloperidol prophylaxis forelderly hip surgery patients at risk of delirium: a randomisedplacebo-controlled study. Journal of the American GeriatricSociety; 53 (10): 1658–1666.
National Institute for Health and Clinical Excellence (2010)CG 103; Delirium: diagnosis, prevention and management.NICE. http://www.nice.org.uk/guidance/CG103 (accessed28/10/11).
Page V (2009). Routine delirium monitoring in intensive carepatients. Critical Care. http://ccforum.com/content/13/1/R16 (accessed 28/10/11).
Page V (2010). Implementing delirium monitoring. http://www.icudelirium.co.uk/uploads/diy-implementing-delirium.pdf(accessed 28/10/11).
Peterson JF, Pun BT, Dittus RS, Thomason JW, Jackson JC,Shintani AK, Ely EW (2006). Delirium and its motoricsubtypes: a study of 614 critically ill patients. The Journalof the American Geriatrics Society; 54: 479–484.
Pun BT, Ely EW. (2007). The importance of diagnosing andmanaging ICU delirium. Chest; 132 (2): 624–636.
Walters C. (2008). Delirium in the intensive care unit: a narrativereview of published assessment tools and the relationshipbetween ICU delirium and clinical outcomes. Journal of theIntensive Care Society; 9 (1): 46–50
6 © 2012 The Author. Nursing in Critical Care © 2012 British Association of Critical Care Nurses





























