Embed Size (px)
Citation preview

IntroductionTon Kuijpers
Content
• Background and rationale for revisiting guideline methodology
• GRADE approach
– Quality of evidence
– Strength of recommendations
• Grade Working Group

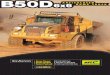
Systematic review
Guideline development
P
I
C
O
Outcome
Outcome
Outcome
Outcome
Formulate question
Rate importance
Critical
Important
Critical
Not important
Create
evidence profile
with GRADEpro
Summary of findings
& estimate of effect for each outcome
Rate
overall quality of evidence
across outcomes based on
lowest quality
of critical outcomes
RCT start high,
obs. data start low
1. Risk of bias
2. Inconsistency3. Indirectness
4. Imprecision
5. Publication
bias
Gra
de
do
wn
Gra
de
up
1. Large effect
2. Dose response
3. Confounders
Rate quality of
evidence for
each outcome
Select outcomes
Very low
Low
Moderate
High
Formulate recommendations:
•For or against (direction)
•Strong or weak (strength)
By considering:�Quality of evidence
�Balance benefits/harms
�Values and preferences
Revise if necessary by considering:
�Resource use (cost)
• “We recommend using…”
• “We suggest using…”• “We recommend against using…”
• “We suggest against using…”
Outcomes
across studies
Content
• Background and rationale for revisiting guideline methodology
• GRADE approach
– Quality of evidence
– Strength of recommendations
• Grade Working Group

Different grading systems
Recommendation for use of oral anticoagulation in patients with
atrial fibrillation and rheumatic mitral valve disease
Evidence Recommendation
• B Class I
• A 1
• IV C
Organization
� AHA
� ACCP
� SIGN
Which grading system?

Hierarchy of evidence
Gradering
A1 Systematic reviews / meta-analysis
A2 Randomised controlled trials (RCT)
B Comparative studies (i.e. cohort studies)
C Non-comparative studies
D Expert opinion
Hierarchy of evidence
Gradering
A1 Systematic reviews / meta-analysis
A2 Randomised controlled trials (RCT)
B Comparative studies (i.e. cohort studies)
C Non-comparative studies
D Expert opinion

Hierarchy of evidence
Expert Opinion
BiasStudy design
•Randomized Controlled Trials
•Cohort Studies and Case Control Studies
•Case Reports and Case Series,
Non-systematic observations
•Expert opinion
Hierarchy of evidence
Expert O
pinion
Bias

Limitations of existing systems
• confuse quality of evidence with strength of recommendations
• lack well-articulated conceptual framework
• criteria not comprehensive or transparent
GRADE unique
• breadth, intensity of development process
• wide endorsement and use
• conceptual framework
• comprehensive, transparent criteria
• focus on all important outcomes related to a specific question
and overall quality

Content
• Background and rationale for revisiting guideline methodology
• GRADE approach
– Quality of evidence
– Strength of recommendations
• Grade Working Group
The GRADE approach
1. quality of evidence (4 categories)
• high
• moderate
• low
• very low
2. recommendations (2 grades)
• strong
• weak (conditional)

The GRADE approach
1. quality of evidence (4 categories)
• high
• moderate
• low
• very low
Systematic review
Guideline development
P
I
C
O
Outcome
Outcome
Outcome
Outcome
Formulate question
Rate importance
Critical
Important
Critical
Not important
Create
evidence profile
with GRADEpro
Summary of findings
& estimate of effect for each outcome
Rate
overall quality of evidence
across outcomes based on
lowest quality
of critical outcomes
RCT start high,
obs. data start low
1. Risk of bias
2. Inconsistency3. Indirectness
4. Imprecision
5. Publication
bias
Gra
de
do
wn
Gra
de
up
1. Large effect
2. Dose response
3. Confounders
Rate quality of
evidence for
each outcome
Select outcomes
Very low
Low
Moderate
High
Formulate recommendations:
•For or against (direction)
•Strong or weak (strength)
By considering:�Quality of evidence
�Balance benefits/harms
�Values and preferences
Revise if necessary by considering:
�Resource use (cost)
• “We recommend using…”
• “We suggest using…”• “We recommend against using…”
• “We suggest against using…”
Outcomes
across studies

I B II V III
Quality: High
Quality: Moderate
Quality: Low
Old system
GRADE is outcome-centric
Rate the relative importance of the outcomes
• Patient important outcomes!
• Maximum 7
• Rate the importance on a 9-point scale
7 – 9 critical for making a decision
4 – 6 important, but not critical for making a decision
1 – 3 not important

Rate the relative importance of the outcomes
Hierarchy of outcomes according to their importance to assess the effect of phosphate-lowering drugs in patients with renal failure and
hyperphosphatemia (Guyatt GH et al. Journal of Clinical Epidemiology 64 (2011) 395-400)
Definition ‘quality of evidence’
• The quality of evidence reflect the extent of our confidence that
the estimates of the effect are correct

Quality of evidence
Quality Symbol Interpretation
High ⊕⊕⊕⊕ We are very confident that the true effect lies close to that of the
estimate of the effect.
Moderate ⊕⊕⊕Ο We are moderately confident in the effect estimate: The true effect
is likely to be close to the estimate of the effect, but there is a
possibility that it is substantially different
Low ⊕⊕ΟΟ Our confidence in the effect estimate is limited: The true effect
may be substantially different from the estimate of the effect.
Very low ⊕ΟΟΟ We have very little confidence in the effect estimate: The true
effect is likely to be substantially different from the estimate of
effect.
Quality criteria
Design Initial quality of a body of
evidence
Lower if Higher if Quality of body of evidence
RCT High → Study limitations
Inconsistency
Indirectness
Imprecision
Publication bias
Large effect
Dose response
All plausible
confounding &
bias
−would reduce a
demonstrated effect−would suggest a
spurious effect when
results show no effect
High
Moderate
Observational
study
Low → Low
Very low

Determinants of quality
• RCTs start high
• observational studies start low
• 5 factors lower the quality of evidence
– risk of bias (Risk of Bias)
– inconsistency
– indirectness
– imprecision
– reporting bias
Determinants of quality
• 3 factors can increase the quality of evidence
– strong association
– dose-respons relationship
– all plausible confounding & bias

Overall quality of evidence
Overall quality of evidence
=
Quality of evidence of the critical outcome with lowest rating
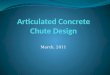
GRADE evidence profile


GRADEpro
http://www.cc-ims.net/gradepro

Example: chronic non-specific low back pain
Key question
Should NSAIDS be used for chronic non-specific low back pain?
Relative importance of the outcomes
Patient relevant outcome Mean score*
1. Pain 8 CRITICAL
2. Disability 8 CRITICAL
3. Return to work 7 CRITICAL
4. Quality of life 6 IMPORTANT
5. Side effects 8 CRITICAL
* Mean score of the 14 members of the GDG (including 2 patients)

Analysis
Analysis 01.01 NSAIDs vs placebo for chronic non-specific LBP, Change in Pain Intensity from baseline on 100mm VAS.
Follow up <=12 weeks.
Analysis 01.02 NSAIDs vs placebo for chronic non-specific LBP, Total adverse events. Follow up <=12 weeks.

GRADE evidence profile

Overall quality of evidence
=
low
Systematic review
Guideline development
P
I
C
O
Outcome
Outcome
Outcome
Outcome
Formulate question
Rate importance
Critical
Important
Critical
Not important
Create
evidence profile
with GRADEpro
Summary of findings
& estimate of effect for each outcome
Rate
overall quality of evidence
across outcomes based on
lowest quality
of critical outcomes
RCT start high,
obs. data start low
1. Risk of bias
2. Inconsistency3. Indirectness
4. Imprecision
5. Publication
bias
Gra
de
do
wn
Gra
de
up
1. Large effect
2. Dose response
3. Confounders
Rate quality of
evidence for
each outcome
Select outcomes
Very low
Low
Moderate
High
Formulate recommendations:
•For or against (direction)
•Strong or weak (strength)
By considering:�Quality of evidence
�Balance benefits/harms
�Values and preferences
Revise if necessary by considering:
�Resource use (cost)
• “We recommend using…”
• “We suggest using…”• “We recommend against using…”
• “We suggest against using…”
Outcomes
across studies

Content
• Background and rationale for revisiting guideline methodology
• GRADE approach
– Quality of evidence
– Strength of recommendations
• Grade Working Group
Evidence to recommendation (EtR)
Factors
Evidence
Factors
Recommendation

Strength of recommendation
“The strength of a recommendation reflects the extent to which we
can, across the range of patients for whom the recommendations
are intended, be confident that desirable effects of a management
strategy outweigh undesirable effects.”
Desirable and undesirable effects
• Desirable effects
– mortality
– improvement in quality of life, fewer
hospitalizations/infections
– reduction in the burden of treatment
– reduced resource expenditure

Desirable and undesirable effects
• Undesirable effects
– deleterious impact on morbidity, mortality or quality of life,
increased resource expenditure
Determinants of the strength of a recommendation
• Quality of the evidence
• Balance between desirable and undesirable effects
• Values and preferences
• Costs (resource allocation)

Developing recommendations
Implications of a strong recommendation
• Patients: Most people in this situation would want the
recommended course of action and only a small proportion
would not
• Clinicians: Most patients should receive the recommended
course of action
• Policy makers: The recommendation can be adapted as a
policy in most situations

Implications of a weak recommendation
• Patients: The majority of people in this situation would want
the recommended course of action, but many would not
• Clinicians: Be prepared to help patients to make a decision
that is consistent with their own values/decision aids and
shared decision making
• Policy makers: There is a need for substantial debate and
involvement of stakeholders
Example: chronic non-specific low back pain
Key question
Should NSAIDS be used for chronic non-specific low back pain?

Overall quality of evidence
=
low
Overall quality of evidence Low
Factors Judgement Explanation
1. Quality of evidence
Is there high or moderate quality evidence? ☐ yes☒ no
…
2. Balance of benifits versus harms and burdens
Are you confident that the benefits outweigh the harms and
burden or vice versa?
☐ yes☒ no
…
3. Values and preferences
Are you confident about the assumed or identified relative values
and are they similar across the target population?
☐ yes☒ no
…
4. Resource implications
Are the resources worth the expected net benefit from following
the recommendation?
☐ yes☒ no
…
Strength of recommendation Weak (conditional)

Recommendation
We suggest the use of NSAID’s for pain relieve on the short term. Due to
potential harms it important to discuss alternative options (wait and see
policy) with the patient.
Given the low quality of the (overall) evidence and the uncertainty of the balance
between benefits and harms the GDG did only suggest the use of NSAID’s for
pain relieve. It is important to discuss the potential harms and alternative
options with the patient.
Rationale
Content
• Background and rationale for revisiting guideline methodology
• GRADE approach
– Quality of evidence
– Strength of recommendations
• Grade Working Group

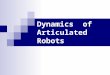
GRADE Working Group
• 2x a year meeting ‘GRADE Working Group’
• Publications in -among others- BMJ (2008) and JCE (2011/2013)
Website: www.gradeworkinggroup.org
Organizations
2005 2006 2007 2008 2009 2010 201320122011

Systematic review
Guideline development
P
I
C
O
Outcome
Outcome
Outcome
Outcome
Formulate question
Rate importance
Critical
Important
Critical
Not important
Create
evidence profile
with GRADEpro
Summary of findings
& estimate of effect for each outcome
Rate
overall quality of evidence
across outcomes based on
lowest quality
of critical outcomes
RCT start high,
obs. data start low
1. Risk of bias
2. Inconsistency3. Indirectness
4. Imprecision
5. Publication
bias
Gra
de
do
wn
Gra
de
up
1. Large effect
2. Dose response
3. Confounders
Rate quality of
evidence for
each outcome
Select outcomes
Very low
Low
Moderate
High
Formulate recommendations:
•For or against (direction)
•Strong or weak (strength)
By considering:�Quality of evidence
�Balance benefits/harms
�Values and preferences
Revise if necessary by considering:
�Resource use (cost)
• “We recommend using…”
• “We suggest using…”• “We recommend against using…”
• “We suggest against using…”
Outcomes
across studies
Conclusions
• GRADE is gaining acceptance as international standard
• Criteria for evidence assessment across questions and outcomes
• Criteria for moving from evidence to recommendations
• Simple, transparent, systematic
– four categories of quality of evidence
– two grades for strength of recommendations
• Transparency in decision making and judgments is key