Embed Size (px)
Citation preview

INTRODUCTION
• The Solution: Point-of-care (POC) continuous glucose sensors offer significant promise for real-time control and artificial pancreas systems in general diabetes.
• The Problem with the Solution: Outlying errors up to 40% with standard deviations of 10-17%1,2.
• The Actual Problem: Large errors inhibit model parameter identification for real-time model-based control3,4. Such errors can span several different clinical action ranges, especially if glucose is tightly controlled to 75-140 mg/dL.
• A Solution to the Actual Problem with “The Solution”: An array of filters that reduces mean absolute errors to less than 5% with minimal lag would enhance the potential for real-time control using these types of continuous glucose sensors.
• Parallel non-linear median filters remove outliers using 3 and 7 consecutive measurements. The output is given to a least mean squares (LMS) filter to further smooth the result.
• Monte Carlo simulations (n=10) using glucose data from 20 critical care patients with a realistic continuous sensor error model.
• Error model has 20% outliers over 20% error with overall mean absolute errors of 9-10%1-3.
• Data: 2410 hours (mean: 120.5 hours/patient, range: 34-502 hours).
• Mean absolute percentage error (MAPE) and its standard deviation are reported after filtering, both overall and for each patient.
J. G. Chase, X. Chen, H. Sirisena, G. Shaw, X. W. Wong, C. E. Hann, A. Le Compte, J. Lin, T. Lotz
Hierarchical Real-Time Filtering for Continuous Glucose Hierarchical Real-Time Filtering for Continuous Glucose Sensor DataSensor Data
METHOD: Filter Array Block Diagram
RESULTS
REFERENCES
[1] P. A. Goldberg, M. D. Siegel, R. R. Russell, R. S. Sherwin, J. I. Halickman, D. A. Cooper, J. D. Dziura, and S. E. Inzucchi, "Experience with the continuous glucose monitoring system in a medical intensive care unit," /Diabetes Technol Ther/, vol. 6, pp. 339-47, 2004.
[2] B. Guerci, M. Floriot, P. Bohme, D. Durain, M. Benichou, S. Jellimann, and P. Drouin, "Clinical performance of CGMS in type 1 diabetic patients treated by continuous subcutaneous insulin infusion using insulin analogs," Diabetes care, vol. 26, pp. 582-9, 2003.
[3] J. G. Chase, G. M. Shaw, X. W. Wong, T. Lotz, J. Lin, and C. E. Hann, "Model-based Glycaemic Control in Critical Care - A review of the state of the possible," /Biomedical Signal Processing & Control/, vol. 1, pp. 3-21, 2006.
[4] J. G. Chase, C. E. Hann, M. Jackson, J. Lin, T. Lotz, X. W. Wong, and G. M. Shaw, "Integral-based filtering of continuous glucose sensor measurements for glycaemic control in critical care," Comput Methods Programs Biomed, vol. 82, pp. 238-47, 2006
PATIENTMean Absolute % Error
(MAPE)5% ~ 95% MAPE
SPRINT Patients
1 1.6 [0.1 3.7]
2 1.4 [0.1 3.4]
3 1.3 [0.1 3.4]
4 1.4 [0.1 3.7]
5 1.4 [0.1 3.7]
6 1.4 [0.1 3.7]
7 1.4 [0.1 3.6]
8 1.3 [0.1 3.7]
9 1.5 [0.1 3.9]
10 1.5 [0.1 4.0]
Overall A 1.4 [0.1 3.7]
Retrospective Patients
1 2.8 [0.2 8.3]
2 3.4 [0.2 9.3]
3 3.4 [0.2 8.4]
4 3.2 [0.2 8.8]
5 2.8 [0.2 8.9]
6 3.0 [0.2 7.8]
7 3.2 [0.2 9.4]
8 3.1 [0.2 7.7]
9 2.9 [0.2 8.9]
10 2.6 [0.2 8.7]
Overall B 2.6 [0.2 8.4]
All Patients (A & B) 1.8 [0.1 5.4]
-0.5 -0.4 -0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 0.50
500
1000
1500
Decimal Percentage Error
Nu
mb
er o
f P
oin
ts (
of
7200
)
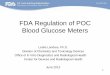
Random Noise Model Results for 1 Patient (7200 mins data)
%Outliers = 24% outsideA band
MAPE = 9.8%
0 5 10 15 20 250
5
10
15
20
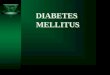
25Clarke Error Grid Plot for 20 Patients
Noisy Blood Glucose Level(mmol/L)
Tru
e B
loo
d G
luc
os
e L
ev
el (m
mo
l/L
)
A
B
B
C
C
D D
E
E
0 1000 2000 3000 4000 5000 6000 7000 8000 90000
2
4
6
8
10
12
Time(Minutes)
Blo
od
Glu
co
se
Le
ve
l(m
mo
l/L)
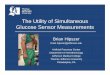
SPRINT Patient Blood Glucose Profile
True Blood Glucose
Noisy Blood GlucoseFiltered Blood Glucose
0 1000 2000 3000 4000 5000 6000 7000 80000
2
4
6
8
10
12
14
Time(Minutes)
Blo
od
Glu
co
se
Le
ve
l(m
mo
l/L)
Retrospective Patient Blood Glucose Profile
True Blood Glucose
Noisy Blood Glucose
Filtered Blood Glucose
CONCLUSIONS
• Continuous glucose data with significant outliers can be effectively filtered using a hierarchy of non-linear median filters and smoothing via LMS or splines.
• More volatile data is more sensitive to error.• Sensor lag is approximately 10 minutes.
• Future Work: this approach does not account for calibration drift or bias – coming soon!
• Noise has ~80% in A-band
• MAPE ~10%1-3
• Estimated for filter design
• Filter removes outliers
• Outliers and variability are too big for useful model-based control