Embed Size (px)
Citation preview

Non-Interpretive SkillsIntroduction to Radiology

Before You Begin
This module is intended primarily for clinical medical students or interns intending to learn or review non-interpretive radiology skills.
Please note that while not integral, this module series assumes some familiarity with basic imaging techniques and interpretive skills. If you wish to learn or review these concepts, please see our “Interpretive Skills” module series.
If material is repeated from another module, it will be outlined as this text is so that you are aware

Learning Objectives
• Describe how images are produced using different radiographic techniques
• Recognize correct orientation of a chest x-ray
• Locate right and left on a properly oriented x-ray
• Locate right and left, anterior and posterior on a CT scan image
• Name two different x-ray views
• Categorize different tissue densities as most lucent to most opaque on an x-ray

Types of Radiology Exams
• X-rays
• Fluoroscopy
• Computed tomography (CT)
• Magnetic resonance imaging (MR)
• Ultrasound
• Nuclear medicine

Film
X-rays
• Directed toward patient
• Some x-rays are absorbed
and others pass through the
body
• The more x-rays that hit the
film, the darker it will appear

Chest X-ray
Areas that
are white
have
absorbed
a majority
of x-rays
Areas that
are dark
have
absorbed
few x-rays

Shoulder X-ray

Abdominal X-ray

1. Density
2. Thickness
3. Superimposition of different structures
X-rays
Degree of whiteness seen on an x-ray is an effect of three different things…

Film
X-ray at the extremes
Metal plate

X-ray at the extremes
Metal plate

Film
X-ray at the extremes
Air

X-ray at the extremes
Air

Air Fat Tissue Bone
Imaging properties: Density
• Density of structures effects their appearance
• Four basic densities• Air
• Fat
• Soft tissue
• Bone

Imaging properties: Density

Imaging properties: Thickness
• Two cups with different amounts of H2O
• Similar density when x-rayed from side
• Cup with more water whiter when x-rayed from top

Imaging Properties: Super-Imposition of Different Structures
Overlapping
structures cause
tissues to look
“whiter” or more
dense

Where the two
ribs overlap they
appear more
dense

Where the heart
and spine
overlap they
appear more
dense

Where the lung
and breast tissue
overlap the lungs
appear more
dense

Benefits of X-rays
• They’re fast and
easy!
• Only take a few
seconds to obtain,
similar to taking a
photo

• They can be
portable!
• We have portable x-
ray machines that
can be brought to
the patient’s bedside
Benefits of X-rays

• They can be
portable!
• We have portable x-
ray machines that
can be brought to
the patient’s bedside
Benefits of X-rays

• They can be
portable!
• We have portable x-
ray machines that
can be brought to
the patient’s bedside
If the patient is well enough, the quality of an x-ray is usually
better if the patient can be transported to the Radiology dept
Benefits of X-rays

• They can be
portable!
• We have portable x-
ray machines that
can be brought to
the patient’s bedside
But if the patient is very ill or in the intensive care unit, portable
films are very useful!
Benefits of X-rays

• They’re not very
sensitive or specific
• In other words…• We can miss
disease when it’s
present
• We can’t always tell
the difference
between different
diseases
Drawbacks of X-rays

• There is an area of
increased density in
the lung which is
abnormal
• But…we can’t tell
what it is for sure
• Other types of
radiology exams
are better at giving
a definitive answer
Drawbacks of X-rays

• There is an area of
increased density in
the lung which is
abnormal
• But…we can’t tell
what it is for sure
• Other types of
radiology exams
are better at giving
a definitive answer
Drawbacks of X-rays

X-ray Orientation
Right Left
HEART

X-ray Orientation
R L
Don’t confuse “right hand side” or “left hand side” with
radiologic right and left. It’s opposite!

Shoulder X-ray

Shoulder X-ray (same film…just flipped!)

Shoulder X-ray All films need a marker

Film
X-ray Views • View describes the position of
the patient relative to the x-ray
beam
• In this example the beam
enters from posterior to
anterior
• This is called a “PA” film
(posterior to anterior)

Film
X-ray Views • View describes the position of
the patient relative to the x-ray
beam
• In this example the beam
enters from anterior to
posterior
• This is called a “AP” film
(posterior to anterior)

Items closer to film appear smaller!
Object
Film

Items closer to film appear smaller!
Object
Film

AP PA
Heart appears larger on an AP film

AP View

X-ray Views
Most x-rays that show a “frontal” image are AP.
Chest x-rays are really the only exception.

Lateral view of the chest
Film

Lateral View of the Chest
PosteriorAnterior
Inferior
Superior

Lateral View of the Knee
AnteriorPosterior

What structures or organs can we evaluate with X-rays?
Bones
Heart and lungs
Bowel

What structures or organs can we evaluate with X-rays?

What soft tissues can we see?
• Bladder
• Psoas muscle
• Bowel loops
Must be of
different density
than the tissue
next to it!

Fluoroscopy


Fluoroscopy
• Uses “real time” x-rays
• Can watch the images on a video screen while the patient changes positions etc…

Fluoroscopy
• Often used to evaluate swallowing or bowel abnormalities
• An oral contrast agent which appears dense is often used to make the bowel lumen visible on x-ray

Fluoroscopy
• Often used to evaluate swallowing or bowel abnormalities
• Can give functional information, since were not just seeing a single point in time

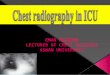
Computed Tomography (CT) Scans
• Uses x-rays
• X-ray camera rotates around patient
• Film (detectors) senses x-rays that pass through patient
• Mathematical equation makes an image of the inside of the body


CT Scans
• An x-ray tube rotates around thepatient in a circle
• X-rays pass through the patient and then are “read” by multipleradiation sensitive detectors
• CT produces a volume of data that the computer can translate into cross sectional images
• Because CT uses x-raysmany of the imaging properties are the same as for plain film x-rays

Red arrow =
rotating x-ray
tube
White arrows =
x-ray detectors

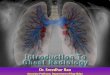
Viewing CT
• CT scans are acquired as cross-sectional (axial, transverse) images
• Viewed as if looking up from the feet• Patient’s right is on
viewer’s left
• If patient supine (face up) -anterior is up
Right
Anterior
Posterior
Left

CT Scans: Orientation
Essentially, CT scans are oriented as if you are a doctor standing at the foot of a patients bedside looking up toward their head as in the illustration below
Right Left
Posterior
Anterior
CT Image provided by Dr. Richard Breiman

CT scans may be obtained at any
location within the body. The next slide
shows CT scans through multiple
locations within the body including the
following:
1.Head
2.Neck
3.Chest
4.Abdomen
5.Mid thigh


Computed Tomography (CT) Scans
Benefits: ➢ Fast
➢ More sensitive and specific
➢ Better soft tissue detail
➢ Better “3D” anatomic evaluation

Computed Tomography (CT) Scans
Benefits: ➢ Fast
➢ More sensitive and specific
➢ Better soft tissue detail
➢ Better “3D” anatomic evaluation

Benefits: ➢ Fast
➢ More sensitive and specific
➢ Better soft tissue detail
➢ Better “3D” anatomic evaluation
Computed Tomography (CT) Scans

Benefits: ➢ Fast
➢ More sensitive and specific
➢ Better soft tissue detail
➢ Better “3D” anatomic evaluation
Computed Tomography (CT) Scans

CT Reformations
Coronal Sagittal

Fracture of Acetabulum?

Transverse or Axial Coronal
CT of the Hip
Confirms fracture
of posterior
acetabulum!

Magnetic Resonance Imaging
• Uses a magnet and radiofrequency pulses
• Images hydrogen protons
• H+ protons are themselves small magnets
• Radiofrequency pulse lines up all H+ protons perpendicular to magnet
• Lined up protons rotate
• We sense this rotation


MRI Imaging
• Measures signal, NOT density
• Signal of tissues different with different MRI settings
• Very specific indications• Brain tumors
• Soft tissues and bones
• Characterization of masses (e.g. liver)
• Heart

MRI Imaging
Comparatively difficult to scan patients :
➢ Long scan times
➢ Have to hold still
➢ Claustrophobia
➢ Loud
➢ Can only scan one body part at a time

Comparatively difficult to scan patients :
➢ Long scan times
➢ Have to hold still
➢ Claustrophobia
➢ Loud
➢ Can only scan one body part at a time
MRI Imaging

Comparatively difficult to scan patients :
➢ Long scan times
➢ Have to hold still
➢ Claustrophobia
➢ Loud
➢ Can only scan one body part at a time
MRI Imaging

Comparatively difficult to scan patients :
➢ Long scan times
➢ Have to hold still
➢ Claustrophobia
➢ Loud
➢ Can only scan one body part at a time
MRI Imaging

Comparatively difficult to scan patients :
➢ Long scan times
➢ Have to hold still
➢ Claustrophobia
➢ Loud
➢ Can only scan one body part at a time
MRI Imaging

Safety issues:
• Very strong magnet!
• Projectiles
• Metal implants, foreign bodies & prosthetic devices
MRI Imaging

MRI Imaging

• Why do we do it then???
• Because it’s the best imaging test for certain
things- Musculoskeletal injuries
- Spine
- Brain tumors
MRI Imaging

Ultrasound
• Ultrasound or sonography uses sound waves to create image
• Like MRI there is no radiation (x-rays)
• Different tissues reflect the sounds waves to different degrees. The more reflective a tissue, the brighter it appears on the image
• Images are obtained “real time”by an ultrasound technician (sonographer) or radiologist

Ultrasound
• Ultrasound is used
frequently to image children
and fetuses because there
is no radiation exposure

Ultrasound
• A technologist or physician holds a transducer on the surface of a patient
• The transducer produces very rapid high frequency sound pulses that travel into the patient
• Tissues reflect a small percentage of these sound waves back to the transducer

Ultrasound
• Most tissues have similar acoustic impedances (attenuate the sound beam)
• Stronger attenuators include bone and air
• When sound passes from one tissue (with a particular acoustic impedance) to another tissue (with a different acoustic impedance), some energy is reflected at the interface
• The greater the difference in impedance between the tissues, the greater the reflection

Ultrasound
• The more sound waves are reflected, the whiter a tissue will appear
• The transducer can calculate the depth of the tissue that reflected the sound waves by measuring the time between their production and return
• Using these two pieces of information (tissue depth and reflectivity), the ultrasound machine creates an image

Fat Muscle
Sound wave or “pulse”
Reflectionor “echo”
When the sound beam passes from one tissue to another (with different acoustic impedences), some of the energy is reflected at the interface between the two tissues

Fat Muscle Liver Fluid
Since the impedence values are similar for most tissues, only a small fraction of the sound beam is reflected at interfaces. This allows most of the energy to penetrate deeper (to the next tissue interface) and be reflected to form an image there, and so on through the depth of the area being imaged.

Fluid (bile) in gallbladder
Ultrasound
• Ultrasound images
seem difficult to
interpret because they
are of lower resolution
• One general rule with
ultrasound is that fluid
appears black

Nuclear Medicine
• Something is tagged with radioactive material
• A tiny amount is injected into the body
• Images are taken with a gamma camera
• Physiologic imaging
• Very poor anatomic resolution

Learning Objectives• Describe how images are produced using different radiographic
techniques
• Recognize correct orientation of a chest x-ray
• Locate right and left on a properly oriented x-ray
• Locate right and left, anterior and posterior on a CT scan image
• Name two different x-ray views
• Categorize different tissue densities as most lucent to most opaque on an x-ray

END