Embed Size (px)
Citation preview

Lesson 1: INTRODUCTION TO EPIDEMIOLOGY
OUTLINE OF PRESENTATION
Block description, Learning outcomes, Course materials
Student contributions and grading Introduction to epidemiology: definitions, aims,
use of epidemiology in medicine, target and study populations, sampling, recruiting, collecting data, data analysis
Group task for today

INTRODUCTION TO EPIDEMIOLOGY
confusion accompanying the term "epidemiology. An apocryphal story is told around CDC that illustrates the confusion sometimes accompanying the
term "epidemiology.
It seems that one of our scientists, on first arriving at CDC from a clinical practice, found himself somewhat unsure of what epidemiology was all about, so he sought an answer down the street at Emory University.
1. The first person he asked was a medical student, who told him that epidemiology was "the worst taught course in medical school.“
2. The second, a clinical faculty member, told him epidemiology was "the science of making the obvious obscure.“
3. Finally, knowing that statistics are important to epidemiology, he asked a statistician, who told him that epidemiology is "the science of long division" and provided him with a summary equation.
4. Giving up on finding a real answer, he returned to CDC. On the way, however, he decided to try one more time. He stopped a native Atlantan who told him that epidemiology was "the study of skin diseases
5. Does it mean the term “Epidemiology” is only understood by Epidemiologist?

What is epidemiology anyway DEFINITIONS OF EPIDEMIOLOGY
1. ‘Epidemiology is the science of epidemics `(Coincide Oxford dictionary,1964)
2. ‘Epidemiology is the study of the distribution and determinants of disease in humans` (McMahon and Pugh,1970)
3. ‘The science of the occurrence of illness’(Miettnen,1978)
4. ‘Epidemiology is the study of how often diseases occur in different groups of people and why’ (Coggon et al, 1997)
5. ‘The study of the distribution and determinants of health-related conditions or events in specified populations, and the application of this study to the control of health problems` (John M Last, 2001).‘(preffered operational defination)

INTRODUCTION TO EPIDEMIOLOGY MAJOR COMPONENTS OF THE DEFINATION Population: The main focus of epidemiology is the effect of disease on the population rather than individuals. Epidemiology deals with endemic, epidemic and pandemic diseases in a population rather than case studies or case s Frequency: This shows that epidemiology is a quantitative science which is concerned with the frequency(occurrence) of diseases and other health related conditions. Health related conditions: Epidemiology is concerned not only with disease but also with other health related conditions such as injuries, births, health related behaviors like smoking, unemployment, poverty etc. Distribution: Distribution refers to the geographical distribution of disease by time, person or place. Determinants: Determinants are factors which determine whether or not a person will get the disease. Application of the studies to the promotion of health and to the prevention and control of health problems: This means the whole aim in studying frequency, distribution and determinants of disease is to identify effective disease prevention and control strategies.

INTRODUCTION TO EPIDEMIOLOGY The definition can furthermore be explained as follows:
1st part of the definition of epidemiology states as follows:
The study of the distribution s of health-related conditions or events in specified populations using morbidity measures such as incidence rate, prevalence etc.
2nd part of the definition of epidemiology state as follows
The study of the determinants of health-related conditions or events in specified populations.
Determinants are risk factors that may
Cause disease(etiologic agent of disease) e.g. Mycobacterium tuberculosis is the etiologic agent of pulmonary tuberculosis. These are called sufficient cause factors to inevitably produce disease
Be associated with disease(necessary cause, contributing, predisposing or aggravating risk factors e.g. pulmonary TB is associated withlow accumulated wealth OR= 16.70), financial insecurity (5.67), consumption of unpasteurized milk (3.58), diabetes (2.66), living with a relative with tuberculosis (2.94), being unemployed (6.10), living in overcrowded conditions (2.99), illicit drug use (8.74),

INTRODUCTION TO EPIDEMIOLOGY Determinants are divided into environmental and of genetic origin. Environmental determinants are classified as 1. Physical agents e.g. humidity, altitude,noise pollution,
lighting, temperatures ,air pollution, gravity, atmospheric pressure, sewage pollution, vibration, radiation
2. Chemical agents e.g. ozone(free radicle),sulphur dioxide, nitrogen oxides, carbon dioxide(greenhouse gas), nitrogen, argon methane(greenhouse),benzene, industrial smoke, tobacco smoke, radon, asbestos dust, arsenic pesticides, fungicides, some food additives.lead, nicotine, tobacco smoke,

INTRODUCTION TO EPIDEMIOLOGY
3. Biological agents e.g. bacteria, viruses such as Hepatitis ,Human papilloma virus, fungi such as Aspergilla's producing mycotoxins e.g. aflatoxins,Protozoa and
Torch organisms
T=Toxoplasma parasite
O =Other agents
R=Rubella virus (German measles)
C=Cytomegalovirus
H=Herpes simplex virus Genetic origin

4. Biological genetic agents : Phenylalanine hydroxylase enzyme
Babies born without phenylalanine hydroxylase, an enzyme that metabolises the amino acid phenylalanine to tyrosine. The health related condition is called Phenylketonuria (PKU) which is an inherited disorder of metabolism that causes an increase in the blood of a chemical known as phenylalanine
Other host risk factors include gender, race age occupation,socio economic status(SES),immune status, previous diseases
Personality traits as observed in Type A behaviour and usually characterised by aggressiveness, competitiveness, ambition, restlessness and impatience and thus have high rates of coronary heart diseases(CHD) as compared to Type B behaviour,
Such Personality traits are said to be associated with predictive increased probability of developing coronary heart disease(CHD)

INTRODUCTION TO THE PROMOTION,PREVENTION AND CONTROL OF DISEASES
3rd part of the definition of epidemiology states as follows
The application of this study to the control and prevent ion of health problems
Control of health problems: This is achieved by
i. Introduction of disease control programmes that aims at reducing disease or lower the incidence of disease
ii. Introduction of ddisease eradication programmes that aims at removing disease from all human population.
iii. Introduction of disease control programmes that aims at eliminating disease from defined areas
Prevention of health problems: This is achieved by
Implementation of prevention programmes such as
I. Primordial prevention of disease or exposure
II. Primary prevention of disease or exposure
III. Secondary prevention of and disease
IV. Tertiary prevention disease

INTRODUCTION TO THE PROMOTION, PREVENTION AND CONTROL OF DISEASES
Primordial prevention Primordial prevention is defined as prevention of risk factors themselves, beginning with change in social and environmental conditions in which these factors are observed to develop, and continuing for high risk children, adolescents and young adults
Primary prevention of disease: keeps the disease process from becoming established by eliminating causes of diseases or increasing resistance to disease. Examples include immunisation and reducing exposure to a risk factor.
The objective of primary prevention is
to promote health,
prevent exposure and
Control the disease.
Secondary prevention of and disease: This is an early detection of the existing disease to reduce the severity and complications. Examples include screening for cancer.
Tertiary prevention disease : This reduces the impact of the disease: examples include rehabilitation for stroke

INTRODUCTION TO THE PROMOTION, PREVENTION AND CONTROL OF DISEASES
4thly epidemiology is also concerned with “study of the natural history and prognosis of disease”
In order to understand the prevention of disease at various levels, we need to first to understand its natural history.
The natural history of disease refers to the course of diseases over time unaffected by treatment.
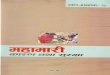
There are four stages of diseases viz
Stage of susceptibility
Stage of presymptomatic disease(Preclinical stage)
Stage of clinical disease(clinical stage)
Stages of cure, disability or death

No disease
Primary Secondary Tertiary Prevention Prevention Prevention
Normal Preclinical Phase Clinical Phase
Clinical
Outcome
No Disease
Biologic Symptom's Disease Therapy Given
Onset Of Disease First Appear Diagnosed

INTRODUCTION TO THE NATURAL HISTORY OF DISEASES
Stage of susceptibility
In this stage ,disease has not developed but the groundwork has been laid by the presence of factors that favour its occurrence.
Example:Unvaccinated child is susceptible to measles
Stage of presymptomatic phase(subclinical) disease
In this stage there are no manifestation of disease but pathologic changes(damages) have started to occur. The disease can only be detected through pathognomonic test(screeing test) since the sighns and symtoms of the disease are not present.
Examples:Detection of antibodies in an apparently healty person
Ova of intestinal parasite in the stool of apparently healthy children

INTRODUCTION TO THE NATURAL HISTORY OF DISEASES
The clinical stage and prognosis
At this stage the person has developed sings and symptoms of the disease. The clinical stage of different diseases differs in duration, severity and outcome. The outcomes of this stage may be recovery, disability or death
Recovery stage: Some diseases run their course and then resolve completely, either spontaneously or under the influence of therapy.
Example: Common cold has a short and mild clinical stage and almost everyone recovers quickly
Disability stage: In this stage disease may result in residual defect, living the person disabled for a short or longer duration
Example:
Polio has a severe stage and many patients developed paralysis becoming disabled for the rest of their lives.
Trachoma may cause blindness.
Death stage:
Example
Rabies has a relatively short but severe clinical stage and almost results in death.
Death stage Diabetes Mellitus has a relatively longer clinical stage and eventually results in death if the patient is not properly treated

INTRODUCTION TO THE PROGNOSIS OF DISEASE Fifthly epidemiology is concerned with the ‘PROGNOSIS OF DISEASE” Prognosis is the measurement of the probability of clinical outcome of disease and can therefore be expressed in term of recovery, disability, survival or death
1. Stage of recovery 2. Stage of disability Some diseases can give rise to a residual defect of short or long duration leaving the person disabled to a greater or lesser extent.
3. Stage of survival: Survival from a disease is measured in various forms and include Five year survival Observed survival Median survival time Relative survival
4. Stage of death: Mortality can be expressed by Case fatality or Person years
Definition of case fatality: Case fatality is a proportion defined as the number of people who die of a disease divided by number of people who have the disease.

Further more epidemiology is concerned with the evaluation of new preventive and therapeutic measures and new modes of health care delivery
It provide the foundation for developing public policy and regulating decisions relating to environmental problems.
It is used in planning and evaluation of strategies to prevent illness

How epidemiologist view the world compared to pessimist and optimist
1. Pessimist view: The glass is half
empty.
2. Optimist: view: The glass is half full.
3. Epidemiologist view: The glass is half empty as
compared to what: – or
The glass is half full as compared
to what:
NTRODUCTION TO EPIDEMIOLOGY

INTRODUCTION TO MORBIDITY MEASURES Measurement of frequency of disease :
The 1st part of the definition viz ‘The study of the distribution of health related conditions or events’ is explained as follows :
The measurement of frequency of disease is measured by morbidity measures such as
(attack rates,, prevalence proportion and incidence rates).
It is important to note that all measurements used in epidemiological studies are based on the understanding of the basic indices of ratios, proportions and rates.
1. Ratio: A ratio is simply one number divided by another number such that the numerator and the denominator are separate quantities neither being included into other. The ratio of two numbers , x and y is simply expressed as x /y or x:y A ratio has no dimension and no fixed range,
Examples of morbidity ratios(LESSON 3)
Risk ratio (RR)(ratio of two probabilities e.g. risk in those exposed divided by risk in those unexposed or the proportion in those exposed divided by the proportion of those unexposed and the
Odds ratio (OR) which in cohort study is defined as the odds of outcome occurring in exposed persons divided by the odds of outcome occurring in unexposed persons. and
In case-control studies, the OR is defined as the odds of exposure in cases divided by the odds of exposure in controls.

INTRODUCTION TO MORBIDITY MEASURES
2. Proportions : A proportion is a special type of ratio in which everyone in the numerator is also counted in the denominator e.g. a/a+b
A note about proportions In epidemiologic terms the denominator in proportions should be at risk of being included in the numerator Proportions can be expressed as a number between 0 and 1 or as percentage between 0% and 100%. All proportions are ratios –not all ratios are proportions
Examples of morbidity proportions include: i. Attack rate(not a rate but a proportion) is defined as the number of
people exposed to a suspect food who became ill divided by the number of people who were exposed to that food i.e.
a/a +b*k population
Attach rate per 1000=
number of people exposed to a suspect food who became ill * 1000 population
number of people who were exposed to that food

INTRODUCTION TO MORBIDITY MEASURES ii. Prevalence of disease which is the number of people
with the disease divided by the number of people with the disease plus the number of people without the disease, that is the populations at risk of the disease.
Prevalence per 1000 population= no of existing cases of disease@ a specified time * 1000 population @ risk at that specified time Other measures for proportions include(Lesson 4) 1. Sensitivity 2. Specificity, 3. Positive protective value (PPV) 4. Negative protective value (NPV) 5. % Agreement between two or more observers etc.

INTRODUCTION TO MORBIDITY MEASURES 3. Rate: Rate is a special form of a proportioning that includes time.it is the
measure that most clearly expresses probability or risk of disease in a defined population over a specified period of time
incidence rate as an example of a rate is defined as the rate at which new cases of disease that occur during a specified period of time in a population at risk for developing the disease i.e. IR per 1000 = Number of new cases of disease in a specific period * k Population at risk i.e. is the number of people with the disease plus number of people without the disease in a specified period IR=Total # of new cases of a disease over a period of time * k population @ risk during the given period of time A note about incidence rate Incidence rates measures transition from a non diseased to a diseased state and
is therefore a measure of a risk. the risk can be looked at in any population by age(age specific incidence rate, by
sex(sex specific incidence rate), by socio economic status(SES specific incidence rate, by occupation(occupation specific incidence rate or by air, water or food contamination(air polluted specific incidence rates, water polluted specific incidence rate and food polluted specific incidence rate etc.
Other measures of rates includes ?????

INTRODUCTION TO MORBIDITY MEASURES
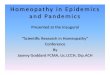
Illustration of incidence rate and prevalence
• Died =
• Cured =
Jan May July Sep Nov Dec
2012 2012

INTRODUCTION TO MORBIDITY MEASURES
The figure shows five cases of a disease in community in 2012
The 1st case of the disease occurred in 2011 and the patient died in in 2012.
The second case developed in 2012 and continued into 2013.
The third case was person who became ill in 2012 and was cured in 2012
The forth case occurred in 2011 ant the patient was cured in 2011
The fifth case occurred in 2011 and continued through 2012 and into 2013.

INTRODUCTION TO MORBIDITY MEASURES What is the numerator for the incidence in 2012
What is the numerator for the point prevalence for the survey done
in May 2012
What is the numerator for the point prevalence for the survey done in July2012
What is the numerator for the point prevalence for the survey done in September2012
What is the numerator for the point prevalence for the survey done in December 2012
From the above it can be noted that the prevalence of disease depend on the point during the year at which the survey is performed.

INTRODUCTION TO MEASURES OF MORTALITY Measurement of mortality: The measurement of death/mortality is measured by mortality measures such as 1. Mortality rates, 2. Case fatality 3. Proportionate mortality and (not prescribed) 4. Years of potential life lost (not prescribed)
A note about mortality measures Like morbidity measures, they are also based on the understanding of indices. Measurement of death by mortality rates(prescribed) 1. The 1st mortality rate is the annual mortality from all causes Annual mortality rate for all causes(per 1000 population)= # No of death from all causes in 1 year *1000 # No of persons in the population at midyear

INTRODUCTION TO MEASURES OF MORTALITY
2. The 2nd may be that we are only interested in death rates of children up to 7 days of life(perinatal mortality)
Annual perinatal mortality from all causes per 1000 population=
# No of perinatal mortality from all causes in one year *1000
# No of perinatal in the population at midyear
3. The third may be that we are interested in death rates of a specific disease e.g. lung cancer
Annual mortality rate from lung cancer (per 1000 population)=
# no of deaths from lung cancer in one year * 1000
# no of persons in the population at midyear
4. The fourth may be that we are interested in death rates with more than one characteristics for instance age and cause of death e g neonates
Annual neonatal mortality rate(death in children less than 28 days) from leukaemia (per 1000 population)=
#No of death from leukaemia in one year in neonatal * 1000
#No of neonatal in the population at midyear

INTRODUCTION TO MEASURES OF MORTALITY Measurement of death by proportion or % (prescribed) Case fatality= # no of individuals dying during a specified period of time after disease onset or diagnosis No of individuals with the specified disease
Case fatality measures the proportion of those dying from a certain disease within certain time after their disease was diagnosed. Difference between case fatality and mortality rate In mortality rate the denominator represents the entire population at risk of dying from the disease including both those have the disease and those who do not have the disease. In case fatality however the denominators limited to those who already have the disease. Thus case fatality is a measure of the severity of disease. See the hypothetical example Assume a population of 100,000 people of whom 20 are sick with disease X, and in one year,18 of the 20 die from the disease X Mortality rate from disease X = 18 =0.018% 100,000 Case fatality from disease X = 18 = 90% 20

INTRODUCTION TO MEASURES OF MORTALITY Proportionate mortality (not prescribed)
Proportionate mortality measures the proportion of death from a specific disease divided by the total number of death.
Proportionate mortality=
# No of death from a specific disease in 1 year
Total death in that year.
See hypothetical example in comparison of two communities A and B
Community A Community B Mortality rate from all causes 30/1000 15/1000
Proportionate mortality from heart disease 10% 20%
Mortality rate from heart disease 3/1000 3/1000
Years of potential life lost (not prescribed)

INTRODUCTION TO EPIDEMIOLOGICAL DESCRIPTIVE STUDIES
All epidemiological studies are divided into
1. Observational and
2. Experimental studies. (not prescibed)
A note about observational studies
Observational studies measures the effects on disease rates of exposures of interest (as they occur in the population).
They are further subdivided into Descriptive and Analytical studies.
Descriptive studies
Descriptive research design is a type of research method that is used when we want to to get information current status from a populaion about the occurrence of disease. It is used to describe what is in existence in respect to health related conditions or variables that are found in a given situation. Descriptive studies are studies that measures the prevalence of disease s or the prevalence of determinants with and or without taking into consideration the association between the disease and the determinant .
Descriptive studies are subdivided into the following studies.
Case study (prevalence study)
Case series (prevalence study)
Cross sectional study(prevalence study) but also an analytical study.
Thus the unit of measurement for this studies is the prevalence proportion or %

INTRODUCTION TO EPIDEMIOLOGICAL STUDIES
Experimental studies or intervention studies: (not prescribed)
These are studies in which the researcher intervene
The study designs include
1. Clinical trial
2. Preventive trial and
3. Community trial.

INTRODUCTION TO EPIDEMIOLOGICAL STUDIES
Analytical studies
the 2nd part of the definition viz “The study of the determinants of health-related conditions or events in specified populations is best explained by analytical studies. f Analytical studies
1. Analytical studies are done in order to find out if an outcome is related to exposure(determinant)
2. They can take the form of observational (we don’t influence the population), or
3. Interventional/experimental (we influence the population, e.g.: in clinical trials we give drugs (not prescribed)
Types of analytical studies
There are four main types of analytical studies viz
Cross sectional study
Case-control
Cohort studies and
Experimental studies (not prescribed)

INTRODUCTION TO EPIDEMIOLOGICAL ANALYTICAL STUDIES
Cross-sectional measure: Prevalence of exposure together with prevalence of disease Information on exposures and disease status are obtained at the same
point in time. Therefore these studies involve data collection at a defined time. The unit of measurement for cross-sectional studies is
prevalence,(existing cases) not incidence of disease. Case-Control Case-control studies are very useful for rare disease (or other rare
health events) Case-control studies compare exposures in disease cases vs. healthy
controls from the same population. The unit of measurement for case-control studies is odds ratio.

INTRODUCTION TO EPIDEMIOLOGICAL STUDIES
Cohort studies
Cohort studies measures the development of disease in those exposed to those unexposed
The unit of measurement in cohort studies is the incidence rate which is the rate of disease in the exposed group versus the rate of disease in the unexposed group and or in other words the risk ratio(RR)

Population
Population: The main focus of epidemiology is the effect of disease on the population rather than individuals. Epidemiology deals with endemic, epidemic and pandemic diseases in a population rather than case studies or cases Target population :That Part of the population about which information is required for example The study population :That part of the target population which eventually takes part in a survey Population at risk: That part of a population which is susceptible to a disease e.g cancer of the cervix can only affect woman with cervix and not women who did hysterectomy or the whole population: The numerator/denominator should be alike Sample population (Study sample): That part of the population which is representative of the study
population and from which conclusions is drawn about this population. This segment can sometimes be the entire study population (the
accessible part of the target population) when this is a small group, but In most cases a study sample is drawn since study populations are usually too large .

Sample size (n):This refers to the number of patients who finish the study and not the patients who enter. Sample size estimations or calculation are influenced by several factor such as : I. statistical power of the test which must not be lower than 80% II. confidence interval which must not be lower than 95%. III. Study design e.g. (descriptive, ecological, cross-sectional, case-
control, and cohort IV. Type of statistical test e.g. Z test, t test, chi square test and F test
and the p value or p level V. The type of variable you are measuring VI. The results of studies on samples smaller than this sample size
will not be able to be extrapolated back to the study population, and cannot be shown to be “statistically significant

Sampling methods :Sampling methods are divided into probability and non probability sampling methods. Non probability sampling: not every member of the population has a chance(probability) of being sampled. • Convenience sampling: e.g.: Including all available specimens collected within a
specific period convenient to the researcher. • Suitable for lab studies on stored specimens when storage may cause loss of
material. • Suitable for population surveys when time and other resources
Probability sampling Random sampling ensures representativeness (probability sampling) Each individual in the study population has a known equal non-zero probability of selection When sampling frame is known, random number tables / software used Stratified random sampling: different strata with random sampling in each stratum Systematic sampling: e.g.: Randomly select first house / participant then systematically sample thereafter (e.g.: using sampling interval [target population ÷ sample size]).Suitable for vaccination coverage studies
Purposive sampling: Only data-rich specimens / participants are selected. Usually reserved for qualitative studies, but suitable for quantitative studies on rare phenomena / diseases (i.e. exploratory studies, and case-control studies on rare diseases, although random sampling will be used for control group)

For research projects, you will need to submit a protocol and get
• ethical approval from the Medunsa Research Ethics Committee
However, the practical's you will be doing here are meant to introduce you to the practice of epidemiology and prime you for auditing your own medical practice, and are not research projects
Face-to-face recruitment when only verbal consent is needed: This is often the case when you are asking questions that cannot
• possibly cause any harm to participants (e.g.: age, gender, occupation,
• opinion about a product, food preferences, smoking habits
Usually identifiers are not included in this type of questionnaire, i.e.
• participants are anonymous
This is the only method we will be dealing with in this block
Introduce yourself
Explain purpose of the study
Invite to take part

Use the data collection sheets / questionnaires in
• your hand-outs
Once a participant has been recruited (i.e. verbal
• consent given), go ahead and ask the questions
Explain anything in the questions if you see there is
• a misunderstanding, but don’t influence answers
Tick the responses given in the appropriate boxes
At the end, remember to thank your participants
• most kindly!
Keep a count of those who you have approached, so
• that you can calculate the response rate

Read chapters 1,3,4 and 6 of Leon Gordis fith edition
Recruit volunteers and collect data for the descriptive study:
• Asthma in students at Medunsa Campus
The sample size should be 96 (based on what you have
• learned from this lecture), but we will increase this to 120.
This means each student should collect data from 3 Medunsa
• students.
Please use the prepared data collection sheet, which has been
• prepared for the collection of data from 3 participants.
After data collection, meet with your group members and
• summarise all your data on the data summary sheet provided.
Bring all these data collection and data summary sheets back
• to class, and present your summarised data to the class

Stratification of data:
• – There are 10 groups in this class. Come to an agreement
• before you leave this class about which population of
• students each group will approach. Define population at 2
• levels: degree level
year of study level
Example: Let group 1’s study population be MBChB II students
•
Exclude those who have already participated today
Keep a record of those who you have approached
• but have refused (this does not include those who
• have previously participated

THANKS FOR YOUR ATTENTION
AND GOOD LUCK!